
Abstract
Objectives:
Examine the effects of a 6-month exercise intervention on neuropsychiatric symptoms, pain, and medication consumption in older people with dementia (PWD) living in nursing homes (NH).
Methods:
Ninety-one older PWD living in NH performed a 6-month structured exercise intervention (n = 44) or a social activity intervention (n = 47). Neuropsychiatric symptoms were measured by the neuropsychiatric inventory (NPI), pain was assessed using the Algoplus scale, and dementia-related drug prescriptions were obtained for all participants.
Results:
Between-group analysis found a nonsignificant difference that could be of clinical relevance: a 4-point difference in the NPI and 1.3-point difference in the reduction of the number of medications favoring exercisers. No significant differences were found for pain, and a trend was found for an increase in medication consumption in the social group.
Conclusion:
Exercise effects did not differ from social intervention effects on neuropsychiatric symptoms, pain, and medication consumption in older PWD living in NH.
Introduction
Behavioral and psychological symptoms of dementia (BPSD) as well as pain are common in older people with dementia (PWD). 1 Psychotropic drugs are often prescribed to deal with such burdensome symptoms in PWD but they increase the risk of adverse health events, 2 including death, 3 particularly in the nursing home (NH) setting. Indeed, around 50% of NH residents have dementia, and they are characterized by polypathology, polypharmacy, and high prevalence of psychotropic drug use, notably benzodiazepines and antipsychotics. 4,5 Therefore, nonpharmacological interventions make part of the frontline treatment of neuropsychiatric symptoms, and they have the potential to decrease medication consumption in PWD. A meta-analysis published from our group showed that there were no benefits from exercise for reducing BPSD in PWD. However, the authors report that heterogeneity was high, and only 4 studies had available data on BPSD. Recently, a 2-week exercise intervention in PWD in hospital care showed that it can significantly decrease BPSD. Nevertheless, data on the effects of exercise on BPSD in PWD are scarce and still remains trivial.
Pain is a common condition in older PWD, and it is frequently undertreated. 6 The appearance of pain is mostly produced by the musculoskeletal system 7 and rarely occurs in the absence of other diseases. 8 Consequently, higher pain perception is related to decreased physical function and quality of life. 9 In PWD, pain is often undertreated because of the difficulty of PWD to communicate and is often complex to ascertain since they experience pain differently. 10 The prevalence of pain is different between various subtypes of dementia. For example, one study showed that people with vascular dementia report higher pain experience than those with Alzheimer’s Disease. 11 The treatment of pain has been shown to reduce neuropsychiatric symptoms in patients with dementia, 12 suggesting that treating pain has broader effects on health in PWD. Exercise has been shown as an efficient strategy to decrease pain in a majority of individuals, such as fibromyalgia and healthy individuals. 13 However, it is still inconclusive whether exercise can decrease pain in PWD living in NHs.
Nevertheless, exercise is known to improve overall health and physical fitness in various populations, 14,15 including PWD. 16 Although a recent meta-analysis undertaken by our team 17 found that exercise training reduces depressive symptoms in PWD (including institutionalized people), its benefits for the global levels of BPSD and for the other specific BPSDs are still mixed. Moreover, the effects of exercise on pain, which remains an underdiagnosed condition in PWD, 18 are still unknown, and its potential benefits for reducing harmful drug consumption has, to the best of our knowledge, never been investigated.
The objective of this cluster randomized controlled trial (RCT) was to compare the effects of a 6-month exercise intervention with a 6-month social (nonphysical) intervention on BPSD, pain, and medication consumption in older PWD living in NHs.
Methods
The methods and procedures of LEDEN have been published in detail elsewhere. 19 In brief, LEDEN was a 24-week pilot cluster RCT that compared the effects of a group-based exercise intervention to those of group-based social intervention on activities of daily living (ADL) in NH residents with dementia. 20 The main results of LEDEN showed no difference in the effects of exercise compared to the effects of social activities on ADL performance. 20 In this study, we analyzed the secondary outcomes of LEDEN: BPSD, pain, and medications. The ethics committee approved the study protocol (Comité de Protection des Personnes - Sud Ouest et Outre-Mer III [CPP SOOM III]), which was registered in a clinical trial registry (registration NCT02444078). Participants (if applicable), next of kin, and legal representatives signed an informed consent form, as appropriate, before baseline assessments.
Participants
Participants were included in the study if they were diagnosed with Alzheimer’s Disease or vascular or mixed dementia according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV); a Mini-Mental State Examination (MMSE) score of 20 or less; aged 65 and older; living in the NH for at least 1 month; ability to walk 4 meters; and to rise from a chair without human assistance. Exclusion criteria were terminal illness (life expectancy <6 months), Parkinson’s disease or dementia with Lewy bodies, unstable condition before the exercise intervention, and physically active (participation of another exercise program for >2 times a week for more than 2 months). Ninety-seven patients were finally included, but only 91 had at least 1 postbaseline assessment of outcome measure. These 91 individuals compose our study sample, with 44 people living in NHs being randomized to structured exercise intervention and 47 to the social activity group. Figure 1 illustrates the flowchart of the study participants.
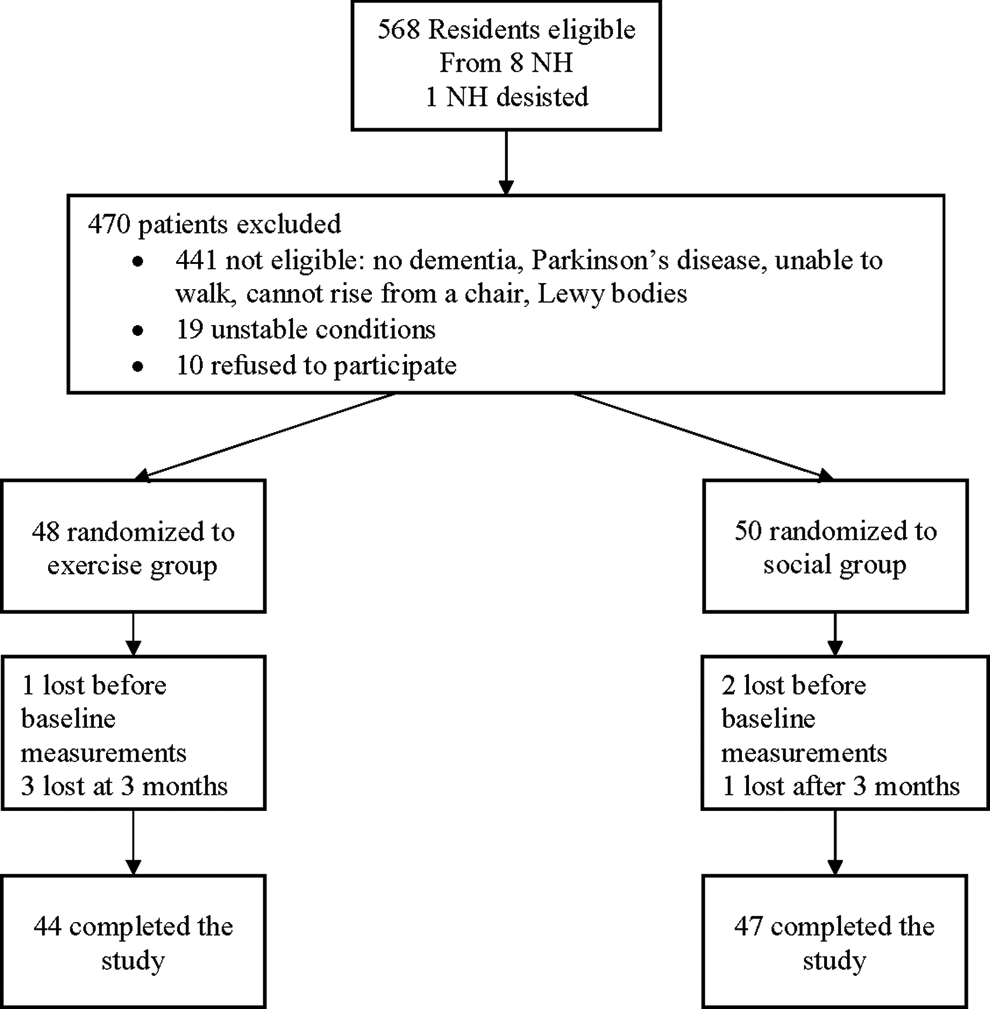
Flowchart of study patients. NH indicates nursing home.
Randomization
LEDEN is a 2-arm pilot cluster RCT with NHs as the unit of randomization and were randomized in a ratio of 1:1. To assure masking, the randomization was performed by a statistician blinded to NH identity and not involved in any other aspect of LEDEN. Group allotment was stratified using the median value of dementia prevalence in the NHs and was performed using random permuted block sizes of 2 within each of the 2 strata. Group allocation concealment was guaranteed using opaque, sealed envelopes until group assignment was revealed to the NHs.
Interventions
Exercise
Supervised, group-based activities took place in the NHs twice per week, for 60 minutes, during 24 weeks. The exercise program was a multicomponent training led by exercise instructors (3-year University diploma on exercise), with warm-up, coordination and balance exercises, muscle strengthening, aerobic exercise, and cool-down. Exercise intensity was targeted to be moderate. Progression was based individually, and participants were regularly encouraged to improve their performance in the absence of pain or breathlessness. This intervention has been proposed to improve health in PWD living in NH. 21
Social activity group
Supervised, group-based nonphysical activities took place in the NHs twice per week, for 60 minutes, for 24 weeks. The selected interventions were new activities for the residents. Social activity instructors, who were external to the NHs, performed either music meditation (eg, relaxation, playing percussion instruments, and singing) or arts and crafts (eg, painting and drawing alone and in pairs, and clay modeling).
Outcome Measures
Neuropsychiatric symptoms
The frequency and severity of neuropsychiatric symptoms were measured at baseline and 6 months (postintervention) using the neuropsychiatric inventory-NH version (NPI-NH). The NPI is a valid questionnaire 22 investigating 10 different behavioral and 2 neurovegetative areas; with scores that vary from 0 to 12 for each item, with higher scores indicating higher behavioral disturbances. The total NPI score is obtained by adding the scores of the 10 behavioral areas, with scores varying from 0 to 120; we also performed a secondary analysis by adding the 2 neurovegetative items to the 10 behavioral items, with total scores varying from 0 to 144.
Pain
Pain was measured at baseline and 6 months (postintervention) using the Algoplus tool, a scale specifically developed for assessing pain in older people who are unable to communicate verbally. 23 This scale contains 5 items which are scored as 0 (absence of pain) or 1 (presence of pain); the total score varies from 0 to 5, with higher scores indicating higher pain.
Medication
Data on each medication were collected at baseline, 3, and 6 months (the NH medical staff sent to the research team drug prescription for each patient in the week of outcome assessments) and was coded according to the Anatomical Therapeutic Chemical/Defined Daily Dose (ATC/DDD) index; 24 we have already used these procedures successfully in another clinical trial we developed previously. 25 For this article, the following drugs were coded: antipsychotics (N05A), benzodiazepines (N05BA, N05CD, N05CF, N03AE, and M03BX07), analgesics (N02), and antidepressants (N06A). For each medication, we created a binary variable (0 = not taking medication, 1 = taking medication). For a more thorough analysis on medications, we summed total medication consumption for each participant at baseline, 3, and 6 months.
Statistical Analysis
LEDEN was a pilot study performed to inform the development of a larger, well-powered study; no formal sample size calculation was performed. Descriptive statistics used mean (SD) and absolute numbers and percentages. Efficacy analysis was undertaken using a modified intent-to-treat (ITTmod) approach excluding people with no postbaseline endpoint assessments as pre-planned in the LEDEN protocol. 19 Multilevel analysis was performed on NPI, total medication consumption, and pain using a 3-level (with random effects at the levels of NH and participants [participants nested into NHs] and a random slope on time) regression model with group, time, and group by time interaction as fixed effects. Models were adjusted (fixed effect) for the variable used to stratify randomization (prevalence of dementia in NH) and for potential cofounders that differed between groups at baseline.
To examine the effects of exercise on the binary medication variables, we used generalized estimating equations (GEEs). Separated models were performed for analgesics, benzodiazepines, antidepressants, and antipsychotics. Covariates were NPI, sex, and nutritional status (variables that differed between groups at baseline). Since the outcomes were dichotomous, the link function was specified as logistic. The working correlation structure for the repeated measurements of the outcome variable was specified as unstructured.
Results
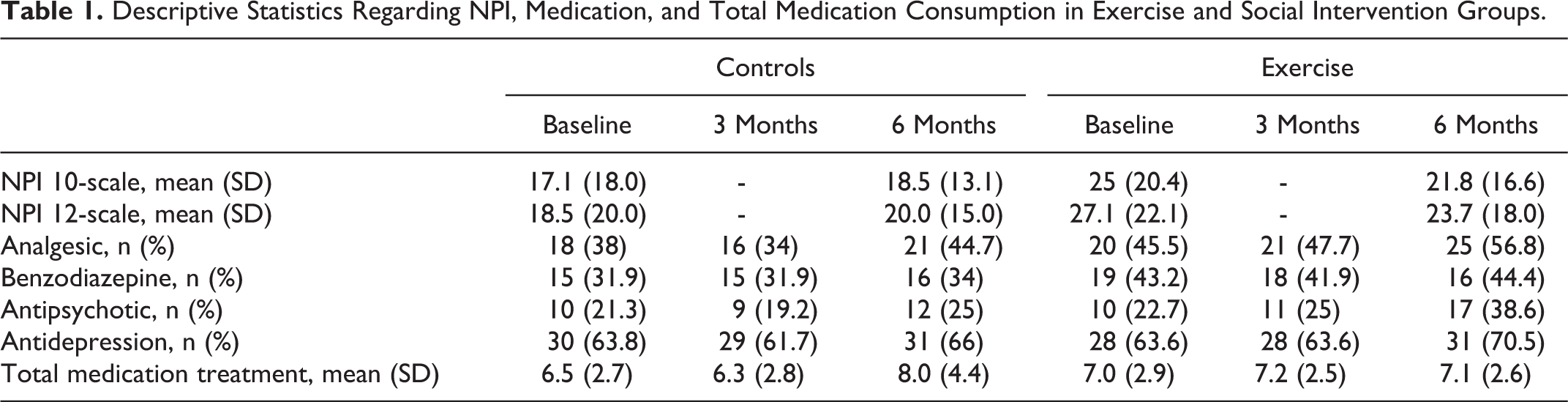
Baseline data from the LEDEN study are published elsewhere. 20 In short, there was a significantly higher prevalence of women in both groups. Descriptive statistics regarding NPI scores and medication consumption are presented in Table 1. The baseline NPI scores were significantly higher in the Exercise group. No significant differences were found in medication consumption in both groups at baseline. Multilevel models adjusted for confounders are shown in Table 2. The group-by-time interaction was not significant for both NPI and pain, indicating that the effects of exercise did not differ from the effects of the social activities. Although not statistically significant, there was a 4-point decrease on BPSD in the exercise group compared to the social activity group, representing a clinically meaningful reduction for the NPI scale. Interestingly, total medication consumption tended to be higher after the 6-month social group intervention (1.26-point increase, P = .056).
Descriptive Statistics Regarding NPI, Medication, and Total Medication Consumption in Exercise and Social Intervention Groups.
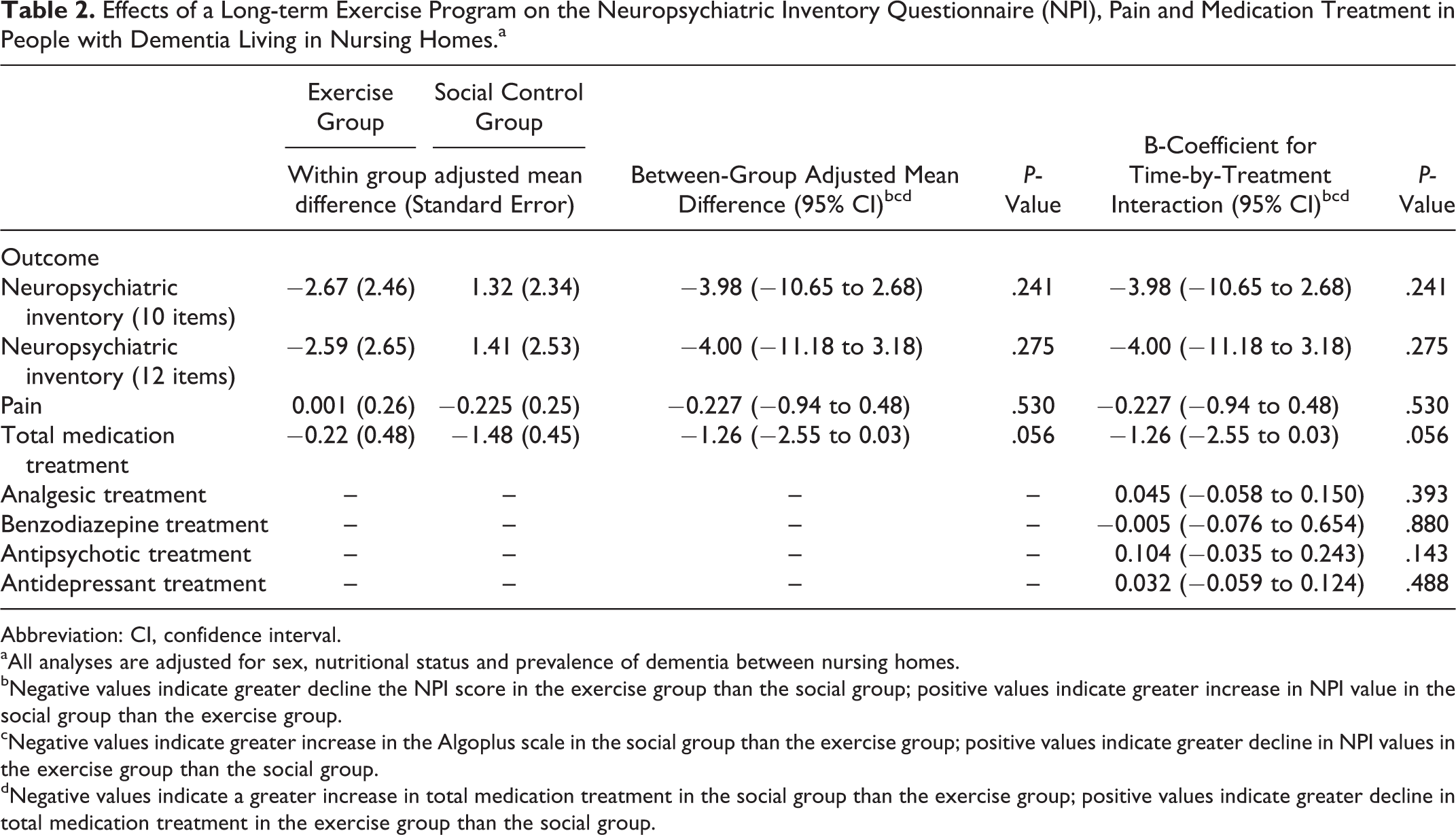
Effects of a Long-term Exercise Program on the Neuropsychiatric Inventory Questionnaire (NPI), Pain and Medication Treatment in People with Dementia Living in Nursing Homes.a
Abbreviation: CI, confidence interval.
aAll analyses are adjusted for sex, nutritional status and prevalence of dementia between nursing homes.
bNegative values indicate greater decline the NPI score in the exercise group than the social group; positive values indicate greater increase in NPI value in the social group than the exercise group.
cNegative values indicate greater increase in the Algoplus scale in the social group than the exercise group; positive values indicate greater decline in NPI values in the exercise group than the social group.
dNegative values indicate a greater increase in total medication treatment in the social group than the exercise group; positive values indicate greater decline in total medication treatment in the exercise group than the social group.
The results of the GEE analysis on medications found no significant differences between the groups on the use of all of antipsychotics, antidepressants, benzodiazepines, and analgesics (Table 2).
Discussion
This work showed that a 24-week exercise intervention, compared to a social activity intervention, and had no statistically significant effects on neuropsychiatric symptoms, pain, and medication consumption in PWDs living in NHs.
A previous report from our team 26 has found positive effects of a 12-month exercise training on ADL performance but has failed to demonstrate any effects on BPSD in people with Alzheimer’s Disease. However, that study employed a no-intervention control group (usual care), differing from the social activity group employed in LEDEN; it is plausible to think that a social intervention could bring about more benefits on BPSD than no intervention, rendering it more difficult to show a positive effect of the exercise intervention in LEDEN. In another RCT, Telenius et al 27 indicated a significant decrease in neuropsychiatric symptoms after a 12-week, high-intensity resistance training program. The participants in their study performed the High Intensity Functional Exercises (HIFE) intervention, developed by Littbrand et al. 28 The HIFE exercise protocol includes resistance training with an intensity set at 12-repetition maximum per set and “challenging” balance tasks. Participants undertook these sessions twice a week, 60 minutes per session. Although it is possible that vigorous exercise may further decrease neuropsychiatric symptoms, others have tested the HIFE protocol on BPSD in PWD and have not found significant effects. 29 The sole exercise RCT designed to decrease BPSD in PWD (having the NPI as the primary end point) found no significant effects of the intervention against usual care controls in a 12-week interval. 30 Although not statistically significant, the effects of LEDEN interventions favoring exercisers (reduction of about 4 points in the NPI scale) may be considered clinically relevant. Indeed, although no consensual cutoff for clinical meaningfulness exists for the NPI, experts indicate that such a cutoff would be around 3 or 4 points. 30,31 This is important, since this opens the perspective that a well-powered RCT may demonstrate a statistically significant effect of exercise on BPSD in institutionalized PWD, although such a hypothesis remains to be confirmed. Of note, the exercise group has had a nonsignificant increase in the use of antipsychotics during the intervention period, which could also have had an additive effect on the reduction of BPSD in this group. Therefore, future RCTs must pay attention to the potential bias caused by drug change during the intervention interval when examining the effects of nonpharmacological approaches on health outcomes in PWD. Regarding pain, caution must be taken in the interpretation of our findings, since pain levels were very low in our population, which may have led to a floor effect, rendering it difficult to show a benefit of the interventions for decreasing pain levels.
Furthermore, the results of this study indicate that our multicomponent exercise program performed twice weekly did not significantly change medication consumption, which is often related to BPSD, in elderly PWD living in NHs; however, the between-group difference of −1.2 drugs favoring the exercise group may be considered a clinically relevant information. Indeed, in very old institutionalized PWD, characterized by polypathology, it is very difficult to reduce medication. Moreover, NH culture and organization contribute to the maintenance of drug prescriptions in this population; for instance, we have previously shown that NH structure and internal organization (eg, number of beds, number of general practitioners in the NH, and presence of a pharmacy for internal usage) may be associated with psychotropic drug consumption. 32 Therefore, if exercise proves to be capable of reducing the total number of medications in a future, properly powered RCT, this will be a major finding for those who care for PWD living in NHs.
The strengths of our study are the medium-term exercise intervention, since most of the previous trials in institutionalized PWD lasted less than 16 weeks. The use of an active control group receiving a structured, nonphysical, group-based activity intervention, thus excluding the attention- and socialization-related bias that may be present in RCTs with usual care controls. The main limitations are the pilot design with no formal sample size calculation, the small sample size (which is, however, higher than the median recruitment for RCT in institutionalized PWD), 33 and the fact that the NH staff were the outcome assessors and, therefore, were unblinded to group assignment. The fact we did not distinguish dementia subtypes and did not undertake informative imaging data are also limitations, since the effects of an intervention may vary according to dementia subtype 34 ; however, subdividing our already small population would have certainly led to a reduced power. Also, although it is a strength of LEDEN compared to other studies in institutionalized PWD, the 6-month intervention may have been a relatively short time period to produce a substantial modification on the outcome measures. Participating NHs were private for-profit institutions belonging to the same company.
In conclusion, neuropsychiatric symptoms, pain levels, and medication consumption related to BPSD after a 6-month RCT did not differ between the exercise intervention group and the social activity group in PWD living in NHs. A nonstatistically significant, but probably clinically relevant, decrease in NPI was observed in the exercise intervention compared to the social group. A similar statistically nonsignificant but clinically meaningful pattern favoring exercisers was found regarding medication consumption, with the social intervention group increasing the number of drugs taken. A properly powered, larger RCT, with a longer intervention length, would inform whether exercise brings forth benefits to the health of PWD compared to social activities.
Footnotes
Authors’ Note
Both the sponsor and funding agencies of the LEDEN study had no role in the design of this study and will not have any role in the execution of the interventions, in the analyses and interpretation of the data, or in the decision to submit results. MM: Statistical analyses and article drafting, YR: study concept and design, interpretation of data, critical revision of article for important intellectual content. PEH, critical revision of article for important intellectual content. BV: interpretation of data, critical revision of article for important intellectual content. MC: interpretation of data, critical revision of article for important intellectual content. DA, PC and LR: critical revision of article for important intellectual content. PSB: study concept and design, interpretation of data and statistical analyses.
Acknowledgments
We would like to thank Arnaud Lendrieux (Direction de la Recherche et de l’Innovation, CHU-Toulouse) and Yasmine Messaoudi and Aude Letty (Institut du Bien Vieillir Korian) for their work, which contributed to the successful completion of the LEDEN study.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Armaingaud and Haÿ are both employees of the Korian group.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded FHT by the Caisse Nationale de Solidarité pour l’Autonomie (CNSA) (HPA-S4-03) in the call released by the Institut de la Recherche en Santé Publique (IReSP)in 2013 and by the Mission Recherche from the Direction de la Recherche, des Études, de l’Évaluation et des Statistiques (MiRE-DREES) (HPA-S4-03). The Centre Hospitalier Universitaire of Toulouse (CHU Toulouse) (14 7292 03) is the sponsor of this study.