
Abstract
Background:
Peripheral arterial disease (PAD) was reported to increase the risk of dementia(s) even more than stroke. We assessed the prevalence of PAD in a group with definite diagnosis of dementia.
Methods:
Patients aged 65 years or older with Alzheimer’s disease (AD), vascular dementia (VaD), or AD-VaD were enrolled (n = 162, mean age: 78.87 [6.05] years). An age- and gender-matched control group was also included (n = 190). Peripheral arterial disease was diagnosed by the ankle–brachial index.
Results:
Frequency of PAD among patients with and without dementia was 35.2% and 16.3%, respectively (P < .001), being similar among different types of dementia. After adjustment for covariates, dementia (odds ratio: 2.41, 95% confidence interval: 1.34-4.32; P = .003) was among the predictors of PAD diagnosis along with older age, female gender, and diabetes.
Conclusions:
The prevalence of PAD was more than double in patients with dementia, with no difference among AD, VaD, and AD-VaD types.
Keywords
Introduction
The prevalence of both cardiovascular disease (CVD) and dementias increases with aging. 1 The relation of established CVD including coronary heart disease (CHD), stroke, and peripheral arterial disease (PAD) to Alzheimer’s disease (AD) and other dementias has been noted in longitudinal settings. 2,3 The risk of dementias that could be attributed to PAD was even more pronounced than CHD or stroke, 3 supporting the notion that vascular-related factors are markedly involved in the pathogenesis of AD. 4 However, although PAD is a manifestation of systemic atherosclerosis, 5 longitudinal Edinburg Artery Study 6 and Rotterdam Study 7 could not show any relation of PAD to cognitive decline, new onset of dementia, AD, or vascular dementia (VaD) after appropriate adjustments for confounders. Whether these inconsistencies can be explained by ethnicity is not clear.
A low or borderline ankle–brachial index (ABI), which is a widely used, reliable diagnostic tool to detect PAD, 8 is associated with greater systemic and lower extremity functional impairment among older adults, 9 though evidence-based preventive measures are mostly lacking. Another serious cause of progressive functional limitations among older adults is dementia, which occurs mostly due to AD, followed by VaD and/or mixed type frequently named AD-VaD. The objectives of this study were to estimate and compare the prevalence of PAD in individuals aged 65 and older with and without dementia (AD, VaD, or AD-VaD) and to explore the risk factors associated with PAD in these individuals.
Methods
Study Population
In this single-center, prospective study, participants aged 65 years or older were recruited consecutively from the geriatrics outpatient clinic. Patients with a clinical diagnosis of AD, VaD, and AD-VaD and an age- and gender-matched control group consisted of cognitively and functionally intact patients based on targeted geriatric and neuropsychological evaluation were included. Individuals who had undergone recent major surgery, resided in nursing homes, were wheelchair-bound, and/or had lower extremity amputations were excluded because of their severely impaired functioning. Patients with prior lower extremity revascularization due to PAD were excluded irrespective of their ABI values to prevent misclassification errors. Patients having mild cognitive impairment or other types of dementias including dementia with Lewy bodies, Parkinson dementia, and frontotemporal dementia; having delirium or overt neuropsychiatric behaviors; being hospitalized; and declining to participate were also excluded. Institutional review board approved the study; a written, informed consent was obtained for each participant; and the study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Working Protocol
At study entry, the basic characteristics recorded were age, gender, attained education level in years, smoking status, and comorbidities including CHD, stroke, diabetes mellitus, hypertension, hypercholesterolemia, and medications. Other unreported covariates were also reviewed through past records before enrollment. Presence of CHD was based on self-reported history of coronary revascularization, angiographic evidence of significant CHD, or a documented clinical history of myocardial infarction or unstable angina pectoris. Presence of cerebrovascular disease was based on self-reported history of stroke, cerebral hemorrhage, or small stroke/transient ischemic attack documented by hospital admission records. Self-reported history or previous records of dyslipidemia, hypertension, or diabetes mellitus were accepted positive even when the patient had never received medication or quit related medications. All participants had their weight and height measured during physical examination. Body mass index was calculated as body weight divided by height squared (kg/m2).
The cognitive function of the participants was assessed with the Mini-Mental State Examination (scores 0-30; higher scores show better cognitive skills), 10 which had previously been directly translated into local language with no major modifications. Dementia was diagnosed following the criteria of the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition), while the National Institute of Neurological and Communication Disorders and Stroke–Alzheimer’s Disease and Related Disorders Association criteria were used for the systematic diagnosis of AD. 11 The National Institute of Neurological Disorders and Stroke and Association Internationale pour la Recherché et l’Enseignement en Neurosciences criteria were used for the diagnosis of VaD. 12 Patients with dementia were classified according to type (AD, VaD, or AD-VaD). Clinical Dementia Rating (CDR) scale was used to stage the severity of dementia. 13 The Cornell Scale for Depression in Dementia was used to determine depression for patients with dementia (scores above 10 indicated depression present). 14 Geriatric Depression Scale 15 (scores 0-15; scores above 5 show depression) was used to record depression in control patients.
Measurement of ABI
The ABI was measured using the conventional method with improved facilities. 16 First, 2 metal armrests were placed under the mattress with an angle of 30° to keep the arms slightly opened. Second, arms and legs were supported under the heels and elbows with sponge rubbers of appropriate size, allowing them to be separated slightly from the surface but not exceeding the heart level. Third, 4 identical Velcro cuffs (ERKA, D-83646, Bad Tölz, Germany) were placed at the same time for easier, safe, and timely readings. Then, the readings were recorded in 2 cycles, starting from the right arm, followed by the right ankle, left ankle, and left arm using a handheld 8-MHz Doppler instrument (Hadeco Echo Sounder ES-101EX, Kawasaki, Japan). Earphones were used in case of weak sounds. The ABI was calculated based on the Trans-Atlantic Inter-Society Consensus Document on Management of Peripheral Arterial Disease II guidelines. 17 First, right and left ABI values were separately calculated by dividing the highest systolic blood pressures measured in each lower limb (arteria tibialis posterior or arteria tibialis anterior) to the highest systolic blood pressure measured in the right or left brachial artery. The lowest of the right and left ABI values recorded were considered as the final ABI value of the tested individual. The ABI ≤0.9 was used as the threshold for the diagnosis of PAD. Patients with an ABI greater than 1.40 were excluded as they may have noncompressible arteries due to medial arterial calcification.
Statistical Analyses
Continuous variables were presented as mean (standard deviation). Categorical data were described as an absolute number and a percentage of the total or either group. Nonnormal distribution was tested by the Shapiro-Wilk test. Differences between patients with and without dementia were analyzed using independent t test, χ2 test, or Mann-Whitney U test. Differences in continuous variables and categorical variables among AD, VaD, and Ad-VaD subgroups were tested by Kruskal-Wallis test and χ2 test, respectively. Spearman rank correlation coefficients were calculated in order to test linear correlations, and partial correlations were calculated by controlling for covariates. Univariate and multivariate logistic regressions were studied to identify independent variables associated with PAD, and associations at a P value ≤.10 in univariate analysis were entered in the full model. Statistical significance was accepted at P < .05. All analyses were performed using SPSS (PASW) 23.0 software (SPSS Inc, Chicago, Illinois).
Results
Study Population
The study included 352 participants, with 162 patients with dementia, mean age: 78.83 (6.14), and 190 control individuals, mean age: 78.97 (6.05). The group with dementia was matched for age and gender. Basic characteristics of patients and controls are shown in Table 1. Of the patients with dementia, 100 (61.7%) were classified as AD, 27 (16.7%) as VaD, and 35 (21.6%) as AD-VaD. Disease duration defined as time after dementia diagnosis was 25.48 (24.8) months, AD: 28.03 (25), VaD: 20.2 (24.61), AD-VaD: 22.29 (24.09), P = 160.
Sample Demographics, Clinical Characteristics, and Frequency of PAD in Participants With and Without Dementia.a
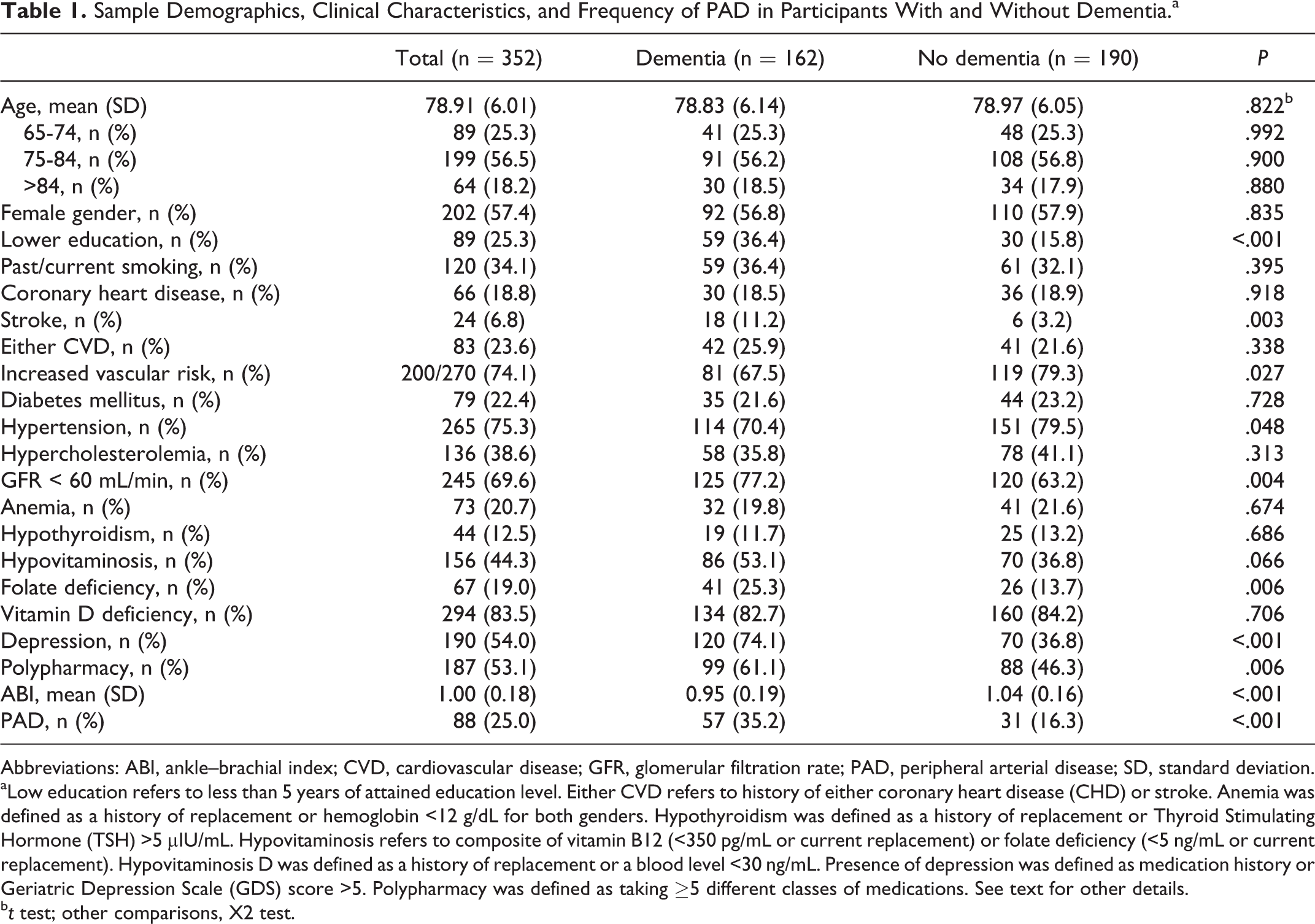
Abbreviations: ABI, ankle–brachial index; CVD, cardiovascular disease; GFR, glomerular filtration rate; PAD, peripheral arterial disease; SD, standard deviation.
aLow education refers to less than 5 years of attained education level. Either CVD refers to history of either coronary heart disease (CHD) or stroke. Anemia was defined as a history of replacement or hemoglobin <12 g/dL for both genders. Hypothyroidism was defined as a history of replacement or Thyroid Stimulating Hormone (TSH) >5 µIU/mL. Hypovitaminosis refers to composite of vitamin B12 (<350 pg/mL or current replacement) or folate deficiency (<5 ng/mL or current replacement). Hypovitaminosis D was defined as a history of replacement or a blood level <30 ng/mL. Presence of depression was defined as medication history or Geriatric Depression Scale (GDS) score >5. Polypharmacy was defined as taking ≥5 different classes of medications. See text for other details.
b t test; other comparisons, X2 test.
Dementia group had lower attained education level, decreased glomerular filtration rate (<60 mL/min), slightly lower frequency of hypertension, and higher frequency of folate deficiency, depression, and polypharmacy. History of stroke was also higher in this group, but a composite of having either CHD or stroke history was similar in participants with or without dementia. The number of participants at risk of vascular risk defined as having at least 2 of diabetes mellitus, hypercholesterolemia, hypertension, obesity, or smoking in the a Global Atherothrombosis Assessment (AGATHA) study 18 was higher in the nondemented group.
Frequency of PAD in Patients With Dementia and Controls
The frequency of a low ABI (≤0.9) consistent with the diagnosis of PAD was 25% in the whole study population. However, PAD was seen in 35.2% of patients with dementia and 16.3% of controls (P < .001; Table 1). The distribution of a low ABI was similar between genders in the dementia group, with 31.4% males and 38.0% females having an abnormal ABI (P = .382). However, males had 5% and females had 24.5% low ABI in the control group (P < .001).
As shown in Table 2, there was no difference in PAD frequency across dementia subgroups. Borderline (0.91-0.99) and normal (1.0-1.4) ABI values were also equally distributed. Mean ABI value as a continuous variable was also not different. The frequency of PAD was marginally nonsignificant across CDR stages among demented individuals, CDR-1: 31.1% (33/106); CDR-2: 37.2% (16/43); CDR-3: 61.5% (8/13) (P = .091).
Distribution of ABI Categories Across Dementia Types.
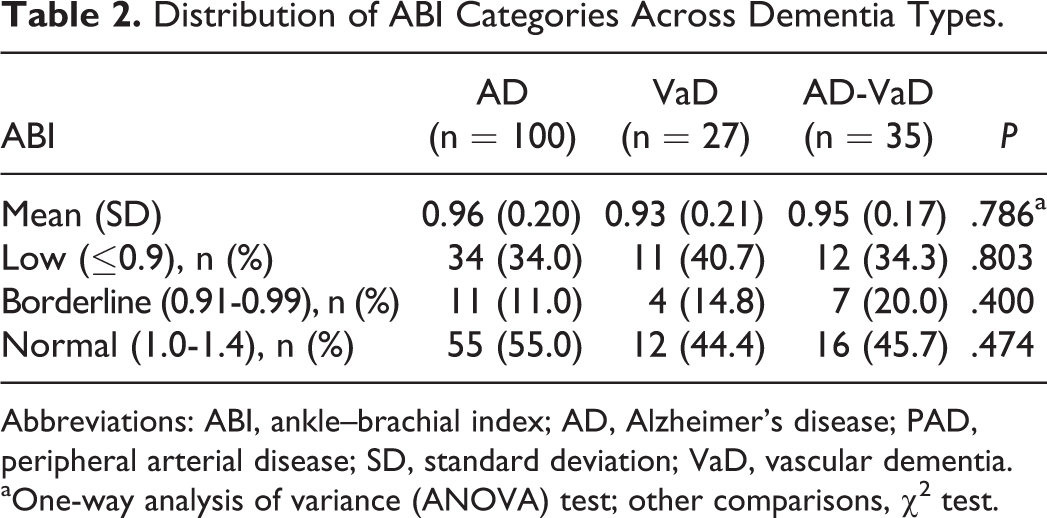
Abbreviations: ABI, ankle–brachial index; AD, Alzheimer’s disease; PAD, peripheral arterial disease; SD, standard deviation; VaD, vascular dementia.
aOne-way analysis of variance (ANOVA) test; other comparisons, χ2 test.
Patients with dementia and controls diagnosed with PAD were compared for diseases or conditions known to be associated with atherosclerotic events or cognitive decline (Table 3). Significant differences were found only in gender, history of smoking, and depression.
Percentage and Number of PAD by the Associated Risk Factors for Atherosclerosis and/or Cognitive Decline.
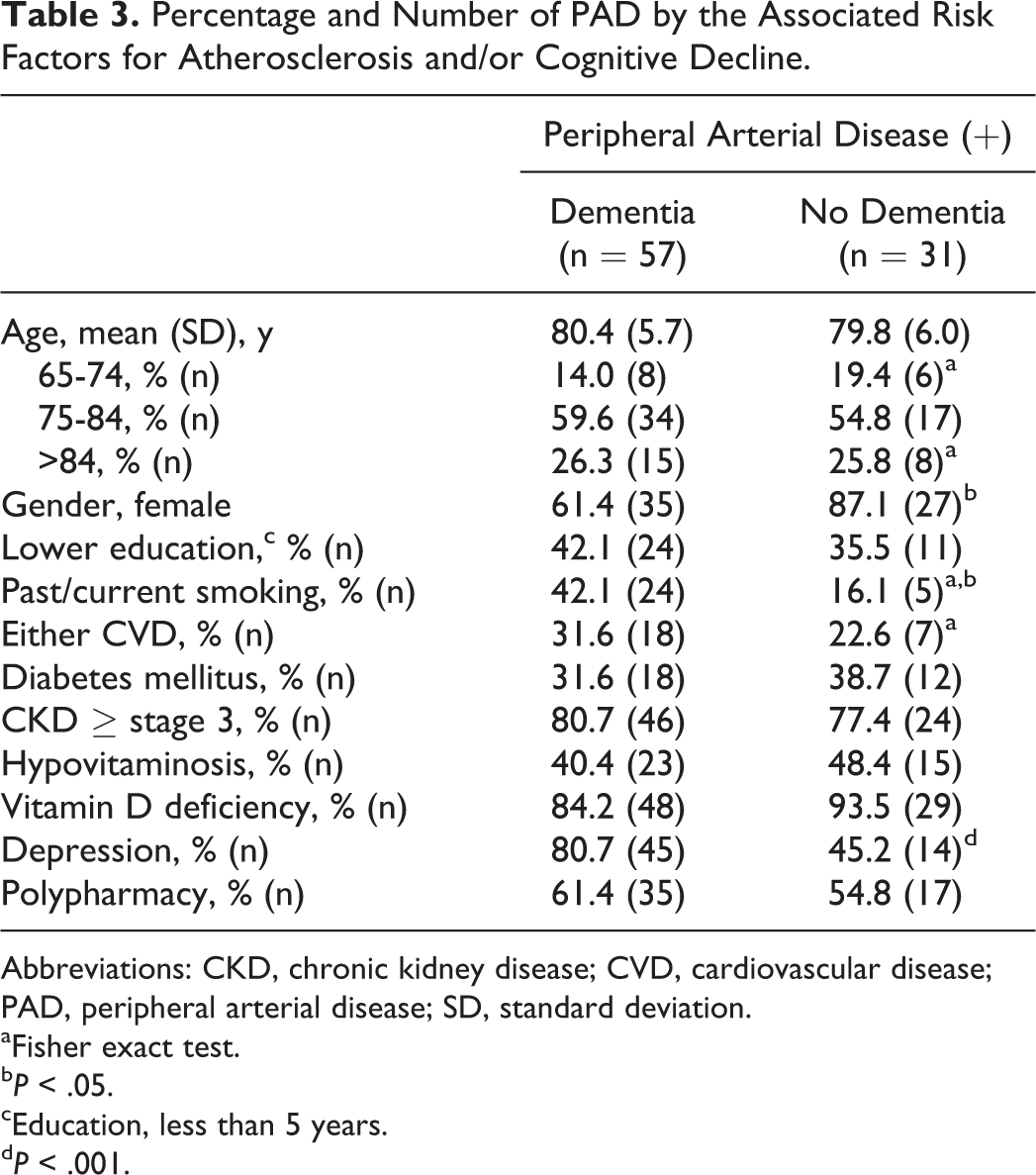
Abbreviations: CKD, chronic kidney disease; CVD, cardiovascular disease; PAD, peripheral arterial disease; SD, standard deviation.
aFisher exact test.
b P < .05.
cEducation, less than 5 years.
d P < .001.
Correlations and Dementia as a Predictor of PAD
Age was inversely correlated with ABI value in demented (Spearman ρ, r = −.209, P = .008) and nondemented (Spearman ρ, r = −.188, P = .010) patients, as well as in the whole group (Spearman ρ, r = −.178, P = .001).
Adjusted for age, ABI did not correlate with disease duration (months) neither in the whole dementia group (P = .974) nor in the subgroups. Age-adjusted frequency of PAD also did not differ by dementia duration (P = .331).
Univariate analyses showed age, female gender, lower education, diabetes mellitus, chronic kidney disease (CKD) ≥ stage 3, depression, and dementia associated with the presence of PAD (Table 4). In multivariable regression analysis, lower education level, CKD stage ≥3, and depression were no longer associated with PAD. In this final model, age, female gender, diabetes mellitus, and dementia (composite of AD, VaD, and AD-VaD) were independent predictors of PAD (Table 4). Predictors of PAD were older age (1.08, CI: 1.02-1.15, P = .010) and diagnosis of diabetes mellitus (2.63, CI: 1.2-5.8, P = .016) among patients with dementia and were female gender (6.17, CI: 1.8-21.1, P = .004) and diagnosis of diabetes mellitus (2.74, CI: 1.12-6.7, P = .003) among patients without dementia. Gender variable among patients with dementia and age variable (in years) among patients without dementia were not among the predictors of PAD in these separate multivariable analyses.
Predictors of PAD in the Whole Group.a
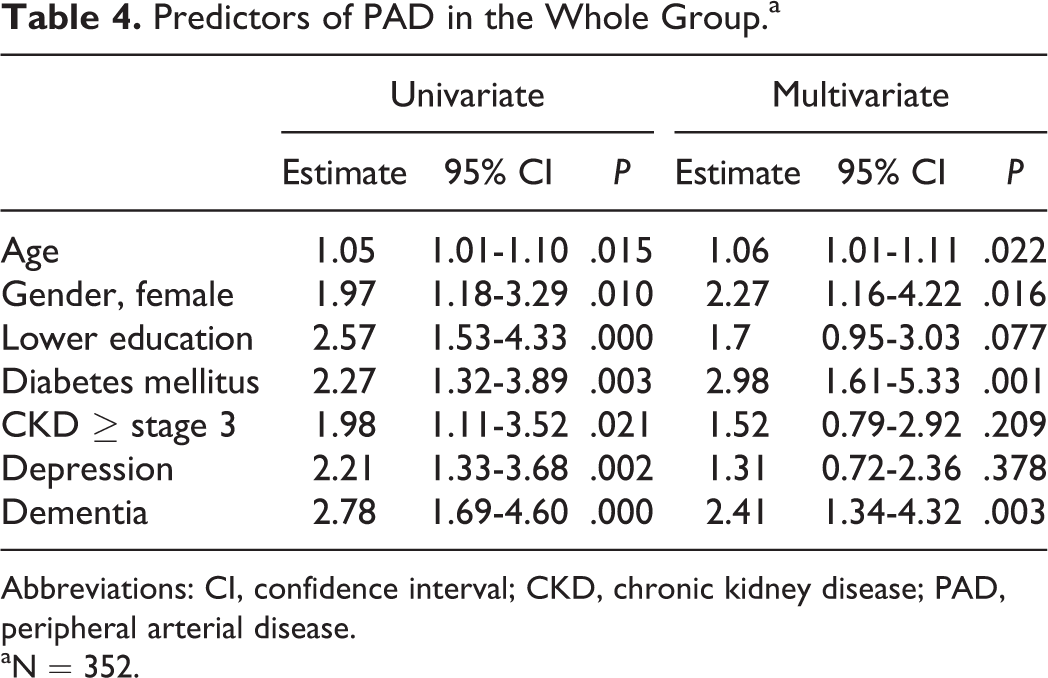
Abbreviations: CI, confidence interval; CKD, chronic kidney disease; PAD, peripheral arterial disease.
aN = 352.
Discussion
Among the participants of the present study with a mean age close to 80 years, almost a 2.5-fold increase in the risk of PAD was observed with the presence of dementia in fully adjusted analysis. One-third of patients with dementia had PAD, and the presence of any one particular risk factor or disease associated with atherosclerosis (smoking, hypertension, hypercholesterolemia, CVD, decreased renal function, and obesity) or conditions that are known to increase the risk of cognitive decline (lower education level, depression, polypharmacy, and hypovitaminosis) were not among the predictors of PAD diagnosis in this population.
Dementia is the case of true functional decline and that comorbid conditions such as diabetes mellitus 19 or vascular risk factors including systolic hypertension, angina, and atrial fibrillation 20 were associated with a more rapid deterioration of functionality. In a similar way, PAD, though silent in many individuals, 21 was also linked to decreased lower extremity functioning as well as neuropathy, mobility loss, impaired balance, global functional decline, and impaired quality of life in various trials, independent of a history of critical limb ischemia. 22 –24 Based on the results of the present study, altered functional performance in patients with dementia may also be associated with the presence of systemic atherosclerosis and/or abnormal lower extremity circulation.
Because the presence of lower extremity arterial occlusive disease is indicative of increased systemic atherosclerosis, 5 similar frequency of PAD across AD, VaD, and AD-VaD subgroups in this study suggested that these patients had similar atherosclerotic burden. Indeed, these 3 subgroups had similar frequency of CHD, stroke, any CVD, or increased vascular risk status (data not shown). 18 Although PAD was associated with a faster cognitive and functional decline independently of previous cerebrovascular disease or cardiovascular risk factors, 25 follow-up of older adults having CVD other than stroke identified that these individuals had a higher risk of dementia or AD than did those without CVD, and the risk was highest in people with PAD. 3 Presence of cardiovascular risk factors also increases the risk of future AD. 26 Thus, equal distribution of patients with PAD among AD, VaD, and AD-VaD subgroups in our study further support the notion that any of these 3 types of clinical diagnosis poses similar atherosclerotic burden.
It is not new that extensive peripheral atherosclerosis was proposed to be a risk factor for new diagnosis of AD, similar to VaD. 27 Strong evidence showed that AD and VaD share not only major clinical risk factors 28 but also some pathophysiological mechanisms. 29 Systemic inflammation that is associated with increased risk of vascular disease is also linked to neurodegenerative diseases including AD. 30 Cerebral blood flow reduces in patients with AD as a consequence of vascular disease and hemodynamic alterations, which also contributes to the mechanisms of AD development. 31 Moreover, these alterations in vascular hemodynamics in the brain occur even in the prodromal stage of AD. 32 Ischemic lesions caused by thrombi also induce AD pathology. 33 On the other hand, dementia type was AD in 62% of the patients in this study, and AD itself may trigger some mechanisms leading to vascular injury. Accumulation of amyloid beta (Aβ), a hallmark of AD in the brain tissue, impaired cerebral neurovascular regulation in experimental conditions. 34 The Aβ is also a toxic substance to the vascular endothelium. 35 It is likely that consequences of endothelial injury such as vascular smooth muscle cell activation 36 and hypercoagulopathy 37 may be associated with an increased risk of new clinical events not only in cerebral vessels but also in other vascular beds in patients with AD. 38 Indeed, a recent cross-sectional study reported an association between increased plasma Aβ concentration and presence of clinical vascular diseases including CHD. 39
Disease duration in dementia was not associated with the ABI value or PAD diagnosis in the present study. Interestingly, however, we recorded a trend toward a higher frequency of PAD in increasing dementia severity as 31.1%, 37.2%, and 61.5% in CDR-1, -2, and -3 stages, respectively (P = .091). Although only less than 10% of patients with dementia had CDR-3 disease reducing statistical power, this finding deserves attention as it may indicate more accelerated atherosclerosis in the natural course of dementias that were investigated here. More severe dementia is undoubtedly anticipated in patients with stroke-related type, but the presence of CHD was also reported to adversely influence cognitive decline in older patients with late-onset dementia. 40 Moreover, treatment of vascular risk factors was associated with a slower decline in cognitive functions in patients with AD without CVD. 41 However, with the exception of smoking and hypertension, presence of vascular risk factors at the time of dementia diagnosis was not associated with a more rapid cognitive decline in AD, 42 although these studies did not include VaD or AD-VaD. Whether more severe CVD or high number of vascular risk factors is found in advanced clinical stages of dementia needs to be further elucidated, as this may be a true case of intensive management of vascular disease in affected individuals.
Lower level of attained education was associated with the presence of PAD in univariate analysis, but the strength of association decreased in the multivariable analysis. As in the case of dementia, 43 higher level of attained education level was found to be protective of incident atherothrombotic events among older adults, with some differences by gender and income status. 44 Moreover, lower level of education was linked to increased odds of PAD in a larger study, 45 but the strength of association decreased in fully adjusted models similar to the present study. These earlier data were from a high-income population and the cutoff for attained education level was 10 years or more, whereas we used a lower but appropriate threshold for a middle-income country. We observed that inclusion of education in years as a continuous variable was inconclusive in terms of correlation with the mean ABI or PAD as a dichotomous variable. Nevertheless, our findings still suggest that, apart from age and diabetes, which are well-known predictors of accelerated atherosclerosis and dementia, 43 lower level of education and dementia may increase the risk of having PAD diagnosis.
Female gender was seen as a predictor of PAD in the present study. As women are known to be under more risk of dementia compared to men, 46 higher prevalence of PAD in women was also reported in some stuides. 47 In the present study, mean age of participants was almost 80 years and females in our control group had significantly higher proportion of PAD. However, women and men in the dementia group had equal frequency of PAD, suggesting that gender difference disappears among individuals with dementia in the case of accelerated systemic atherosclerosis.
A significant association between low ABI and cognitive impairment was previously found in cross-sectional studies. 48 Regarding dementia, a cross-sectional analysis from the Rotterdam Study reported higher frequencies of all dementia, AD, and VaD, with increasing severity of atherosclerosis as measured by the ABI and carotid atherosclerosis, with an odds ratio of 3.0 of AD. 49 Our study confirms these findings, with the addition of adjustments for prevalent diabetes mellitus, gender, and attained education level, which are well-known risk factors for atherosclerotic events as well as cognitive decline. Our findings are also in agreement with another study which reported diabetes mellitus per se caused a double increase in the frequency of PAD in individuals with dementia. 50
The present study has some limitations. First, several of medical conditions were self-reported or related information was obtained from the relatives of the patients. This might have caused underdiagnosed cases of CHD or some other conditions due to unrecognized or underreported symptoms particularly in the dementia group. Second, relation of dementia severity and PAD would be an interesting research question, but the number of enrolled patients in the VaD and AD-VaD groups did not allow separate sets of multivariable regression analyses in subgroups. Third, given the cross-sectional design of the study, the observed association of PAD with dementia and other variables cannot be assumed to be causal.
In conclusion, the current study suggests that presence of not only VaD but also AD or mixed type dementia known as AD-VaD is associated with increased odds of established systemic atherosclerosis as evidenced by the diagnosis of PAD. Although clearer evidence are required regarding the impact of cardiovascular risk reduction approaches in the prevention or treatment of dementias, screening patients with dementias including AD, VaD, or AD-VaD for PAD on a regular basis might worth benefit in terms of detecting individuals at high risk of new CVD events, where evidence-based secondary prevention measures can be applied.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.