
Abstract
Herein we describe 6 cases of patients with Alzheimer’s disease presented with syncope, dizziness, and dyspnea soon after the initiation of cholinesterase inhibitor therapy. All patients had bradyarrhythmia on electrocardiogram (ECG). Two patients had complete atrioventricular block, 2 pateints had 2/1 type atrioventricular block, 1 patient had sinus bradycardia and hypersensitive carotid sinus syndrome, and 1 had sick sinus syndrome. All these patients were treated with pacemaker implantation and the cholinesterase inhibitor therapy continued. At 13-month follow-up, no syncope, dizziness, or dyspnea was reported.
Patients and Methods
A total of 668 patients presented in high volume to our cardiology clinic tertiary referral hospital with symptomatic bradyarrhythmia, between January 2008 and June 2009. Among these, 574 patients had a pacemaker implanted. Of the 668 patients, 22 had Alzheimer’s disease (AD). The diagnosis of AD was established by the neurologist according to the revised fourth edition of Diagnostic and Statistical Manual of Mental Disorders criteria. 1 Patients with gradual onset of memory loss and continuing cognitive decline without any underlying causes such as infections, nutritional deficiencies, traumatic brain injury, endocrine conditions, cerebrovascular diseases, seizure disorders, brain tumors, and substance abuse were defined to have AD. 1 Twenty patients with AD had a pacemaker implanted. Six of these were on cholinesterase inhibitor (ChE-I) therapy (Table 1) started 2 to 8 weeks before the initial symptom (Table 2). Thyroid function test and serum potassium levels were obtained, and echocardiography was performed for every patient (Table 2).
Characteristics of the Patients
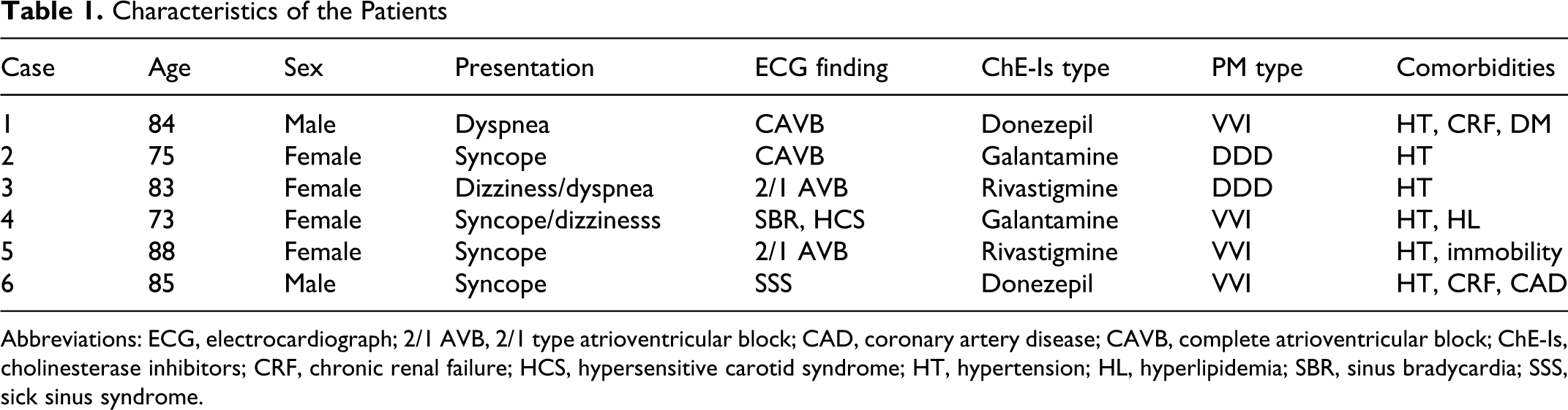
Abbreviations: ECG, electrocardiograph; 2/1 AVB, 2/1 type atrioventricular block; CAD, coronary artery disease; CAVB, complete atrioventricular block; ChE-Is, cholinesterase inhibitors; CRF, chronic renal failure; HCS, hypersensitive carotid syndrome; HT, hypertension; HL, hyperlipidemia; SBR, sinus bradycardia; SSS, sick sinus syndrome.
Additional Examinations and Initial Time of Symptom Onset After ChE-I Therapy
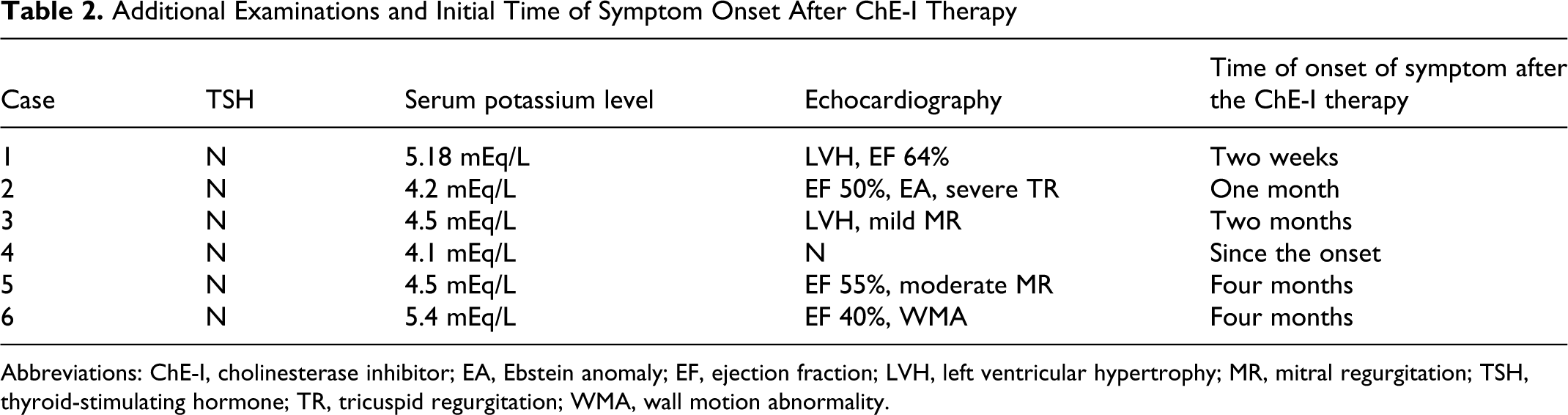
Abbreviations: ChE-I, cholinesterase inhibitor; EA, Ebstein anomaly; EF, ejection fraction; LVH, left ventricular hypertrophy; MR, mitral regurgitation; TSH, thyroid-stimulating hormone; TR, tricuspid regurgitation; WMA, wall motion abnormality.
Case Reports
Case 1
An 84-year-old male with AD was hospitalized because of dyspnea. He had a past history of hypertension, diabetes mellitus, and chronic renal failure but no syncope. He had been on metoprolol 5 mg/d for 5 years for hypertension, ramipril 5 mg/d, and metformin 1000 mg/d. An electrocardiograph (ECG) revealed complete atrioventricular (AV) block. Blood chemistry and echocardiography were obtained (Table 2). Donezepil (5 mg/d) had been started 2 weeks before syncope. Metoprolol and donezepil were discontinued. Two days later, the complete AV block resolved spontaneously to sinus rhythm. Donezepil 5 mg/d was reinitiated, and complete AV block recurred on the fifth day of therapy. A VVIR (single chamber) pacemaker was implanted and all the medications were continued. Fifteen months after discharge, the patient remained asymptomatic and donepezil dose was increased to 10 mg/d.
Case 2
A 75-year-old female with AD was admitted because of syncope. Her medical history included a diagnosis of hypertension (treated with atenolol 5 mg daily). She had been taking this drug for over 10 years. She also had been treated with galantamine for early AD for 5 months. She had experienced dizziness for 4 months. A 12-lead ECG showed a complete AV block. The AV block was resolved with atropin (1 mg). Only atenolol was discontinued. After 6 days, AV block recurred. This was treated by implantation of a VVIR pacemaker. Both atenolol and galantamine were continued. The patient remained asymptomatic at the first year of follow-up.
Case 3
An 83-year-old female who for 2 months had been being treated with rivastigmine for AD, suddenly became unwell. She had a past history of hypertension and had been on nifedipine 30 mg/d. She was bradycardic and her ECG showed a 2/1 type AV block. A DDD (two chamber) pacemaker was implanted. She remained asymptomatic at 16-month follow-up.
Case 4
A 73-year-old female with AD was admitted because of syncope, dizziness, and persistent sinus bradycardia at 48 bpm. She had a past history of hypertension and hyperlipidemia. She had been on perindopril 5 mg/d for 3 years, memantine HCL 20 mg/d, and galantamine 8 mg/d for 6 months. She had multiple episodes of syncope and dizziness since the onset of memantine HCL and galantamine therapy. The patient’s physician thought that the syncope and dizziness might be related to the hypotension and decreased the perindopril dose to half. On admission a 12-lead ECG revealed sinus bradycardia at 48 bpm. Carotid sinus massage caused sudden loss of consciousness 4 seconds after the onset of sinus arrest without escape rhythm. She was treated with a pacemaker implantation. A 13-month follow-up appointment revealed that no further syncope episodes or dizziness had occurred.
Case 5
An 88-year-old female who had been treated for 8 months with rivastigmine for AD was referred because of multiple episodes of loss of consciousness. She had been immobile for 3 years. She had a past history of hypertension and had been on ramipril 10 mg/d. The patient was bradycardic and her ECG showed a 2/1 type AV block. A VVIR pacemaker was implanted. She had no episodes of loss of consciousness until she suddenly died at 5 months after discharge.
Case 6
An 85-year-old male with AD was hospitalized following 3 episodes of syncope on the same day. There was no previous history of syncope. He had been taking donepezil 5 mg/d for 1 year and experienced dizziness for 8 months. His past history consisted of hypertension and chronic renal failure treated with trandolapril, coronary artery disease treated with acetylsalicylic acid 100 mg/d, isosorbide mononitrate 40 mg/d, and trimtazidine 60 mg/d. The ECG revealed Wenchebach type AV block. In 24-hour Holter monitoring sinus pause of 3.6 seconds with clinical evidence of syncope was determined. He was treated with a VVI pacemaker implantation. There was no syncope attack during the 20-month follow-up.
Results
The youngest patient was 73 years old. Two patients had mild AD, 3 patients had moderate AD, and 1 patient had moderately severe AD, according to the Mini-Mental State Examination (MMSE) score. 2 Average time from the initiation of ChE-I therapy to the hospital admission was 18 weeks. The most common symptom was dizziness starting just after the initiation of ChE-I therapy, but the most common presentation was syncope. All of the patients were treated with a permanent pacemaker implantation and ChE-Is were continued. Symptoms were dramatically improved in all of the patients. The AD was improved in 2 patients and was on the same level in 3 patients according to the MMSE score. 2 The progression of the disease could not be evaluated in case 5.
Discussion
Alzheimer’s disease in people over the age of 65 years is estimated to be 4.9 per 1000 person-years. Between 50% and 64% of people with AD are estimated to have mild to moderately severe disease, and approximately 50% have moderately severe to severe disease. 2 The disease most often presents with subtle onset of memory loss followed by a slow progressive dementia that has a course of several years. The management of AD is challenging and gratifying, despite the absence of a cure or a robust pharmacologic treatment. Donezepil, rivastigmine, galantamine, and memantine are the drugs presently approved by the Food and Drug Administration (FDA) for the treatment of AD. The pharmacologic action of the first 3 drugs is inhibition of cholinesterase, with a resulting increase in cerebral levels of acetylcholine. 3
Peripheral cholinergic adverse effects of ChE-Is include nausea, vomiting, diarrhoea, dizziness, syncope, and even seizure that may lead to discontinuation of treatment. 4 –9 Cholinergic-dependent side-effects on cardiac rhythm are related to vagal tone stimulation. 10 Sinus bradycardia, sinoatrial block, worsening of sinus node disease, and AV block can be induced. 11 –13 These abnormalities resolve with atropine and by stopping of medication. 12 A summary of clinical trials, observational studies, and case series and reports concluded that bradycardia occurred more commonly in patients taking galantamine (2%) than patients taking placebo (1%). 14 Leentjens et al described galantamine-related AV block which caused deterioration in the clinical status of the patient. Although they did not clearly identify the relationship between galantamine and AV block, symptoms improved and never recurred after the pacemaker placement. 15 Kayrak et al demonstrated ChE-related AV block which was resolved by discontinuation of the rivastigmine and recurred shortly after the reinitiation of the drug therapy. 16 However idiopathic intermittent AV block may also occur by episodes, the rivastigmine had strong evidence to be a culprit drug in this case. Donezepil, another essential drug that slows cognitive deterioration in patients with AD, was reported by Bordier et al to cause an AV block. 17 They reported 3 patients with cardiac syncope which occurred soon after the initiation of donezepil, and the symptoms were resolved by the placement of a pacemaker despite continuation of increasing doses of donezepil therapy. 17 There is a greater risk of bradycardia in patients treated with ChE-Is, particularly those taking higher doses of donepezil. 18
Two of our cases were on AV node blocking agents during admission, which could cause an AV block. However, they had been receiving these medications for a long time and did not experience symptoms of dyspnea or syncope until the initiation of ChE-I therapy. The AV conduction response to the donezepil and galantamine therapy, in patients 1 and 2, respectively, strongly implicates the causal relationship between the AV block and ChE-Is. Administration of atropin (1 mg), by anticholinergic effect on AV node, improved AV conduction in patient 2. This had occurred despite the atenolol therapy, which supported the evidence of anticholinesterase-induced AV block. Although, the role of Ebstein anomaly on AV block is not clear in patient 2, we thought that AV block was caused by galantamine.
In patients 3 to 5, there were no risk factors contributing to AV block, except for older age. ChE-I was the only drug that could impair AV conduction in these patients. We did not test the impact of ChE-Is on AV conduction. Patient’ histories suggested that symptoms could be related to the ChE-I therapy which were attributed to the bradyarrhythmia.
Memantine is approved for treatment of moderate to severe Alzheimer's disease 19 and has now received a limited recommendation by the UK's National Institute for Clinical Excellence for patients who fail other treatment options. 2 Evidence is lacking for a benefit of memantine in mild AD, and there is meager evidence for its efficacy in moderate AD. 20 In our cohort, only case 5 had moderate to severe AD, but we did not try a memantine in that patient; it might be effective compared to the pacemaker placement. Because there is no drug therapy, except ChE-Is, that slows AD progression in mild and moderate forms, we decided to continue ChE-I therapy and implanted a pacemaker in all the patients. The outcome of pacemaker placement has had an excellent effect, and each patient experienced an improvement. Also, the disease remained stable or improved in 5 of 6 patients.
Patient 6 had coronary artery disease that could induce an AV block in addition to the older age. Because of the increased risk for dialysis we did not perform a coronary angiography. She had no complaints of chest discomfort and felt well after the pacemaker placement.
Irrespective of the accuracy of the ECG in defining the characteristics of the bradyarrhythmia, electrophysiologic study was not performed in our series. Also, the impact of ChE-Is on AV conduction was defined in only patient 1 and 2. During a follow-up in all patients the absence of recurrence of syncope after pacemaker insertion may be further evidence of causal relationship between ChE-Is and bradyarrhythmia. All patients received ChE-Is with no adverse effects during follow-up. This supported the appropriateness of continuing drug therapy, while managing the secondary bradyarrhythmias with permanent pacing.
In conclusion, AD is frequent worldwide among elderly people who have multiple comorbidities. Effective drugs for AD are few and mainly consist of ChE-Is. Patients starting treatment with ChE-Is should be screened for an increased risk of cardiac arrhythmias and routinely obtain an ECG. In case of bradyarrhythmia, a pacemaker implantation may be justified instead of drug cessation in mild and moderate AD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.