
Abstract
This study explored psychosocial and cognitive predictors of perceived threat of Alzheimer’s disease (AD). Respondents were 1641 adults (mean age: 64.4; 54% female; 82% white) who completed a module in the Health and Retirement Study, a nationally representative survey of adults aged ≥50. Findings show that perceived threat was significantly higher for those aged 50 to 64 (P < .001) and 65 to 74 (P < .05) than for those ≥75. Respondents with a family history of AD had significantly greater perceived threat (P < .001) than those with no experience. Stronger endorsement of the beliefs that stress (P < .01) or genetics (P < .01) are important AD risk factors was significantly associated with greater perceived threat, as was having more depressive symptoms (P < .01), poorer self-rated memory (P < .01), and lower cognitive function (P < .01). Personal experience moderated the relationship between perceived threat and 2 variables: age and self-rated memory. Understanding perceived AD threat may inform practice and policies centered on early and accurate diagnosis.
Introduction
Alzheimer’s disease (AD) is among the most debilitating and prevalent diseases in the United States. 1,2 In recent years, researchers, health-care professionals, advocacy organizations, the media, and families and patients have attempted to raise awareness of the personal, social, and economic challenges posed by the disease. Although there is currently no cure or proven strategy to prevent AD, methods are emerging to detect and diagnose early stages of the disease. These include the implementation of clinical criteria for diagnosing mild cognitive impairment (MCI), 3 a precursor for AD, and the identification of blood, brain, and spinal fluid biomarkers that may help to detect prodromal stages of the disease before clinical manifestation occurs. 4
Future public health efforts to prevent or delay the onset and progression of AD may be heavily reliant on public support and participation in programs centered on early detection and diagnosis. Many organizations have emphasized the importance of early detection and diagnosis, pointing to potential benefits such as improved access to treatment and support services, greater autonomy of affected individuals in legal, financial, and care planning, and reduced health-care costs. For instance, Healthy People 2020 aims to increase AD diagnosis disclosure by 10% from a baseline of 34.8% of adults aged ≥65 with a dementia diagnosis, 5 and the Alzheimer’s Association and Centers for Disease Control and Prevention’s (CDC) Healthy Brain Initiative calls for greater promotion of early detection and diagnosis. 6
Perceived threat of AD potentially serves as a key factor in the likelihood of seeking timely diagnosis or participating in screening programs. Many individuals express a high level of perceived AD threat, especially those with a family history or personal experience. 7 Adult children of patients who have AD are more likely than those without a family history to engage in “symptom-seeking behavior,” opening the possibility for misinterpretation of a cognitive error as a disease symptom. 8 Among individuals who consult their physician about memory-related concerns, a significant proportion show no signs of cognitive impairment. 9 These individuals, who have been termed the “worried well,” may also have heightened perceived AD threat, leading them to report memory changes and concerns to a doctor. Such individuals may also be at a heightened risk for misdiagnosis. In addition, a 3-year follow-up study of patients who sought help for memory complaints at an outpatient memory clinic found those individuals to have low conversion rates to MCI and dementia and that memory complaints were significantly associated with psychosocial stress and feelings of anxiety. 10 Thus, psychosocial factors may explain why individuals with no evidence of cognitive impairment may experience memory problems.
Despite progress in early detection of AD, the current emphasis on early diagnosis and screening may result in heightened perceived threat of AD, leading to overdiagnosis and overtreatment with adverse consequences for patients and families. 11,12 Because there are no preventive or curative treatments for AD, patients may try nonevidence-based therapies (eg, vitamin E, gingko biloba, cholinesterase inhibitors, etc) potentially causing adverse and costly medical events. 11 There are also concerns about false positives and misdiagnosis, psychological distress and stigma associated with receiving an early AD diagnosis, and overburdening health-care systems with increased diagnostic testing and screening. 11 The flip side of these concerns is that low perceived AD threat may suppress help-seeking among cognitively impaired individuals in need of diagnosis, further widening disparities in health care and outcomes.
Relatively few studies have examined predictors of perceived AD threat. Those that exist focus mainly on individuals who may be genetically at risk for AD (eg, first degree relatives) and/or have been conducted in small convenience samples with limited racial and ethnic diversity. 13 -18 Several studies have been guided by health behavior theories and constructs, including the Health Belief Model (HBM) and the Common-Sense Model of Illness Representations (CSM), as well as models of health anxiety. 13,14,17,18 The HBM includes factors such as perceived threat, perceived benefits and barriers, self-efficacy, and cues to action and has been largely successful in predicting a variety of health-related preventive and screening behaviors. 19 -21 Within this framework, perceived threat has been defined as a combination of perceived susceptibility (ie, belief about the likelihood of getting the disease) and perceived severity and concern (ie, perceptions about the seriousness of getting the disease). The CSM has also been applied to many health conditions and includes a variety of cognitive (identify, causes, consequences, and timeframe) and emotional processes that shape personal perceptions of a disease and may predict help-seeking behavior. 22,23
In one of the most comprehensive studies of perceived AD threat to date, Suhr and Kinkela used social-cognitive theories of health anxiety to guide their investigation of predictors of perceived AD threat in 97 healthy older adults self-referred for community-wide memory screening. 13 The models, proposed by Warwick and Salkovskis 24 and Williams, 25 consider previous experience with an illness (eg, observing the disease in a family member), as well as individual factors such as beliefs about the disease, anxiety, and selective attention to symptoms, to be important factors influencing worry about a disease or perceived threat. Suhr and Kinkela found significant relationships between perceived AD threat and several explanatory variables, including personal experience with AD (whether genetic or nongenetic), depression, and belief in negative age stereotypes. The authors also found that personal experience with AD moderated the relationship between actual cognitive performance and perceived AD threat. Participants with genetic AD experience (ie, first or second degree relative) had generally higher perceived threat when they had better cognitive performance, whereas those with nongenetic (eg, spouse, friend, etc.) or no AD experience had higher perceived threat when they had worse cognitive performance. This suggests that personal experience with AD may play a particularly salient role in perceived AD threat and cognitive performance.
While the Suhr and Kinkela study provides valuable insight into predictors of perceived AD threat, the sample was relatively small and participants were “self-referred,” limiting the generalizability of the findings to the general aging population. The study also does not examine associations between self-reported or subjective memory complaints and perceived AD threat. Perceived AD threat is likely to be a response to a complex set of determinants, including knowledge and beliefs, family experience, psychological well-being, cognitive function, etc. and to our knowledge no studies to date have examined this complex set of factors in a large and diverse sample that is broadly representative of the US adult population. Gaining a better understanding of potential factors related to perceived AD threat using a nationally representative sample of adults, with an emphasis on further delineating the role of family experience with AD, would provide useful information not only for assessing patients in clinical settings but also for large-scale public health efforts aimed at early and accurate AD detection and diagnosis.
The aim of our study is to examine psychosocial and cognitive predictors of perceived AD threat, an understudied construct related to help-seeking behavior, among a nationally representative sample of US adults. We were specifically interested in 2 main questions: (1) What are the significant psychosocial and cognitive factors associated with perceived AD threat? and (2) Does family experience with AD moderate the relationship between cognitive factors and perceived threat? Based on prior research, we hypothesized that family experience with AD, 13 strong beliefs about genetic risk for AD, 26 higher levels of depressive symptoms, 13,16 poorer self-rated memory, 15 and lower objective cognitive functioning, 13 will be associated with higher perceived AD threat. Based on the results of the Suhr and Kinkela study, we expected to find significant moderating effects of family experience on the relationship between cognitive function and perceived AD threat (ie, for those with family experience, lower objective cognitive function will be associated with greater perceived threat), and on the relationship between age group and perceived AD threat (ie, for those with family experience, younger age will be associated with greater perceived threat). 13 Social-cognitive theories of health anxiety, which consider experiential factors like personal experience with a family member who has the disease and selective attention to symptoms as important influences on worry or anxiety about a disease, 24,25 also provide support for a potential moderating effect of family experience. There is evidence that younger age is associated with higher perceived threat in those who have genetic experience with AD, 14,27 while older age has been found to significantly predict higher AD symptom-seeking behavior in those without genetic experience. 17 In addition, we also hypothesized that those with greater knowledge about AD will have lower perceived AD threat. 28 Finally, given the potential benefits of certain health behaviors in reducing the risk of cognitive decline and dementia, we wanted to examine the association between personal beliefs about the effectiveness of protective factors in lowering dementia risk (ie, physical exercise, keeping mentally active, etc) and perceived AD threat. To our knowledge, this is the first study to examine this association. Based on the notion that those who believe something can be done to reduce disease risk will feel less vulnerable, we hypothesized that people who have stronger beliefs that AD risk can be modified through health behaviors will have lower perceived AD threat.
Methods
Participants and Procedures
Data for this project come from the Health and Retirement Study (HRS), a longitudinal community-based cohort study with a nationally representative sample of over 30 000 individuals older than 50 years. The RAND enhanced version of public release data from the 2010 wave of the HRS study, including a brief supplementary survey module focused on knowledge and beliefs about AD, was used for this analysis. 29 A random subsample of individuals (n = 2213) who participated in the 2010 HRS survey (n = 22 037) was invited to complete this ∼3 minute module. Of the sampled respondents, 320 were determined ineligible for reasons of requiring proxy respondents, or current nursing home residency (sampling weights of 0). Among those who were eligible (n = 1893), 1840 individuals were Hispanic, non-Hispanic black, and non-Hispanic white. Of these, 1641 individuals completed the module and were included. We focused our analysis on respondents from these 3 racial/ethnic groups, given the small numbers of respondents in our sample from other backgrounds. The 1641 respondents were compared to the larger HRS sample (excluding “other” race and those with sampling weights of 0), and no significant differences were found with regard to age, gender, education, and race/ethnicity. Complete details of the development, sampling, and administration of the supplementary module have been published elsewhere. 30
Measures
Demographics
Demographic characteristics included age (50-64, 65-74, or ≥75), gender, race/ethnicity (Hispanic, non-Hispanic black, or non-Hispanic white), marital status, and education (no degree, GED or high school diploma, or ≥2-year college degree).
Perceived AD threat
Three items were used to examine perceived AD threat. Participants indicated their level of agreement (strongly agree, somewhat agree, neither agree nor disagree, somewhat disagree, and strongly disagree) with the following 3 statements: (1) “You would like to know your chances of someday getting Alzheimer’s,” (2) “You believe you will get Alzheimer’s someday,” and (3) “You worry about getting Alzheimer’s someday.” These items have been used in previous studies. 14 “Don’t know” responses (1.2%-1.6% of responses across the 3 items) were folded into the “neither agree nor disagree” category. Items were reverse coded to aid model interpretability, and a composite mean score was calculated for each participant by averaging scores across the 3 items (Cronbach α of 0.635).
Knowledge about AD
Two previously validated items from the Alzheimer’s Disease Knowledge Scale 31 assessed understanding of AD risk and protective factors: (1) “Prescribed drugs that prevent AD are available” (True/False; correct answer = false) and (2) “Having a parent or sibling with AD increases the chance of developing it” (True/False; correct answer = true). “Don’t know” responses were categorized as incorrect. A knowledge composite score was computed (with possible values of 0-2) by summing the number of correct responses for each participant (Cronbach α = 0.058).
Family experience with AD
Family experience with AD was assessed with 2 items. The first asks respondents: “Has your [husband/wife/partner], or a parent, sibling, or adult child of yours been diagnosed with Alzheimer’s?” (Yes/No). The second asks respondents “do you know someone who has had Alzheimer’s disease?” (Yes/No). Responses were recoded into 3 categories: 1 = no experience, 2 = knows someone, and 3 = family experience.
Beliefs about AD risk factors
Two items were used to examine beliefs about AD risk factors. Respondents were asked to rate on a 3-point scale how important (ie, very, somewhat, or not at all) stress or genetics are in increasing a person’s chances of getting AD: (1) “Do you believe stress is very important, somewhat important, or not at all important in increasing a person’s chances of getting Alzheimer’s?” and (2) Do you believe genetics is very important, somewhat important, or not at all important in increasing a person’s chances of getting Alzheimer’s?” “Don’t know” responses (2.7%-3.0% of responses across items) were categorized as not endorsing the belief. These items were treated as 2 separate ordinal variables in the regression model, and reverse coded to increase interpretability: 1 = not at all important, 2 = somewhat important, and 3 = very important.
Beliefs about AD protective factors
Four items assessed beliefs about AD protective factors. Respondents were asked how effective (ie, very effective, somewhat effective, not at all effective) they believe 4 health behaviors are in lowering one’s chances of getting AD: (1) keeping physically active, (2) keeping mentally active, (3) eating a healthy diet, (4) taking vitamins or dietary supplements. “Don’t know” responses (1.3%-2.3% of responses across items) were categorized as not endorsing the behavior. Items were reverse coded to increase model interpretability (ie, 1 = not at all effective, 2 = somewhat effective, and 3 = very effective), and a composite score was generated by summing responses across the 4 items for each participant (Cronbach α of 0.80). The composite measure had a score range from 4 to 12 with higher scores indicating stronger beliefs in the effectiveness of health behaviors in lowering risk for AD.
Symptoms of depression
Depression symptoms were assessed using a shortened version of the Center for Epidemiologic Studies Depression Scale (CES-D), 32 included in the HRS Core survey. The 2010 HRS measure of symptoms of depression consists of a subset of 8 items from the original 20-item CES-D scale and an additional item assessing respondents’ level of energy. This shortened scale is commonly used in epidemiological studies to assess frequency of depressive symptoms, and has been previously established as having comparable reliability and validity to the 20-item CES-D scale. 33,34 We also chose to include the additional item “You had a lot of energy” as it is related to the construct of depression and has been found to load onto the common depression factor in factor analysis. 35 Respondents were asked to respond to the statements (response codes: 1 = Yes, 0 = No): (1) You felt depressed, (2) You felt that everything you did was an effort, (3) Your sleep was restless, (4) You were happy, (5) You felt lonely, (6) You enjoyed life, (7) You felt sad, (8) You could not get going, and (9) You had a lot of energy. “Don’t know” responses (between 1 and 3 responses across items) were classified as not endorsing the statement. A composite score was created by reverse coding 3 positively worded items (ie, You were happy, You enjoyed life, You had a lot of energy) and summing scores across the 9 items (Cronbach α of 0.80). Higher scores indicate more depressive symptoms (range: 0-9).
Subjective memory complaints
Subjective memory complaints were assessed using 1 item: “How would you rate your memory at the present time?” (on a 5-point scale: excellent, very good, good, fair, or poor). This measure is consistent with other studies that have examined subjective memory complaints in older adults. 36
Cognitive function
Cognitive function was assessed through the use of a cognition summary variable. The total cognition score sums the total recall and mental status indices in the HRS and has a range of 0 to 35 with higher scores indicating better cognitive function. 37 The total recall index includes an immediate recall task (0-10) and a delayed recall task (0-10). The mental status index includes several tasks: serial 7s (0-5), backward count from 20 (0-2), object naming—scissors or cactus (0-2), president naming (0-1), vice president naming (0-1), and date naming (0-4). Of the 1641 respondents, 346 had missing data on the total cognition summary variable included in the RAND/HRS dataset. This was due to an age cutoff implemented in the HRS survey for reinterviewed respondents younger than 65 years on specific mental status index items: date naming, object naming (scissors or cactus), and naming the president or vice president. 38 Under the assumption that respondents younger than 65 years would have virtually no inaccuracies on these items, we imputed full accurate responses for these missing data points. A total cognition score was then re-computed by summing all mental status and total recall items.
The construct validity of the cognition measures and the consistency of the inter-relationships between individual items that compose the total cognition score have been previously demonstrated, and factor analysis supports the creation of a cognitive summary score. 38 The total cognition score in this study had a Cronbach α of 0.643, consistent with previous estimates for the HRS population. 38,39
Data Analysis
All analyses were conducted using SPSS version 22 software for Windows. Because the HRS uses a complex sampling design that involves clustering, stratification, and weights, the SPSS Complex Samples module was used to account for sampling weights and other design elements.
Univariate descriptive analyses were conducted to characterize the sample in terms of demographics, including age, gender, race/ethnicity, education, and so on, as well as cognitive and psychosocial variables of interest. Bivariate associations were explored through a series of chi-square and correlation analyses. Chi-square tests of association were performed to examine inter-relationships between categorical predictors, while a Pearson’s r correlation matrix was generated to explore inter-relationships between ordinal predictors. Multicollinearity was assessed among independent variables by examining bivariate correlations. Cronbach α statistics were computed for composite measures.
Linear models were fit to the data to examine predictors of perceived AD threat. The complex samples general linear model (CSGLM) procedure was used in SPSS, which provides regression analysis for 1 dependent variable by specified factors and covariates. Categorical predictors were entered into each linear model as factors and automatically coded as dummy variables by SPSS. Simple contrasts were used to compare each group/level within the categorical predictor to a designated reference group. A hierarchical approach to fitting the data was taken to assess the unique contributions of demographic, psychosocial, and cognitive predictors. Demographic variables were modeled first (model 1), followed by psychosocial variables (model 2), and cognitive variables (model 3), with each subsequent model adjusting for variables in the previous models. The full model (model 3) contained 13 predictors: age (50-64, 65-74, ≥75), gender (male or female), race/ethnicity (Hispanic, non-Hispanic black, and non-Hispanic white), education (No degree, GED or high school diploma, ≥2-year college degree), marital status (married or single), AD knowledge, personal experience with AD (has spouse or first degree relative with AD, knows someone with AD but not a spouse or first degree relative, and no experience with AD), belief about stress as a risk factor, belief about genetics as a risk factor, beliefs about AD protective factors, depressive symptoms, subjective memory complaints, and cognitive function. Age was entered into the model as a categorical variable for ease of interpretation and to assess differences between age groups, as dementia risk substantially increases after age 65. Interaction effects were also examined, including family experience as a possible moderator of the relationship between cognitive predictors and perceived AD threat (model 4).
Results
Respondent Characteristics
Demographics characteristics are summarized in Table 1. The mean age was 64.4 years, with most respondents younger than 75 years. The majority were non-Hispanic white (81.7%), followed by non-Hispanic black (10.3%) and Hispanic (8.0%). Over half knew someone with AD who was not related (50.5%), while 13.3% had a spouse or first degree relative with AD.
HRS Population Characteristics.a,b
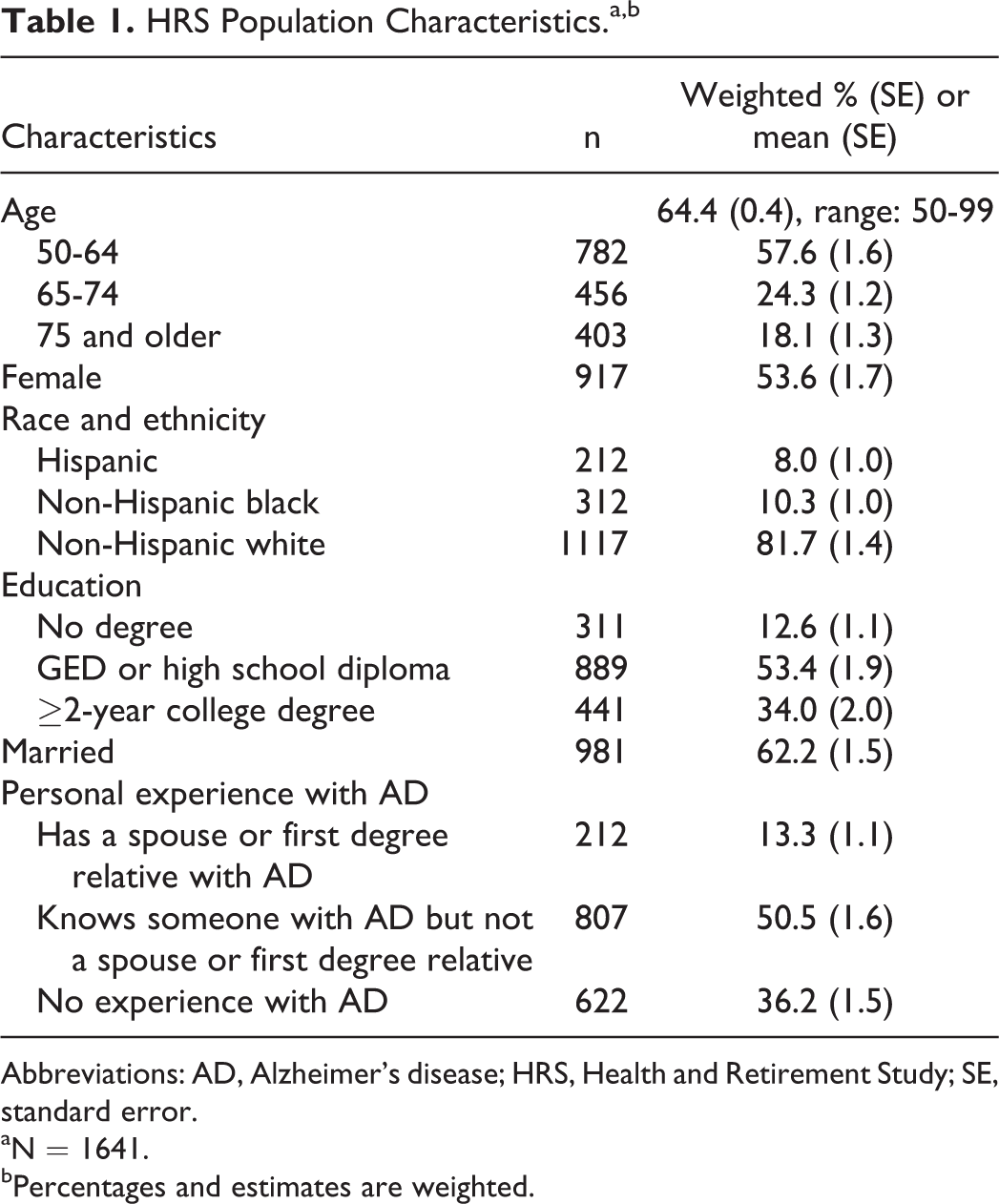
Abbreviations: AD, Alzheimer’s disease; HRS, Health and Retirement Study; SE, standard error.
aN = 1641.
bPercentages and estimates are weighted.
The means, standard errors, and score ranges of psychosocial and cognitive variables are presented in Table 2. While most respondents correctly answered either one (43.3%) or both (42.8%) AD knowledge items, a considerable percentage (13.8%) still received an incorrect score on the 2 items. A high percentage saw genetics as a somewhat important or very important risk factor (90.7%), whereas just over half (58.7%) indicated that stress as a risk factor was somewhat or very important. The AD protective factors composite had a mean score of 9.1 (score range: 4-12), with respondents tending to believe that one could effectively lower one’s chances of getting AD through specific health behaviors. Overall, respondents reported few depressive symptoms (mean = 1.64; range = 0-9 symptoms), and displayed relatively high cognitive function (mean = 23.3; range = 0- 35). About a quarter rated their memory as poor (4.4%) or fair (18.5%). Over half (60%) wanted to know their chances of developing AD, 22.9% believed that they would someday have AD, and 29.4% worried about getting the disease.
Means, SE, and Score Range of Psychosocial and Cognitive Variables.a,b
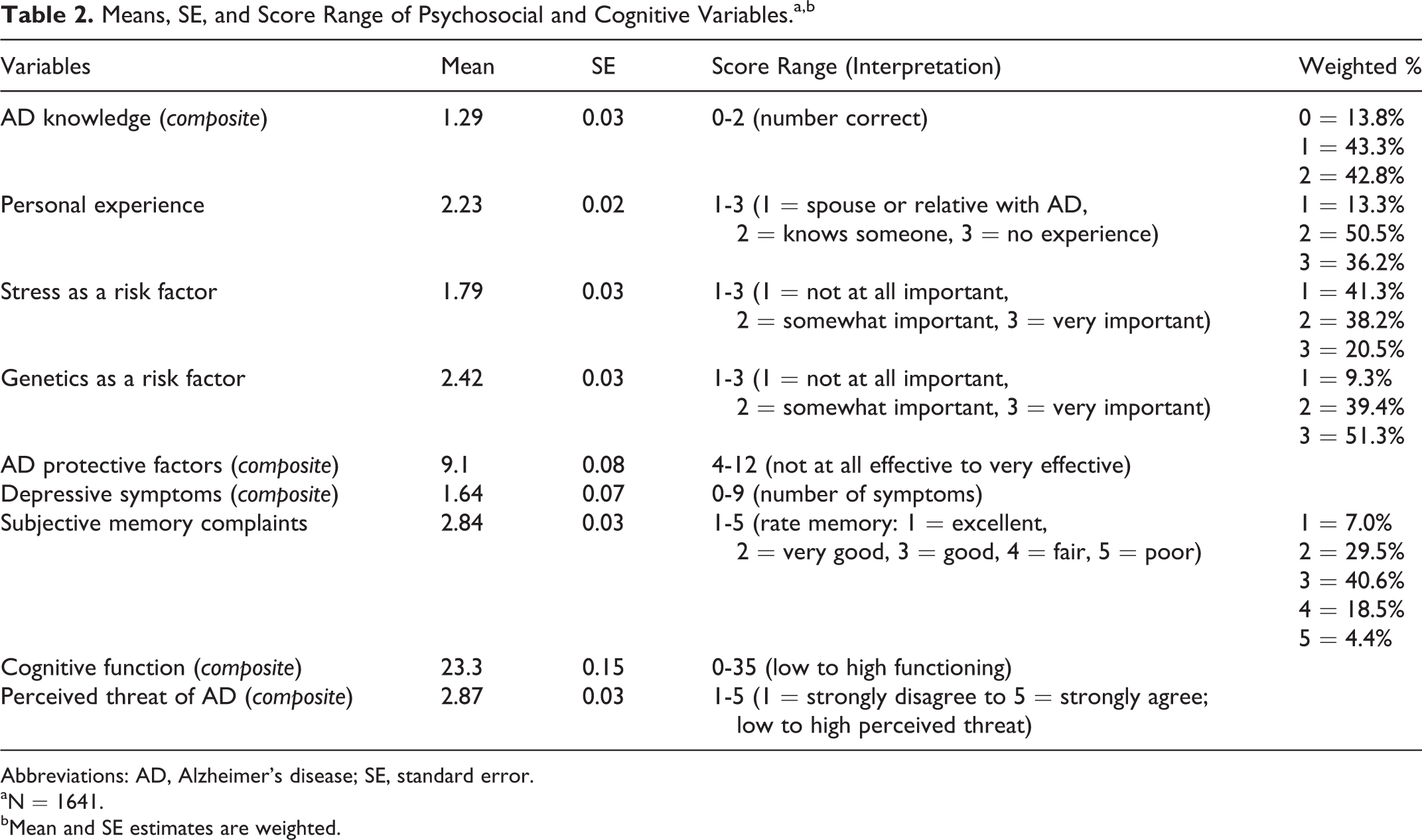
Abbreviations: AD, Alzheimer’s disease; SE, standard error.
aN = 1641.
bMean and SE estimates are weighted.
Bivariate Summaries
Table 3 provides a bivariate summary of psychosocial and cognitive predictors. Pearson r correlations showed significant positive associations between perceived AD threat and stress as a risk factor, genetics as a risk factor, depressive symptoms, and subjective memory complaints. Cognitive function showed significant inverse relationships with subjective memory complaints and depressive symptoms, while there was a significant positive association between subjective memory complaints and depressive symptoms. In our assessment of multicollinearity, we did not find evidence of the independent variables being highly correlated. Pearson correlations ranged from −0.264 (stress as a risk factor and education level) to 0.417(education level and cognitive function).
Bivariate Summary With Pearson Correlations for Perceived AD Threat and Psychosocial and Cognitive Predictors in the Regression Model.a,b
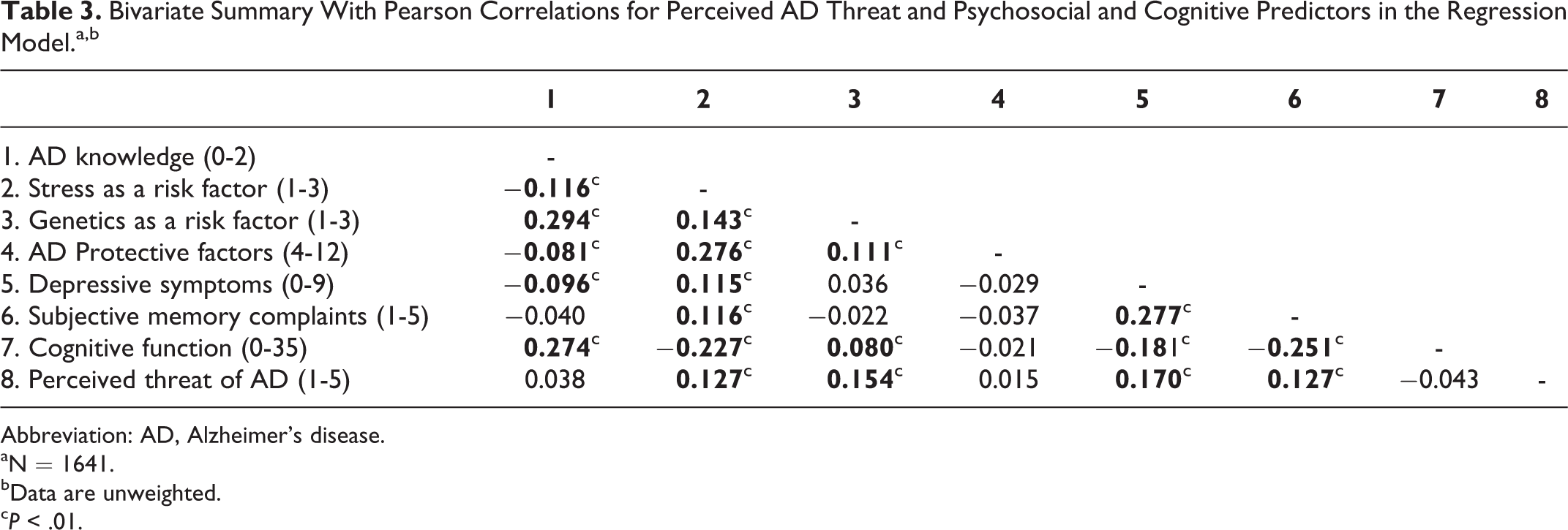
Abbreviation: AD, Alzheimer’s disease.
aN = 1641.
bData are unweighted.
c P < .01.
Regression Analysis of Perceived AD Threat
Table 4 presents the results of the linear regression analysis for the composite measure of perceived AD threat. The addition of psychosocial and cognitive variables produced a small improvement in the amount of variance explained across the models. In the full model (model 3), 6 predictors emerged as significantly associated with perceived AD threat. Compared to those aged 75 and older, perceived threat was significantly higher for respondents aged 50 to 64 and 65 to 74. Those with a family history of AD had significantly greater perceived threat than those with no experience. Stronger beliefs that stress or genetics are important AD risk factors were significantly associated with greater perceived threat. Higher perceived threat was significantly associated with having a greater number of depressive symptoms. Perceived AD threat was also significantly higher for those with poorer self-rated memory and those with lower objectively measured cognitive function.
Summary of Linear Regression Analysis of Perceived AD Threat.a,b,c
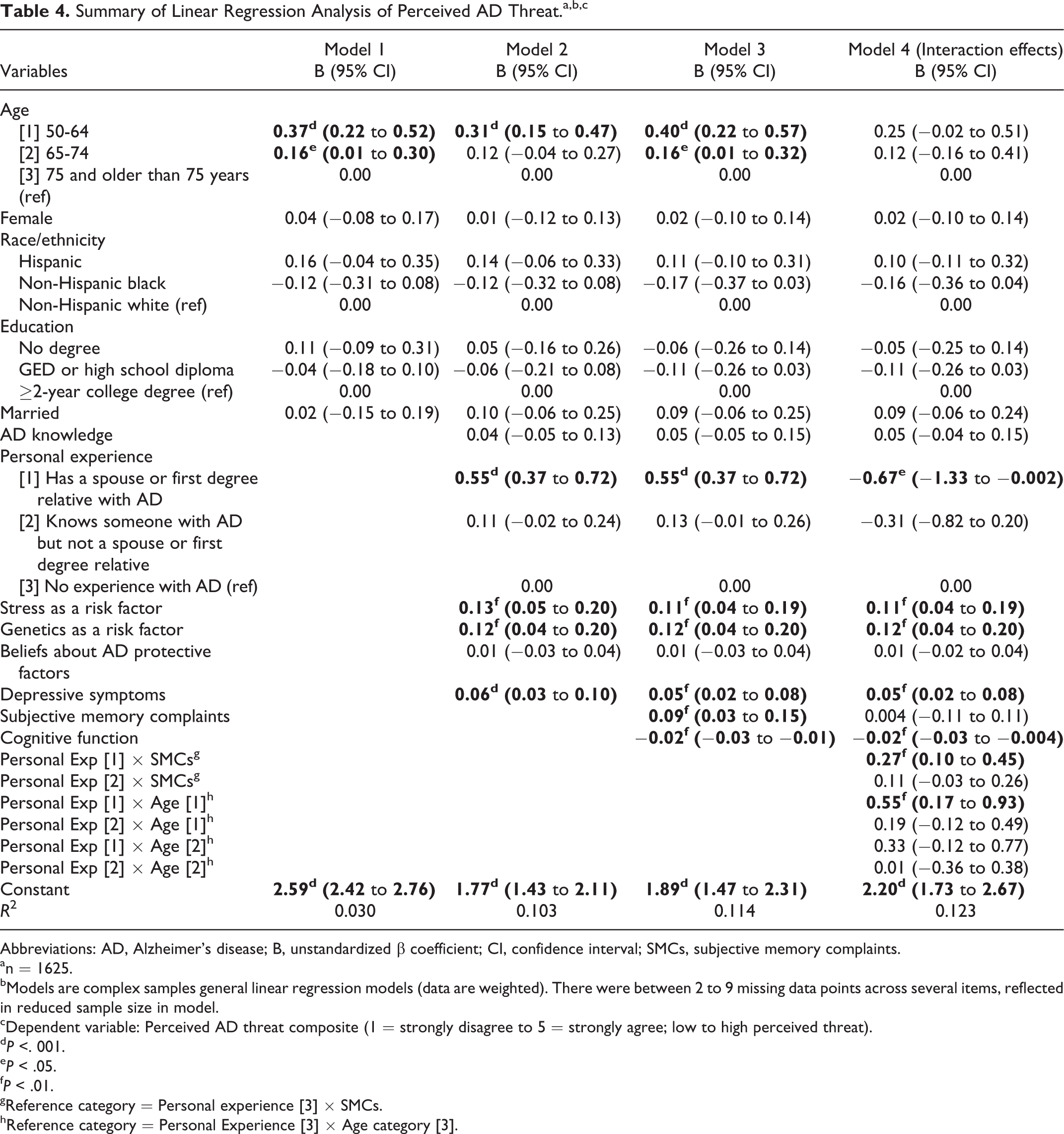
Abbreviations: AD, Alzheimer’s disease; B, unstandardized β coefficient; CI, confidence interval; SMCs, subjective memory complaints.
an = 1625.
bModels are complex samples general linear regression models (data are weighted). There were between 2 to 9 missing data points across several items, reflected in reduced sample size in model.
cDependent variable: Perceived AD threat composite (1 = strongly disagree to 5 = strongly agree; low to high perceived threat).
d P <. 001.
e P < .05.
f P < .01.
gReference category = Personal experience [3] × SMCs.
hReference category = Personal Experience [3] × Age category [3].
Two significant interaction effects were observed (model 4). First, personal experience with AD moderated the relationship between subjective memory complaints and perceived AD threat. The predicted increase in perceived AD threat associated with having subjective memory complaints was significantly greater for those who had a spouse or first degree relative with AD compared to those with no experience (B = 0.27, P < .01). Second, personal experience with AD moderated the relationship between age group and perceived AD threat. The predicted increase in perceived AD threat associated with being in the youngest age group (50-64) was significantly greater for those who had a spouse or first degree relative with AD compared to those with no experience (B = 0.55, P < .01). The regression lines are graphed in Figures 1 and 2.
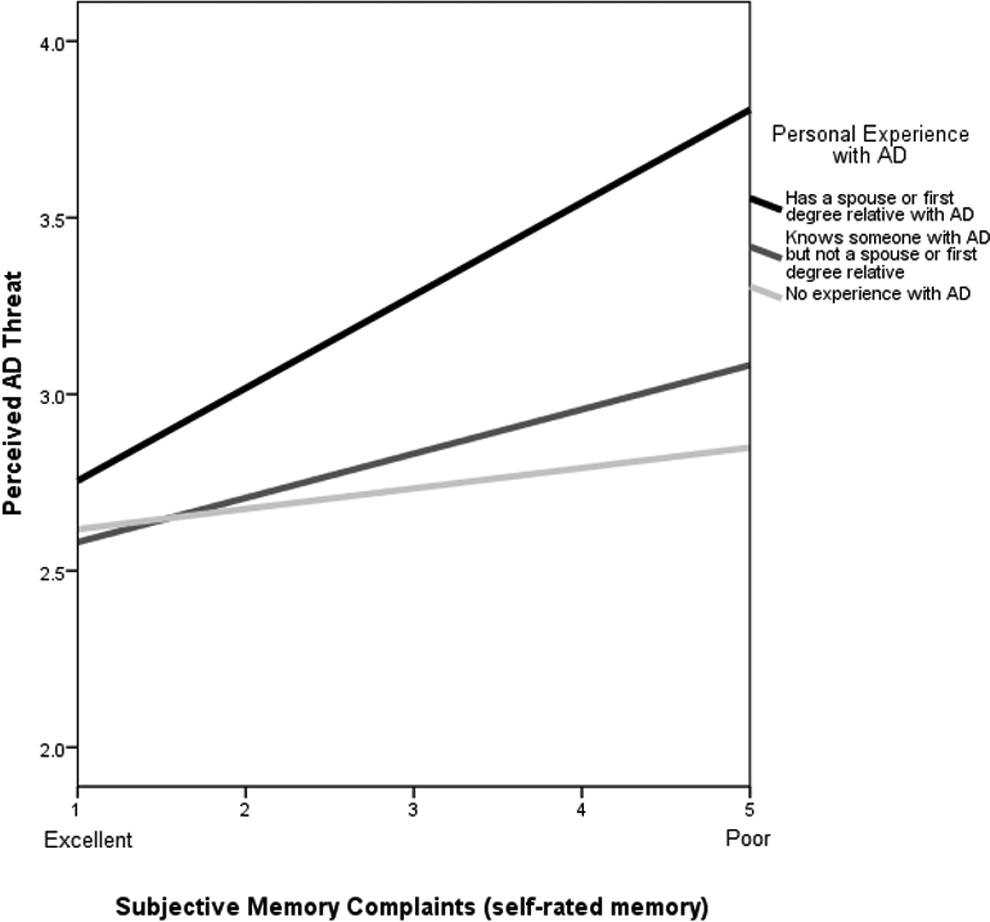
Moderating effect of personal experience with Alzheimer’s disease (AD) on the relationship between subjective memory complaints and perceived AD threat.
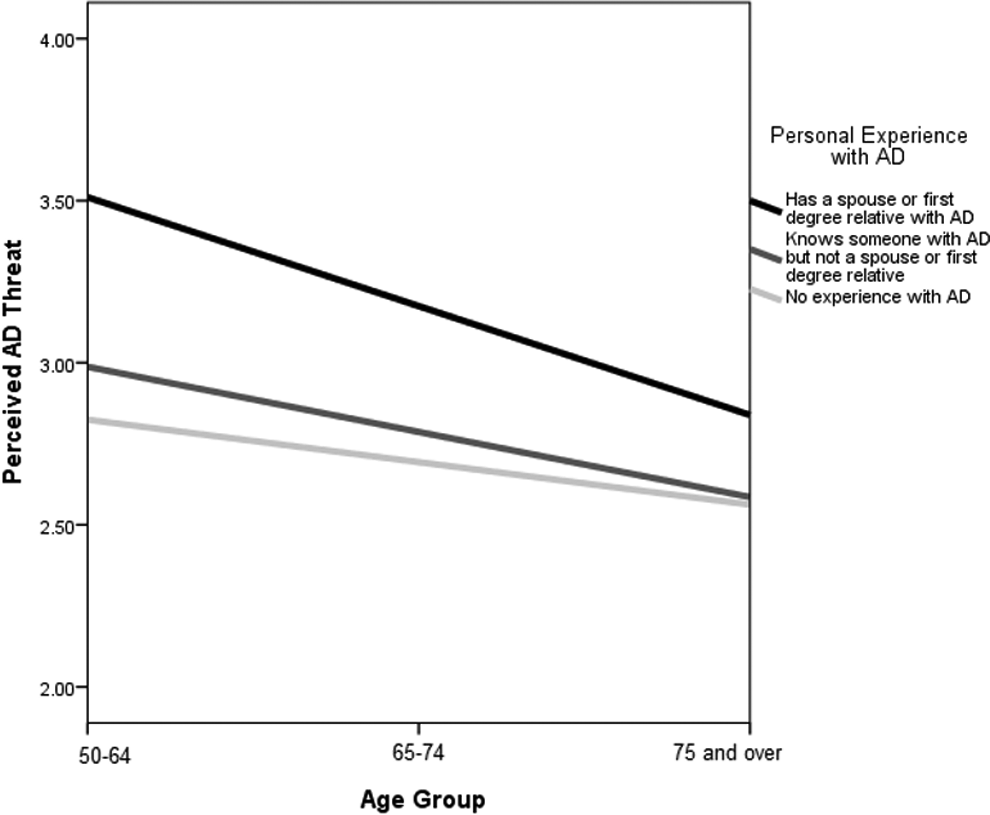
Moderating effect of personal experience with Alzheimer’s disease (AD) on the relationship between age group and perceived AD threat.
Discussion
This study sought to explore psychosocial and cognitive predictors of perceived AD threat in a nationally representative sample of adults. The purpose was to gain insight into factors that influence perceived AD threat, an understudied construct that may predict who seeks out cognitive evaluation, and to inform clinical and public health efforts aimed at improving early and accurate diagnosis. Results from the multivariate linear regression analysis revealed significant relationships between perceived AD threat and age, personal experience with AD, beliefs about stress and genetics as AD risk factors, depressive symptoms, and subjective memory complaints, and cognitive function. Family experience with AD also played a significant moderating role in the relationship between subjective memory complaints and perceived AD threat. These findings suggest that among the general adult population, perceived AD threat is associated with a number of factors in addition to actual cognitive function. Personal beliefs, experiences, perceptions, and psychological well-being may underlie concerns and worries about AD.
As expected, several psychosocial factors were found to be significantly related to perceived AD threat, including personal experience with AD, depressive symptoms, and beliefs about stress and genetics as AD risk factors. The finding that personal experience with AD is related to perceived AD threat is consistent with prior research. 13 We found that perceived AD threat was significantly greater for those with a family history of AD (eg, spouse/partner, first degree relative) compared to those with no experience. The effect did not hold up for those who knew someone with AD but not a spouse or first-degree relative. This suggests that having a close family member with AD (whether genetically-related or not) may lead to heightened concerns about developing AD, whereas just knowing someone with AD may not confer the same effect. This likely reflects an awareness that family history and genetics are important contributors to AD risk. Those who have a close family member with AD may also experience more day-to-day contact with the person, or have taken on a caregiving role. In contrast to our study, Suhr and Kinkela conceived of personal experience as strictly genetic (ie, first or second degree relative) or nongenetic (ie, knowing someone not genetically related to them, including a spouse), and found that personal experience was significantly associated with perceived AD threat regardless of whether it was genetic or nongenetic. 13 Slight differences in categorization of personal AD experience (ie, spousal/partner relationships) may account for why our study did not also find a significant effect among those who knew someone with AD. Future research should determine whether the degree of personal closeness and contact with persons who have AD plays a role in perceived AD threat, above and beyond genetic relatedness.
Consistent with our hypotheses, having a greater number of depressive symptoms was significantly associated with higher perceived AD threat. Other studies have found similar associations between perceived AD threat and depressive symptoms 13,16 or distress symptoms related to AD experiences. 14,27 Given that we cannot determine cause-effect relationships, we can only speculate as to the reasons behind the observed association between perceived AD threat and depressive symptoms. One explanation is that depression itself can affect memory and cognition, 40 -42 which in turn may influence self-rated memory and perceived AD threat. Symptoms of depression often include forgetfulness, confusion, difficulty concentrating, and other cognitive or memory-related problems that could be misinterpreted as AD symptoms. Another possible explanation is that personal concerns and worry about developing AD may lead to more depressive symptoms.
We also found significant associations between personal beliefs about risk factors for AD and perceived threat. As hypothesized, stronger endorsement of the importance of stress or genetics as risk factors were significantly associated with greater perceived threat. The fact that both genetic and psychosocial (ie, stress) contributors to AD risk were strongly endorsed by respondents suggests an awareness that the disease isn’t strictly genetically or environmentally determined, but that both factors are important. The association between these risk factor beliefs and heightened perceived AD threat may also indicate that respondents who strongly endorse genetics or stress as risk factors may feel they have less control over the disease and view it as less preventable. Hiraki and colleagues also found that strong beliefs about genetics as an important risk factor was associated with higher perceived risk of AD, and attributed this finding to the fact that genetic disease is often viewed among the public as more severe and uncontrollable. 26
Perceived AD threat was found to be significantly higher for those with poorer self-rated memory, and those with lower cognitive function. This is consistent with our hypothesis that individuals who perceive they have memory problems, or who have lower cognitive function, will also have greater concerns about AD. Cutler and Hodgson found a similar association between self-assessments of memory functioning and concerns about developing AD in a small sample of adult children with a living parent with probable AD and those with no family history. 15 Specifically, negative assessments of memory functioning were associated with greater personal concerns about developing AD. Prior research has also found evidence that worse cognitive performance is significantly correlated with higher AD threat in individuals with nongenetic AD experience. 13 Similarly, we explored potential interaction effects of personal experience with AD on cognitive factors and perceived AD threat. We found a significant moderating effect of personal experience on subjective memory complaints and perceived threat, but not for objective cognitive function. The direction of this relationship suggests that those with a spouse or first degree relative with AD have higher perceived AD threat when they have more subjective memory complaints. One potential explanation for this is that the experience of having a close family member with AD may cause individuals to engage in more symptom-seeking behavior, 8 leading to misinterpretation of cognitive errors and greater concerns about AD. Thus, this finding may reflect the experience of the “worried well” in that family experience with AD may be playing a role in whether memory errors are interpreted as a disease threat. Whereas when an individual is experiencing actual cognitive decline, perceived threat may be less a function of family experience and more related to an individual’s own declining health.
Age was the only demographic characteristic that was significantly associated with perceived AD threat in the multivariate linear model. Our findings revealed that perceived threat was significantly greater for those aged 50 to 64 and 65 to 74 than for those aged 75 and older. Prior research has found associations between younger age and higher levels of perceived AD threat. 13,14 This runs contrary to actual risk of AD, which increases with age. Nonetheless, younger individuals who are at or nearing age 65 may be more focused on future planning issues, and may feel particularly vulnerable given that disease onset typically occurs after this age. Those older than 75 years may be relieved they don’t already have dementia, less anxious about the future, and more inclined to “let the chips fall where they may.” There may also be possible cohort effects at play, as baby boomers tend to be more health-focused than the WWII generation preceding them. For instance, middle age adults are more likely to seek predictive genetic testing for AD than older adults. 43 We also observed a significant moderating effect of family experience with AD on the relationship between age group and perceived AD threat. In those who had family experience with AD, younger age was significantly associated with greater perceived AD threat. This finding is consistent with prior studies which have found that in those with genetic experience with AD, younger age is significantly associated with higher perceived threat. 14,27 This suggests that personal experience with a close family member who has AD may heighten perceived threat especially among younger individuals.
There are several limitations to the present study. First, to minimize participant burden, the HRS requires that experimental modules be kept brief (∼3 min), necessitating the use of shortened scales for perceived AD threat and AD knowledge. In the case of AD knowledge, the 2 items used in this study were chosen to assess knowledge of certain risk and protective factors for AD, and may not reflect the full range of an individual’s understanding or knowledge about AD. Full scales would have allowed for a more in-depth examination of these factors with increased reliability of measures, and we recommend the use of full validated instruments in future studies. 14,31 Despite this limitation, we believe that the AD knowledge measure provides useful insight into respondents’ understanding of AD. The first item assesses understanding of AD protective factors (whether prescribed drugs that prevent AD are available), while the second item assesses understanding of an important risk factor (whether having a parent or sibling with AD increases the chance of developing it). Second, the supplemental survey module was administered in the 2010 wave of the HRS survey, which did not include a measure to assess help-seeking behavior for memory complaints. It was therefore not possible to examine the association between perceived AD threat and whether participants had sought help or intended to seek help for memory concerns. While the link between perceived threat and health behavior has a well-established theoretical and empirical basis, it would be informative for future research to examine this association using a diverse and nationally representative sample. Third, the cross-sectional nature of this study did not allow us to investigate causality (all findings were correlational) or examine variable relationships across time. Future studies should take a longitudinal approach to further examine predictors of perceived AD threat, as well as the relationship between perceived AD threat and help-seeking intentions or behavior. Lastly, this study draws upon existing theoretical frameworks, as well as previous work from smaller scale studies identifying factors related to perceived AD threat, but does not formally test any specific theory or framework. This might weaken our study findings in terms of connecting to existing theories. While our data set did not allow for formal testing of health behavior theories, future work should seek to formally test existing theories using population-based data.
Despite these limitations, to our knowledge this is the first study of perceived AD threat using nationally representative data from a large and diverse sample of participants. As the prevalence of AD rises in the United States over the coming years, more people will have personal experience with a family member who has the disease. As this happens, public awareness and concerns about AD will also grow, as will public interest in early diagnostic testing. Therefore, there is a need to understand perceived AD threat in the general aging population. As the findings of this study suggest, perceived AD threat is not just a function of an individual’s cognitive impairment, but a response to a complex set of determinants that include personal beliefs and experiences, and psychological well-being. While this study does not examine the association between perceived AD threat and health actions, perceived AD threat may affect a range of behaviors including the decision to seek medical help. Given the important roles that personal beliefs, experiences, and subjective memory complaints play in perceived AD threat, continued public education efforts are needed that focus on how to distinguish between early signs of dementia and mild cognitive changes that occur as part of normal aging, when to consult a health-care professional, and what prevention and treatment options are available. There is also a need to reduce stigmatization of the disease and raise awareness of the benefits of early AD diagnosis. A moderate level of perceived AD threat may be necessary in motivating older adults to seek help for concerns about cognitive changes, but high levels of perceived AD threat may potentially lead to unnecessary and frequent health-care visits, misdiagnosis, or other harms. Future research should examine the conditions under which perceived AD threat may either benefit or adversely affect patients and health-care systems.
Information about factors likely to drive help-seeking behavior for AD concerns will be particularly helpful for formulating diagnostic guidelines and practices among health-care professionals. For instance, our finding that family experience moderates the association between self-rated memory and perceived threat, but not objective cognitive function, highlights the need for careful initial cognitive screening of individuals who present with memory complaints, which includes objective measures of cognitive functioning and informant history. There are many causes of cognitive difficulties, and patients and health-care providers need to be educated about nondementia factors that can influence subjective memory perceptions and objective cognitive function. Factors such as family experience with AD and depressive symptoms should be taken into consideration during patient visits. Future research should focus on further delineating the relationships between perceived AD threat and family experience, as well as its role in help-seeking behavior.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.E.O. was supported by a predoctoral traineeship in Public Health & Aging at the University of Michigan (T32 AG027708), and a Summer Writing Award from the Department of Health Behavior and Health Education in the U-M School of Public Health. J.S.R. was supported by NIH grant P30 AG053760 (Michigan Alzheimer’s Disease Center). The HRS (Health and Retirement Study) is sponsored by the National Institute on Aging (grant number NIA U01AG009740) and is conducted by the University of Michigan.