
Abstract
Although cholinesterase inhibitors (ChEIs) have been proved to help reduce cognitive deterioration in patients with Alzheimer’s disease (AD), their effects on survival remain inconclusive. This study aims to assess the effects of the persistent use of ChEIs on the risk of mortality in patients with AD. This population-based cohort study included 8614 patients having AD with ChEI prescription from 2002 to 2006 and followed until 2010. Kaplan-Meier curves and hazard ratios (HRs) of mortality were estimated in association with ChEI treatment duration and adherence. The average annual mortality rate per 100 person-years was 9.2 for the short-duration group (discontinued < 1 year) and 7.2 for the long-duration group (discontinued ≥ 2 years). Compared to the short-duration group, the long-duration group had a lower mortality (HR = 0.76, 95% confidence interval: 0.69-0.84) and shorter annual inpatient days. But the annual health-care costs did not differ significantly between the 2 groups.
Introduction
According to the latest estimate of the global impact of dementia, worldwide 46.8 million people had dementia in 2015, and this number is expected to double every 20 years. 1 Though there are still no effective drugs for Alzheimer’s disease (AD), cholinesterase inhibitors (ChEI) are proved to slow down the progression of this disease and may allow patients to remain independent in mild cases. 2 However, the effects of ChEI treatment on patients’ survival rate are still under debate. 3,4 Some studies showed that ChEIs did not prolong survival in patients with AD, 5 –7 whereas others reported a survival advantage for ChEI users with a lower mortality. 4,8 –10 Another related issue is whether longer survival under ChEIs therapy for patients with dementia may result in higher medical costs. A previous study in the United States found that 1 more month of ChEI treatment was associated with a 1% reduction in total health-care costs. 11 Pharmacoeconomic studies found that ChEI therapy was able to reduce the costs of hospitalization and increase the time to nursing home admission by maintaining the cognitive function of patients. 11 –13 However, most of the existing cost-effectiveness data on ChEIs are based on either clinical trials or decision modelling, 3 and few are based on population-based data. 10 Furthermore, whether the economic benefits of ChEIs, commonly reported in Caucasian populations, could apply to other ethnic groups also needs to be clarified.
Therefore, by conducting a population-based cohort study in Taiwan, this research aimed to evaluate the effects of treatment duration and adherence to ChEIs on the survival of patients with AD. The second aim of this study was to examine whether persistence with ChEI drugs could reduce health-care costs for patients.
Materials and Methods
Data Source and Identification of Study Participants
Taiwan launched a single-payer national health insurance (NHI) program on March 1, 1995. The data analyzed in this study were retrospectively retrieved from the claims of the NHI Research Database (NHIRD) provided by the NHI Administration, Ministry of Health and Welfare in Taiwan. The NHIRD provides all inpatient and ambulatory medical claims for around 99% of the Taiwanese population. 14 In this study, we used data from NHIRD for the ambulatory care claims, all inpatient claims, and the updated enrollment files for beneficiaries from 2002 to 2010.
In Taiwan, ChEI therapy for dementia, including donepezil, rivastigmine, and galantamine, is covered by the NHI, although under strict payment regulations since 2000. Participants with ChEI prescription must be patients with AD who have been diagnosed as such after the completion of case studies of clinical symptoms and signs, blood tests, cognitive tests, and neuroimage workups, such as brain computed tomography or magnetic resonance imaging. The clinical diagnosis must conform to the criteria in the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), the Diagnostic and Statistical Manual of Mental Disorders (Third Edition), or the National Institute of Neurological and Communicative Disorders and Stroke–Alzheimer’s Disease and Related Disorder Association (NINDS-ADRDA), with a history of dementia for more than 6 months. Patients with mild to moderate dementia, with a Mini-Mental State Examination (MMSE) score between 10 and 26, as well as Clinical Dementia Rating (CDR) from 1 to 2, are eligible for treatment within the NHI system. However, patients with old vascular insults, hydrocephalus, or brain tumors are excluded. Upon completion of the aforementioned diagnostic workup, clinical neurologists or psychiatrists can apply to the NHI administration for ChEI reimbursement. The data of all patients are reviewed by an expert committee of neurologists or psychiatrists who thus examine the patient’s the medical history, laboratory data, imaging data, and cognitive function records. Only those individuals who meet the criteria are allowed to take ChEI therapy. 15 During the treatment period, patients are regularly followed, and cognitive tests are performed every year. If the MMSE score worsens by more than 2 points or the CDR by 1 grade or more, as compared to the test result of previous year, the NHI payment for this treatment is terminated.
Figure 1 shows the flowchart for selection of the study population. In this population-based cohort study from year 1999 to 2010, we identified 13 665 persons with ≥1 admission or ≥ outpatient visits with diagnoses of AD (ICD-9-CM codes 331.0x) or dementia (ICD-9-CM codes 290.xx) and prescribed ChEIs during the period from January 1, 2002, to December 31, 2006. We traced the medical claims back to 1999 for each study participant and considered the first date of ChEI prescription as the index date. The follow-up was made from the index date to the occurrence of mortality, withdrawal from the insurance, or December 31, 2010, whichever came first. To avoid immortal time bias, only those who had survived for more than 3 years after the index date were enrolled. 16 Patients with the following conditions were excluded (1) admission with a principal diagnosis of stroke (ICD-9-CM code 430-438) before the index date and (2) prior ChEI use before 2002. The final sample consisted of 8614 patients with AD.
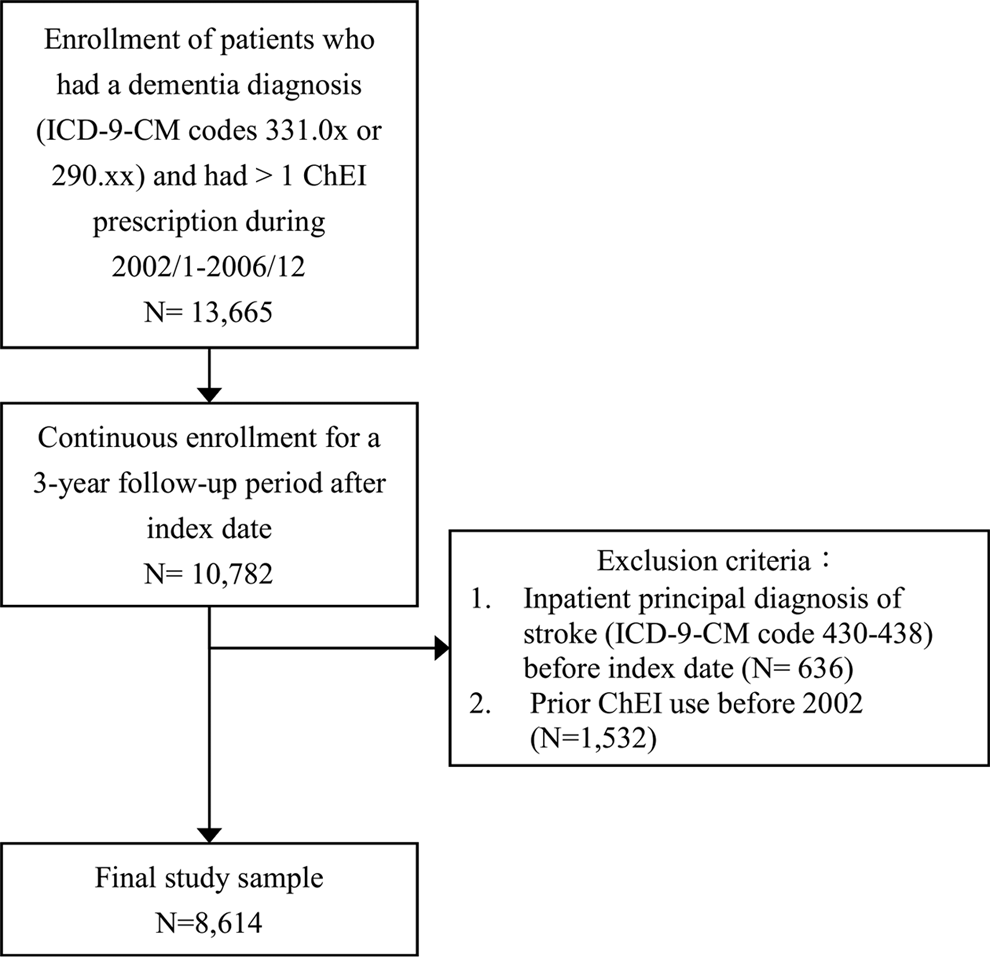
Flowchart for selection of the study sample.
Measurement of Persistent Treatment Duration and Medication Adherence
Measurements of the prescription dosage of ChEI drugs, including donepezil, rivastigmine, and galantamine, were based on the Anatomical Therapeutic Chemical Classification System. Persistence of ChEI drug utilization (ie, treatment duration) was assessed by time to discontinuation of ChEIs, measuring the number of days from the index date to the end date of the drug supply of the last ChEI prescription. Since ChEIs can be given to patients as continuously refilled prescriptions, and 30 days’ supply can be dispensed at 1 time for 3 intervals up to 90 days, so patients who did not refill aprescription for ChEIs for more than 90 days were considered nonpersistent. We chose not to analyze the differences between users of those 3 drugs, since patients could switch from one substance to another due to side effects within 3 months’ time. Treatment duration within 1 year was defined as the “short group,” between 1 and 2 years as the “intermediate group,” and between 2 and 3 years as the “long group.” Medication possession ratio (MPR) is a measure of adherence that calculates the proportion of days when a patient was in possession of medication. 17 The MPR was calculated as the total days’ supply of all ChEI claims (numerator) divided by the time to discontinuation (denominator). The MPR was censored at the value of 1.
Baseline covariates included age, gender, urbanization, Charlson Comorbidity Index (CCI), and the number of ambulatory care visits. The CCI was calculated using all medical claims of an individual in the index year and was used as a weighted score to adjust for comorbid conditions. 18 Adjustments of urbanization and number of ambulatory care visits were made to account for the potential confounding due to the fact that individuals who live in urban areas or are treated with long-term ChEIs might make more physician visits and receive more aggressive pharmacological therapies against other comorbid disorders, which would in turn affect the risk of mortality. We also examined 2 health-care utilization outcomes by ChEI treatment. The first one was the annual health-care cost covered by the NHI, including the cost of outpatient visits, emergency room visits, inpatient admission, and prescription drugs. This health-care cost measure includes all health expenditures incurred by patients with AD, which may be attributable to other comorbid conditions. The second outcome was the annual inpatient admission days during the follow-up period.
Statistical Analysis
The demographic characteristics of patients receiving different durations of ChEI treatment was compared using χ2 tests for categorical variables and 1-way analysis of variance (ANOVA) tests for continuous variables. The average annual death rate during the follow-up years was calculated by dividing the number of individuals who died by person-years at risk during the follow-up period. Survival curves obtained by the Kaplan-Meier method were plotted, and the survival rates were compared using log-rank tests. To test the proportional hazards assumption, we assessed the interaction of ChEI treatment duration with follow-up time on the risk of mortality but found no evidence that the assumption was violated. Therefore, 2 sets of Cox models were used to estimate the hazard ratios (HRs) of ChEI treatment duration and adherence on mortality: The basic model adjusted for age, sex, and CCI, while the full model additionally adjusted for the level of urbanization and annual number of ambulatory care visits. Since only 2% of our sample had a missing value on any of the control variables included in our full model, we performed complete case analysis for each regression model based on observations with complete data. For analysis on health-care costs, we used a generalized linear model (GLM) with a log link function and a γ distribution after running a modified Park’s test. 19 The results of the same test performed on inpatient days suggested a log link function and a Poisson distribution instead. We used both SAS 9.3 (SAS Institute Inc, Cary, North Carolina) and Stata 12 (Stata Corporation, College Station, Texas) to conduct our statistical analyses.
Ethical Statement
Since this study used de-identified secondary data released by Taiwan’s National Health Research Institute, it was exempt from full review by the institutional review board of En Chu Kong Hospital (IRB: TCHIRB-1021224-E).
Results
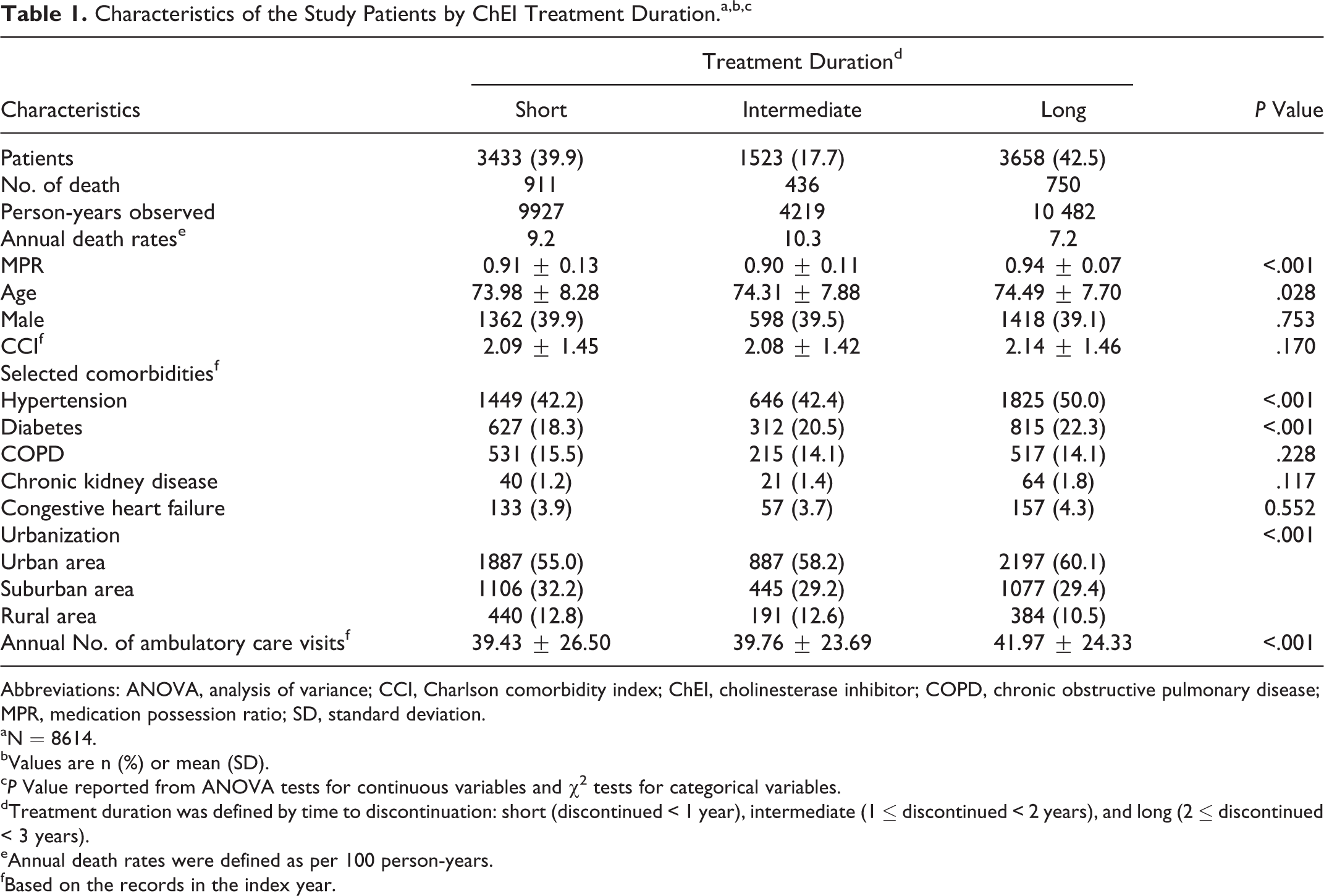
The characteristics of the study groups categorized by treatment duration of ChEIs are presented in Table 1. Nearly 40% of the patients discontinued ChEIs treatment after 1 year (short treatment group), 17.7% discontinued after 2 years (intermediate), 42.5% of the patients received ChEIs therapy for more than 2 years (long), and the average treatment duration was 2.3 years (standard deviation [SD] = 2.1). The annual mortality rates after 3 years of follow-up for the short-, intermediate-, and long-duration groups were 9.2, 10.3, and 7.2 per 100 person-years, respectively. Results from ANOVA tests for MPRs also showed difference among the ChEI groups, with the highest ratio of 0.94 observed in the long group compared to 0.91 for the short group. There was no significant difference in the comorbidity indices, but the prevalence of hypertension, diabetes, and chronic kidney disease was higher in the long treatment group. The number of ambulatory visits in the index year was also higher in patients with long ChEI treatment duration compared to the other 2 groups.
Characteristics of the Study Patients by ChEI Treatment Duration.a,b,c
Abbreviations: ANOVA, analysis of variance; CCI, Charlson comorbidity index; ChEI, cholinesterase inhibitor; COPD, chronic obstructive pulmonary disease; MPR, medication possession ratio; SD, standard deviation.
aN = 8614.
bValues are n (%) or mean (SD).
c P Value reported from ANOVA tests for continuous variables and χ2 tests for categorical variables.
dTreatment duration was defined by time to discontinuation: short (discontinued < 1 year), intermediate (1 ≤ discontinued < 2 years), and long (2 ≤ discontinued < 3 years).
eAnnual death rates were defined as per 100 person-years.
fBased on the records in the index year.
Figure 2 compares the cumulative survival rates by treatment duration. Patients in the long treatment group over the study period had a higher survival rate than the intermediate and short treatment groups, and the results from the log-rank test were statistically significant (P value < .0001).
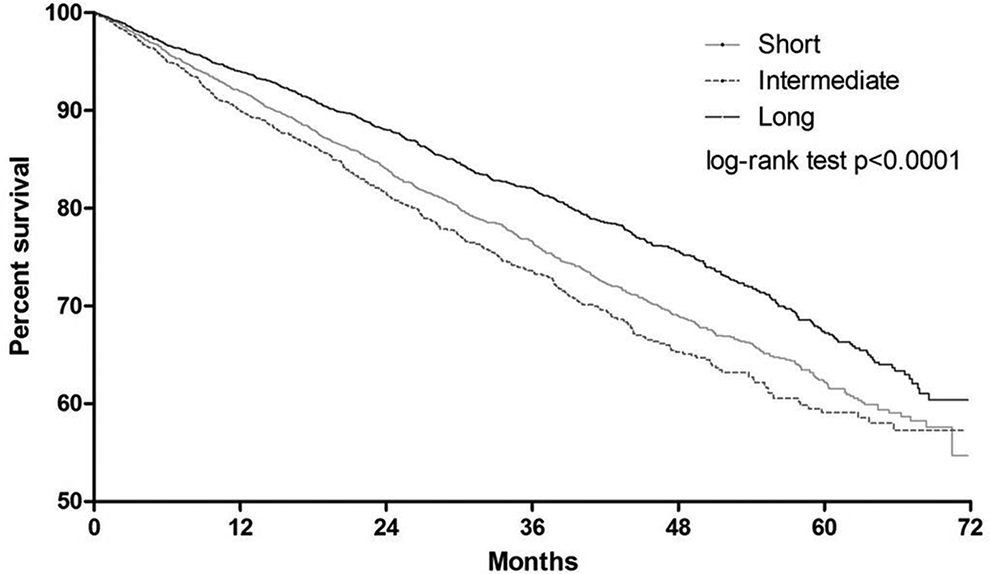
Kaplan-Meier survival estimates by cholinesterase inhibitor (ChEI) treatment duration.
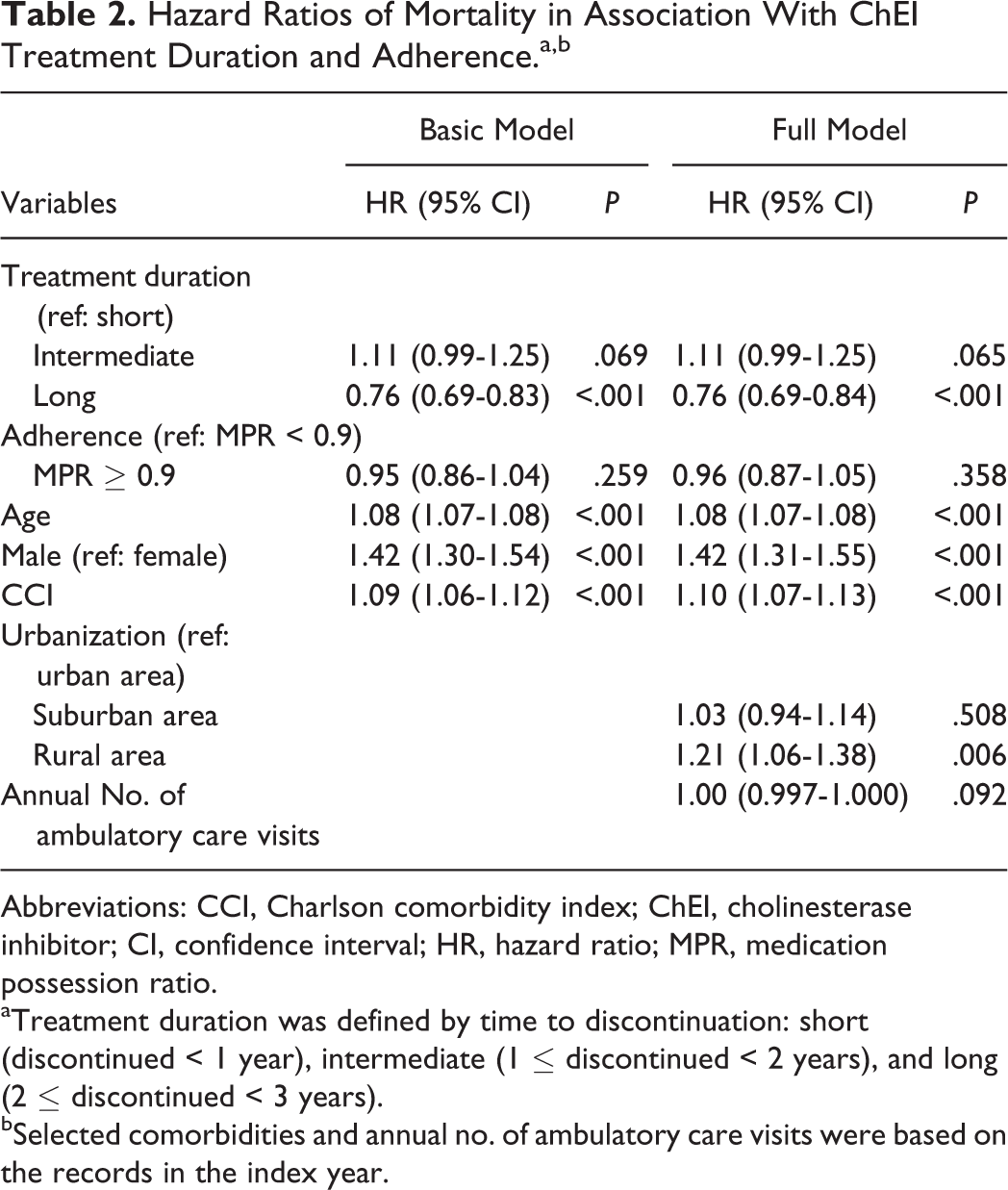
The results of the survival models among different treatment duration groups are shown in Table 2. Compared to that seen in the short-duration group, the mortality in the long group was lower, with HRs 0.76 (95% confidence interval [CI]: 0.69-0.84) in the full model. The HRs for those in the intermediate-duration group was not significantly different from that seen with the short group, with a 95% CI of 0.99 to 1.25. In the full model, the HRs for those with high adherence (MPR ≥ 0.9) were also found to be nonsignificantly different (HR = 0.96; 95% CI: 0.87-1.05) from those in the low adherence group (MPR < 0.9). Older age, being male, living in a rural area as well as having more comorbidities were all independent predictors of higher mortality.
Hazard Ratios of Mortality in Association With ChEI Treatment Duration and Adherence.a,b
Abbreviations: CCI, Charlson comorbidity index; ChEI, cholinesterase inhibitor; CI, confidence interval; HR, hazard ratio; MPR, medication possession ratio.
aTreatment duration was defined by time to discontinuation: short (discontinued < 1 year), intermediate (1 ≤ discontinued < 2 years), and long (2 ≤ discontinued < 3 years).
bSelected comorbidities and annual no. of ambulatory care visits were based on the records in the index year.
The results from the GLM models on the relationship between ChEI treatment duration and 2 health-care utilization outcomes are presented in Tables 3 and 4. Table 3 shows that the annual health-care costs of patients with long- or intermediate-duration ChEI treatment were not significantly different from those with short duration, both in the basic and full models. There was also no significant effect association between ChEI adherence and health-care costs in the GLM models. However, older age, being male, and having more comorbidities or ambulatory care visits were all independent predictors of higher health-care costs. Table 4 shows that patients with long ChEI duration reported significantly fewer annual inpatient days than the short-duration group. On the other hand, the average annual inpatient days for patients with intermediate duration did not differ significantly from the referent group of short duration. Other independent predictors of longer inpatient admission were similar to those reported for higher health-care costs, including age, gender, and comorbidities.
Generalized Linear Models of Health-Care Cost in Association With ChEI Treatment Duration and Adherence.a
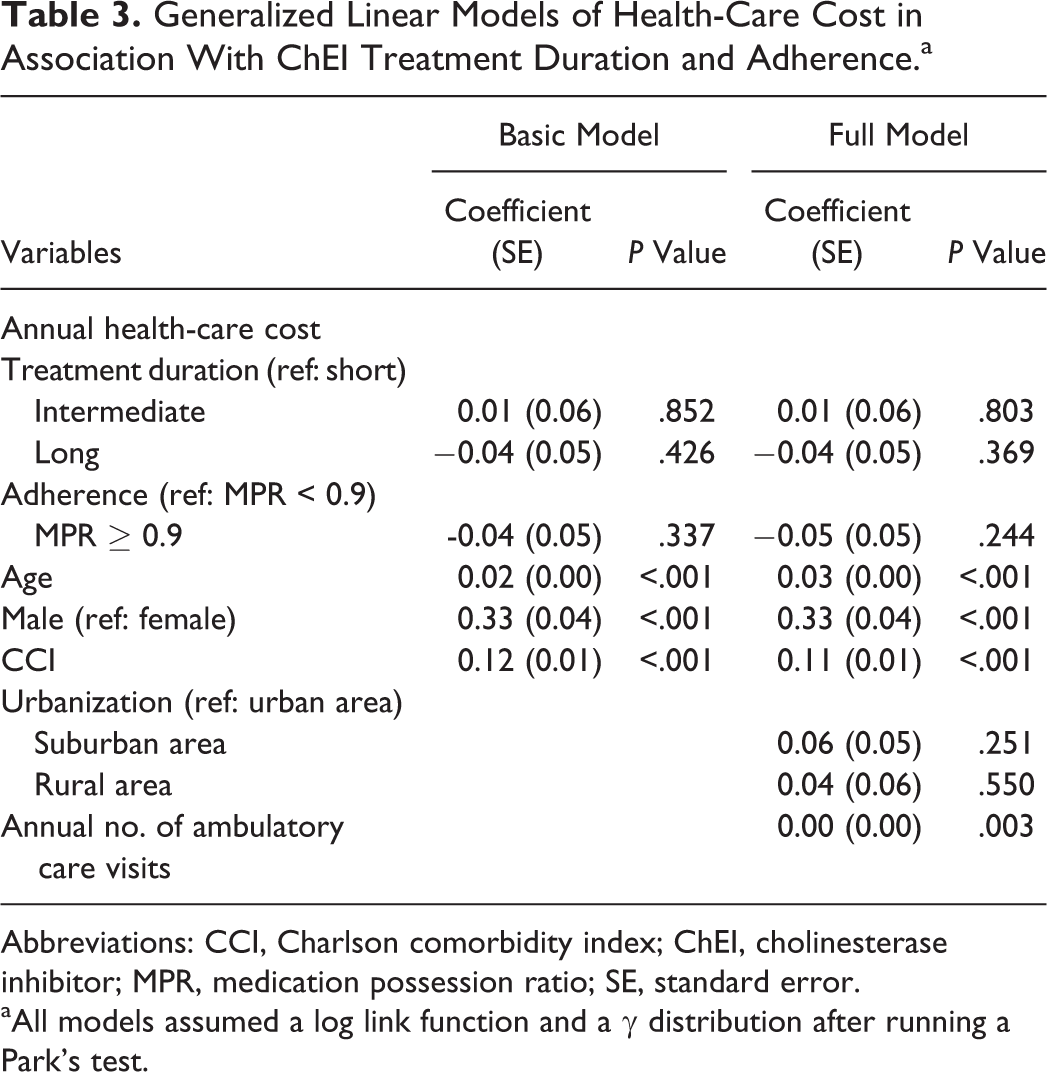
Abbreviations: CCI, Charlson comorbidity index; ChEI, cholinesterase inhibitor; MPR, medication possession ratio; SE, standard error.
aAll models assumed a log link function and a γ distribution after running a Park’s test.
Generalized Linear Models of Inpatient Days in Association With CHEI Treatment Duration and Adherence.a

Abbreviations: CCI, Charlson comorbidity index; ChEI, cholinesterase inhibitor; MPR, medication possession ratio; SE, standard error.
aAll models assumed a log link function and a Poisson distribution after running a Park’s test.
Discussion
In this study, we found that sustained ChEI treatment for more than 2 years is associated with lower mortality risk after the first 3 years, as compared to those treated for less than 1 year. However, only treatment duration was associated with improved survival but not adherence. However, because 72% of our sample reported high adherence (MPR > 0.9) as opposed to those with low adherence, it is possible that the effect of ChEI adherence on survival was not detected due to the lack of variation. Furthermore, over our 8-year follow-up period, patients with long-term ChEI treatment on average have shorter inpatient days than the short-duration groups. Despite the higher medication costs of ChEIs incurred by patients with long treatment duration, their annual total health-care costs were not greater than those of the short treatment duration patients.The fewer hospitalization days in the long treatment group presumably explain why their total health-care costs were similar to those in the short treatment group.
Studies have shown that long-term ChEI treatment benefits patients’ cognition, functioning, and behavior. 20 Recent studies also show that declines in cognition are a robust predictor of mortality in older people. 21 Deterioration of cognitive and daily functions indicates more problems related to self-care, eating, physical activity, and adherence to multiple medications, which are common in the elderly population and related to survival. 22 A prospective, observational, multicenter study in Sweden showed that a better response to ChEIs might prolong survival in patients with AD receiving higher-dosage ChEI for longer duration. 10,23 This finding echoes our results, showing that lower mortality occurred in patients under long-term treatment of ChEIs, because these patients had a better response to ChEIs and could be allowed to continue these treatment agents.
The potential anti-inflammatory effects of ChEI may be another explanation for the lower mortality rates associated with long duration of ChEI treatment. 24 Inhibition of acetylcholinesterase in the brain has been reported to suppress systemic inflammation. 25 Nordstrom et al reported that ChEI use was associated with a reduced risk of myocardial infarction and death in a nationwide cohort of participants diagnosed with AD. 26 The current study also found evidence that the ChEIs are associated with fewer hospitalization days. Acute hospital admissions play a detrimental role in the disabling process among the elderly population. For older patients, admission to hospital with progressive or persistent levels of severe disability represents more than half of the reported mortality. 27
An important strength of this study is that we used a large and representative sample of patients with AD among the whole population in Taiwan. These patients were identified not only by the ICD codes but also by their ChEI medication records. Only those patients diagnosed with AD who fit the clinical criteria with complete cognitive tests and neurological images are allowed to receive insurance-covered ChEIs. This greatly increased the accuracy of diagnoses among our study sample and reduced the possibility of miscoding common to other studies using claims data. Another contribution of this study lies in using long-term observational data over 8 years to compare health-care utilization between different ChEI treatment durations. Given that none of the existing studies has reported the health economic outcomes of ChEI treatment with an Asian population, this is the first article that confirms the economic benefits of ChEIs that were previously reported in Caucasian populations. Finally, compared to a previous study that found no association between the persistent use of ChEI and patient survival, 7 the design of the current study was improved to address the immortal time bias by excluding those patients who died before the end of the 3-year treatment duration, so that the effect of the ChEI on mortality would not be overestimated.
However, there are some limitations to this study. First of all, patients were no longer eligible for NHI payment for ChEIs if their MMSE score worsened in the annual reevaluation. It is possible that persons with a shorter duration of ChEI use may represent a patient group with more severe AD or fast-progressing disease forms compared to those with a longer duration of ChEI use. In addition, because we counted only ChEIs prescribed at outpatient setting, the shorter ChEI duration group could include those patients admitted to a hospital. These potential methodological problems could lead to certain degrees of bias for our observation, noting that ChEIs posed a beneficial effect on survival. We did manage to reduce such confounding by indication by controlling the comorbidity index, which is commonly used as a proxy of disease severity for patients with dementia. 28,29 Additionally, because only mild to moderate patients with AD having MMSE scores between 10 and 26 as well as CDR scores from 1 to 2 were eligible for ChEI reimbursement in Taiwan during our study period, severe patients with AD were not enrolled in our study. This would further diminish the variation in severity of dementia among the study patients. Furthermore, in order to assess the degree of remaining confounding by indication, we conducted a sensitivity analysis to compare the propensity scores of receiving different treatment duration for patients in each of the 3 observed ChEI groups. Results from that analysis (not shown here but available upon request) found the distribution of propensity scores for 3 ChEI duration groups largely overlapped, suggesting that patients receiving ChEI for different durations were similar in observed characteristics.
Although we adjusted for comorbidities using the CCI, we were not able to control for other factors that might affect ChEI utilization and survival time among patients with AD such as years of education, dementia severity, psychiatric symptoms, functional status, or health behaviors. Such information was not available in the claims data and thus was not included in the models. In addition, there might be some patients who took ChEIs out of pocket without the insurance reimbursement of the NHI. For those patients whose cognition deteriorated rapidly, it was not possible to know whether they continued to pay for ChEI therapy privately, and this could lead to misclassification of treatment status. Despite this concern, if we misclassified the treated as the untreated, the result would only be a bias toward the null, and we still obtained a significant finding in this regard. Finally, as we do not have any measure of actual intake of the medication, our best assumption was that patients were adherent to ChEI after refilling a prescription claim.
In conclusion, the population-based data examined in this study provide evidence that patients with AD who continue with ChEI therapy for more than 2 years have lower mortality and fewer hospitalization days, with no increase in annual health-care costs as compared to those receiving short-duration treatment. Treatment with ChEI thus seems beneficial for survival and cost-effective in patients who tolerate ChEI well and continue treatment, as compared to those who discontinue it. Further studies are needed to examine the effective dose of each type of ChEI in association with survival and to provide more evidence that can then inform the related insurance reimbursement decisions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partly supported by the Ministry of Science and Technology, ROC under Grant number MOST 102-2410-H-006-001-SS2.