
Abstract
Video feedback at home (VFH) aims to improve the well-being of informal caregivers and persons with dementia by training the caregiver to communicate successfully. This feasibility study had 2 aims: (1) to investigate possible effects regarding VFH, caregiver self-efficacy and the burden experienced, and the frequency of challenging behavior in persons with dementia, and (2) to perform a process evaluation of barriers and facilitators regarding the use of VFH. The respondents were caregivers of home-dwelling persons with dementia participating in VHF (N = 10), a group of caregivers who declined participating in VFH (N = 18), stakeholders (N = 6), and field experts (N = 55). The assessments performed were Positive and Negative Affect Scales, Cohen-Mansfield Agitation Inventory, Sense of Competence Scale, semistructured interviews, and questionnaires. Results demonstrated that caregivers were satisfied with VFH and that various (sub)scores on questionnaires improved. Caregivers mentioned a reluctance toward being filmed and both caregivers and referrers were unfamiliar with VFH. Recommendations have been made for health-care professionals and researchers to overcome these barriers.
Introduction
Caring for a person with dementia is demanding and stressful for informal caregivers. 1 Communication problems such as difficulties with finding words, naming, comprehension, and verbal fluency are common in dementia and are known to be associated with challenging behavior 2,3 and social withdrawal of the person with dementia. 4,5 Additionally, both communication problems and challenging behavior are major risk factors for caregiver burden and distress 3,6 –8 and may result in decreased quality of the relationship. 8 –10
Teaching caregivers about the impact of dementia on communication and about adequate communication strategies enables them to support communication with the person with dementia. 11 –15 Although the evidence base for interventions improving communication in dementia is still quite small, 16 previous studies on enhancing communication between caregivers and persons with dementia by training (informal) caregivers in using facilitating communication strategies have shown positive effects on the behavior of persons with dementia, 9,17 on the relationship between caregivers and persons with dementia, 18,19 and on burden levels and feelings toward caring of caregivers. 19
Caregiver training through video feedback (VF) may be useful for improving communication. This is supported by 2 previous studies that apply VF in nursing homes 11,20 and an earlier feasibility study by Williams et al on in-home video recording to support dementia caregivers. 21 Research in child care has shown that interventions using VF are more effective than interventions without VF and that positive feedback may enable positive reinforcement of desirable behavior. 22,23
Video feedback at home (VFH) focuses on supporting informal caregivers and stems from the assumption that problems in interaction can be solved by focusing on the quality of communication and on the strengths of caregivers rather than their shortcomings. 24 The focus on strengths is supported by research demonstrating that enhancing positive behavior is more effective than diminishing negative behavior. 25 VF is based on a successful technique developed in child care. 26 Although it is considered effective in daily practice, there is little scientific evidence for VF 11,20,21 apart from a small number of studies in child care.
Since people with dementia remain at home longer nowadays, supporting their caregivers is becoming increasingly important. This is why we conducted a feasibility study aiming to investigate whether VF may be an applicable and effective intervention for community-dwelling people with dementia and their informal caregivers, to decrease the burden of caregivers and challenging behavior of the person with dementia.
Methods
We performed a nonrandomized pilot study—a subtype of feasibility study. 27 In order to prepare for future randomized controlled trials, we carried out the intervention of interest (pilot effect study) and performed a process evaluation of barriers and facilitators to using the intervention (pilot process evaluation). 27
Pilot Effect Study
Participants
Twenty-five dyads receiving VFH were to be included by 2 health-care organizations in the Netherlands. For practical reasons (limited time frame and funding of the study), a maximum of 25 dyads was deemed possible. This was considered sufficient for the study, as large effects (d = 0.5) may be demonstrated (power of 0.8) using 20 cases with a significance level of .1. Requests for VFH were made by health-care professionals (eg, general practitioner, psychologist, employee of day care facility, case manager). These requests were considered for inclusion if the caregiver mentioned a request for help in “communicating” or “managing the behavior.” Three additional organizations joined during the study to improve recruitment.
Participants were included if the person with dementia had been diagnosed with dementia by a physician and was community dwelling; if the caregiver had a request for help concerning the interaction with the person with dementia; and if both gave informed consent. Data collection took place from September 2012 to May 2014 (originally 12 months, extended twice by 6 and 3 months, respectively, to improve inclusion). In the end, 15 dyads (7 from the first and 8 from the second organization) were referred for a VFH program and agreed to participate in the study.
Design and procedures
Assessments were conducted before and after the VFH program in a pre/postdesign. Certified VF trainers with several years of experience, trained by way of a 5-day theoretical course and 20 hours of supervised practical training, conducted the VFH interventions. Prior to the start of the VFH program, the VF trainer visited the informal caregiver and the person with dementia at their home and determined whether a VFH program was appropriate. The trainer used an assessment form to clarify the caregiver’s needs and determine whether these could be addressed using VFH. If appropriate, the VF trainer asked written informed consent for participating in the study of both the informal caregiver and the person with dementia, with the understanding that their responses and video recordings would be kept strictly confidential and that they could withdraw from the study at any point, without consequences. Pre- and postassessment included questionnaires; postassessments also included a semistructured interview. These were administered to the caregivers in their homes by a trained researcher.
The VFH program
As part of the VFH program, the VF trainer assessed characteristics of the caregiver and the person with dementia, their interaction, difficulties experienced by the caregiver, situations experienced as difficult by the caregiver, and the behavior of the person with dementia, during an initial visit. Based on this, the VF trainer proposed and acquired agreement from the caregiver regarding the specific goals and content of the intervention. During the program, the caregiver was trained by means of several feedback sessions using personal video footage of interaction moments between the person with dementia and the caregiver. The feedback provided focused on 5 basic interaction principles, that is, following the initiative of the person with dementia, confirming the reception of a message, approving, taking turns during the interaction, and leadership in communication. 24 The first recording was of a nondemanding situation, enabling the caregiver to become aware of the basic interaction principles that they were already applying and to explain how these interaction principles could also be used in more demanding situations. Subsequently, video footage was recorded of situations the caregiver had assessed as difficult during the visit before the intervention. This was done in 1 to 4 subsequent instances, with the number depending on the caregiver’s progress, and with about 4 weeks between 2 recordings. After each recording, a 1-hour feedback session was held. The VF trainer made the recordings using a video camera (JVC camcorders, type GZ-MS230BE) and the recordings were stored digitally (MOD-type or VLC media type files) in a safe digital environment within the care organization, accessible only to VF trainers. Files were deleted from the camera on the day of the recording. The intervention was considered successful when the informal caregiver recognized the interaction principles in daily interaction, was able to apply these, and demonstrated insight into communication in problem situations and their own contribution to this process. The VFH programs were concluded with a session (30 minutes) evaluating the intervention with the caregiver and, if possible, the person with dementia.
Measures
Qualitative evaluation
A semistructured interview with the caregiver was set up to investigate the caregiver’s experiences and satisfaction with the VFH program and to obtain a subjective rating by the caregiver regarding the quality of the interaction with their loved one, changes in self-efficacy and burden, and challenging behavior of the person with dementia.
Questionnaires
Informal caregiver affect was measured using the Positive and Negative Affect Scales (PANAS), which consists of 20 items: 10 for the positive and 10 for the negative affect scale. Items are scored on a 5-point Likert scale using “in recent days” as the time frame; the total scores of both scales range from 10 (no positive/negative affects affirmed) to 50 (all positive/negative affects affirmed). This scale has been shown to be internally consistent with good convergent and discriminant validity. 28,29 Caregiver burden was measured using 2 subscales (satisfaction with the care recipient: 11 items, and satisfaction with one’s own performance as a caregiver: 12 items) of the Sense of Competence Questionnaire (SCQ). Both subscales are scored on a 5-point Likert scale. Total scores range from 11 (very dissatisfied) to 55 (very satisfied) and from 12 to 60, respectively. The SCQ was reported to have satisfactory reliability and validity. 30,31 Challenging behavior of the person with dementia was measured using the Cohen-Mansfield Agitation Inventory (CMAI). 32 It consists of 29 items, each rated on a 7-point frequency scale (1-7) ranging from “never” to “several times an hour.” The CMAI items can be summated into a total score with a range from 29 to 203, with a higher score indicating more agitation. The CMAI total score was calculated, as well as 3 subscale scores for physical aggression (range: 8-56), verbal agitation (range: 4-28), and restlessness (range: 7-49). 33 Construct validity has been established for the Dutch version of the CMAI, and reliability appears to be good for subscales and total scores. 33,34 Emotional distress caused by challenging behavior was measured by an expansion of the CMAI based on the burden scale of the Neuropsychiatric Inventory, the NPI-D. 35 For each CMAI item rated above score 1 (“never”), the caregiver rated the extent to which they were able to manage the behavior on a 5-point Likert scale, with a higher score indicating higher ability to manage the behavior. Per caregiver, an average coping-with-behavior score was calculated, ranging from 1 (very unable to cope) to 4 (very able to cope).
Analyses
Analysis of interviews
The interviews were transcribed verbatim and analyzed using Atlas.ti, version 7.1, applying inductive content analysis. One researcher (D.v.V.) derived codes and categories from the data. Codes that were related through meaning or content were grouped into categories and discussed with 2 researchers (V.W. and D.L.G.), thereby reaching consensus on the themes that represent the experiences of the caregivers with VFH.
Analysis of questionnaires
The differences between pre- and postassessment for the PANAS, SCQ, and CMAI were calculated by subtracting the score obtained before the intervention from the score obtained afterward. This was done for each subscale and total score, and for the total score on the Emotional Distress Scale. Wilcoxon signed ranks tests were performed to test for statistically significant differences, using the Statistical Package for the Social Sciences, version 20. Given the explorative nature of the pilot study and the small sample size, the results of the tests are presented using an uncorrected significance level of P < .05.
Pilot Process Evaluation
Design and procedure
For the process evaluation, information was collected on possible barriers to using or participating in the VFH program and on recommendations for overcoming these barriers. The procedures for each informant group were as follows:
Participating caregivers
The caregivers in the pilot effect study were asked about their considerations with respect to participating, possible barriers to participating, and beliefs on and recommendations for overcoming these barriers in a semistructured interview.
Caregivers who declined
A group of caregivers (N = 18) attending 2 support groups were informed about the intervention, but chose not to participate. They subsequently participated in a questionnaire that included open and closed questions about considerations for refusal, appropriateness of the intervention, possible barriers, and recommendations for overcoming these barriers.
Stakeholders
Stakeholders of the organizations involved (3 VF trainers, 2 managers, and the coordinator of a VF expertise center) were given a questionnaire and participated in an evaluation meeting halfway through and at the end of the project. These meetings were about beliefs on using video in interventions, appropriateness of the intervention, and potential or encountered barriers.
Field experts
The VF experts (N = 50) and health-care professionals who were initially contacted for referrals (N = 100) were asked to participate in a survey that was developed on the basis of the results obtained from the caregivers and stakeholders. The survey included the potential barriers that were identified by the caregivers and stakeholders, which were rated on a 5-point scale to investigate the extent to which these factors were actually perceived as a barrier in clinical practice. Open-ended questions were included to determine the appropriateness of the intervention, additional barriers, and recommendations for overcoming these barriers.
Analyses
The potential barriers and recommendations were extracted from the various information sources. Percentages were calculated for each of the barriers that were rated on a 5-point scale on the survey data.
Ethical considerations
The official local medical ethics review committee “CMO Regio Arnhem-Nijmegen” reviewed the study protocol (http://www.ccmo.nl/nl/erkende-metc-s/cmo-regio-arnhem-nijmegen) and declared that formal approval in accordance with the Dutch Medical Research Involving Human Subjects Act was not necessary (2012/485). The management boards of participating care organizations gave permission for the study, which was conducted in accordance with the Declaration of Helsinki (https://www.wma.net//declaration-of-helsinki) and the Code of Conduct for Health Research (version 2005; https://www.federa.org/federa-english) as well as the rules that apply in the Netherlands.
Results
Pilot Effect Study
Sample characteristics
Fifteen dyads were included in the study. However, 5 cancelled their participation before or just after the start of the intervention for the following reasons: the behavior had suddenly become less challenging (1), the person with dementia was admitted to a nursing home (2), the person with dementia died (1), or withdrawal without explanation (1).
Table 1 shows the characteristics of the remaining 10 dyads. Of the 10 people with dementia who participated, the mean age was 80.1 years and 6 were male. The dementia diagnoses included Alzheimer’s (1), mixed Alzheimer-vascular (2), vascular (3), frontotemporal dementia (1), Huntington (1), and unspecified (2). On average, the participants had been diagnosed with dementia 4.4 years ago. All had been employed: 4 in production, 1 in management, 1 in housekeeping, 1 as a kindergarten teacher, and 2 had been self-employed.
Sample Characteristics.
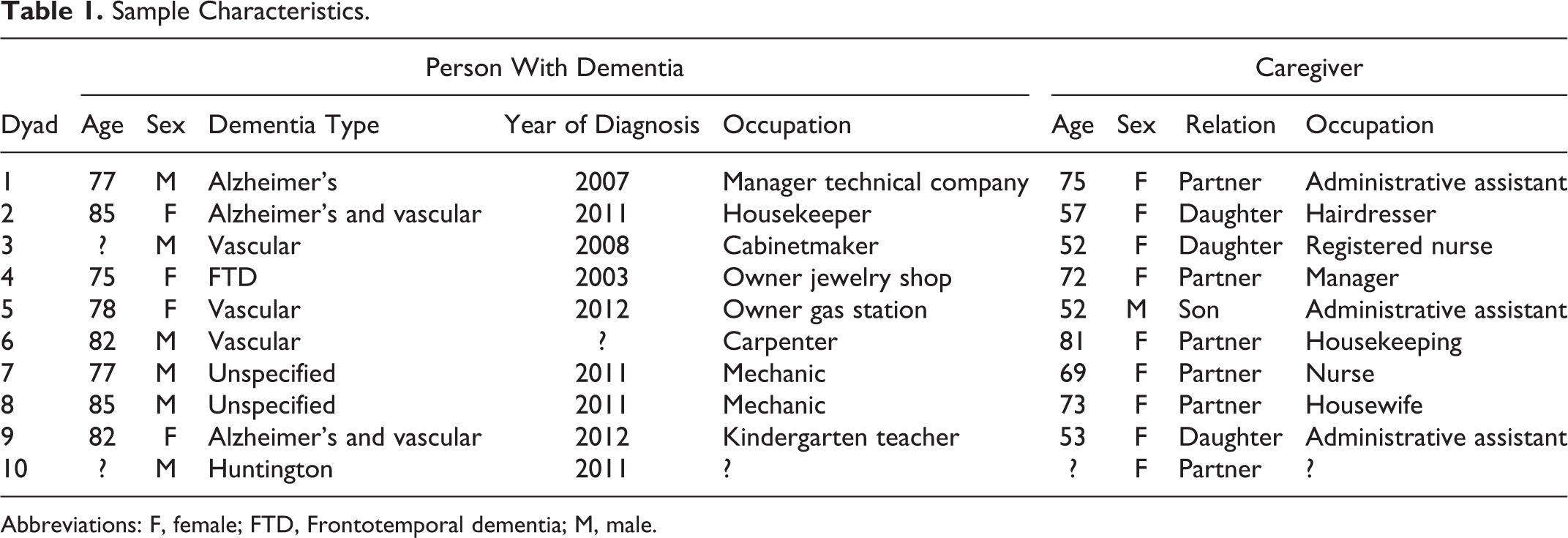
Abbreviations: F, female; FTD, Frontotemporal dementia; M, male.
Nine of the caregivers were women. In 4 cases, the person with dementia was the parent of the caregiver; in 6, they were the partner. The mean age of the caregivers was 64.9 years. All but 1 were or had been employed: 3 in administration, 1 in management, 1 in housekeeping, 1 as a hairdresser, and 2 as a nurse.
Of these 10 dyads, 1 dropped out of the study after the first VFH session because the care for the person with dementia was transferred to another family member. Another caregiver decided to participate in the study after the first VFH session so that the preassessment was missing. In addition, one caregiver agreed to a semistructured interview and the use of the video footage, but did not wish to participate in the questionnaires. This left data on education and occupation for 8 dyads, interview data for 9 caregivers, and 7 pre/postassessments.
The specific requests for help of the caregivers were questions about how to manage (particular) challenging behavior of the person with dementia (n = 6), requiring tools for communication (n = 2), requiring insight into their own behavior (n = 1), and the request for help from the dyad who dropped out was missing. The number of video recordings per dyad was 1 for the dyad that dropped out after the first VFH session, 2 for 3 dyads, 3 for 4 dyads, and 4 recordings for 2 dyads.
Self-efficacy and burden of informal caregivers
Semistructured interviews
All 8 caregivers reported positive experiences with VFH. The themes resulting from the qualitative analyses on the experiences of caregivers with VFH were insight, acceptance, coping, confidence, peace, and contact. Caregivers indicated that the VFH program provided them with insight into their own behavior (and responses) as well as the behavior of the person with dementia. Some caregivers reported an increased ability to see the causes of particular behavior of the person with dementia and understand their experience. For caregivers, it was also important to see what they could do to change their responses. Seeing the video images was highly valued in this respect. Having more insight also led some caregivers to increased acceptance of the changes in the person with dementia, their limitations, and the loss of an equal relationship. Caregivers mentioned several communication strategies that helped them cope with the communication problems, such as attracting attention, tolerating silence, supporting messages with visual information, and repetition. Furthermore, most caregivers indicated they felt more confident as a result of the VFH program. They reported reduced feelings of guilt and being able to manage certain situations. Most caregivers reported highly appreciating that the VFH program was especially focused on providing positive feedback, which they had not expected. This was considered important and gave them a sense of confidence. In addition, several caregivers reported they experienced more peace within themselves and some in their family member with dementia. The caregivers reacted with more patience and less irritability, for example. The feeling of connectedness between the caregiver and the person with dementia was also considered to have improved in some cases. Caregivers experienced better contact, more affection, more pleasant conversations, and fewer difficult discussions, among others.
Questionnaires
The PANAS showed mixed, statistically nonsignificant results. An overall decrease in negative affect was observed, as well as a decrease in positive affect. Sense of competence increased in all caregivers, with a significant difference in total score before and after the VFH program (Z = −2.201, P = .028). This difference was also significant for both subscales: satisfaction about the person with dementia as care recipient (Z = −2.023, P = .043) and satisfaction about self as caregiver (Z = −2.120, P = .034). The extent to which the caregiver felt able to cope with problem behavior increased in most caregivers, but the differences were not statistically significant (see Table 2).
Sense of Competence: Total Scores and Scores on the 2 Subscales of the SCQ and the Extent to Which the Caregiver Feels Able to Cope With Problem Behavior (Subscale Cohen-Mansfield Agitation Index) Before (T1) and After (T2) the VFH Program and the Difference Scores (Diff) Between T2 and T1.a
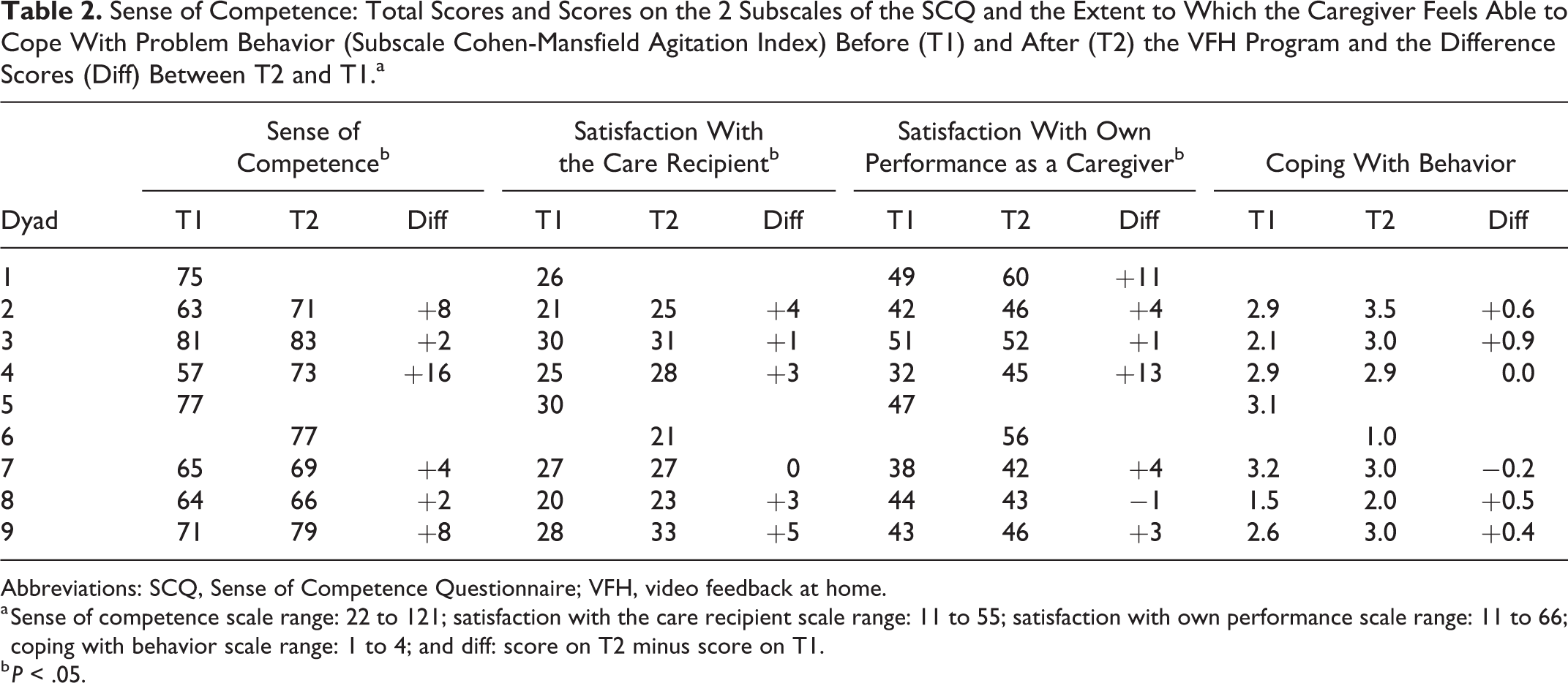
Abbreviations: SCQ, Sense of Competence Questionnaire; VFH, video feedback at home.
a Sense of competence scale range: 22 to 121; satisfaction with the care recipient scale range: 11 to 55; satisfaction with own performance scale range: 11 to 66; coping with behavior scale range: 1 to 4; and diff: score on T2 minus score on T1.
b P < .05.
Number and intensity of challenging behaviors
Challenging behavior as measured by the CMAI decreased in all but one participant (Z = −2.023, P = .043). Of the subscales of physical aggression, verbal agitation, and restlessness, restlessness showed a significant decrease (Z = −2.041, P = .041; see Table 3).
Challenging Behavior as Measured With the CMAI (Cohen-Mansfield Agitation Index) and Its 3 Subscales Before (T1) and After (T2) the VFH Program and the Difference (Diff) Between T2 and T1.a
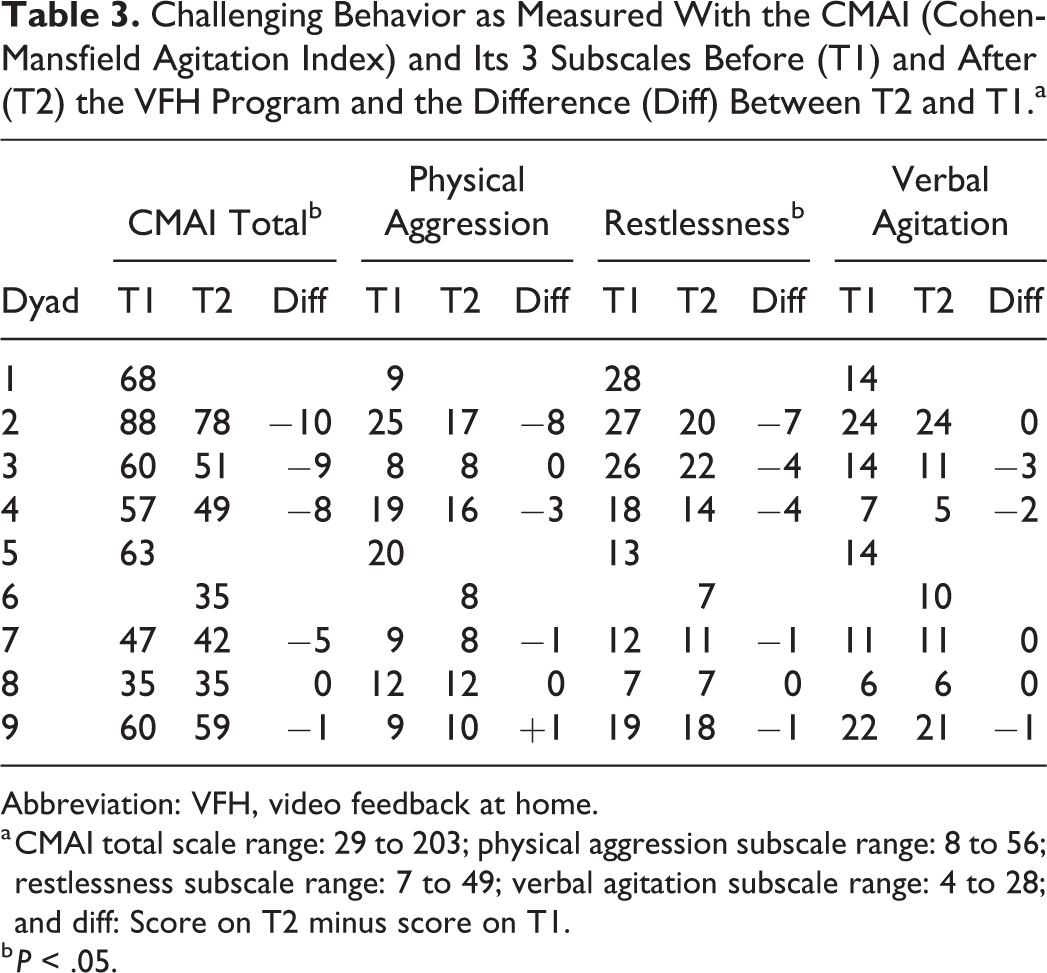
Abbreviation: VFH, video feedback at home.
a CMAI total scale range: 29 to 203; physical aggression subscale range: 8 to 56; restlessness subscale range: 7 to 49; verbal agitation subscale range: 4 to 28; and diff: Score on T2 minus score on T1.
b P < .05.
Pilot Process Evaluation
Appropriateness of the intervention
Participating caregivers
All caregivers reported positive experiences with VFH after the intervention and found the intervention helpful in a variety of ways.
Caregivers who declined
Of the 18 caregivers, 10 were positive about the intervention and the information received, 3 were negative, and 5 neutral. Negative responses reflected not wanting to be videotaped or not needing help. Half of the caregivers could imagine using VFH in the future, yet most indicated they would postpone it until they were no longer able to cope or make contact with the person with dementia.
Stakeholders
All stakeholders believed VF to be an appropriate intervention for caregivers. The stakeholders mentioned that, in their experience, potential referrers (case managers, day care facilities, general practitioners, psychologists, and home care organizations) responded positively to the intervention.
Field experts
We received 55 responses (17 VF trainers and 38 referrers) in the survey among field experts (N = 150). Of these, 89% felt VF was an appropriate intervention to conduct in the home environment. They indicated that caregivers may gain insights into problems and learn how to improve communication. Watching what happens through video was considered a useful tool for clarifying matters. They further mentioned that the method is especially useful nowadays given that people with dementia remain at home longer. The reasons reported for making referrals were challenging behavior, conflicts, low level of knowledge of the caregiver about dementia or about ways in which to approach the person with dementia, high caregiver burden, and low sense of competence of the caregiver. Three respondents indicated VFH was not an appropriate intervention but provided no explanation.
Potential barriers
Potential barriers spontaneously mentioned and/or rated in a questionnaire by the various informants are shown in Table 4. Of the field experts, 69% indicated experiencing problems regarding the use or referral of VFH. In the survey, field experts had been asked to rate 9 possible barriers for caregivers. For each barrier, responses were missing in 11 to 17 cases. The highest barriers for caregivers according to these professionals (50% or more perceived a particular barrier as high) were being unfamiliar with VFH, the camera being perceived as threatening, caregivers believing they act differently in front of the camera, caregivers being afraid to be confronted with mistakes, and caregivers perceiving an unfamiliar person as threatening (Figure 1). Barriers for referrers themselves in referring people for a VFH program were obtaining funding, the possibility of VFH not occurring to them, not being sufficiently familiar with the intervention, and seeing no benefits: Levels of substantial or major barrier were 18%, 23%, 20%, and 13%, respectively. For the caregivers who declined the intervention, the highest scoring barriers were that it was “too early,” or their problems were not severe enough for the intervention to be necessary, or they felt they would not benefit from the intervention.
Potential Barriers for Participating in or Using a VFH Program According to Caregivers, Stakeholders, and Field Experts.
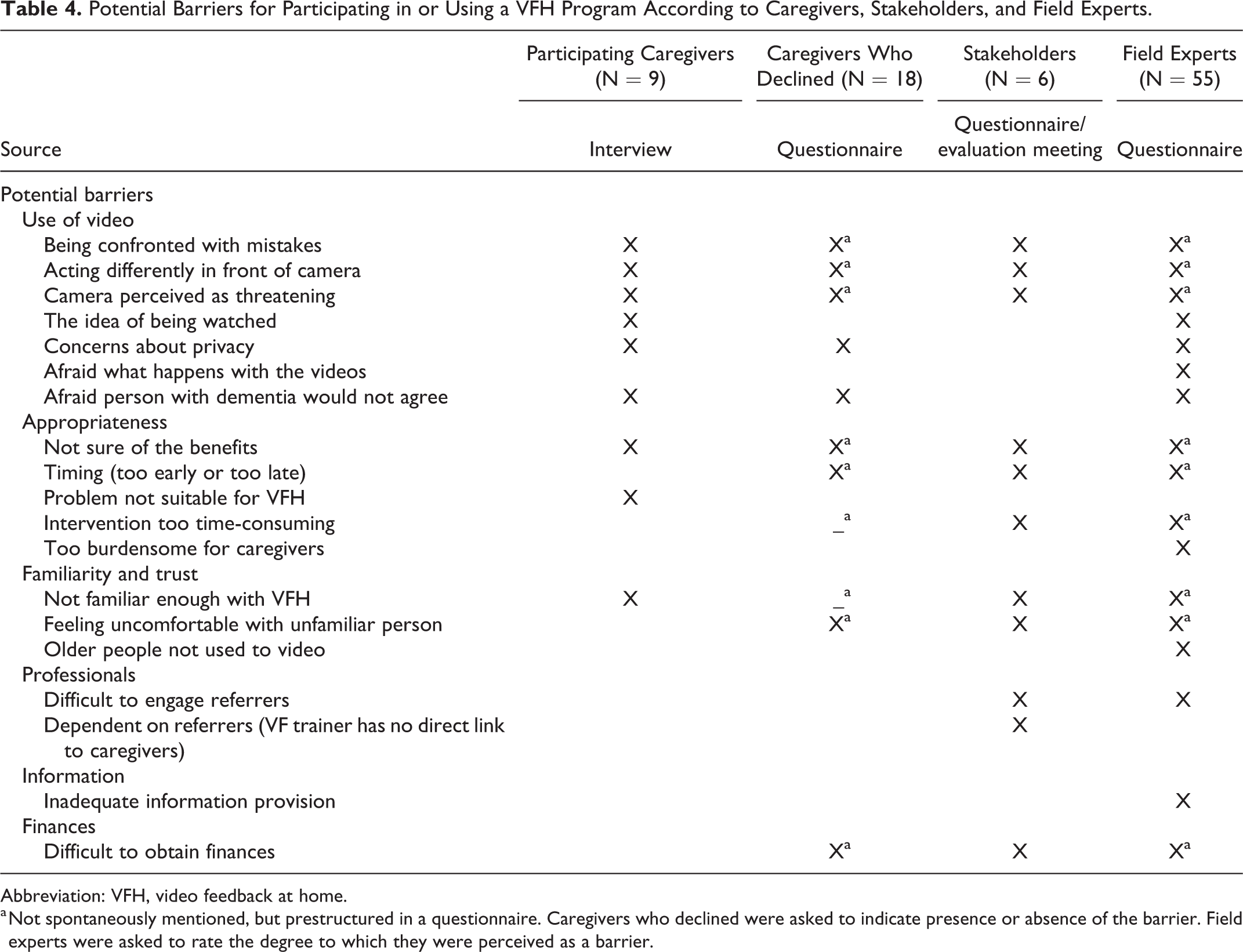
Abbreviation: VFH, video feedback at home.
a Not spontaneously mentioned, but prestructured in a questionnaire. Caregivers who declined were asked to indicate presence or absence of the barrier. Field experts were asked to rate the degree to which they were perceived as a barrier.
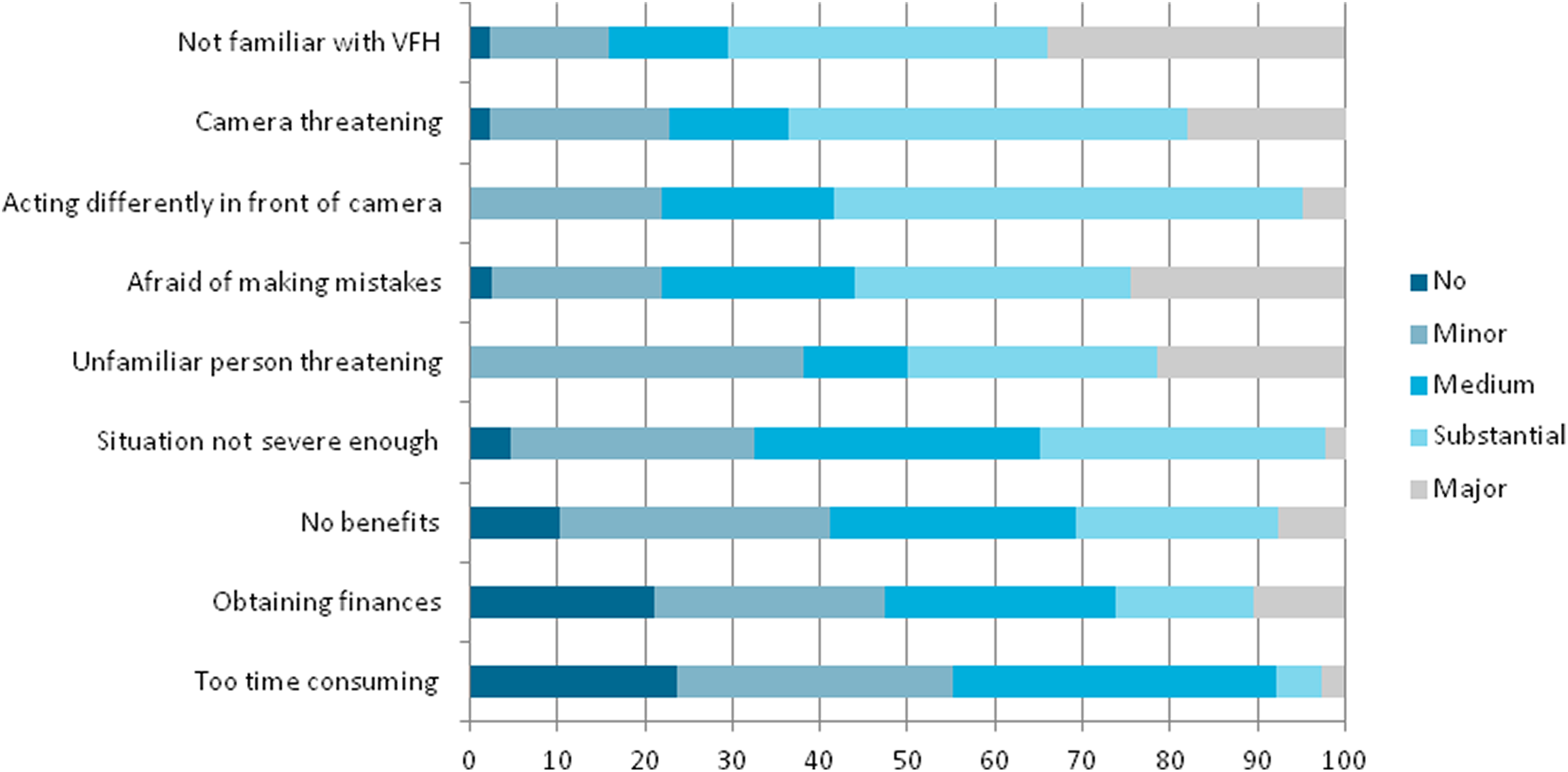
Degree to which potential barriers for caregivers into participating in VFH are perceived as a barrier by health-care professionals, divided into no, minor, medium, substantial, and major barriers. VFH indicates video feedback at home.
Recommendations mentioned
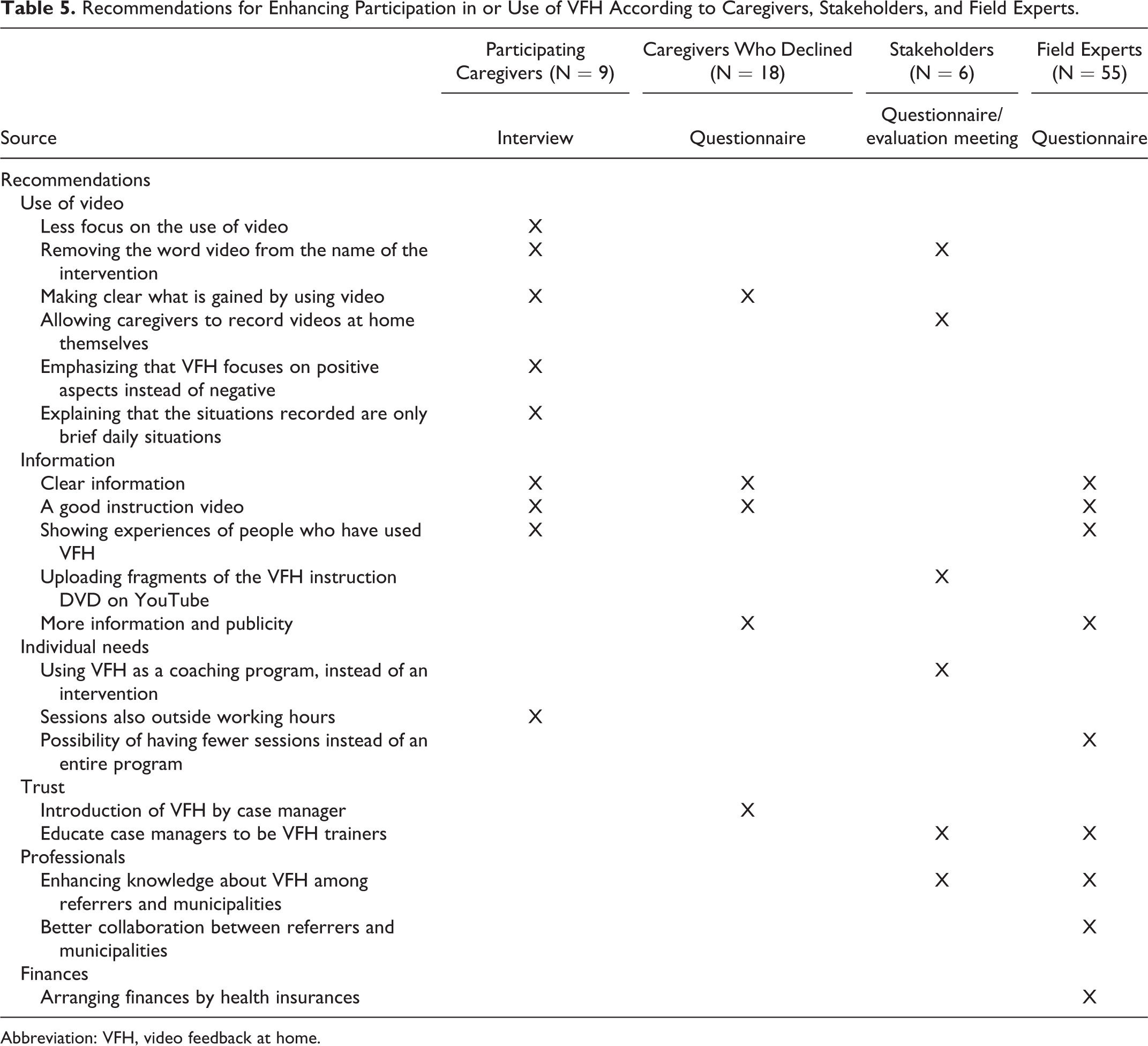
The recommendations for enhancing the application of VFH as made by the different informants are shown in Table 5. Most recommendations focused on the reluctance toward being filmed and providing adequate information. Caregivers predominantly made recommendations regarding the use of video, while professionals’ recommendations focused more on enhancing knowledge, gaining trust, and arranging finances.
Recommendations for Enhancing Participation in or Use of VFH According to Caregivers, Stakeholders, and Field Experts.
Abbreviation: VFH, video feedback at home.
Discussion
This feasibility study into the use of VFH in dementia care shows, despite the small sample size, that caregivers were highly satisfied with the intervention and experienced many benefits in terms of insights, acceptance, coping and self-confidence, and a sense of peace and connection with the person with dementia. Specific aspects of the intervention were positively rated by the caregivers, that is, watching the videos, which provided insight into their behavior, and receiving positive feedback, which increased their confidence. The results from the quantitative measures concerning sense of competence, burden, and behavior imply that it might well be possible to demonstrate the effects of VHF in a larger study using these measures. The main barriers to participating in a VFH program according to caregivers as well as health-care professionals appeared to be reluctance toward being video recorded as well as not being familiar with the method. The most important recommendations, therefore, were aimed at these barriers and enhancing knowledge about VFH.
Our results are in line with the positive effects found in previous studies on enhancing communication, where training the (informal) caregiver in using facilitating communication strategies had a positive effect on the person with dementia, the caregiver, and the dyad’s relationship. 9,17 –19 Furthermore, the results correspond to previous studies that applied VF. 11,20,21
Contrary to expectations, it was impossible to recruit the planned 25 VFH dyads. An earlier feasibility study on in-home video recording to support dementia caregivers indicated that caregivers may hesitate to video record the person with dementia because of privacy issues. 21 However, acceptability of the intervention is high in child care. 36 In addition to a high degree of familiarity with VF in child care, certain inherent differences such as age may help to explain this. Older people may, for example, be more reluctant to use technological methods. 21 Furthermore, interventions aimed at improving interaction may be more acceptable to young parents having to learn a new parenting role, as opposed to caregivers slowly evolving into a caregiver role, who may have known the person with dementia for a long time. Finally, caregivers of people with dementia may shy away from showing their private situation to others, because of the vulnerability of their relative and the persisting taboo on dementia.
One limitation of this feasibility study is that the number and profiles of people who were contacted during the recruitment period and declined to participate are not known, as the researchers were not in direct contact with potential referrers. This information could have provided insights into subgroups of caregivers and people with dementia for whom the intervention might be suitable or unsuitable. We used broad inclusion criteria in our relatively small study, and at the moment, it is not yet appropriate to specify these. The barriers experienced (eg, reluctance toward using video and unfamiliar intervention) can be addressed with implementation strategies, which should be explored before limiting the group for whom the intervention is considered usable. Future studies should address this issue. The response rate of the field experts in the survey was also relatively low, making the results inconclusive.
Despite these limitations, we believe this feasibility study is a significant contribution to the field of intervention studies in dementia care, given the combined use of quantitative measures, qualitative interviews with participants, and a process evaluation among a broad palette of relevant informant groups. The intervention may have excellent potential for supporting specific groups of caregivers, for example, caregivers of people with young-onset dementia or home care nurses. In the future, the role of the persons with dementia themselves requires attention. For instance, given recent insights into the learning abilities of people with dementia, 37 they might take a more active role in the intervention. Furthermore, addressing the timing of the intervention is relevant. Half of the caregivers who declined reported they might use the intervention in the future, for instance, if they were “no longer able to cope.” Nevertheless, the dropout level during the pilot study was very high and probably partly a result of inadequate timing; 2 dyads dropped out because the person with dementia was admitted to a nursing home as the caregiver was no longer able to provide care at home and 1 dyad because the person with dementia died (3/5 cancellations). Implementation strategies in daily practice and recruitment strategies for an effect study may thus wish to focus on including dyads at an earlier stage and on formulating more specific inclusion criteria.
The barrier regarding reluctance toward using video could be lowered by, for example, focusing less on the use of video, changing the name of the intervention, and enhancing knowledge about VFH among referrers and municipalities by providing adequate information and increasing publicity. Additionally, VFH could be part of case management trajectories for people with dementia by trained case managers. This would also enable starting VFH at an earlier stage, thereby possibly extending the perseverance time of the caregivers. 38 It is only when the barriers to the use of VFH are overcome by using these practical implementation guidelines that a large randomized effectiveness study—which is necessary to provide evidence on the usefulness of VFH—will be feasible.
Footnotes
Authors’ Note
All authors participated in the study’s concept and design. D.v.V. and V.W. conducted the data collection and analyses. D.v.V. wrote the draft paper, while D.G. wrote the final paper. D.G. and R.K. supervised the data collection and analyses. V.W. and R.K. contributed to writing the paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dutch Alzheimer’s Society under grant number WE03.2011-20.