
Abstract
Objectives:
Participation in group activities can benefit persons with dementia, alleviating boredom, improving affect, maintaining function, and decreasing problematic behaviors.
Methods:
We describe patterns of attendance of residents with dementia at nursing home activity groups and investigate stimulus and environmental factors that may affect attendance.
Results:
Residents participated in 60.8% of the activities, with reasons for nonattendance including refusal (9.7%), not being on the unit (7.8%), being asleep (6.8%), and being involved in activities of daily living and other activities (8.3%). On average, 3.5 other residents not recruited for the study chose to participate in each group session. Group attendance was significantly related to group topic.
Implication:
The need for activities was evident by the attendance of both invited and other residents. Understanding the factors that affect attendance is the first step toward developing procedures to maximize participation in activities in order to decrease loneliness and boredom in this population.
Background and Objectives
The provision of activities for persons with dementia in long-term care remains limited, and those activities that are offered are often inappropriate because they fail to take into account the functional capabilities or interests of the residents. 1 -3 Similar opinions have been voiced by residents themselves. 4 Buettner and Fitzsimmons 1 found that almost 45% of nursing home residents with dementia were offered few or no facility activities, 20% were presented with occasional activities, while 12% participated in activities on a daily basis, but these activities were not considered appropriate as they were not matched to resident needs. Residents on special care units fared the worst. This lack of available activities may contribute in part to observations that nursing home residents with dementia spend most of their time alone, immobile, and unoccupied. 5 -8 This inactivity can lead to loneliness and boredom, a decline in affect and function, and, ultimately, problematic behaviors. 5,9 -11
Alternately, participation in structured activities has many benefits for nursing home residents with dementia. Activities provide the opportunity to engage with meaningful stimuli, 12,13 which can help alleviate boredom, 14 improve affect and well-being, 8,15 -17 and decrease problematic behaviors. 5,18,19 Group activities have added value, as they provide opportunities for social interaction as well as meaningful engagement. 20
Studies investigating the effects of group activities on persons with dementia remain limited and have been concerned primarily with demonstrating the benefits for residents on outcome measures such as mood or behavior. 14,15,21,22 Studies are just beginning to look at factors that might affect engagement in group activities and may impact their utility in this population. 23,24
A framework for understanding influences on engagement of persons with dementia in group activity settings is presented by the Conceptual Process Model of Group Engagement [GOME 25 ]. This model posits that a participant’s engagement with a group can be affected by characteristics of the (1) person—for example, demographics, cognitive and functional level, sensory abilities, and preference for group activities; (2) stimulus—for example, activity content; and (3) environment—for example, location of activity, time of day as well as by characteristics of the group itself, including group size, cognitive level of group participants, and participant behavior.
Studies based on this model found level of cognitive function to be the most important personal characteristic influencing engagement. 23,24 Other personal variables, including impairment in activities of daily living (ADL), speech impairment, number of medications, and liking to participate in groups were also highly correlated with various measures of engagement—engagement, attitude, active participation, asleep during activities, and positive mood 25 These personal characteristics explained 46% to 62% of the variance in the measures of engagement. 23 The stimulus variable of activity content was also shown to significantly affect these levels of engagement. 24
One dimension of engagement, attendance, appears to be distinct from the others. In the abovementioned study, 23 attendance showed less of a relationship with personal characteristics, when compared to the other measures, and predicted less of the variance. Attendance also shows little correlation with the other measures of engagement, which are themselves highly intercorrelated. As such, attendance is considered to be a separate and independent dimension of engagement. Attendance can be measured on both an individual level through attendance duration (ie, what portion of the activity the person attends) and, on a group level, through number of persons attending. 25 However, studies of engagement typically do not include these measures among the items used to assess engagement. Accordingly, there is little information on whether factors that affect other measures of engagement (ie, personal, stimulus, and environmental attributes) also affect attendance.
Attendance has rarely been studied in the context of group activities. It is crucial, however, because in order to benefit from group activities, one must attend them. Yet, little is known about patterns of attendance/nonattendance of persons with dementia at nursing home activity groups or of factors that can affect attendance. Attendance can be whole or partial, that is, individuals can stay for the entire session or only a part of it. But the factors which affect how much of a session residents typically attend, and the reasons for partial attendance, have not been described. Similarly, residents may not attend sessions for various reasons from refusal or involvement in another activity to being sick or having a guest. Activity content (a stimulus attribute) and time of day (an environmental attribute) could also affect attendance. However, little information exists pertaining to these issues.
Understanding the influences on attendance could aid in generating and maintaining participation of residents in nursing home activities. Knowing which activities residents are likely to attend would provide useful information both for designing programs of group activity and for assessing the feasibility and utility of such programs for persons with dementia in the nursing home environment. Similarly, knowing the time of day at which residents are most likely to attend group activities would aid in maximizing attendance.
This study investigated patterns of attendance at group activities by nursing home residents with dementia. Addressing attendance on an individual level, we described what the resident was doing prior to the activity, patterns of attendance/nonattendance, and reasons for nonattendance, duration of attendance at each session—whether the whole time or part of the time—and reasons for partial attendance. We also examined the impact on attendance of the stimulus attribute of activity content, and of the environmental attribute of time of day, both on an individual level through attendance duration (ie, what proportion of the activity the person attends) and on a group level through number of persons attending.
Research Design and Methods
Participants
This study was reviewed and approved by the research ethics board of Baycrest Health Sciences. Participants for the study were recruited from 6 nursing home units for persons with dementia at a geriatric residential facility between January 2015 and May 2015. Of 151 potential participants, 33 (21.9%) were excluded because of entry criteria. Recruitment was staggered, in that we involved 1 unit at a time. Once consent was obtained from the substitute decision makers for 10 to 12 eligible participants from a unit, recruitment for that unit was closed, based on the opinion of recreation staff members that up to 10 to 12 participants would be an appropriate size for each group. The final sample consisted of 69 (45.7%) participants. Consent was refused in 15 (9.9%) cases. In the remaining cases, decision makers were not contacted either because they could not be reached or because the recruitment quota was satisfied.
The criterion for inclusion was a diagnosis of dementia (derived from the medical chart). Exclusion criteria were (1) a diagnosis of bipolar disorder; (2) a lifelong diagnosis of schizophrenia; and (3) Cognitive Performance Scale (CPS 26 ) Score 1 or below. This criterion corresponds to the criterion of a diagnosis of dementia, and scores 0 or 1 represent no or borderline cognitive impairment. Persons with this level of cognitive function can articulate their interests and needs most of the time; (4) no dexterity movement in either hand; (5) inability to be comfortably seated in a chair or wheelchair, or to be moved to the location of the group therapeutic recreation; and (6) inability to speak English. In order to ascertain the utility of activity groups to the full spectrum of persons with dementia in the nursing home setting, we purposefully did not select participants on the basis of their interest in particular activity groups.
Background information was gathered from the electronic health record system (Meditech, Westwood, MA) and also using Minimum Data Set (MDS) version 2. This information included age, gender, marital status, years of education, number of children, total number of medications, and total number of medical diagnoses. Cognitive functioning was assessed via the CPS 26 through the MDS, which has the scale of 0 = “intact” to 6 = “very severe impairment.” Activities of daily living performance was assessed via the ADL long form 27 with a scale of 0 = “total independence” to 28 = “total dependence.” Functional impairments were assessed with the following scales taken from the MDS 26 : mobility (1 = mobile, ie, walking, 2 = use of cane/walker/crutch, 3 = wheelchair independently, 4 = wheelchair with assistance from others, 5 = immobile, ie, bedridden); speech impairment (0 = clear speech, 1 = unclear speech, 2 = no speech); English language comprehension (English as first language = 1, English as second language = 2, minimal English = 3, no English = 4); hearing (scale: 0 = hears adequately to 3 = highly impaired); and vision (scale: 0 = adequate to 4 = severely impaired).
In addition to the participation of residents formally enrolled in the study, activities were also attended by spontaneous or drop-in participants. Although there were no general announcements about the activity groups, nonparticipating residents could become aware that they were taking place. If the activity was held in the unit lounge, other residents could see that there was a gathering of people and could try to join. When the activity was not in the lounge but elsewhere on the unit, one could hear or see that something was happening, and this would draw people in. Sometimes participants’ private duty attendant brought them. These drop-in participants who wanted to join the activity were accommodated, and we include their attendance numbers here as an indicator of interest in the activities presented for the general nursing home population.
Procedure
Each therapeutic recreation (TR) staff member led 10 different group activities for the persons with dementia on her assigned unit. The 10 activities, which were chosen by 3 experienced Certified Therapeutic Recreation Specialist® (CTRS) TRs with an average of 11.5 years of experience, were considered to be common activities in nursing home settings. They included choral singing, baking, creative storytelling, reading with discussion, brain games, active games (eg, ball toss), exercise, reminiscence poetry, holiday newsletter, and holiday discussions (for additional details see the study by Cohen-Mansfield 28 ).
One group activity was conducted per session, and each group activity was conducted twice, in random order, so that each unit completed 20 group activity sessions. The sessions were scheduled to last approximately 30 minutes based on TR experiences. The time of day the activities were presented was determined by the schedule of the TR staff members so that each unit had 2 time slots per week, which generally remained constant throughout the study. The length of the study was approximately 3 to 4 months on each unit and lasted 7 months overall. The usual program of nursing home activities continued concurrently during the research period.
The TRs approached each study participant on her unit prior to the start of the session to describe the activity and to ask for his or her assent to attend. Those who agreed or did not otherwise indicate refusal were then escorted to the activity location by the TR, a research assistant, or a private aide. Participants who were incapable of assenting were informed about the activity and taken to it unless they indicated disagreement. The TR indicated—using a multiple-choice questionnaire with the ability to write in additional options—whether the resident agreed to participate, reasons for nonparticipation, and what the resident was doing when approached about the group activity.
Assessment
Attendance at an individual level
Various aspects related to attendance were recorded by the TR for each person enrolled in the study at each session. These included: (1) how the participant was occupied before the activity; (2) whether the participant agreed/refused to attend, and reasons for not attending; (3) attendance duration or how much of the session the participant attended, rated on a 7-point scale from 0 = none of the time to 6 = all of the time; and (4) reasons for partial attendance. Attendance duration was also used as the outcome measure of engagement in analyses at the individual level.
Attendance at a group level
The number of enrolled persons attending each session, and the number of drop-ins, were recorded as the dependent variables. Environmental conditions during the activity were also noted, including location and time of day.
All observations were recorded on a multiple-choice questionnaire. Interrater reliabilities for the dependent variables between 2 research observers on a somewhat larger sample were 1.0 (intraclass correlation) and 99.9% (1-point discrepancy) for attendance duration, with corresponding reliabilities of 0.97 and 87.8% for number of participants. Correlations between research observer and TR ratings were 0.97 for attendance duration and 0.96 for number of participants. 25
Analytic Approach
Frequencies and descriptive statistics were used to summarize participant demographics. Frequencies were also used to describe rates of attendance/nonattendance at group activities. Means for attendance duration were used as an individual-level measure of engagement. Mean number of persons attending, both total participants and drop-in attendees, was used as the dependent variables for group-level analyses. Mixed model analyses using the Mixed Models procedure in SPSS Version 24 with linear model selection and compound symmetry as type of repeated covariance were used to assess whether group topic and/or time of day affected the attendance measures of engagement. Cognitive Performance Scale was added as a covariate term, as it was shown to be the most important factor in engagement. 23,24 In specific comparisons, holiday news was the reference group for activity topic.
Results
Participants
Of the 69 participants enrolled in the study, over half (62.32%) were female; average age was 86.81 years (standard deviation [SD] = 7.97, range: 63-100). Most were widowed or married (42% each). Activities of Daily Living–Long Form averaged 20.52 (SD = 6.34, range: 3-28) and CPS averaged 4.19 (SD = 1.35, range: 2-6). Participants had an average of 5.52 medical diagnoses (SD = 2.32, range: 2-12). The greatest impairment was with respect to mobility, as only 15.94% were mobile without any aids, while 46.38% required a wheelchair with assistance to get around. Less than half had adequate vision (44.93%), and two-thirds had adequate hearing on the MDS; 26.09% had unclear speech; and another 5.80% had no speech. English was the first language for 60.87% of the sample.
As the drop-ins were not enrolled in the study, the only information we have for them is number attending.
Session Characteristics
Most activities took place in the unit lounge (70.83%), with some in the activity room off-unit (17.50%). In 1 unit, most of the activities took place in the dining room on the unit because of construction; this represented 11.67% of all group sessions. Activities were offered throughout the day (except during lunch), with 24.17% starting before 10:30
Attendance Rates
Each of the 69 participants had the opportunity to attend 20 activity sessions, resulting in attendance records for 1380 individual sessions. Attendance rate data deriving from these 1380 sessions or subsets thereof are presented in Table 1. When approached by the TR to invite them to the activity, the largest percentage of residents was awake and not engaged in another activity (36.59%), while 20.72% were sleeping. Some were involved in another activity (13.77%) or were with a visitor (5.22%), and some could not be approached because they were sick (0.58%) or out of the facility (8.41%).
Rates of Attendance/Nonattendance.
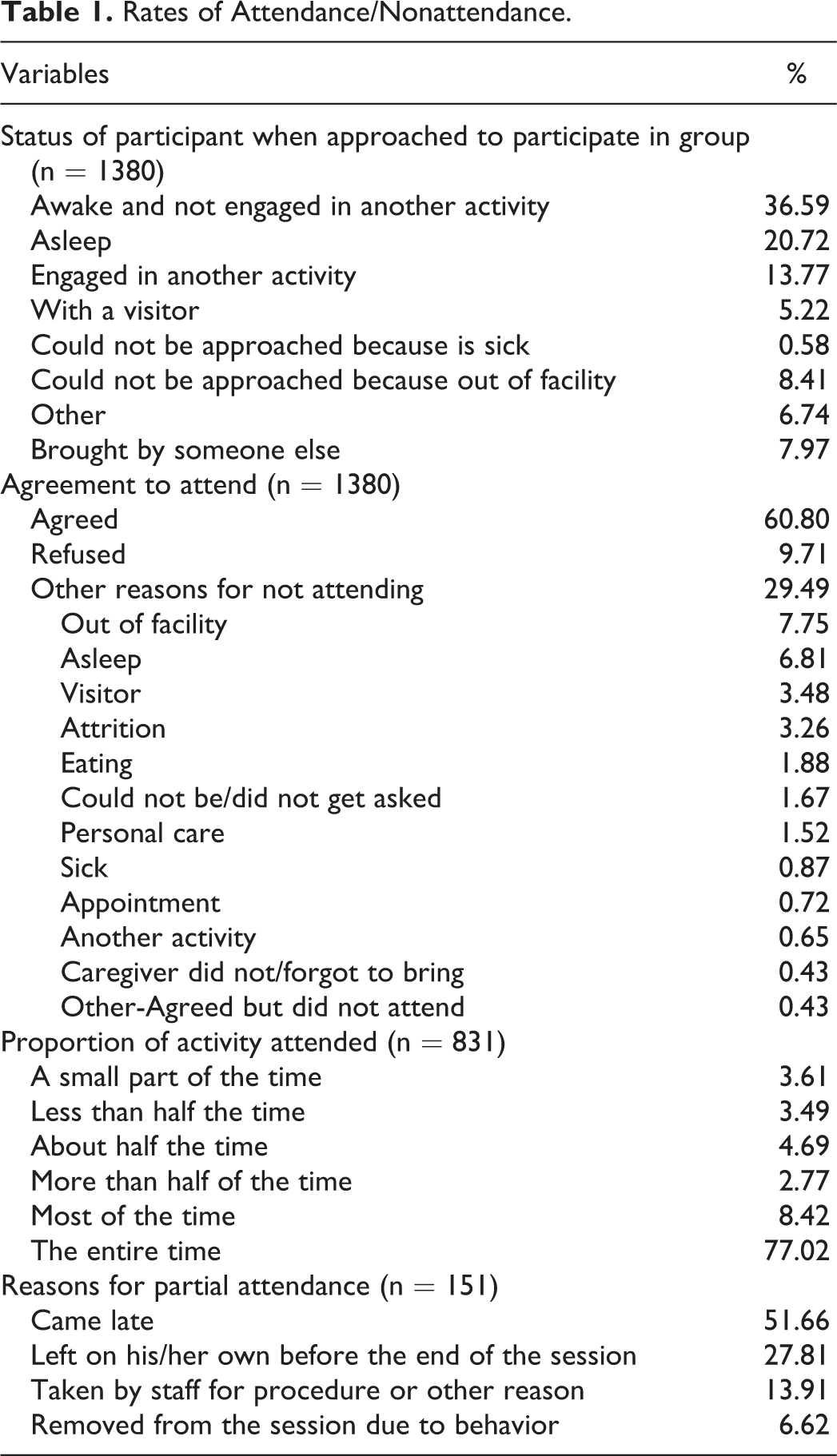
There was a 60.80% attendance rate of enrolled participants over all sessions. Mean number of sessions attended by participants was 12.16 (SD = 5.69, range: 1-20). One person attended only 1 session, and 3 participants attended all 20 activities. Median and modal attendance were both 14.
Outright refusal to attend occurred in only a small number of cases (9.71% of sessions). Refusals were more likely for participants with significantly lower levels of cognitive impairment, 3.80 vs 4.10, t(971) = 2.55; P = .0110, less functional impairment, 18.22 vs 20.50, t(971) = 4.02; P < .0001, and greater mobility (χ2(3) = 12.42, P = .0061). The rate of refusal varied with time of day, being lower than expected for early morning sessions, and higher for sessions in late afternoon, χ2(3) = 10.06, P = .0180. Refusals were most frequent for holiday news (14.19%), followed by creative storytelling (12.69%), baking (11.94%), and exercise (11.19%); refusals were least frequent for holiday discussion (6.72%).
The principal reasons for nonattendance were due to competing activities (29.49%) not directly related to the study, with the principal ones being the participant was out of the facility (7.75%), sleeping (6.81%), or with a visitor (3.48%). When not considering this group that did not attend for unrelated reasons, attendance and refusal rates changed to 86.23% and 13.77%, respectively. Attrition from the study was 3.26%.
Over three-quarters (77.02%) of those attending the sessions were there for the entire activity, and 92.90% attended for at least half of the time. Only a small percentage of participants (7.10%) was present for less than half of the activity. Roughly half (51.66%) of the participants who attended only part of the session came late, while slightly more than one-quarter (27.81%) left on their own before the end of the session. Only a very small percentage (10 of 831 occurrences of attendance) of participants had to be removed for problematic behavior.
Attendance Duration
The mean of the attendance duration scores was 3.25, indicating a range between about half the time to more than half the time (see Table 2). Tests of fixed effects in the mixed model procedure with attendance duration as the dependent variable and with group topic and time of day as independent variables, and cognitive function as a covariate, revealed no significant effects on attendance duration.
Mean Attendance Duration of Enrolled Participants for Group Topic and Start Time.a
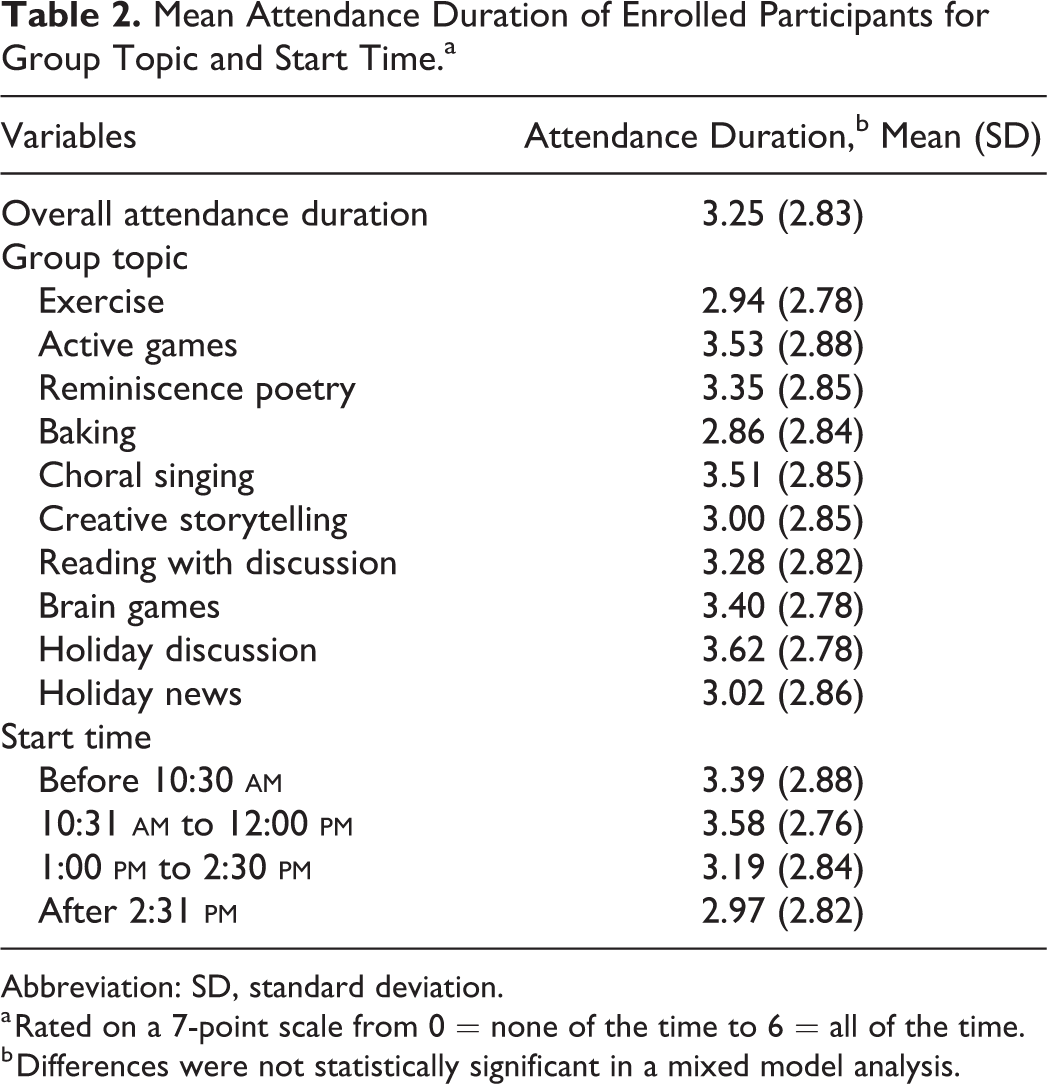
Abbreviation: SD, standard deviation.
a Rated on a 7-point scale from 0 = none of the time to 6 = all of the time.
b Differences were not statistically significant in a mixed model analysis.
Attendance Numbers
Total participants
An average of 10.67 (2.96, 5-17) residents attended each session, comprised of 7.13 enrolled participants and 3.54 drop-in residents from the unit who were not specifically invited to participate. Mixed model analyses with number of group participants as the dependent variable showed that time of day was not significantly related to the total number of participants attending each group nor was the average cognitive level of enrolled participants in the group. Group topic had a significant effect on number of attendees (F 9,101.464 = 2.393, P = .017), when controlling for start time and CPS. Estimates for choral singing, t(101.046) = 3.025, P = .003, holiday discussion, t(101.087) = 2.532, P = .013, brain games, t(101.143) = 2.161, P = .033, reading with discussion, t(101.038) = 2.092, P = .039, and exercise, t(101.004) = 2.014, P = .047, showed that these had significantly more attendees than the reference holiday news group. Table 3 provides means for the total number of persons attending each specific activity and at each time period. Choral singing (12.00) and holiday discussion groups (11.58) were the most well-attended sessions overall. Other more popular activities were exercise (11.17), reading with discussion (11.17), and brain games (11.08). Baking (9.00) was least well attended followed by holiday news groups (9.42).
Number Attending for Total and Drop-in Participants.a
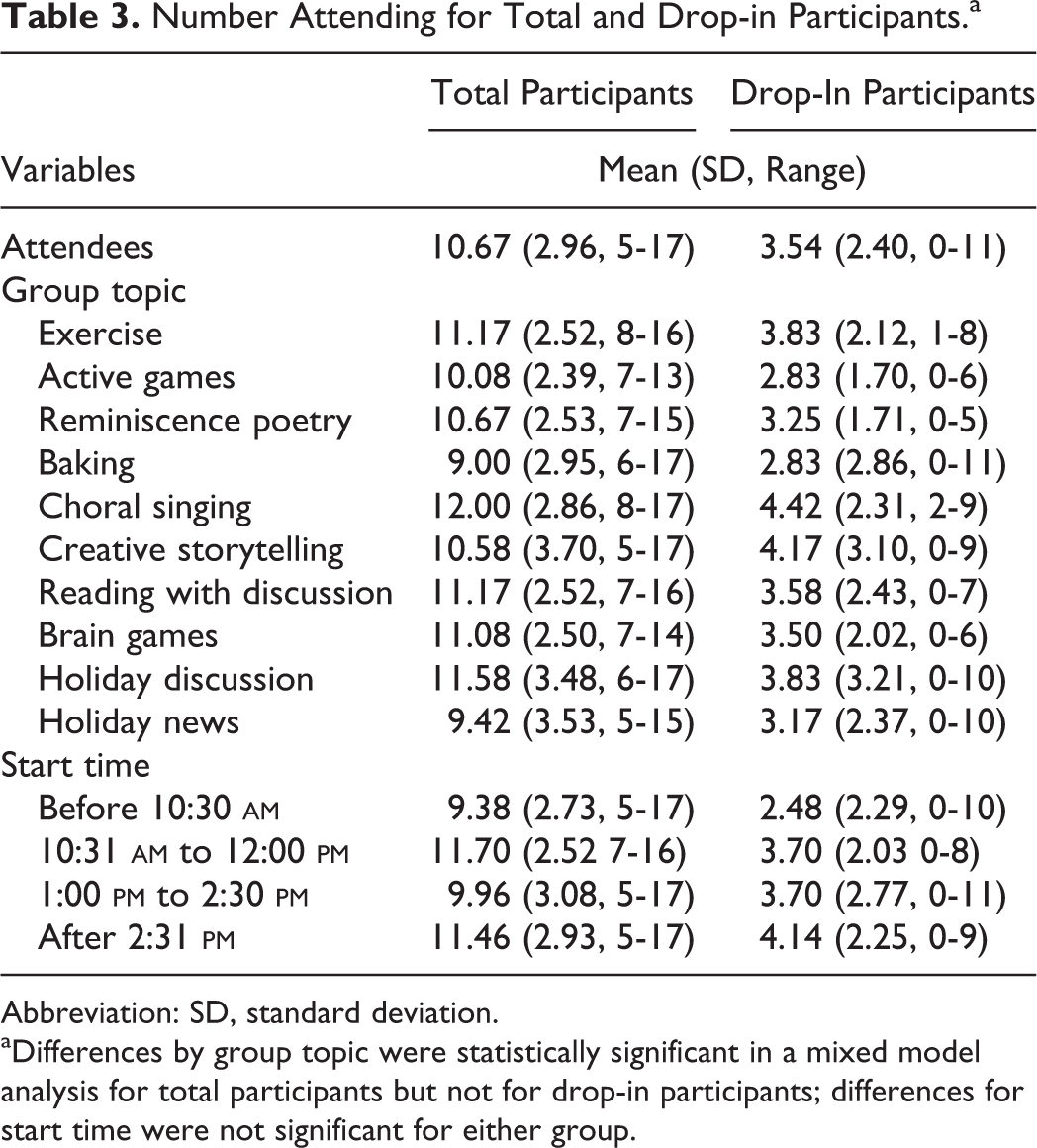
Abbreviation: SD, standard deviation.
aDifferences by group topic were statistically significant in a mixed model analysis for total participants but not for drop-in participants; differences for start time were not significant for either group.
Drop-in participants
A mean of 3.54 (2.40, 0-11) drop-in participants attended each session. There were drop-in participants for 91.67% of the sessions; only 8.33% of sessions did not have drop-in participants. In some sessions, the number of drop-in participants equaled (4.17%) or exceeded (8.33%) that of enrolled participants.
The number of drop-in participants did not vary significantly with either group topic or time of day. The distribution of number of drop-in participants by group topic and by time of day are presented in Table 3.
Discussion and Implication
The goal of this study was to describe patterns of attendance of nursing home residents with dementia at group activity programs, and to assess whether attendance varied as a function of group topic or time of day, using attendance duration and number of persons attending as dependent variables. Enrolled participants attended around 60% of the sessions to which they were invited, with reasons for nonattendance varying from being asleep or sick to being engaged with other matters, including visitors. Refusals were reported for <10% of sessions and were associated with less cognitive and functional impairment. This last finding concurs with Cohen-Mansfield et al, 29 who reported explicit refusal of individual activities to occur more in persons with higher cognitive function.
Nonattendance of enrolled participants was more than compensated by attendance of drop-ins—residents of the unit who were not recruited for the study but chose to attend, or, in cases of advanced dementia, residents whose personal caregivers brought them to the activity—with the number of drop-ins equaling or exceeding that of enrolled participants in approximately 12% of sessions. Altogether, the level of attendance reflects the need and desire for such groups. Duration of attendance was not affected by time of day the activity was offered or by the topic presented, indicating that for those who were invited to attend, these factors did not affect the length of time they spent at the sessions.
The data on group size, however, suggest that residents are more likely to attend some activities rather than others. Choral singing, holiday discussion, brain games, reading with discussion, and exercise attracted the highest total number of attendees. In contrast, drop-in participants were equally likely to attend regardless of topic, although their numbers were highest at choral singing and creative storytelling groups. Baking had the smallest number of participants, probably due to its location off the unit at an activity room equipped with a large table and refrigerator; baking also had the lowest duration of attendance. Reasons for attending a group likely include not just preference for the topic, but accessibility to location of the group, to visibility, and to awareness.
The need and desirability of activity groups is also demonstrated by the facts that enrolled participants attended the sessions the majority of the time they were asked, and most participated for the entire session. Only a small percentage of participants refused to attend an activity. For the remaining 30% of cases in which persons did not attend, this was primarily due to reasons not related to the study, such as acute disease, visits by family, or competing activities. For the few who attended less than the entire session, the primary reason was late arrival. And not only did the enrolled residents attend the activities, the activities attracted spontaneous, drop-in participants at most sessions, who found the activity interesting, and sought to join in, further highlighting the need and desirability for such activities in the nursing home. This favorable level of attendance occurred notwithstanding the ongoing presentation of the nursing home’s usual activities.
It is noteworthy, however, that the majority of participants were either doing nothing or sleeping when the TR approached them about the group activity. This finding provides a snapshot into the daily functioning of nursing home residents, corroborating findings obtained from longitudinal observation studies. Both sets of data demonstrate that nursing home residents with dementia spend much of their time doing nothing or sleeping. 5 -8 Hence, the heightened need for group activities. By providing residents with something meaningful to do, programming helps alleviate inactivity and boredom and may reduce the possibility of agitated behavior.
There was some concern that participation in a group situation would result in agitation and behavioral symptoms in some persons with dementia that would interfere with the ongoing activities of the group, 25 but there were only a few instances in which participants had to be removed for problem behavior. Elsewhere, it has been noted that negative interactions among group members were minimal. 25
We did not select participants as to their liking of groups, as we wished to work with a more representative sample. Nor did we select tasks based on resident preferences. Rather, tasks were selected to represent activities common in nursing homes and long-term care settings. Both of the abovementioned factors, however, can impact attendance. Liking to participate in groups was significantly correlated with number of sessions attended, 23 and personalized prompts for activities on the basis of resident preferences increased social activity attendance. 30
The limitations of the study are the small sample size whose participants were from one nursing home only. The validity of the results needs to be checked with larger samples and in other venues. For example, the relatively low attendance numbers and duration shown here for baking are not corroborated by Buettner and Fitzsimmons, 1 where cooking/baking is the third most frequently endorsed leisure interest of nursing home residents with dementia; the activity engaged in the greatest number of times, and with the second highest length of involvement. Although some nursing home residents prefer watching TV or doing nothing over attending activities they find irrelevant or uninteresting, others participate in activities they might otherwise find unappealing specifically for the social contact and sense of community provided. 4 Even residents who do not actively participate in the group activity or interact with others may gain some benefit from simply spending time in a social context. 31
In contrast, the high attendance at choral singing reflects other research in that music has consistently been found to be a preferred activity across a number of studies 1,4 or has brought about greater levels of engagement 32,33 or lower levels of agitation. 22 This is irrespective of music format and can include listening groups, 34,35 singing groups, 32,34 and live performances. 4,36
Even when nursing homes offer activities, generating and maintaining an interest in attending these has been a common problem. 37 Brenske et al 38 reported baseline levels of attendance of 17%, Reitz and Hawkins, 37 of 10%, and Polenick and Flora, 30 of 6.78%. The group activities in the present study had an overall attendance of 60%. Three elements incorporated in the protocol may have aided in achieving these levels: prepreparation of the activities with all the materials needed for optimal running of the groups (see the study by Cohen-Mansfield 28 ], personal invitations of the TR, and escorting residents to the location of the activity.
Various kinds of prompts have been used to try to increase attendance at nursing home activities: for example, descriptive prompts, 38 personal invitations from the recreation director or direct prompts from the nursing staff, 37 and personalized prompts based on resident activity preferences. 30 Reitz and Hawkins, 37 using personal invitations, and Brenske et al, 38 with descriptive prompts, reported increases in attendance to just under 50% and 75%, respectively. Yet, when the prompts were discontinued, attendance fell to baseline levels. Although escorting residents to an activity has not been directly studied with respect to attendance, the assistance removes one of the barriers to participation. Residents with dementia report they have little motivation to attend activities, especially those they do not find interesting or personally meaningful, and an escort may help provide the impetus needed to get there. Other residents, especially those with mobility difficulties, including most of our sample, largely rely on assistance from staff in order to attend activities. 4
Finally, although activities were not chosen on the basis of resident preferences, something which may not be feasible in all environments, a broad range of activities were included which were likely to encourage engagement by participants. The materials provided for the activities allowed modification to match the physical and cognitive capabilities of the persons attending each session, thereby allowing for inclusive participation of residents at all ability levels. This inclusiveness and the group format sought to provide participants with social support and to foster a sense of community. Future work will need to assess how integral these elements are in maintaining attendance at these types of programs.
Engagement in group activities has positive effects for persons with dementia. But it is not yet clear how these benefits can best be maximized. 39 The present article provides some information pertaining to stimulus and environmental variables that can affect attendance at group activities, which can be of value in selection and scheduling of activity programs for nursing home residents with dementia. By studying attendance, we are studying the first step in engagement, the prerequisite for using groups to impact engagement and mood and ultimately to improve quality of life.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.