
Abstract
The objective of our study was to demonstrate that living with a person affected by mild to moderate Alzheimer’s disease can lead to an increased perception of the caregiver’s burden using the Caregiver Burden Inventory (CBI). The sample consisted of 153 dyads, caregiver–patient. At baseline, a greater perception of the caregiver’s burden was observed in the live-in caregivers. A further increase in the total burden of the live-in caregivers was noticed at the 6-month follow-up. More specifically, with the inclusion of correction factors such as the caregiver’s age and the CBI subscales at baseline, the social and emotional burden becomes statistically significant (P < .001). The present paper confirms our hypothesis that live-in caregivers perceive a greater burden than nonlive-in, and this difference increases further after 6 months. The difference in involvement between live-in and nonlive-in caregivers could be the foundation to tailor more specific interventions.
Introduction
The care of people affected by Alzheimer’s disease (AD) is often very challenging and burdens the whole family. The family’s quality of life and the psychophysical well-being can be negatively affected, 1,2 due to the effects of a disabling disease such as dementia. The caregiver is a figure with an increasing role in Western societies. It is becoming more and more common because of the increase in the average life expectancy, the aging population, and the decrease in mortality due to preventive diagnostics and treatments. Ory et al 3 define caregiver burden as an impact on the family caused by the patient’s cognitive–behavioral changes. Other authors describe the burden as multidimensional and subjective, emphasizing the global impact on the caregiver caused by the care needs and the physical, psychological, social, and economic demands involved in taking care of such patients. 4,5,6
According to a widely accepted cognitive model, 7 also evaluated in the caregiving context, 8,9 stress increases when an individual perceives a lack of resources to address a situation considered dangerous. Pearlin’s stress process model, 8 integrated by Schultz 10 and Noonan, 11 and revised by Conde-Sala et al in 2010, 12 takes into account the multidimensional evaluation of burden as well as the interventions; furthermore, it stresses that the issues pointed out by caregivers cannot be considered homogeneous or uniform due to factors related to both caregivers and patients. 13 In the caregiver experience, it is important to understand how positive aspects of caring relate to the negative consequences such as burden and depression. 14 Interventions to support caregivers have become a priority, since they seem to improve their quality of life and indirectly the quality of life of the loved ones for whom they care. 15 The main social and emotional issues that live-in caregivers have to deal with while caring for a patient could be the objective of very specific interventions based on the real needs the caregivers have in this distinct role.
Many researchers have identified the causes of the different incidence of the caregiver burden on the contextual factors, on factors related to caregiving, and on primary stressors. 5,6,10,16 In our previous descriptive study, we showed that in patients diagnosed with mild to moderate AD, a greater burden was felt by the live-in group compared to the nonlive-in group. 17
The objective of the study was to demonstrate that living with a person with mild to moderate AD increases the burden of live-in caregivers compared to the nonlive-in, even after 6 months. To that end, we correlated the caregivers’ burden (live-in/nonlive-in) with their sociodemographic characteristics and in reference to the functional, cognitive, and behavioral aspect of patients with mild to moderate AD. Up to date, there is a need for studies on the caregivers’ different perception of the burden in the short term in patients with mild to moderate AD. These studies should focus on keeping the sociodemographic characteristics of caregivers and patients constant, avoiding any intervention on them.
The identification of the key factors capable to affect the perception of the caregiver burden has become essential, since it represents the foundation to tailor interventions aimed at all different issues caused by the care of patients with mild to moderate AD.
Methods
From January 2011 to January 2012, 159 caregiver–patient dyads have been enrolled in the study, referred by the Unità Valutativa Alzheimer (Alzheimer Evaluation Unit) of the Italian National Research Center on Aging (INRCA), Ancona, Italy. Patients were diagnosed with AD according to National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association criteria. Patients with a score of 10 to 26 (mild to moderate AD according to Perneczky) 18 in the Mini-Mental State Examination (MMSE) were included; they lived in their own home and were assisted by family members. Patients with severe AD (MMSE <10 according to Perneczky) 18 and those living in nursing homes were excluded. Six months after the patients had been taken into the Unità Valutativa Alzheimer’s care, the sample decreased; 2 patients moved to a different city, 3 did not come back for the 6-month follow-up visit, and 1 patient died. Therefore, the study was on a sample of 153 dyads, caregiver–patient, 112 live-in and 41 nonlive-in. The dyads did not change their life conditions during follow-up. Caregivers’ sociodemographic information were collected, including age, gender, living arrangements with the patient, family relationship to the patient.
A cognitive test was administered to the patient: Mini-Mental State Examination
19
: This is a global cognitive assessment tool.
The following tests regarding functional independence and noncognitive disorders relative to the sick loved ones were administered to the caregivers: Activities of Daily Living (ADL)
20
: This assesses the ability of independently carrying out the basic tasks of everyday life, such as taking a shower, getting dressed, going to the bathroom, eating, ambulation, and continence. Instrumental Activities of Daily Living (IADL)
21
: This assesses the ability of carrying out instrumental activities of daily life, such as using a telephone, going shopping, cooking, taking care of the house, doing laundry, using public transportation, taking medicines, and managing money. Neuropsychiatric Inventory (NPI)
22,23
: This is a scale to assess the frequency and severity of 12 psychic and behavioral symptoms, such as delusions, hallucinations, agitation, depression, anxiety, euphoria, apathy, disinhibition, lability, aberrant motor behavior, sleep and nighttime behavior disorders, and eating disorders.
In addition, caregivers completed a questionnaire to measure burden: Caregiver Burden Inventory (CBI)
24,25
: It is a self-administered questionnaire to assess the perceived burden by caregivers of people with dementia. It includes 24 items divided into 5 subgroups, namely, (1) objective burden associated with the family member’s time restrictions; (2) developmental burden relative to feeling “out of sync” with respect to their peers’ expectations and opportunities; (3) physical burden relative to tiredness and issues of somatic health; (4) social burden relative to role’s conflicts with job and with the other family members; and (5) emotional burden associated with feelings of shame and embarrassment.
Statistical Analysis
SPSS (ver. 19) package software was used for the statistical analysis. Differences between live-in and nonlive-in participants were compared by univariate analysis using the independent sample Student’s t test (t) for continuous variables and the chi-square test for categorical variables. In the first step, to analyze the differences of clinical characteristics between live-in and nonlive-in patients, 1-way analysis of variance for repeated measure was performed to evaluate the change over 6 months. The analysis of covariance (ANCOVA) was performed to increase the precision of comparisons between groups by accounting for the variation in caregiver’s age and the baseline value of CBI scores. P value less than.05 was considered statistically significant. The reported P values were 2 tailed in all calculations.
Results
Table 1 summarizes the main sociodemographic characteristics of the caregiver and the patient samples studied. In these samples, the gender distribution shows that among live-in and nonlive-in, the majority is represented by women. The live-in group shows an age significantly higher than the nonlive-in group.
Sociodemographic Characteristics of Patients and Caregivers.
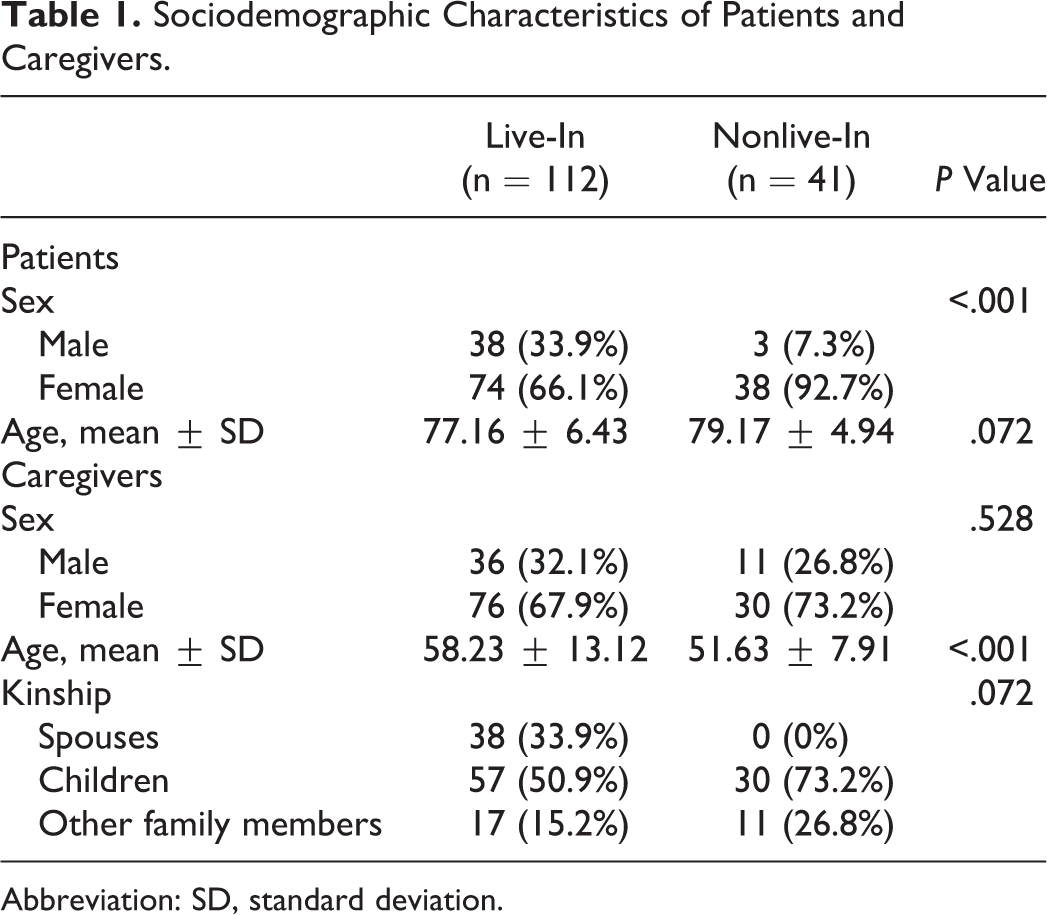
Abbreviation: SD, standard deviation.
At baseline, no significant difference was noted between live-in and nonlive-in patients as regards to age (t = 1.813; P = .072) and some of the clinical characteristics, namely, MMSE (t = 0.654; P = .514), ADL (t = 1.698; P = .092), and NPI (t = 1.268; P = .207); IADL was instead statistically significant (t = 3.129; P = .002).
After 6 months, the cognitive (MMSE; paired t = 8.92; P < .001) and functional assessments (IADL paired t = 11.56, P = .010; ADL paired t = 20.00, P < .001) worsened in all patients. The psychic and behavioral assessments were not significant at baseline and were unchanged after 6 months (Table 2).
Clinical Characteristics of Live-In and Nonlive-In Patients at Baseline and After 6 Months.
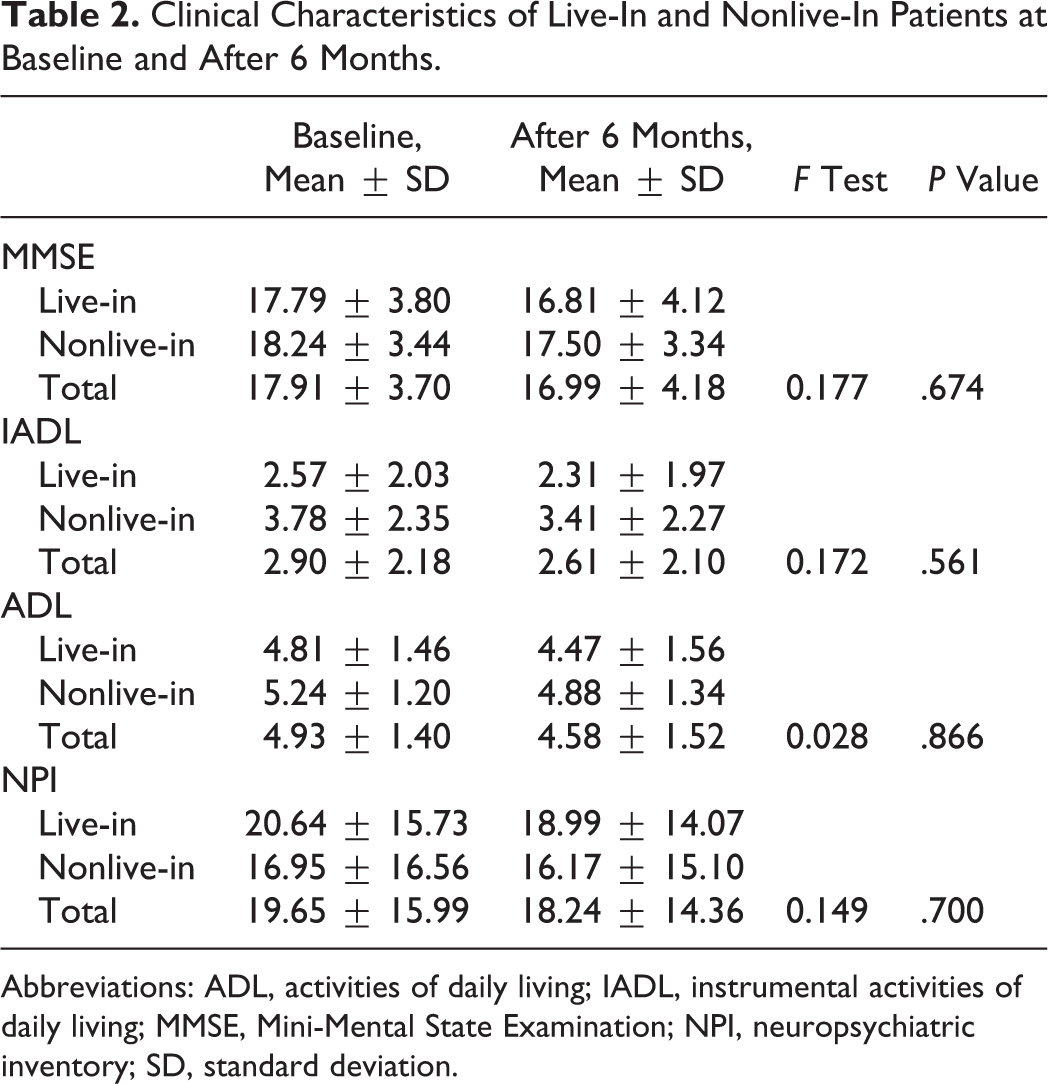
Abbreviations: ADL, activities of daily living; IADL, instrumental activities of daily living; MMSE, Mini-Mental State Examination; NPI, neuropsychiatric inventory; SD, standard deviation.
At 6 months, the total sample of caregivers showed a significant increase in burden in all subscales (CBI-1 paired t = 4.382, P < .001; CBI-2 paired t = 3.305, P = .001; CBI-3 paired t = 2.707, P = .008; CBI-4 paired t = 2.145, P = .034; CBI-5 paired t = 3.807, P < .001) and in the CBI total scale (CBI-6 paired t = 5.239, P < .001). With regard to sharing a residence with the patient, live-in caregivers showed a greater total burden compared to nonlive-in caregivers after 6 months. For all CBI subscales, ANCOVA was used to compare the 2 groups of live-in and nonlive-in caregivers, using the caregiver’s age and CBI single subscales scores at baseline as covariates. In particular, the social burden and the emotional burden subscales appeared significantly higher in the live-in caregivers than in the nonlive-in group (Table 3). The data analysis in our sample shows that living with the patient is the only index to determine the increased perception of the caregiver burden.
The CBI Characteristics of Caregivers at Baseline and After 6 Months.
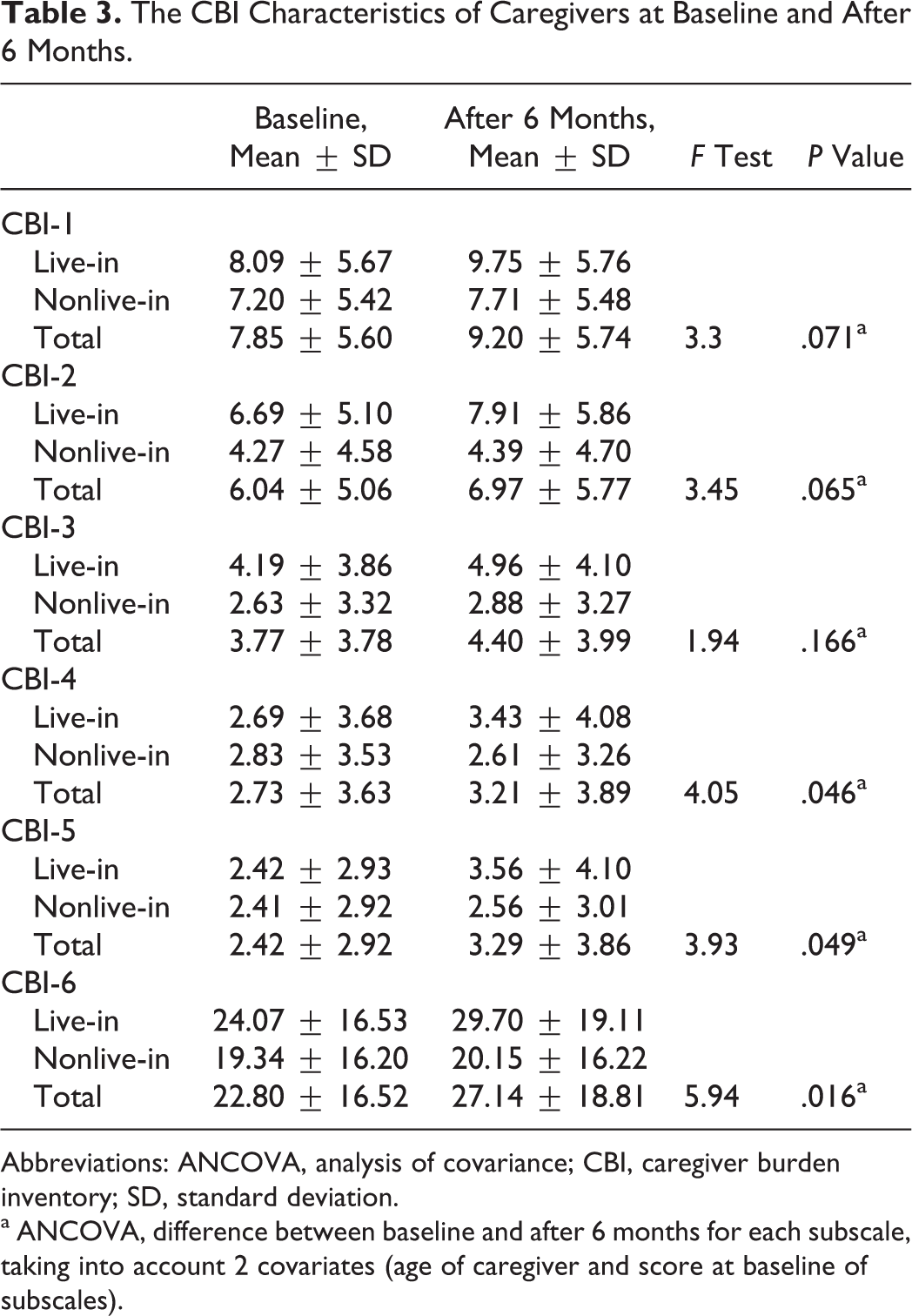
Abbreviations: ANCOVA, analysis of covariance; CBI, caregiver burden inventory; SD, standard deviation.
a ANCOVA, difference between baseline and after 6 months for each subscale, taking into account 2 covariates (age of caregiver and score at baseline of subscales).
Discussion
Alzheimer’s disease is a degenerative pathology that leads to the dissolution of the patient’s self, and over time, the level of interaction with other people is reduced to a caregiving relationship. 26 The caregiving experience is sometimes extremely stressful 8 and often associated with feelings of guilt and helplessness. 27
The care of patients with dementia is very complex and puts at great strain the psychophysical balance of the caregiver and the entire family. 5,6,28,29
In the literature, there are several socioeconomic and clinical variables regarding the dyads (caregiver–patient) that can influence the caregiver burden when patients affected by AD are involved. With respect to the variables related to the caregivers, some authors have studied kinship and found out that spouses report a high level of stress, 10,25,30,31 and this seems to be an independent risk factor for mortality. 9,32 Furthermore, female spouses report the perception of a greater emotional burden compared to a male caregiver. Live-in children report a great burden, as spouses do, 12,33 in particular in relation to the objective burden. 17 Women perceive higher levels of objective, developmental, physical, and social burden than men. 34
The patient’s characteristics also have an impact on the caregiver’s burden. As the ability of daily living activity decreases, the caring burden increases. 25,35,36,37 In particular, the objective burden increases with the decrease in the patient’s functional independence. 17 Conversely, other studies have found no correlation between the patient’s functional decline and the caregiver’s burden. 38,39,40 The degree of cognitive deterioration does not seem to have a significant impact on burden for spouses and children. 12,17 The behavioral and psychic disorders of the patient seem to be associated with an increase in the caregiver burden, 17,41,42 but they do not seem to have a significant impact in mild to moderate AD. 12,13
In our previous study, 17 the living-in factor already explained the greater perception of the caregiver burden 12,13 in reference to physical and developmental burden.
The aim of this study was to evaluate the perception of burden in the natural history of mild to moderate AD. After analyzing the contextual and more important factors relative to the caregiver and to the patient (Table 1), this study shows that the cohabitation factor affects the greater perception of burden by the live-in caregivers compared to the ones who do not live with the patient. In fact, in the whole sample, all CBI subscales increased at follow-up, and when considering cohabitation, caregiver’s age, and baseline CBI values, live-in caregivers showed an increase in social and emotional issues caused by caring for their loved ones. Both groups of patients showed a cognitive and functional worsening, indicating that the increase in the live-in caregiver burden is not justified by the different clinical worsening of the patients. Furthermore, psychic and behavioral disorders were not observed in these patients at baseline 17 nor after 6 months.
Our data confirm the initial hypothesis; living with a patient seems to be the main factor that explains the greater perception of burden by live-in caregivers even after a period of time. In particular, the increase in social burden (CBI-4) and emotional burden (CBI-5) represents a specific burden profile, showing the issues that live-in caregivers face in their assistance efforts. Our study has some limitations. First, participants in our study were recruited from a specialized clinical center, the Alzheimer Evaluation Unit, INRCA, Ancona, and so this is not a population study. Second, the sample used was adequate to study the effect of age and baseline burden of the caregiver, but its relatively small size did not allow to investigate the effects of other variables, such as the stage of dementia (mild vs moderate), caregiver’s sex (male vs female), and the kinship (daughter/son vs spouse carer) on the caregiver’s burden. In order to confirm our results and study more deeply the burden in caregivers of different sex and family relationship, there is a need for studies with a larger sample. This profile can be considered as a base on which personalized interventions could be tailored. The challenges relative to role’s conflicts with job and with other family members, and the feelings of shame and embarrassment that live-in caregivers show when taking care of their loved ones, could be the privileged objects of therapeutic and supportive interventions, while for the nonlive-in caregivers, a more informative intervention seems more appropriate.
Footnotes
Acknowledgments
The authors would like to thank Mrs Maria Rita Pignatelli for her assistance and supervision in the translation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.