
Abstract
Background:
Alzheimer’s disease (AD) has become a concerning public health issue. We aimed to analyze the trends of hospital morbidity from AD in the European Union (EU) in the period 2000 to 2014.
Methods:
Data from hospital discharges of men and women over 50 years old hospitalized due to AD in the EU were extracted from Eurostat database. We tested for secular trends computing anual percent change, and identified significant changes in the linear slope of the trend.
Results:
Hospital morbidity from AD showed a 0.8% (95% confidence intervals −2.2 to 0.6) slight declining trend in the EU. In men and women, we recorded a −0.5% and −1.0% decrease in hospital morbidity rates, respectively. Several countries showed changing trends during the study period.
Conclusion:
Alzheimer’s disease hospital morbidity has slightly declined in the entire EU in the past years. Eastern European countries showed steadily increasing trends, whereas in western and Mediterranean countries the rates decreased or leveled off.
Introduction
Alzheimer’s disease (AD) is the most common type of dementia, accounting for 60% to 70% of all cases. 1 In 2015, almost 47 million people worldwide had dementia, and this figure could reach 131 million by 2050. Among them, the number of patients in Europe is estimated to rise from 10.46 million in 2015 to almost 19 million in 2050. 2
Several studies have studied the epidemiology of AD in different world regions. In European countries, a meta-analysis estimated that the overall prevalence and incidence in people older than 55 years were 5.05% and 11.08 per 1000 person-years, respectively, 3 and mortality has increased in the past decades. 4 In the United States, prevalence of the disease was 9.51%, 5 while in developing countries it was estimated to be 3.4%. 6
Patients with AD live several years from the onset of the disease 7 and are at higher risk of hospitalization. 8 Therefore, AD leads to a great societal and economic burden. In Europe, in 2010, the total costs of dementia reached 238 billion dollars, of which direct medical costs accounted for 36 billion dollars, 9 while total payments for health care, long-term care, and hospice for patients with AD and other dementias in the United States were estimated at 236 billion dollars. 10
Despite the well-known impact of AD, to date, there is a lack of research regarding the trends of hospital morbidity from the disease, probably given its role of underlying, but not main condition, for hospitalization in many cases. Therefore, we aimed to analyze the trends of hospital morbidity from AD in the European Union (EU) in the period 2000 to 2014. Our findings may reflect the trajectories of hospitalizations from the disease in European countries in the past years, thus providing new evidence essential for planning public health policies.
Methods
Data from hospital discharges, defined as formal release of a patient from a hospital, including patients discharged alive, dead, or transferred to another hospital, 11 of men and women older than 50 years hospitalized due to AD (defined as the main condition determined as principal cause of the episode of hospitalization) for a minimum of 1 night or more than 24 hours (inpatient) or discharged on the same day (day-cases) in the member countries of the EU. We extracted data from Eurostat, the statistical office of the EU, for the period 2000 to 2014 due to the availability of the data for most of European countries in these years. 12 Eurostat receives data from each country’s statistical authorities, checks the comparability of the data, and ensures the internal coherence by annual validation processes.
Diagnosis for hospital discharges were coded using the International Shortlist for Hospital Morbidity Tabulation. 13 Code 0601 (Alzheimer's disease, International Classification of Diseases [ICD] 9th and 10th revision codes 331.0 and G30, respectively) was used.
To broaden the focus of the study, we conducted an additional analysis of men and women over 50 years old hospitalized due to dementia. Diagnosis for hospital discharges were coded with ICD codes F00-F03. 12
Estimates of resident population, based on official censuses, were also extracted from the Eurostat database. 14
The EU member countries and their data availability included: Austria (2000-2014), Belgium (2000-2009, 2011-2013), Croatia (2002-2014), Cyprus (2005-2007, 2010-2013), Czech Republic (2000-2014), Denmark (2000-2014), Finland (2001-2014), France (2000-2014), Germany (2000-2014), Hungary (2004-2014), Ireland (2000-2014), Italy (2001-2014), Latvia (2004-2014), Lithuania (2001-2014), Luxembourg (2002-2014), the Netherlands (2004-2012), Poland (2005-2014), Portugal (2000-2014), Slovakia (2000-2012, 2014), Slovenia (2004-2014), Spain (2000-2014), and the United Kingdom (2000-2014).
Unfortunately, for several countries (Bulgaria, Greece, Estonia, Malta, Romania, and Sweden) most of the data were not available and were excluded from the study. In addition, in a few countries, data for 1 or more calendar years were missing. No extrapolation was made for missing data, assuming trends would not vary substantially in countries with less missing data, whereas in countries with more missing data, results should be interpreted carefully.
From the number of hospitalizations and resident population, age-standardized hospital morbidity rates per 100 000 for each 5-year age-group (from 50-54 to 85 and older) and calendar period for men and women were computed using the direct method and based on the 2013 European Standard Population. Some countries (Czech Republic, Denmark, Italy, and Slovenia, the 2 latter countries only for day cases) considered multiepisode cases as 1 hospital discharge, while the remaining countries considered them as separate discharge records or do not allude to this issue. 11
Joinpoint regression software (version 4.2.0.2), provided by the Surveillance Research Program of the USA National Cancer Institute (Bethesda, Maryland), was used to analyze significant changes in morbidity trends. This analysis identifies inflexion points (joinpoints) at which there was a significant change in the linear slope of the trend. 15
We computed the estimated annual percent change (APC) and corresponding 95% confidence intervals (95% confidence interval [CIs]), describing the magnitude of change in the identified trends. In this model, age-standardized morbidity rates were used as the dependent variable and the year of hospital discharge as the independent variable. A P value lower than .05 was considered as statistically significant. No approval by an institutional review board was required.
Results
Trends of Hospital Morbidity From AD
Between 2000 and 2014, the number of hospital discharges of inpatients and day cases over 50 years old hospitalized due to AD in the EU increased from 38 428 to 59 937.
Throughout the study period, among the member states of the EU, the highest hospital morbidity rates were found in Finland, Belgium, and Austria, whereas Cyprus, Latvia, Denmark, and Portugal showed the lowest rates. The highest overall age-standardized morbidity rate was observed in Finland in 2007, 329.7 per 100 000, and in Latvia, we found the lowest, 0.7 per 100 000, in the year 2006. (Supplemental Data 1).
During the 2000 to 2014 period, the entire EU showed a slight nonsignificant downward trend (APC = −0.8%; 95% CI: −2.2 to 0.6), identifying 2 joinpoints. Between 2000 and 2004, hospital morbidity rates showed a statistically significant rising trend (APC = 6.6%; 95% CI: 2.2 to 11.1), followed by a significant decrease in the period 2004 to 2012 (APC = −1.8%; 95% CI: −3.5 to −0.1) and a nonsignificant pronounced downward trend thereafter (APC = −11.4%; 95% CI: −22.4 to 1.2).
Morbidity rates increased in 12 countries throughout the EU. The Netherlands, Latvia, and Spain showed the largest growths, whereas Finland and Germany had the less pronounced increases. On the contrary, the remaining 10 countries showed overall downward trends. We recorded in France, Luxembourg and Italy the steepest declines, while in Hungary and Portugal morbidity rates descended slightly (Table 1).
Joinpoint Analysis for Alzheimer's Disease Hospital Morbidity Trends in the European Unión, 2000 to 2014.
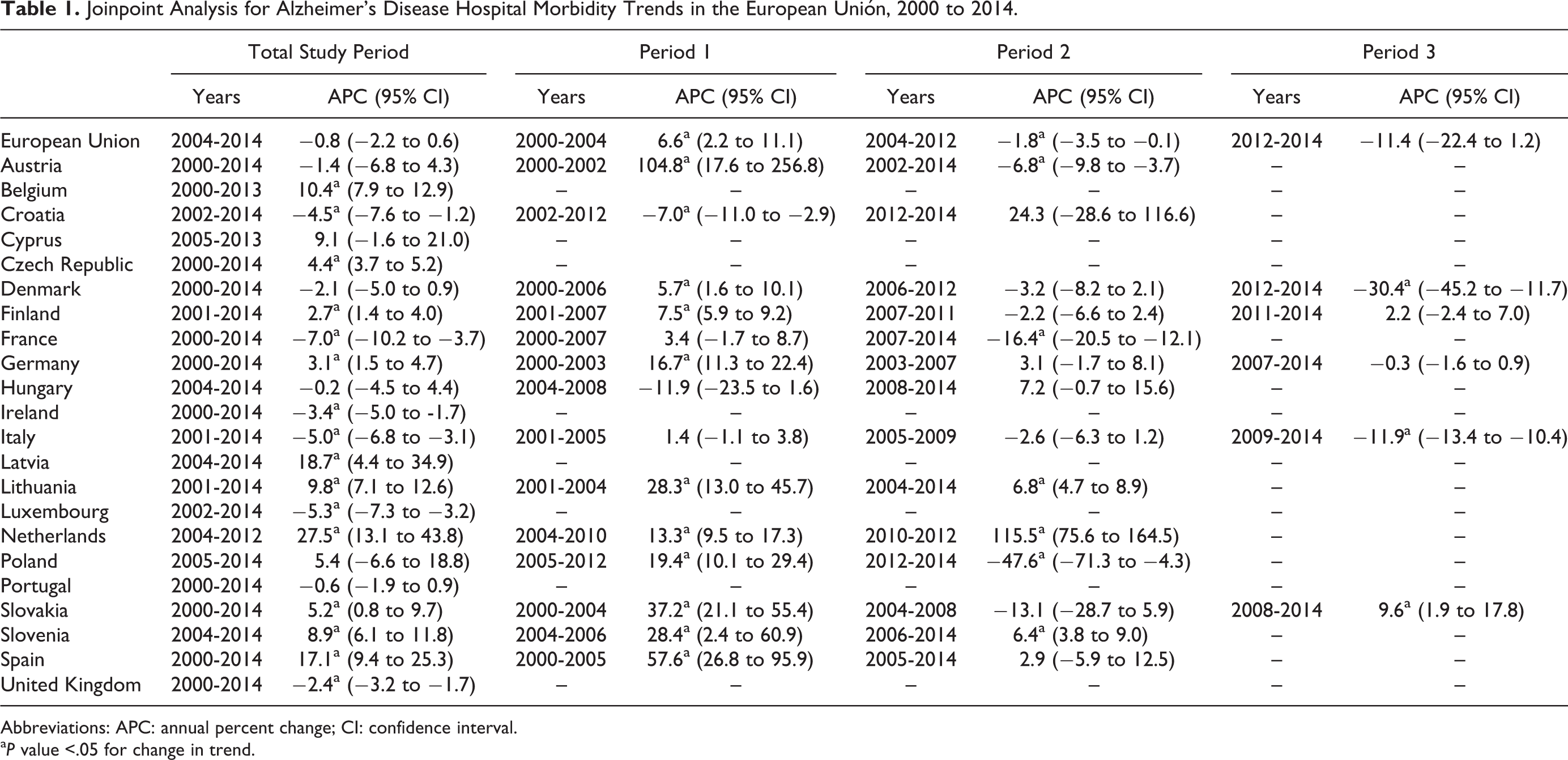
Abbreviations: APC: annual percent change; CI: confidence interval.
a P value <.05 for change in trend.
Trends of Hospital Morbidity From AD in Men
In 2000, the highest rates in men were recorded in France, Belgium, and Czech Republic (over 50 per 100 000), while Spain, Slovakia, Denmark, and Portugal showed the lowest (below 8 per 100 000). In 2014, we observed the highest rates in Finland, Czech Republic, and Slovenia (over 80 per 100 000), and the lowest in Denmark, Portugal, and Latvia (below 9 per 100 000; Supplemental Data 2).
Along the study period, European men showed an overall nonsignificant downward trend in hospital morbidity (APC = −0.5%; 95% CI: −1.8 to 0.8), identifying 2 joinpoints. In the first years, a statistically significant growing trend was recorded, followed by nonsignificant decreasing trends afterward, more pronounced in the latter years.
Morbidity rates rose in 13 countries. The Netherlands, Latvia, and Spain showed the steepest increasing trends, while in Cyprus, Hungary, and Finland the less pronounced growing trends were observed. Conversely, in 9 countries, rates lessened over the study period. In France, Italy, and Luxembourg, we recorded the largest declining trends, while in Portugal, Austria, Croatia, and the United Kingdom, we found the less pronounced decreases. (Table 2)
Joinpoint Analysis for Alzheimer’s Disease Hospital Morbidity Trends in Men in the European Union, 2000 to 2014.
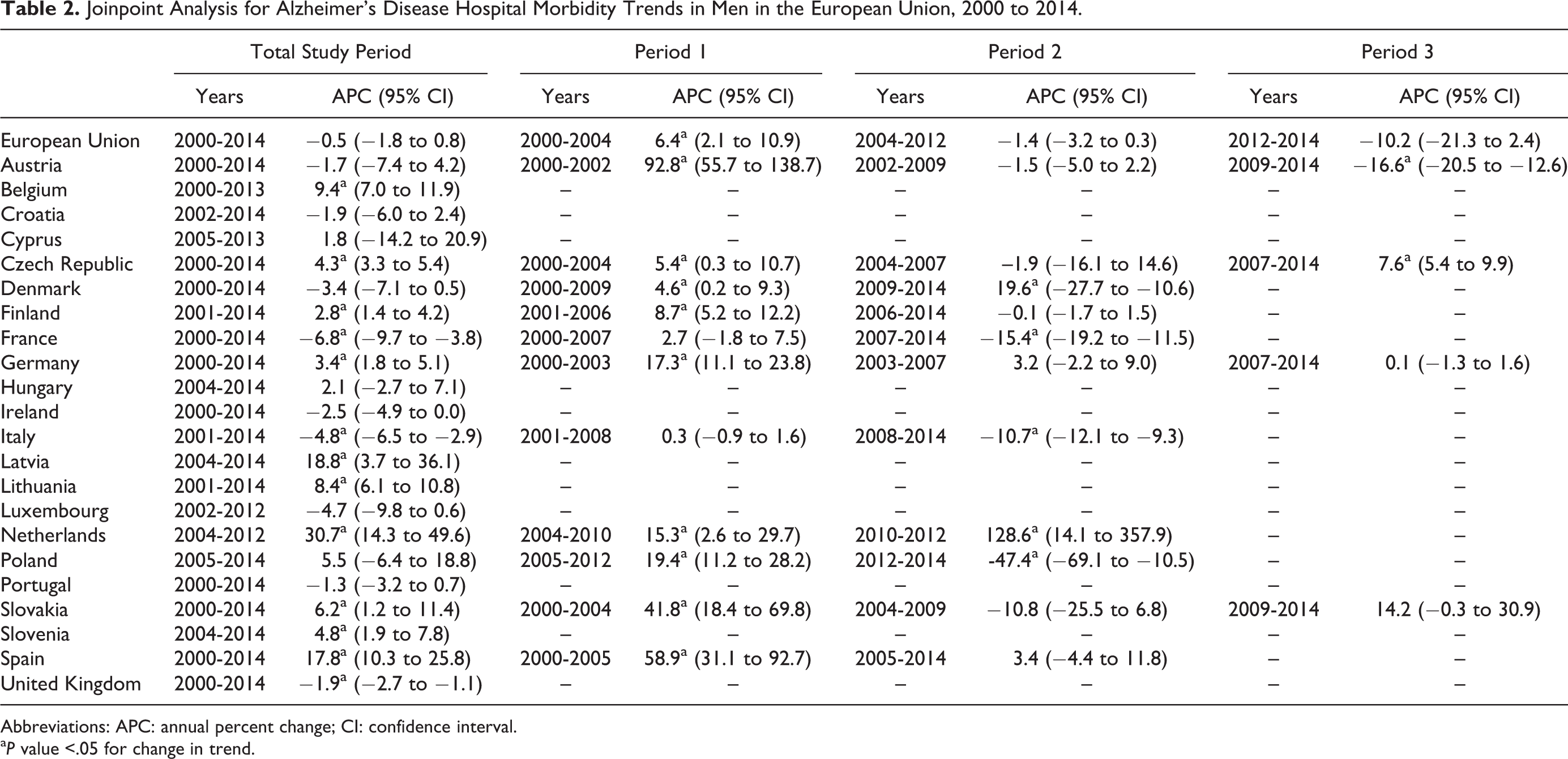
Abbreviations: APC: annual percent change; CI: confidence interval.
a P value <.05 for change in trend.
In Austria, Denmark, Finland, France, and Poland, APC peaked, decreasing thereafter. Hospital morbidity rates in Italy increased at a lower rate in the first years, almost leveling off, significantly descending afterward. In Germany and Spain, after a significant increasing trend in the first period, rates continued growing at a lower rate, in contrast to the Netherlands, where it rose sharply in the last years. In Czech Republic and Slovakia, fluctuating trends were observed.
Trends of Hospital Morbidity From AD in Women
For European women, in 2000, we found the highest rates in France, Belgium, and Czech Republic (over 60 per 100 000) and the lowest in Spain, Slovakia, Portugal, and Denmark (below 6 per 100 000). In 2014, the highest rates were recorded in Finland, Czech Republic, and Slovenia (over 80 per 100 000) and the lowest in Denmark and Portugal (below 7 per 100 000; Supplemental Data 3).
Likewise, among women, an overall nonsignificant downward trend was recorded (APC = −1.0%; 95% CI: −2.4 to 0.5), identifying 2 joinpoints. We observed a significant growing trend in the first years, followed by a significant decrease, and a more pronounced nonsignificant declining trend in the latter years.
During the study period, 13 countries showed an upward trend. The Netherlands, Latvia, and Spain showed the steepest growths, while in Finland, Germany, and Portugal the rates increased slightly or almost leveled off. In contrast, 9 countries showed declining trends. France, Luxembourg, and Croatia had the largest decreases, while Austria, Denmark, and Hungary showed the less pronounced declines. (Table 3)
Joinpoint Analysis for Alzheimer’s Disease Hospital Morbidity Trends in Women in the European Union, 2000 to 2014.
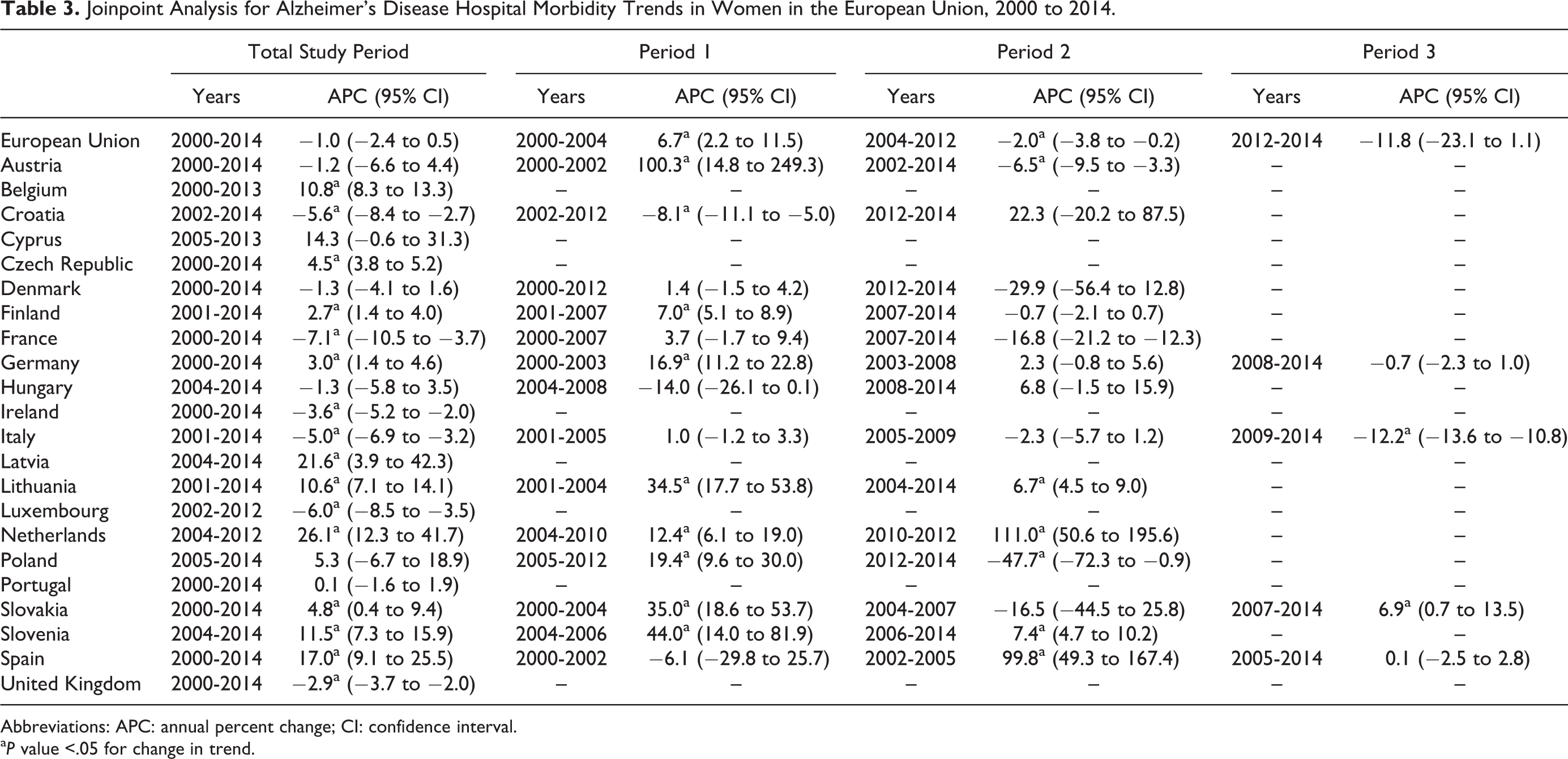
Abbreviations: APC: annual percent change; CI: confidence interval.
a P value <.05 for change in trend.
In Austria, Denmark, Finland, France, Germany, Italy, and Poland, APCs peaked, declining thereafter. In 2 countries (Lithuania and Slovenia), significant pronounced upward trends were recorded in the first period, significantly increasing at a lower rate afterward, contrasting with the pronounced growing trend found in the Netherlands in the latter years. In Croatia and Hungary, morbidity rates lowered in the first period, showing a nonsignificant rising in the latter. In Slovakia and Spain, fluctuating trends were observed.
Trends of hospital morbidity by gender in the whole EU are shown in Figure 1. Except in Austria, Denmark, Finland, Germany, the Netherlands, Poland, Slovakia, and Spain, trends were more pronounced in women than in men. Furthermore, in Hungary and Portugal, trends were divergent (Figure 2).
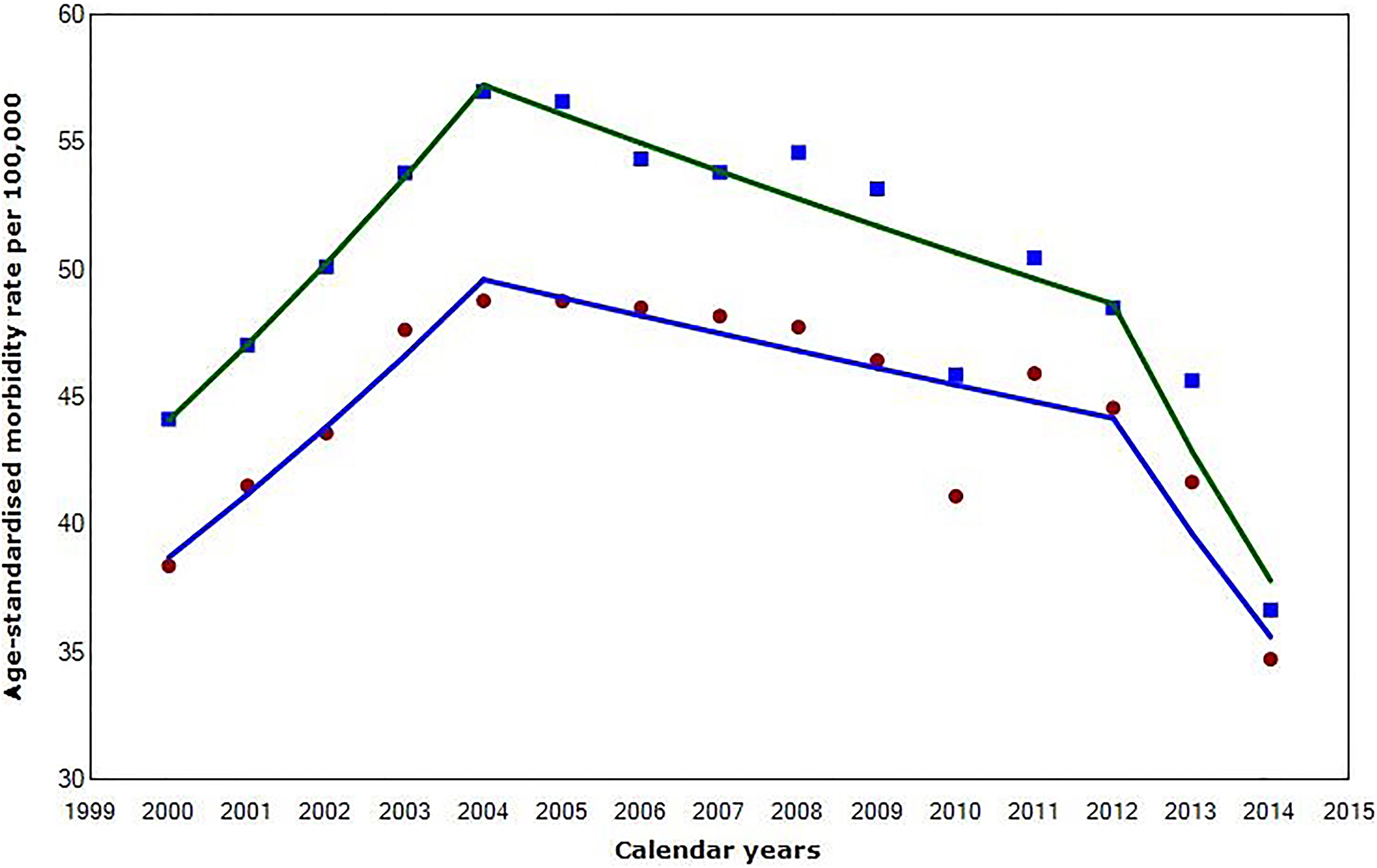
Trends in hospital morbidity from Alzheimer’s disease in the entire European Union, 2000 to 2014. Square: women (age-standardized morbidity rates); circle: men (age-standardized morbidity rates); upper line: trends in hospital morbidity from Alzheimer's disease for European women; lower line: trends in hospital morbidity from Alzheimer's disease for European men (color figures appear in the online version).
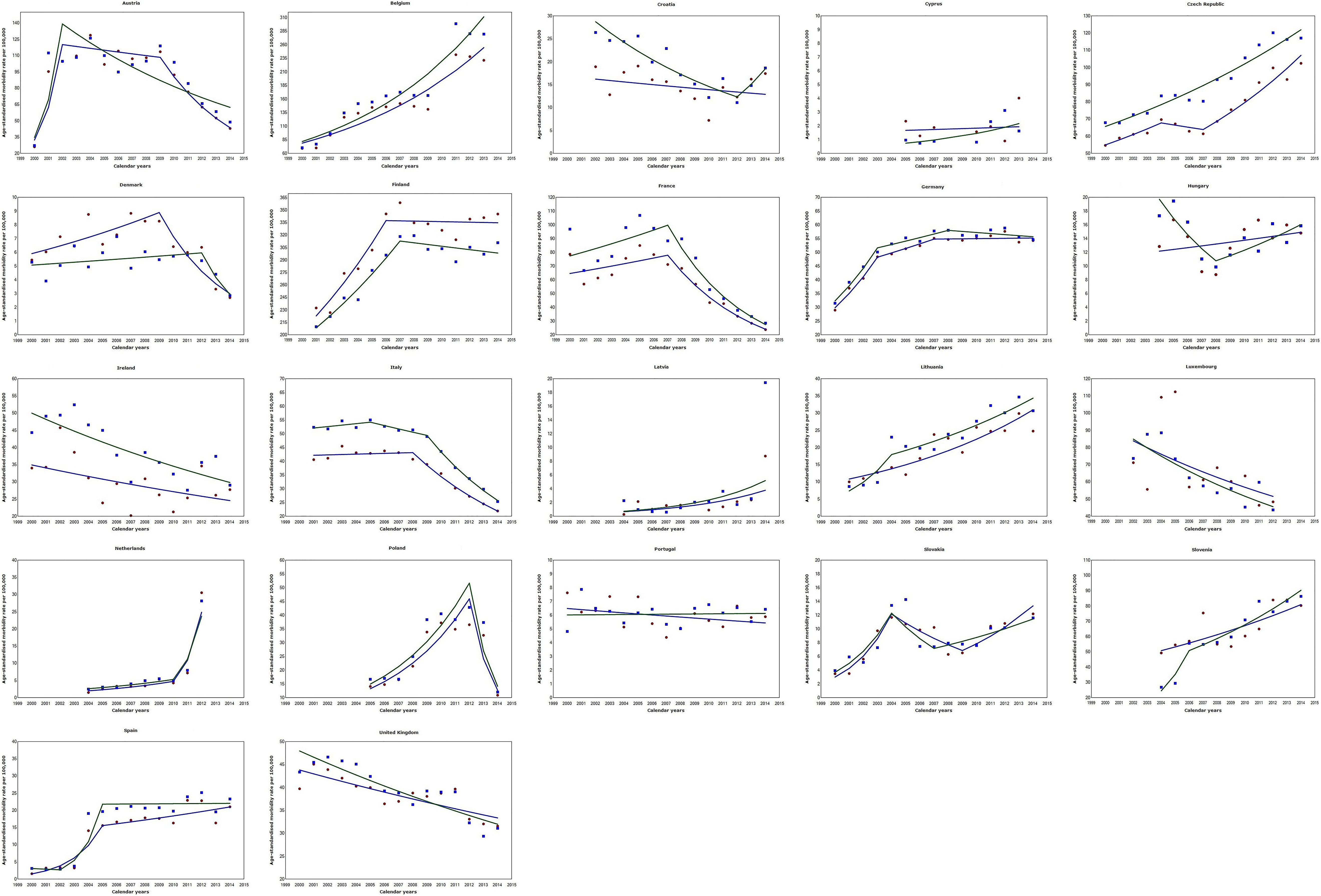
Trends in hospital morbidity from Alzheimer’s disease in the member countries of the European Union, 2000 to 2014. Square (blue): women (age-standardized morbidity rates); circle (red): men (age-standardized morbidity rates); green line: trends in hospital morbidity from Alzheimer’s disease for European women; blue line: trends in hospital morbidity from Alzheimer’s disease for European men (color figures appear in the online version).
Trends of Hospital Morbidity From Dementia
Between 2000 and 2014, hospital morbidity rates from dementia showed a significant downward trend (APC = −3.9%; 95% CI: −4.2 to −3.7). We did not identify any joinpoints.
Morbidity rates increased in 4 countries: Cyprus, Ireland, Latvia, and Slovenia. In the first 3 countries, we recorded the largest increases (all statistically significant), especially in Cyprus. Conversely, the remaining countries showed overall declining trends. We found in Belgium, Germany, Italy, and Lithuania the steepest decreases, while in Croatia, France, and Slovakia morbidity rates declined slightly (Supplemental Data 4-6).
Morbidity trends from AD and dementia showed the same direction in 12 countries (Austria, Croatia, Cyprus, Denmark, France, Hungary, Italy, Latvia, Luxembourg, Portugal, Slovenia, and the United Kingdom), while in the remaining 10 countries (Belgium, Czech Republic, Finland, Germany, Ireland, Lithuania, the Netherlands, Poland, Slovakia, and Spain) hospital morbidity trends were divergent.
Discussion
To the best of our knowledge, this is the first study analyzing the trends in hospital morbidity from AD in the EU according to hospital discharge data. Our results indicate that, despite the growing number of hospital discharges, trends declined slightly in both sexes along the past years. By countries, the steepest increases were found in the Netherlands, Latvia, and Spain, whereas in France, Luxembourg, and Italy, we recorded the largest descending trends.
Our results are in line with a US study which reported a slight decline of trends in hospitalizations between 1999 and 2009, describing an increasing trend in the first years, followed by a subsequent decrease. 16 In other European studies, both prevalence of dementia in hospitalized population and hospitalization rates tended to increase in the early 2000s, which also seem to be consistent with our findings. 17,18
This study retrieved data from 22 EU countries. Therefore, differences in diagnosis and hospital practice, discharge patterns, and cultural differences within these countries, considered as inherent factors, might explain to a certain extent the divergences observed. In this line, in a previously published study, Waldemar et al 19 identified the economic barriers, including not only differences in per capita gross domestic product but variations in care costs across European regions, 20 the fear of social stigma and cultural beliefs and the lack of specialists as the main barriers affecting the access to diagnostic evaluation and treatment for the disease in EU.
In the former-Soviet Baltic States and eastern European countries, where steady growing trends were recorded, improvement in social conditions, economic development, and the adoption of healthier lifestyle habits, which have led to the rise of life expectancy in the past decades, 21 and therefore to rising prevalence of age-related diseases such as AD, might be a reason of the trends observed. Also, changes in the survival period among people who had the disease, with a prolonged survival of several years, 22,23 might increase the probability to be hospitalized for this cause.
Conversely, in most of the western and Mediterranean countries, after increasing in the first years, hospitalization rates tended to decrease. Prior investigations have ascertained that prevalence of dementia have lessened in these countries, 24 probably due to societal changes that brought about better living conditions and the progressive adherence to healthier lifestyles. 25 Therefore, we speculate that the lowering in prevalence might be, to a certain extent, related to the descending trends observed in the latter years. Other related factor that may explain this decline is the considerable increase in utilization of ambulatory services and primary care services by patients diagnosed with AD, 26,27 especially among rural population. 28
In some countries, very pronounced upward trends were observed in the first study period. We propose several hypotheses for this observation. On the one hand, this could be the reflection of an increased awareness of the condition by the physicians, as reported in a Finnish study finding that predictive positive value for hospital discharge diagnoses improved considerably after 1998. 29 On the other hand, methodological issues, for example, in Austria, there was a change from ICD-9 to ICD-10 in year 2001 11 that could explain the sharp increasing trend observed in this country.
The fact that, despite recent efforts, AD is still underreported in hospital discharge registers should also be mentioned. In a Swedish study testing 2 disease registries, sensitivity was 55%, thus missing 45% of prevalent patients in the inpatient registry. 30 More recently, Douzenis et al 31 also found that cognitive decline was greatly underdiagnosed.
Other factors that may confuse AD diagnosis is the fact that some patients might have delirium during their hospital stay. Some investigations reported that prevalence of delirium in older patients ranged between 16% to 20%. 32,33 Also, delirium appears to be phenomenologically similar among patients with or without dementia. 34 This fact may lead to misdiagnose AD among nondementia patients and should be taken into account. We could not use algorithms to validate AD diagnosis in this study and should be acknowledged. However, Eurostat conducts annual validation processes and consistency checks, 11 thus we assume data used have sufficiency quality to ensure study’s validity.
One of the reasons of this underreporting might be that most of the patients with AD were not admitted for the disease itself, but to comorbid conditions. 35 Comorbidities, besides being independently associated with higher costs of care, 36 also increased the risk of subsequent hospital admission and emergency department visit. 37 In this line, Browne et al 38 found that the clear majority of patients with dementia had at least 1 comorbid condition and reported that a higher number of comorbidities was related to increased primary care consultation rates and hospital admission rates. Other recent investigations also found that comorbidity burden of patients with dementia was heavier than nondementia patients. 39 This causes difficulty in recognizing and correcting the diagnosis of AD by physicians when a patient is admitted, consequently leading to underreport the real AD hospitalization. This underreport is reflected in our findings, where only those patients diagnosed with AD as the main cause of hospitalization were included. Therefore, it seems reasonable to assume that the real hospital morbidity rate might be higher.
Another issue that deserves discussion is that many of the elderly individuals with AD might have been admitted to nursing homes. In institutionalized people, probability of hospitalization decreased as dementia worsened. 40,41 However, this institutionalized population has not been considered in this study as well as people treated at home. Therefore, it is plausible to think that we might have underestimated the real hospital morbidity rates.
As expected, morbidity trends in women were more pronounced than in men in most of European countries, possibly due to their longer life expectancy 42 and biological and social factors. 43
Our study has several strengths. To our knowledge, this is a novel study analyzing hospital morbidity trends in the whole of the EU. In addition, we decided to only use official data and not extrapolate or impute any missing data, which ensure the validity of our results. However, this work also has some limitations. First, the lack of data from several years or the whole period in some countries, whose inclusion would have improved the validity and generalization of our results. Second, the use of ICD codes may influence diagnosis coding, leading to undercode the condition. 44 This fact affects to some extent the validity of our data and should be taken into account. Another limitation is the noninclusion of institutionalized population, which could have led to underreport the real morbidity and should be duly acknowledged.
In summary, our findings confirmed a slight downward trend of hospital morbidity from AD in the EU, according to hospital discharge data, in the past years. Disparities among countries were observed, finding steady growing trends mainly in eastern European countries, whereas in most of western and Mediterranean countries hospital morbidity rates tended to decrease or almost leveled off, especially in the latter years. This novel approach in studying trajectories of hospitalization from AD in the EU provide new evidence for planning future public health policies in aged societies. The inclusion of institutionalized population, the effect of medical awareness and diagnostic improvements, and inclusion of secondary hospital diagnoses deserve further studies.
Supplemental Material
Supplemental Material, Supp - Trends in Hospital Morbidity From Alzheimer’s Disease in the European Union, 2000 to 2014
Supplemental Material, Supp for Trends in Hospital Morbidity From Alzheimer’s Disease in the European Union, 2000 to 2014 by Hao Niu, Ismael Alvarez-Alvarez, Ines Aguinaga-Ontoso, and Francisco Guillen-Grima in American Journal of Alzheimer's Disease & Other Dementias
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.