
Abstract
Background:
Previous research shows that informal caregivers of individuals with a memory disorder experience financial strain, declining physical health, and psychological distress. Various resources and services have been developed to address and/or prevent these potential outcomes, yet caregivers continue to be negatively affected by the demands of caregiving. We hypothesize that better identification and clarification of concrete patient and caregiver needs will aid in the modification and improvement of the available resources. The purpose of this study is to determine the psychosocial needs of the cognitively impaired population and their caregivers.
Methods:
A one-page Needs Assessment was created to address areas of potential concern for the individual with a memory disorder and the caregiver. This assessment was administered during visits to an outpatient clinic in Philadelphia.
Results:
A total of 204 Needs Assessments were collected. The significant needs found in our study cohort include sleep, exercise, clinical trials, education, and assistance with ADLs and IADLs.
Conclusions:
This study satisfied the initial identification of caregiver and patient needs; now each must be explored further to determine how to successfully meet such needs. If the primary needs of the patient can be met by a focused service, the caregiver will no longer be the sole provider of meeting the specific need. This will decrease the involved role of the caregiver, maximize patient homecare, minimize caregiver stress, and increase the quality of life for both the patient and caregiver.
Introduction
Dementia is a term used to describe a loss of mental abilities that is severe enough to impact daily functioning. This includes memory loss, learning difficulties, language, orientation, judgment, and comprehension problems. 1 The clinical presentation of dementia can be caused by a variety of different pathologies. Alzheimer’s disease (AD), cerebrovascular disease, several frontotemporal pathologies, and Lewy bodies are examples of pathogenic causes. Of these, AD is the most common dementia subtype. 1,2
Alzheimer’s disease is the 6th leading cause of death in the United States. 3 In 2010, it was estimated that 4.7 million adults aged 65 and older were diagnosed with AD nationally. 4 Due to the aging population, this number is expected to increase to 13.8 million by 2050, unless advancements are made to slow the progression or treat the disease. The cost of care for AD and dementia is currently 203 billion dollars and is estimated to increase to 1.2 trillion dollars in 2050. 2 This staggering financial cost places strain not only on the economy but also on the caregiver responsible for caring for the individual with dementia.
Contrary to popular belief, the caregiver of an individual with dementia is typically a family member in the home rather than a professional caregiver in a long-term living facility. 5 According to the 2009 World Alzheimer’s Report, “[informal caregivers] are the cornerstone of the system of care and support.”1(p48) In 2012, 15.4 million informal caregivers provided 17.5 billion hours of unpaid care to their demented loved one, resulting in 216.4 billion dollars of unpaid care. 2 In addition to this financial strain, caring for a person with dementia also causes the caregiver to experience physical and emotional burdens.
Greater than one-third of caregivers have poor health themselves while providing continual care to an individual with dementia. 6 In 2012, caregivers of individuals with dementia added 9.1 billion dollars in health care costs, likely due to the lack of prioritizing personal medical care. 2 There is a positive correlation between increased stress, increased depressive symptoms, and increased age of the caregiver. 7 Changes in behavioral symptoms (agitation, sleep disturbance, wandering, and apathy) and psychological symptoms (anxiety, depression, delusions, and hallucinations) of the patient typically have the most impact on caregiver strain. 1,8 The emotional impact of caregiving (loneliness, isolation, and anger) also significantly contributes to the burden experienced by the caregiver; meta-analyses indicate 40% to 75% of caregivers experience psychological distress and, also, a 15% to 32% prevalence of a major depressive disorder. 9,10
The strain and burden of caregiving have been recognized, which is evident by the presence of day programs, respite care options, and federal and local organizations. 11 Regardless of these resources, caregivers continue to feel and be affected by the strong demands associated with caring for an individual with dementia. This may be because the services are understaffed, underfunded, and not proportional to demand, or, because the programs that are in abundance do not necessarily meet all of the caregiver needs. 11
We hypothesize that better identification and clarification of concrete needs will aid organizations in the further development of their respective programs, resulting in efficient, reliable, and focused resources. This will also further our understanding of how to better serve our local patient population, ultimately maximizing patient home care and minimizing caregiver stress. In order for the needs of the caregiver to be met, patient need must simultaneously be identified. If the primary needs of the patient can be met by a focused resource, the caregiver will no longer be the sole provider of meeting the specific need. This will decrease the involved role of the caregiver and the overwhelming burden the caregiver is experiencing. The purpose of this study is to determine the psychosocial needs of the cognitively impaired population and their caregivers through the administration of a Needs Assessment Survey.
Methodology
Clinical Site
Data were gathered from patients and caregivers during outpatient visits to the Memory Disorders Program at Drexel Neurological Associates, affiliated with Drexel University College of Medicine, in Philadelphia, Pennsylvania. The Memory Disorders Program provides care to patients with a variety of neurodegenerative diseases, including AD, dementia with Lewy bodies, frontotemporal dementia, vascular dementia, dementia of mixed etiology, mild cognitive impairment, and hydrocephalus. The clinical site is located in an urban area and is also an academic center. In addition to patients from the Philadelphia area, referrals come from the entire tristate area. The protocol and supporting documents were approved by Drexel University’s Human Research Protection Program and the institutional review board.
Needs Assessment and Mode of Administration
We developed our Needs Assessment survey to assess the psychosocial needs of patients with memory disorders and their caregivers. The assessment was in the form of a one-page questionnaire. This format was utilized in order to prevent overwhelming the patient and caregiver with an intimidating form and to evaluate the overall situation in a concise manner. The content included in the questionnaire addressed areas of potential concern, including the care network, living situation, safety, physical state, level of independence, activities of daily living (ADLs) and instrumental activities of daily living (IADLS), caregiver education, and available resources and services. The aforementioned areas of focus were chosen based on the principal investigator’s knowledge as a memory disorder physician, the coauthor's experience as an AD caregiver education specialist, findings in the available literature, and topics of concern expressed by caregivers and patients. The Needs Assessment was completed at the patient appointments and in a private room with the patient, caregiver (when present), and research coordinator (KB). When the level of cognition was a limitation, the caregiver acted as a proxy on behalf of the patient with impairment. The Needs Assessments were physically completed by either the patient or the caregiver or both depending upon the cognitive limitations of the patient. The Needs Assessment included the language “you” or “your,” which referred to the patient with memory disorder, regardless of who completed the questionnaire. A total of 204 Needs Assessments were collected for this study.
Data Capture Method
Once the form was completed, additional information from the electronic health record was recorded. Demographic data, including age, race, and ethnicity, as well as medical diagnosis, Mini-Mental State Examination (MMSE) score from 0 to 30, 12 and who completed the form, were documented. IBM SPSS Version 20 was the software used for statistical analysis. Descriptive statistics were obtained to derive the respective frequencies and percentages for each response to the Needs Assessment questions.
Results
Respondent
In the present cohort, 33% of the Needs Assessments were completed solely by the patient who demonstrated the ability to comprehend and respond to each question, 38% of the Needs Assessments were completed as a group with the patient and present caregiver, and 29% were completed strictly by the caregiver.
Demographics and Living Situation
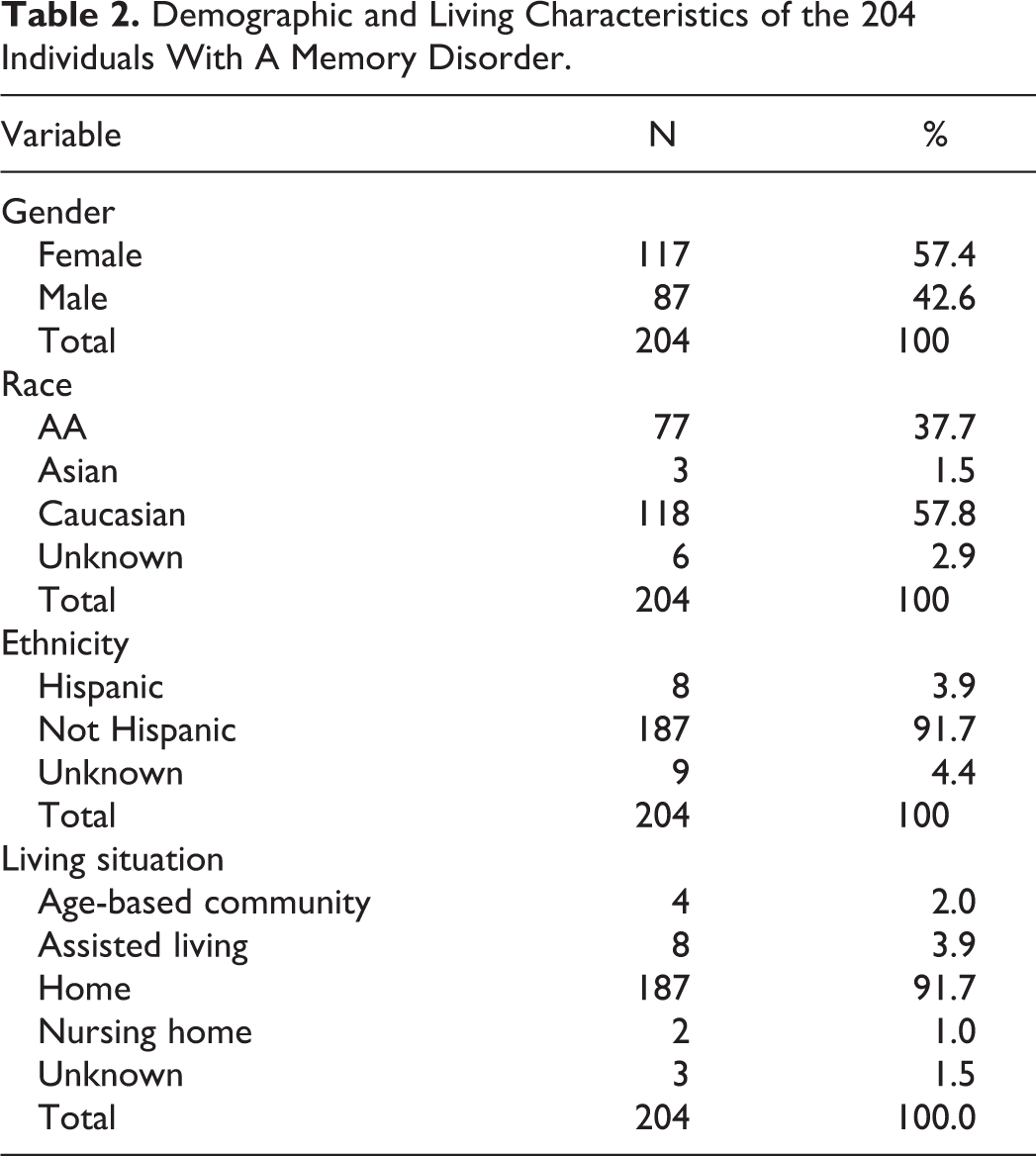
Demographic data were collected to determine the profile of the patient pool. The average age of the participants was 69, with a range of 25 to 97 years of age (Table 1). Females accounted for 57.4% and males accounted for 42.6% of the study population (Table 2). Race and ethnicity were as follows: 57.8% white, 37.7% African American, 1.5% Asian, and 2.9% unknown; 91.7% not Hispanic, 3.9% Hispanic, and 4.4% unknown. Regarding the description of the living quarters of the individual with dementia, 91.7% of patients lived at home, 3.9% in assisted living, 1.0% in a nursing home, 2.0% in an age-based community, and 1.5% unknown (Table 2).
Distribution of Ages Among Those With A Memory Disorder in the Present Study.
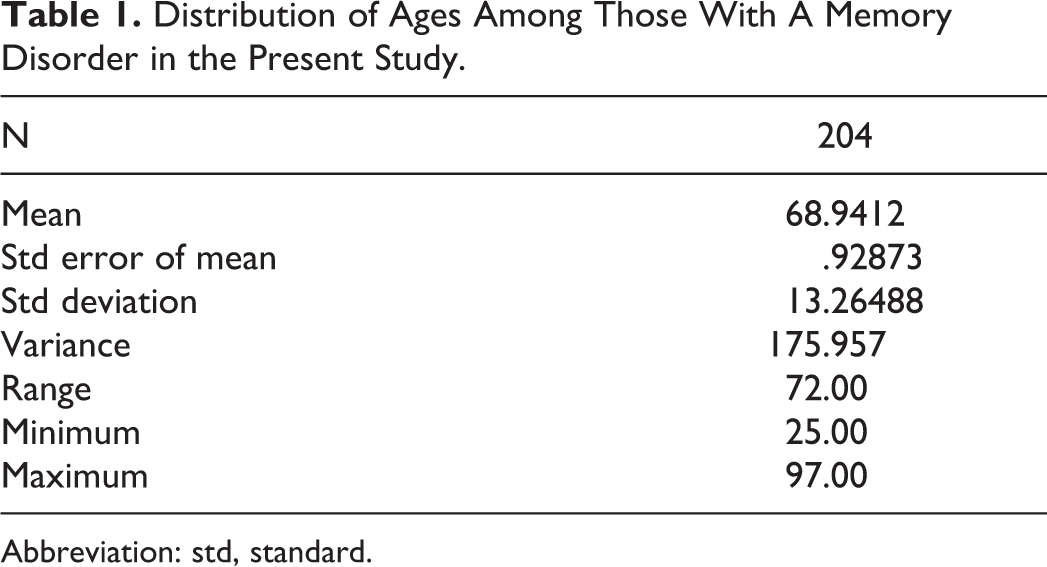
Abbreviation: std, standard.
Demographic and Living Characteristics of the 204 Individuals With A Memory Disorder.
Care Network
We explored the formal (ie, home health aide, skilled nursing, and nonskilled companion) and informal (ie, family, spouse) care network of the population and found 15.76% received formal aide, while 84.24% did not. In terms of informal caregivers, 71.6% of patients had an informal caregiver and 28.4% did not (Table 3). Individuals with an informal caregiver either had 1 primary caregiver type or a mix of caregiver types who shared equivalent care time. Of those who had a single type of caregiver, 27.9% of caregivers were family members, 29.9% were the spouse of the individual with dementia, and 1.5% identified as “other.” In addition, complex care networks of greater than 1 type of caregiver existed; 8.8% of patients with caregivers were cared by the family and a spouse, 2.9% by the family and other, and 0.5% by a spouse and “other.”
Description of the Informal Care Network.a
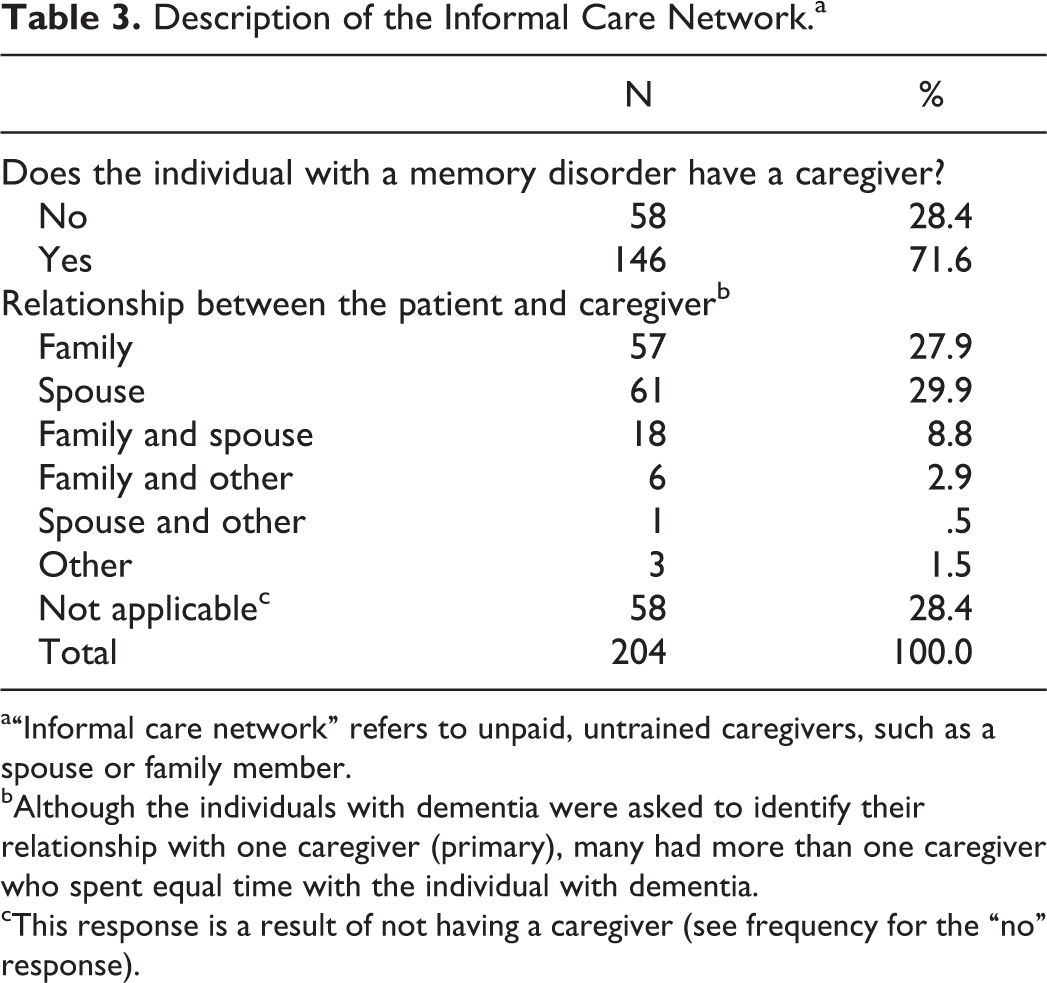
a“Informal care network” refers to unpaid, untrained caregivers, such as a spouse or family member.
bAlthough the individuals with dementia were asked to identify their relationship with one caregiver (primary), many had more than one caregiver who spent equal time with the individual with dementia.
cThis response is a result of not having a caregiver (see frequency for the “no” response).
Physical Pain, Mood, Safety, Sleep, and Motor Skills
Physical pain was rated numerically from 0 to 10, with 0 indicating no pain and 10 indicating severe pain. Pain levels within the 0 to 3 range accounted for 62.7% of the population, for 22.1% within 4 to 7, and 8.3% between 8 and 10 (Table 4).
Summary of Selected Clinical Variables Addressed in the Needs Assessment.a
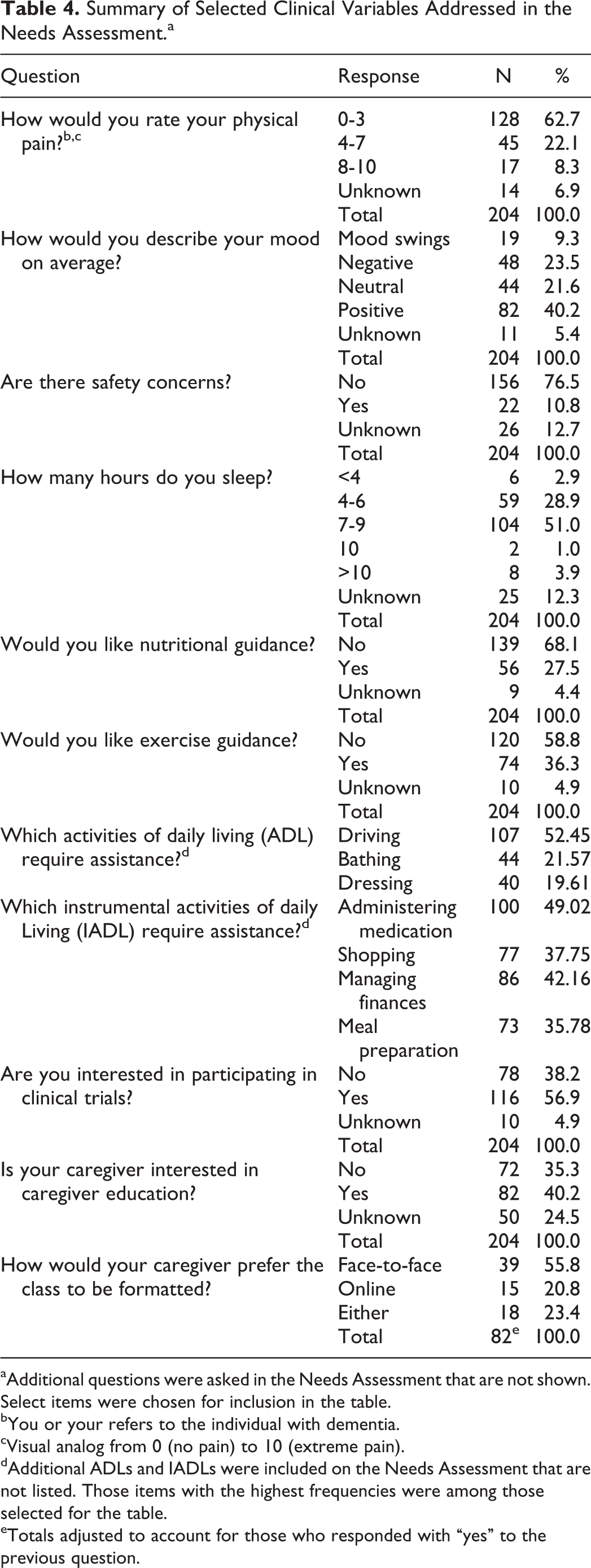
aAdditional questions were asked in the Needs Assessment that are not shown. Select items were chosen for inclusion in the table.
bYou or your refers to the individual with dementia.
cVisual analog from 0 (no pain) to 10 (extreme pain).
dAdditional ADLs and IADLs were included on the Needs Assessment that are not listed. Those items with the highest frequencies were among those selected for the table.
eTotals adjusted to account for those who responded with “yes” to the previous question.
The response for daily mood of the patient was open ended; therefore, the analysis of the response is relatively subjective. Responses were categorized into mood swings, negative mood, neutral mood, and positive mood. Mood swings were reported for 9.3% of individuals, a negative mood for 23.5%, a neutral mood for 21.6%, and a positive mood for 40.2%.
Safety concerns were asked with a general question, but encompassed home safety, wandering, and driving. Only 10.8% of the population had safety concerns, while 76.5% felt as though the safety was not an issue.
Hours slept were as follows: 2.9% slept less than 4 hours, 28.9% slept 4 to 6 hours, 51.0% slept 7 to 9 hours, 1.0% slept 10 hours, and 3.9% slept greater than 10 hours. Motor skill difficulty was a factor for 54.08% of participants, in addition to the cognitive problems, including difficulties with balance walking, handling utensils, writing, and dialing the phone.
Nutrition and Exercise
Nutritional guidance was of interested for 27.5% of the patients and 68.1% were satisfied with their current eating habits. Exercise guidance was requested by 36.3% of the study cohort, including advice for how to become more active, Web sites with online programs, handouts of basic movements, discussions of local gyms and pools. The remaining 58.8% were either satisfied with their current exercise program or were resistant to adding exercise into their daily routine.
Activities of Daily Living and Instrumental Activities of Daily Living
About one-third of the cohort, or 34.8%, were independent when it came to initiation, administration, and completion of ADLs and IADLs. Complete dependence and assistance with all activities were required for 8.33% of the population. The majority of patients needed assistance with only specific activities; 52.45% driving, 49.02% medication administration, 42.16% finances, 37.75% shopping, 35.78% food preparation, 21.57% bathing, and 19.61% dressing. Feeding, transfer, and participating in leisure activities were the lowest at 9.8%, 12.75%, and 15.20%, respectively.
Clinical Trials and Caregiver Education
Interest in learning about available clinical studies accounted for 56.9% of the population, while 38.2% did not want to participate.
Participation in a caregiver education program was of interest for 40.2% of the caregivers. This purpose of this program was to learn more about the biological basis behind the disease, methods of caregiving, support, and stress reduction tips. The 35.3% of caregivers who responded “no” to the caregiver education class felt they already knew enough about the neurodegenerative disease, were not interested, or previously/currently attend a support group. Of those who said “yes” to the class, 55.8% preferred an in person class, 20.8% preferred an online class, and 23.4% would attend regardless of the mode of administration.
Additional Services
Assistance obtaining assistive equipment, such as a cane, wheel chair, and bathroom modifications, was not necessary for 89.13% of the population. Of those who requested a referral to an additional service, 6.37% requested physical therapy, 1.47% occupational therapy, 1.47% psychiatry, 1.47% pain management, 1.47% were interested in working with a social worker, and 0.98% wanted neurocognitive rehabilitation. The majority of the population, or 89.22%, did not need additional assistance and were satisfied with the medical services provided by their current medical providers.
Mini-Mental State Examination
To objectively categorize the demented state of the participant, MMSE scores were utilized (Figure 1). Scores were as follows: 8.8%, 0 to 10; 18.1%, 11 to 20; 20.6%, 21 to 25; 41.1%, 26 to 30; 1.5%, other (language or education limitation); and 9.8%, unknown.
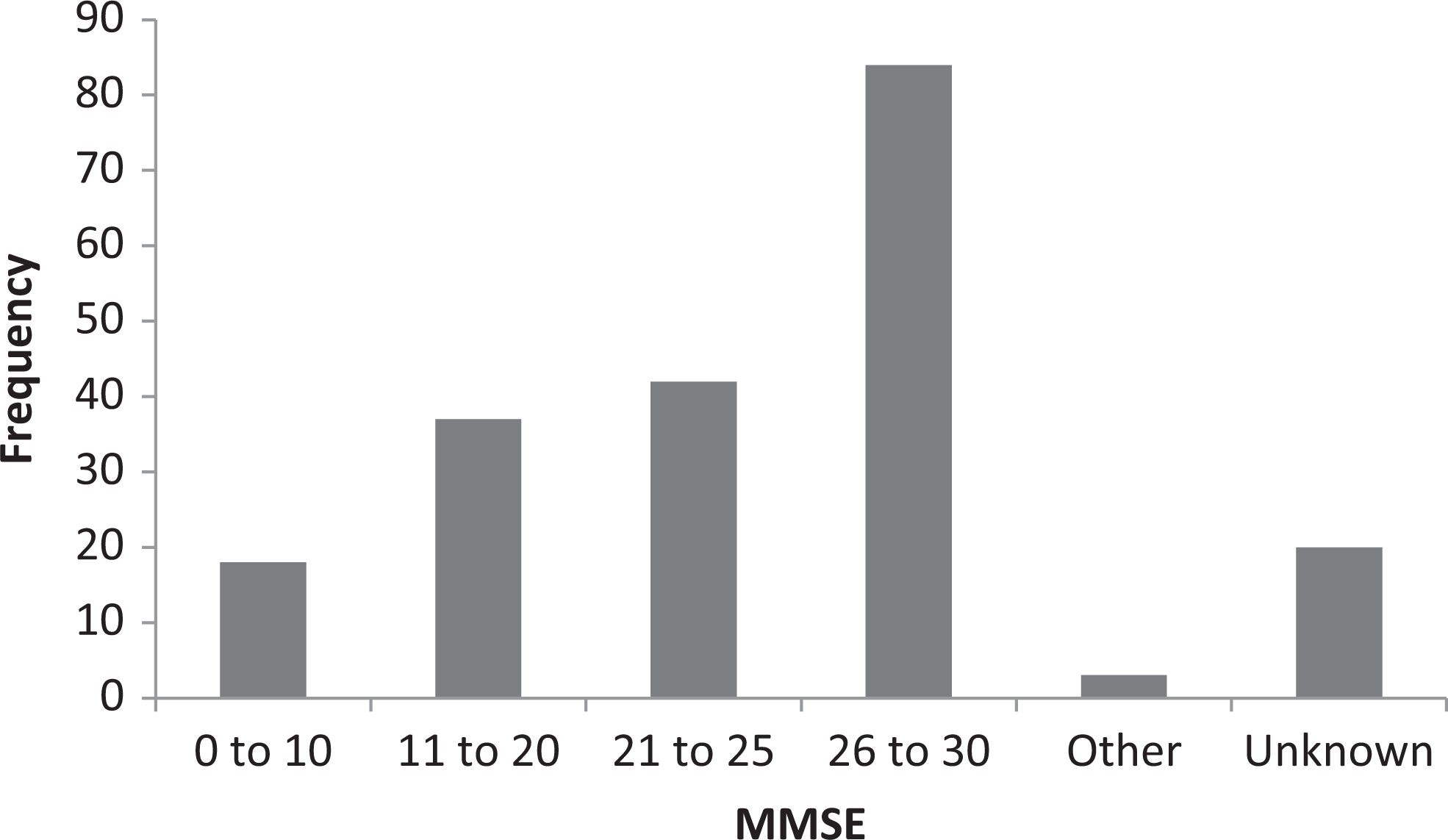
Distribution of MMSE scores among those with a memory disorder, captured following completion of the Needs Assessment. Classification of severity is as follows: 26 to 30, minimal impairment; 21 to 25, mild; 11 to 20, moderate; and 0 to 10, severe.
Discussion
The urban location of the Memory Disorders Program allowed for a racially diverse study demographic, with the exception of a weak Latino community sample. From a gender lens, both males and females were relatively equally represented, providing a diverse gender cohort.
An overwhelming majority of patients live at home and almost universally express a desire to remain there. In-home care is preferentially chosen over institutionalization and assisted living, although many affected individuals require moderate assistance, overseeing of activities, or full-time supervision. Previous studies show that external aide in the form of institutionalization is influenced by caregiver type, with nonspousal caregivers more likely than spouses to consider such an option. 13 Spouses also report difficulty in transitioning to assisted living, while adult children report a lesser degree of hesitation. 14 Personal in-home care was utilized by a minority of our study patients; the majority of our study cohort did not receive any additional help from professional outside sources, such as a home health aide or a skilled nurse.
There are a number of potential reasons to explain the lack of additional help for the caregiver. Initially, it may be assumed that this absence of aid is due to the current dementia stage; if the patient has not progressed to dependency, additional help is unnecessary. The MMSE scores were collected to provide a window into such stages. Collection of these data verified that the patients within the study were a mix of dementia stages, ranging from severe and completely dependent to mild and independent. Potential explanations for the lack of utilization of external aide include: a patient and family commit to keep the care network limited and exclusive, lack of available resources within the community, or financial obstacles. Regardless of the reason, caregivers are left as the sole provider to meet all of the needs for the individual with a memory disorder.
A number of needs were explored in our memory disorder cohort, including, but not limited to, sleep, exercise, clinical trials, education, and assistance with ADLs and IADLs. In terms of sleep, over one-quarter of the surveyed population reported sleeping 6 hours or less per night. Although changes in the sleep–wake cycle are characteristic of aging, this is particularly an issue for those who are not independent. 15 Required supervision during atypical hours of wakefulness prevents the caregiver from getting adequate sleep, affecting all aspects of the caregiver’s daily functioning.
About one-third of the patients requested exercise guidance, while the remaining indicated satisfaction with their current exercise program or were resistant to adding exercise into their daily routine. The caveat here is, are the “satisfied” patients getting the optimal exercise to maximize cognitive health? Research suggests physical activity reduces risk and delays onset of dementia, possibly by improving control over and decreasing vascular risk factors. 16 Adequate exercise may aide in delaying the progression of the disease, maintaining independence as long as possible, and ultimately decreasing caregiver requirements.
Over half of the patients and caregivers were interested in learning about clinical trials. This suggests that the current disease state and/or perceptions of disease progression are so daunting that patients and caregivers are willing to go to great lengths to delay the progression, treat the symptoms, or cure the disease. This also indicates that there is an altruistic desire among caregiver and patients alike to help others in the future that may face a similar situation. In addition, almost half of the caregivers were interested in participating in an educational program, to optimize safety and function and to decrease caregiver stress. Interest in this program indicates that the caregivers need guidance and support to properly care for both their loved one and themselves. When exploring patient diagnosis and caregiver experience, 84% of caregivers do not feel as though they are adequately educated on the disease and providing care. 17 Adult children emphasize a need for learning about the progression of dementia. 14
Exploration of ADLs and IADLs provided insight into the daily needs caregivers must address for the patients. Only one-third of the patients were completely independent, leaving the majority of the caregivers to have at least one type of role in the patient’s daily functioning. About half of the patients were unable to drive, administer their medications, and take care of finances. A significant portion of patients were also unable to neither go out alone and shop nor prepare their meals. The aforementioned activities are both time consuming and inconvenient for the caregiver to address on a daily basis and prevent adequate time to satisfy personal needs, physically, spiritually, emotionally, mentally, and medically. Past studies indicate that daily living need varies based on caregiver gender and adherence to gender norms. 18 Typical male caregivers express need for domestic aide (ie, cleaning and meals), while female caregivers request financial and driving need more readily.
The caregiver must have resources and services on hand in order to properly and efficiently meet these demands. Although a variety of services exist within the community in the form of online venues and physical centers, there is a gap between physician diagnosis and caregiver awareness. 17 A previous study found that merely 7% of caregivers feel as though they are provided with adequate community information once receiving the official dementia diagnosis from their physician. Caregivers report dissatisfaction with the services primarily stemming from difficulty obtaining information and poor perceived control over the service. 18 This gap needs to be bridged between physicians, community and Internet resource providers, and caregivers.
It is important to consider the results of this study while also keeping in mind the study limitations. A potential limitation is the medical facility type and location, which may be reflected in the population living situation summary (age-based community, assisted living, home, and nursing home). These statistics may be influenced by the fact that the patients were seen at an outpatient clinic in Philadelphia. Many long-term care facilities provide in-house medical care with a physician for the residents. Elderly patients with dementia may take advantage of this option rather than venturing into the city to see a specialist.
A second limitation of this study is we did not directly ask the caregiver to explain their needs and describe their sources of burden. The Needs Assessment was primarily patient centered to determine the needs of the patient, not the direct needs of the caregiver. The goal was to address what can be done for the patient so the caregiver does not have to fulfill that need.
Now that the needs have been identified, the next steps are to explore each individual need further and to determine how to successfully meet such needs. The vital questions must be asked in order to progress forward in meeting needs: Why is this need in demand? What are the innovative options to address the need? What community resources are currently available and how can their services be made more transparent? The current identification and later exploration of patient and caregiver need are vital in order to decrease caregiver burden and stress; ultimately, increasing the quality of life of both the patient and the caregiver.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.