
Abstract
Older adults with dementia have higher rates of institutionalization than those without dementia. Desire to institutionalization (DTI) is an important factor influencing the actual institutionalization but is less well studied. This cross-sectional study examines the DTI with the scale of same name developed by Morycz, in 1985, in a sample of 50 caregivers of patients with dementia in a tertiary clinical care setting in a developing country. Caregiver burden associated with personal strain (by factor analyzed Zarit Burden Interview scale), and stress perceived out of caregiving (by Perceived Stress Scale) predicted higher DTI. Besides, those who were married had lower DTI scores. The factors which didn’t affect DTI were total caregiver burden, family and social support, age of patient and caregiver, education of caregiver, severity and duration of dementia, and treatment duration. These results were different from those of developed country-based DTI studies and may indicate sociocultural differences.
Introduction
The diagnosis of dementia is an important contributor to institutionalization of older adults, with the prevalence of up to 70% in nursing home residents 1 and attributable risk of 60% for institutionalization in 3 years. 2 The rates of admission to long-term institutions rise from about 20% in first year to up to 60% in 3 to 5 years in patients with dementia. 3 Many factors starting from the sociodemographic variables to those related to the caregiver burden and finally to the presence of personal and community level resources predict the institutionalization in these patients. 3 -7
Besides the abovementioned factors, the consideration of future institutional care by the caregiver is an independent factor influencing the final institutionalization of the person with dementia. This was first proposed by Morycz 8 and was later supported by others. 4,5,9 The placement of the elderly patients relative to a long-term residential care setting by caregiver is actually a process rather than single step and does involve contemplation, gradually moving toward the final decision. 10 This is labeled as desire to institutionalization (DTI) and probably governed by the same model which explains the actual institutionalization (AI). 3,8 According to Luppa et al, 3 the variables affecting institutionalization can be classified into 3 main groups. Sociodemographic and relationship characteristics of patients and caregivers come under predisposing variables; dementia-related aspects and caregiver-related aspects (both primary and secondary perceived stressors) come under need variables; resources in the form of personal and social ones and available community-based care including short- and long-term care come under enabling variables. However, the degree to which the variables of this model influence DTI may not be the same as that in AI. The understanding of DTI and its associated predictors might also help us to predict the future AI and give us opportunity to work on other variables influencing AI.
Unfortunately, many studies assessing AI 3 had ignored DTI. Further, there are very few studies those have tried to assess predictors of DTI. The variables significant in these studies were more related to psychosocial factors such as caregiver burden, potentially harmful behavior of caregiver, nonspousal status of caregiver, family dysfunction, and poor social support. 11 -13 McLennon 14 studied the themes behind the process of institutionalization in a qualitative manner and found that the anticipation of inevitable complications by the caregiver and current feelings of reaching to their limit of caregiving were the 2 prominent themes.
The studies exploring DTI are not only limited in number but are also restricted to developed countries. Dementia in developing countries differs in aspects which can have substantial impact on DTI as well as AI. The prevalence of dementia based on Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) criteria in India and other developing countries remained quarter to half of that in European countries 15 -17 unless the diagnosis was made with a different protocol, which took care of clinical variability in developing countries. 16,18 Another distinguished aspect is the misinterpretation of behavioral and psychological symptoms in dementia by caregivers in India as patient’s deliberate behavior, and in turn, leading to perception of greater distress by these caregivers. 19 Such perceived caregiver burden becomes further high due to culture-based feeling of caregiving as responsibility. The financial burden due to unavailability of insurance or government monetary support and absence from the job is more typical in developing countries and adds to the agony. 20,21 The shortage and high costs of long-term residential facilities for elderly patients 22,23 increases further the dilemma of institutionalization and thus are likely to influence DTI.
In short, DTI is an important aspect in the process of AI and can vary in its prevalence and predictors with variation in the presentation of dementia and caregiving aspects. These matters do get influenced by psychosocial and cultural factors. There is a need to determine whether the findings of conducted studies for DTI in developed countries hold true for developing countries like India as well. Hence, we planned to study DTI in the background of stress and burden in caregivers of persons with dementia, who seek treatment from a geriatric neuropsychiatric clinic.
Methods
Participants
The participants were 50 caregivers of patients having dementia who visited geriatric neuropsychiatric clinic in a tertiary care hospital. The diagnosis of dementia was made by the treating clinician based on DSM-IV. 24 The duration of dementia was at least 1 year. These caregivers had been staying with the patient for last 6 months at least, were actively involved in the treatment of the patient, were aged 18 years or older, and gave informed consent for participation. Neither the patient with dementia nor the caregiver nor other family members staying with them had any major neurological/psychiatric illness including traumatic brain injury, cerebrovascular accidents, Parkinson disease, schizophrenia, and other psychotic disorders, schizoaffective disorder, and bipolar affective disorder. The other medical illnesses which would cause significant disability were also ruled out. This was ensured to avoid an additional burden of care. The absence of these illnesses was ascertained by treating doctor through history, by examination, and by reviewing available medical records. There were no specific criteria or questionnaire used for determining disability. The study was approved by the institutional ethics committee.
Procedure and Instruments
The study was cross-sectional in nature. Caregivers of patients having dementia were recruited if inclusion/exclusion criteria were met and they provided informed consent. Information was collected in a single visit. We conducted semistructured interview of caregiver (participant) for collecting sociodemographic details of them and their patient and details of their patient’s illness. This was followed by administration of structured instruments to assess the severity of dementia and stress, social support, and burden felt by the caregiver. Finally, the participants were asked through structured questionnaire about their desire to institutionalize their relative (patient). In case of self-reported assessment instruments, the English version was used by the interviewer and translation of the scale in the appropriate vernacular version was provided to individuals who were not fluent in English. All instruments used in this study are described below. Clinical Dementia Rating Scale (CDRS): Its updated version by Morris
25
is widely used for global measurement of severity of dementia. It has 6 domains: memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care, yielding a global CDR score which can be interpreted as questionable, mild, moderate, or severe dementia. It was administered here by the doctor as a part of routine clinical protocol. Perceived Stress Scale (PSS)
26
-28
: It is a self-reported questionnaire intended to measure the degree to which situations in one’s life are considered stressful, comprising events that may cause strain.
26
Here, we used 10-item revised version of the scale,
27
which taps negative and positive psychological states
28
that are present during stress. It contains 6 positively worded “stress” items and 4 negatively worded “counter-stress” items. Items are rated on a 5-point scale of occurrence over the past 4 weeks (0 = never, 1 = almost never, 2 = sometimes, 3 = fairly often, 4 = very often). In scoring the measure, the 4 positive items are reverse scored, and then, all the items are summed (ranging from 0-40). A higher total score indicates greater stress. Multidimensional Scale of Perceived Social Support (MSPSS)
29,30
: This measure is composed of 3 specific dimensions of perceived sources of social support—the family, friends, and significant others. Each dimension is designed to assess (a) perceived availability of support and (b) function of the support. The final version
29
retained 12 items. Each revised MSPSS subscale is made up of 4 items, and the response options are scored from 1 (very strongly disagree) to 7 (very strongly agree). Responses to items within each of the subscales are summed to derive a total subscale score. Scores on all 12 items are summed to obtain a composite MSPSS scale score (ie, global perceived social support). A higher total score on subscale or whole scale indicates high levels of perceived support from that source or as a whole, respectively. Zarit Burden Interview (ZBI)
31
: It is a 22-item self-report inventory that examines burden associated with functional/behavioral impairments and the home-care situations. The items are worded subjectively, which helps to focus on affective responses of the caregiver. Each item is scored on a 5-point Likert scale ranging from 0 (never) to 4 (nearly always present). Total scores range from 0 (low burden) to 88 (high burden). The 11 of 22 items of ZBI are considered for further division of burden to that caused by personal strain (7 items) and role strain (4 items)
32
in this study, total ZBI score, ZBI-personal strain, and ZBI-role strain were calculated. Desire to institutionalization
8
: The desire to institutionalize was measured with this 6-item self-report measure developed by Morycz.
8
It quantifies stages in considering nursing home placement, ranging from discussion with family about nursing home placement to actually have taken steps toward nursing home placement by eliciting the caregiver’s thoughts and intentions over the past 6 months. All items are scored using a 3-point Likert scale: yes; often (3); yes, now and then (2); no (1) with a higher score reflective of a greater desire to institutionalize. The maximum score is 18.
Data Analysis
Descriptive statistics were used for patient-, caregiver-, and illness-related variables and scores of the assessments done. The relationship of DTI score to the continuous variables was assessed initially using Pearson bivariate correlation test. For the relationship of DTI to the categorical variables, Mann-Whitney U and Kruskal-Wallis tests were used as they had nonparametric distribution. A hierarchical stepwise multiple linear regression analysis was performed after conducting collinearity diagnostics (ie, tolerance, variance inflation factor). The DTI score was considered as the dependent variable, and significantly correlated categorical variables (along with dummy coding/variables) were placed individually as independent variables in the earlier blocks and significantly correlated continuous variables as independent variables together in the last block. The level of significance was considered as (P < .05).
Results
Sample Characteristics
The relevant sociodemographic profiles of the caregivers and their patients are presented in Table 1. Clinical Dementia Rating Scale ratings revealed mild dementia in 24 patients, moderate in 18 patients, and severe dementia in 8 patients, corresponding to 48%, 36%, and 16% of the sample, respectively. The mean duration of illness was 3.04 ± 2.58 years, and mean duration of caregiving was 2.62 ± 2.08 years. The mean duration of treatment was 2.14 ± 2.11 years.
Sociodemographic Profile of Caregivers and Patients.
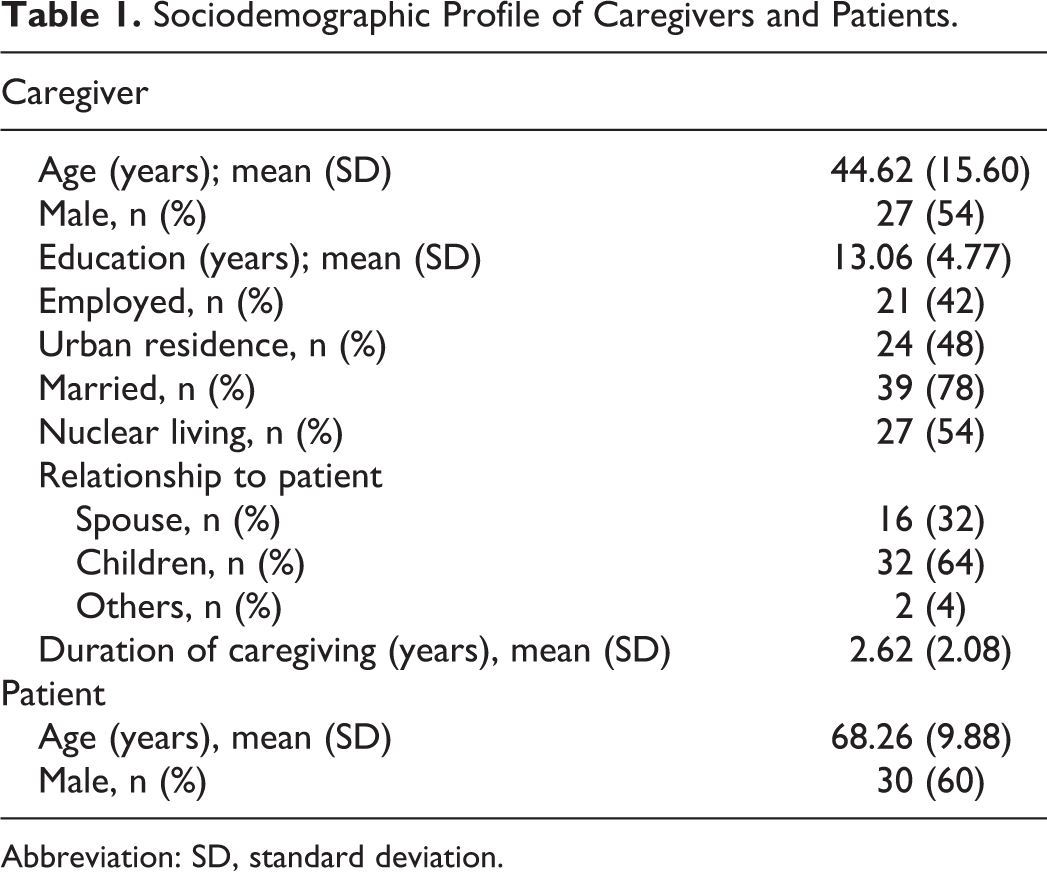
Abbreviation: SD, standard deviation.
Distribution of Scores of DTI and Measures of Caregiving
Desire to institutionalization score varied between 6 and 18 with the mean of 8.02 ± 2.68. Twenty-two caregivers (44% of the sample) had score of 6 indicating no DTI. The mean rating of PSS was 19.38 ± 5.30 and that of MSPSS was 56.72 ± 17.82. Among subgroups of MSPSS, caregivers perceived maximum support from family with mean of 22.56 ± 5.85. The supports perceived from friends and social circle were similar with mean of 17.06 ± 7.45 and 17.01 ± 7.44, respectively. The mean score of ZBI was 36.28 ± 16.37. Here, the mean score of burden due to personal strain was 11.18 ± 5.82 and that due to role strain was 6.7 ± 4.03.
Association and Predictors of DTI
Among continuous variables, ratings of PSS, total ZBI score, and ZBI personal were significantly correlated with DTI score (Table 2). Age of the caregiver, education of caregiver, age of the patient, duration of illness, duration of treatment, duration of caregiving, MSPSS total and various subgroups of MSPSS, and ZBI role were not associated with DTI (Table 2). Among categorical variables, only marital status was significantly (P = .038) associated with DTI score with mean DTI in married caregivers group as 7.67 ± 2.46 and that in single/separated caregivers group as 9.27 ± 3.16. Desire to institutionalization scores did not significantly vary between the groups based on gender, occupation, residence (rural versus urban), type of family, and the caregiver’s relationship with the patient. Similarly, we didn’t find any relationship between the severity of dementia and DTI scores. The comparisons of DTI scores among various subgroups of categorical variables are shown in Table 3.
Pearson Correlation Analysis for DTI and Continuous Variables.
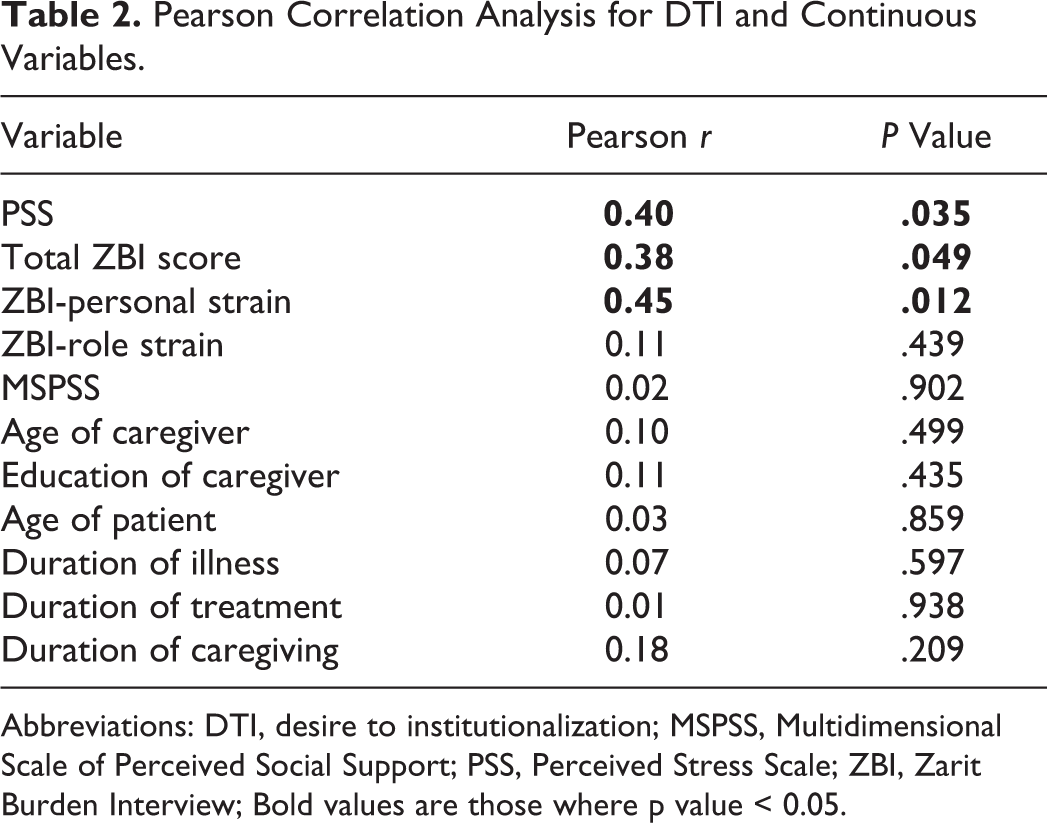
Abbreviations: DTI, desire to institutionalization; MSPSS, Multidimensional Scale of Perceived Social Support; PSS, Perceived Stress Scale; ZBI, Zarit Burden Interview; Bold values are those where p value < 0.05.
Analysis of DTI Scores in Categorical Variables.
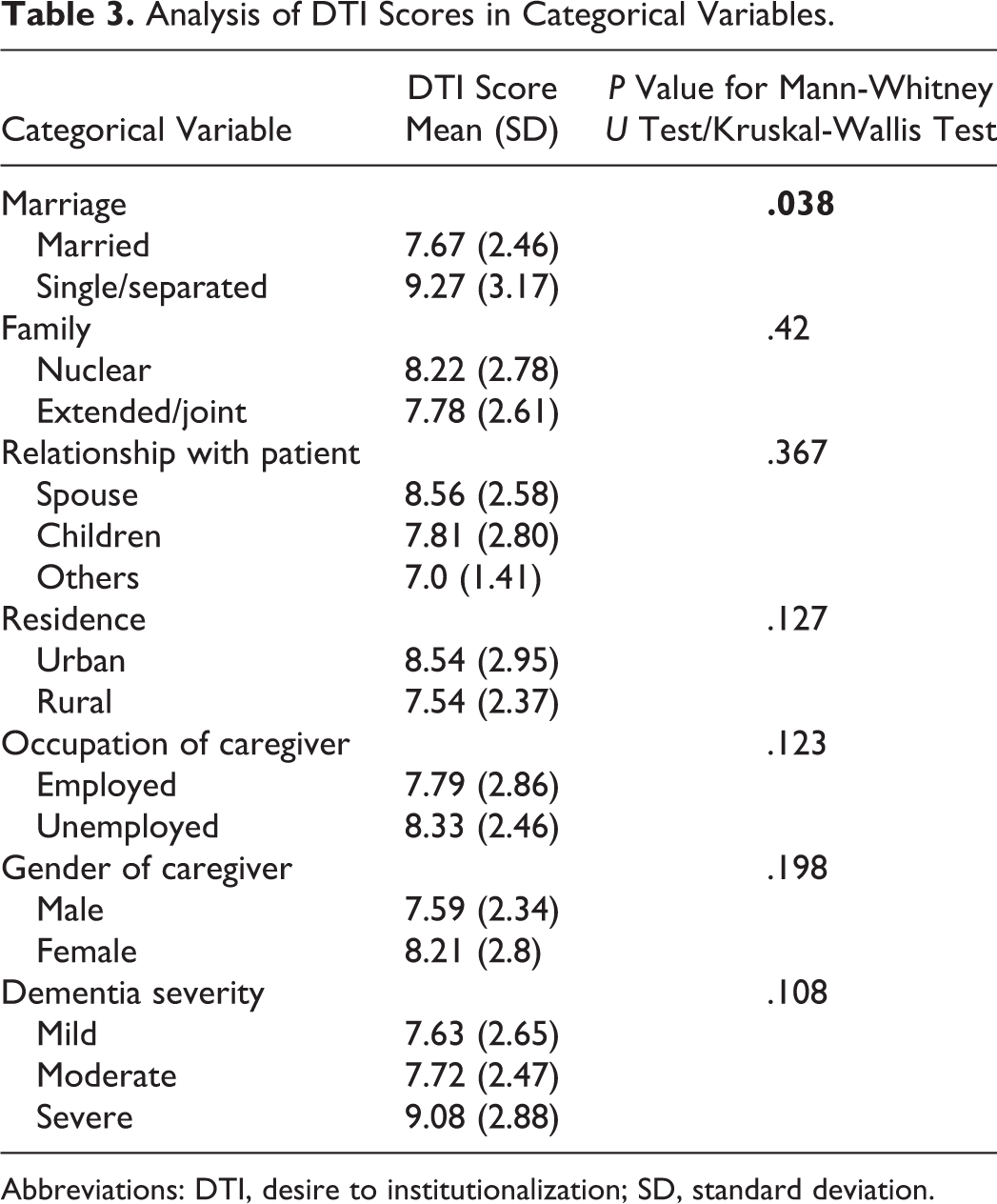
Abbreviations: DTI, desire to institutionalization; SD, standard deviation.
Further, hierarchical stepwise multiple regression analysis was performed. It was carried out in 2 blocks with first block containing categorical variable, marital status. The second block included PSS, total ZBI score and ZBI personal as independent variables. In this analysis, PSS, marital status, and ZBI-personal strain came as significant predictors (Table 4). The R 2 of this model was 0.261, thus explaining the 26% of the variability of the DTI score around its mean. The part correlation of ZBI-personal strain and PSS was 0.319 and 0.221, respectively.
Predictors of DTI With Regression Analysis.

Abbreviations: DTI, desire to institutionalization; PSS, Perceived Stress Scale; ZBI, Zarit Burden Interview.
Discussion
Many caregivers face more stress and depression after AI of their patients with dementia and felt if somehow AI could have been delayed. 33,34 In this context, DTI is an important stage in the caring. Intervention at this stage can help delaying and smoothening the process of AI. Studies have shown DTI to be an important predictor of AI. Our study on the factors associated with DTI would help in identifying and predicting DTI and thus initiating focused involvement of health professionals at the stage of DTI. This study becomes more important being the first study of DTI in India and gives the perspective of developing countries. Further, many Indian experts and people don’t favor AI as the culture promotes guilt feelings in caregiver if AI is planned. 23,35 In addition, the opinion is of increase in mortality in patient after AI. 36
The sample size (n = 50) of this study was lesser to that in earlier studies assessing DTI (n = 70-84) 5,11,12 and was an important limitation. At the same time, the DTI-based studies which had sample size in 100s were secondary data analysis of a different study. 4,13,37 In our study, 44% (n = 22) of the sample didn’t express DTI, which matches to the proportion (40% to 50%) found at other places. 11,12 We had mean age of caregivers as about 45 years and 54% of them were males. In contrary, previous studies had 60% to 80% of them as female caregivers and the mean age crossed 60 years. 12,13,37 This might be because the spouse was the primary caregiver in majority cases of these studies, where as we had only 32% (n = 16) of cases with spouse as caregiver. It illustrates the cultural difference between developed countries and developing countries like India. Children often consider themselves responsible for caregiving as much as the spouse of patient with dementia in Indian culture. 5,21,38,39 The level of caregiver burden (mean ZBI score = 36.28) was similar in our and previous studies. 11,12,19 We couldn’t compare our score of ZBI-personal strain, the significant predictor of DTI in our study since this measure was not used in earlier studies.
We got total ZBI score, ZBI-personal strain, PSS, and marital status as the significant variables correlated with DTI scores during univariate analysis (Tables 2 and 3). However, multiple regression analysis excluded total ZBI score. ZBI-personal strain was most prominent predictor (Table 4). Increase of ZBI-personal strain score by 5.82 (1 SD of this sample = 5.82; maximum possible score = 44) could increase the DTI score by 1.33 (0.51 times SD of DTI), which was ahead of the other 2 significant predictors (being married and higher score of PSS). Thus, personal strain component of caregiver burden contributed much more than role strain burden in initiating thoughts in caregivers of this study population about institutionalizing the dementia-care recipients.
Ours is the first study which used the factor structure of ZBI to study DTI. This becomes more important since in our study, the caregiver burden as a whole didn’t influence DTI, but ZBI-personal strain did. We used the factor analysis performed in acquired brain injury 32 instead of available factor analysis of ZBI in patients with dementia. 40 -42 This is because Siegert 32 applied Rasch model after usual confirmatory analysis, which improved the objectivity of the final interval scale and removed the items with inconsistent responses. The factor analysis done in dementia patients in different studies have so much variability that it is difficult to fit to other samples. 43 Further, many of them used abridged 12-item ZBI scale for factor analysis. 40,41
The other 2 variables which predicted DTI in this sample were marital status and perceived stress. Although they had lesser impact, they indicate the other dimension of caregiving of patients with dementia. Those who were married had less of DTI score by an average of 1.61 compared to those who were not. The married population (n = 39) comprised both of patient’s spouse as caregivers (N = 16) as well as those who were children or other family members of patient and were married (n = 23). Hence, it probably signifies the significance of both intimate relationship with the patient (in case of spouse as caregiver) and sharing of role and stress of caregiving of the patient with their own spouse (in case of child or other family member caregiver), which reduces the DTI. However, these two factors related to marital status were not enough on their own to influence DTI more than their counterparts. That may be one of the reasons why neither the relationship with the patient nor the family support was a significant predictor of DTI.
The effect of perceived stress (as measured by PSS) on DTI came down from univariate (r = 0.398) to multivariate analysis (part r = 0.221). This might be because of possible contribution of caregiver burden by personal strain on the correlation between perceived stress and DTI. Burden due to personal strain indicates the emotional and subjective stressful part of caregiving experience, which is then felt as the burden. 44 Nevertheless, the caregiving stress did contribute to caregiver’s preference to institutionalization of relative having dementia irrespective of whether they could cope or not with the stress to take it as the burden or not. This might be due to obtained higher PSS scores (19.38 ± 5.30) similar to those in patients with cancer. 28
As discussed earlier, family-based caregiving of patients with dementia is quite prominent in countries like India, probably due to the culture which considers taking care of your spouse, children, and your parents as your responsibility rather than optional out of love. 38,39 Lack of long-term residential care for elderly patients with dementia in developing countries further increased the necessity of home-based care. 22,23 The compulsive situation can generate more emotions and subjective frustration, which are sincerely tapped by ZBI-personal strain. Thus, our results indicate that this personal stressful feeling of caregiver burden which may be high and more troublesome in countries like India gives way to thought about institutionalization of patients with dementia. On the contrary, caregiving of patients with dementia has greater component of choice than obligation in developed countries, and the availability of nursing home-based care is better. Hence, the feeling of inability to take adequate care of patient and causing harm possibly may prompt caregiver to look for option of long-term institutionalization. They may not wait for upsurge of personal stressful emotions. 14 This concept has its roots in stress process model proposed by Pearlin. 45 Role of culture and caregiving beliefs–practices in predicting DTI for dementia family was explained using the same model in a recent study. 13
As reflected in our study, previous studies have also found caregiver burden as an important predictor for DTI. 11,12 However, none of the earlier studies looked specifically into the personal strain component of the caregiver burden. But a qualitative study assessing the process of institutionalization found the major theme as the either anticipating or current feelings that they are not able to fulfill various demands of caregiving. 14 This seems to go more with burden due to role strain than personal strain. Some of the other predictors that were significant according to earlier studies but were not in the current study are nonspousal status of caregiver, 11 less social support, 12 and gender. 37 We didn’t note any significant association between DTI and total MSPSS or its components pertaining to family, friends, or significant others. We also didn’t find the effect of severity of dementia as measured by CDRS on DTI although it is shown to be associated with AI of patients with dementia. 3 It is difficult to hypothesis the reasons for these differences at this stage. More similar studies in India and other developing countries in the future may give us clearer picture of the role of cultural and regional factors in DTI and whether the found disparity is secondary to methodological variations. Further, the difference in findings might also due to different demography and illness features (higher proportion of mild/ moderate dementia, shorter duration of illness and caregiving, lesser mean age of patients) of our study compared to earlier studies, which again may have influence by cultural aspects.
There were also some factors which were positive predictors in previous studies but were not assessed in our study such as depression in caregiver, 11 quality of premorbid relationship, 37 current relationship 5 between caregiver and patient, and knowledge about dementia. 12 This was an important limitation of our study. We also didn’t assess other possible predictors such as coping strategies used by caregivers and behavior and psychological problems associated with dementia in the patients. Besides, the cross-sectional nature of this study does preclude knowing about how the positive factors influence DTI over the course of time and how do they correlate to the later outcome of institutionalization. We also don’t know at this stage whether addressing these factors and reducing their impact would affect DTI and AI or not. Finally, the usage of English version of self-reported scales for non-English-speaking participants should also be considered as the limitation of study. Here, the translation to the vernacular language was provided to the participants by interviewer without going through the whole process of validation of translated scale. This was done mainly because of time constraints.
To conclude, this study has focused into determining factors of DTI in patients with dementia, which is also thought to be a stage of intervention to delay AI and improve home-based caregiving. We found caregiver burden depicting personal strain as most important predictor for DTI followed by marital status and perceived stress. The results of our study might have been influenced by culture and inadequate availability of dementia-care facilities in India and thus warrant further similar studies to be conducted in India and other developing countries.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.