
Abstract
Little research exists examining the relationship between beta-amyloid neuritic plaque density via [18F]flutemetamol binding and cognition; consequently, the purpose of the current study was to compare cognitive performances among individuals having either increased amyloid deposition (Flute+) or minimal amyloid deposition (Flute−). Twenty-seven nondemented community-dwelling adults over the age of 65 underwent [18F]flutemetamol amyloid-positron emission tomography imaging, along with cognitive testing using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) and select behavioral measures. Analysis of variance was used to identify the differences among the cognitive and behavioral measures between Flute+/Flute− groups. Flute+ participants performed significantly worse than Flute− participants on RBANS indexes of immediate memory, language, delayed memory, and total scale score, but no significant group differences in the endorsed level of depression or subjective report of cognitive difficulties were observed. Although these results are preliminary, [18F]flutemetamol accurately tracks cognition in a nondemented elderly sample, which may allow for better prediction of cognitive decline in late life.
Introduction
A key feature of the neuropathology of Alzheimer’s disease (AD) is the accumulation of amyloid plaque deposits in the brains of individuals with the disease. 1 –3 Over the past 2 decades, imaging substrates have been developed to identify the deposition of amyloid in patients with either AD or mild cognitive impairment (MCI) prior to autopsy. 4 [18F]Flutemetamol 5 is a radioactive diagnostic agent (Vizamyl; GE Healthcare, Wauwatosa, Wisconsin) indicated for positron emission tomography (PET) imaging of the brain to estimate beta-amyloid neuritic plaque density in adult patients who are being evaluated for AD or other causes of cognitive decline. 6 It has a molecular structure modeled off the successful Pittsburgh Compound B, or [11C]PiB, 7 while possessing the extended half-life of [18F]fluorine with properties similar to other [18F]fluorine-based PET amyloid imaging agents. 8 [18F]Flutemetamol uptake has shown high concordance with [11C]PiB in patients with AD and MCI 9,10 or normal cognition, 10,11 and also has displayed comparable findings with histology studies examining amyloid binding in vivo. 12,13 Additionally, when used with magnetic resonance imaging (MRI), [18F]flutemetamol has been shown to incrementally improve diagnostic specificity 14 in amnestic MCI and AD patients and improve the prediction from MCI to AD. 15
Although previous investigations have supported [18F]flutemetamol as a reliable imaging agent, little research has been undertaken to date specifically examining the relationship between [18F]flutemetamol amyloid binding and cognition. One study identified that while increased amyloid burden was observed using [18F]flutemetamol for healthy controls displaying higher levels of subjective memory complaints, there was no association between [18F]flutemetamol binding and episodic memory performance. 16 Similarly, although Duara and colleagues 14 identified differences in [18F]flutemetamol uptake between cognitively intact, MCI, and AD participants, the relationships between amyloid accumulation and episodic memory or verbal fluency were nonsignificant among all 3 groups. Conversely, Duff and colleagues 17 observed that increased [18F]flutemetamol binding was significantly associated with decreases in delayed memory, visual spatial construction, and language in nondemented adults (MCI and normal cognition), with this relationship being further strengthened when factoring in premorbid intellectual functioning.
The current study was undertaken to better understand the relationship between cognition and amyloid accumulation/deposition using [18F]flutemetamol. Additionally, the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) 18 has been increasingly used as a measure of cognition in clinical drug trials, particularly as AD-related drug trials are attempting to enroll patients in more preclinical stages of the disease. Consequently, a more thorough understanding of the relationship between amyloid deposition and RBANS performance will be worthwhile in cognitively normal patients and those with MCI. It is hypothesized that increased [18F]flutemetamol uptake will be significantly associated with decreased RBANS delayed memory performance in our sample of nondemented individuals, above and beyond the impact of premorbid intellectual functioning.
Methods
Sample and Design
Twenty-seven nondemented older adults over the age of 65 were recruited either from a cognitive disorders clinic or through community presentations on brain health at independent living facilities and senior centers. Exclusion criteria included an International Classification of Diseases, Tenth Revision diagnosis of dementia; medical comorbidities likely to affect cognition (eg, history of major neurological disorders including strokes, brain lesions, head injury with loss of consciousness >30 minutes, radiation therapy to the brain, major psychiatric disorders [schizophrenia, bipolar disorder, severe major depressive disorder], or substance abuse); and use of anticonvulsant or antipsychotic medications. Three patients were prescribed donepezil and 1 participant was prescribed memantine at the time of the study. This study followed an observational design, and sampling procedures were based on convenience sampling.
Neuropsychological and Behavioral Self-Report Measures
All participants were administered the following neuropsychological and behavioral tests:
The RBANS
18
is a neuropsychological test battery comprising 12 subtests that are used to calculate the index scores for domains of immediate memory, visuospatial/constructional, attention, language, delayed memory, and global neuropsychological functioning. The RBANS has been extensively researched and found to be effective at both detecting cognitive decline in a number of conditions (probable AD,
19
stroke,
20
and schizophrenia
21
) and characterizing dementia from different etiologies (probable AD and Huntington disease
18
). Across a 1-year retest interval, stability coefficients for the RBANS from a community-dwelling elderly sample ranged from 0.58 to 0.83 for the index scores, and from 0.51 to 0.83 for the subtest scores, with practice effects being largely absent.
22
The index scores utilize age-corrected normative comparisons to generate standard scores (SSs; M = 100, standard deviation [SD] = 15). The Wide Range Achievement Test IV (WRAT)–Reading subtest
23
was used as an estimate of premorbid intellectual functioning. In this task, participants were presented a form that lists 55 words, many of which cannot be sounded out phonetically, and were asked to loudly pronounce out each word accurately. The number of correct responses was summed and then normative comparisons were utilized to create age-matched SSs (M = 100, SD = 15). The Geriatric Depression Scale (GDS)
24
is a 30-item self-report questionnaire related to current depressive symptomology. Participants were asked to respond to questions in a “yes/no” format that best fit how they felt over the past week (eg, “are you basically satisfied with your life?”). Each positive endorsement of depressive symptoms was worth 1 point, for a range of scores from 0 to 30. Higher scores indicated more severe depression, with severity ranges being 0 to 9 for normal mood, 10 to 19 for moderate depression, and 20 to 30 for severe depression.
24
The Cognitive Failures Questionnaire (CFQ)
25
is a 25-item self-report questionnaire related to current perceptions of cognitive functioning. Participants were asked to indicate the frequency that they experienced the commonly occurring events related to memory loss (eg, “Do you forget appointments?”) using a scale of 0 (never) to 4 (very often). Total scores ranged from 0 to 100, with higher scores indicating greater subjective complaints of cognitive functioning.
Amyloid Imaging
Participants underwent [18F]flutemetamol imaging as described previously. 17 [18F]Flutemetamol was produced under PET Current Good Manufacturing Practice (cGMP) standards, and the studies were conducted under an approved Federal Drug Administration Investigational New Drug application. Imaging was performed 90 minutes after the injection of 185 mBq (5 mCi) of [18F]flutemetamol. Emission imaging time was approximately 30 minutes. A GE ST PET/computed tomography scanner (GE Healthcare) was used for [18F]flutemetamol imaging in this study, which possessed the full width at half-maximum spatial resolution at 5.0 mm. The field of view for reconstruction was set to 25.6 cm on the scanner to generate a pixel size of 2.0 × 2.0 mm (image matrix size 128 × 128). The native slice thickness was 3.27 mm. Volumes of interest were automatically generated by the CortexID Suite analysis software (GE Healthcare), with Z axis dimensions substantially larger than the slice thickness. [18F]Flutemetamol binding was analyzed using a regional semi-quantitative technique described by Vandenberghe et al 9 and refined by Thurfjell et al. 26 In this technique, semi-quantitative regional (prefrontal, anterior cingulate, precuneus/posterior cingulate, parietal, mesial temporal, lateral temporal, occipital, sensorimotor, cerebellar grey matter, and whole cerebellum) and global composite standardized uptake value ratios (SUVRs) in the cerebral cortex were generated automatically and normalized to the pons using the CortexID Suite software. 27 This software uses a threshold z score of 2.0 to indicate abnormally increased regional amyloid burden that corresponds to a composite SUVR of approximately 0.59 to 0.62 when normalized to the pons, providing a 99.4% concordance with visual assessment. 26 For [18F]flutemetamol amyloid imaging, there is no specific age-related “normal” level of binding in the CortexID Suite database to assess age-matched normality. Therefore, the study images were compared to the intrinsic software database control group (of >100 amyloid negative flutemetamol healthy controls from GE Healthcare) as a whole to calculate the z scores compared to clinically negative amyloid scans.
Procedure
All procedures were approved by the local institutional review board before the study commenced. Participants provided informed consent before completing any procedures. As part of a larger study, participants completed a neuropsychological test battery to characterize their performances based on relevant cognitive domains, including the Hopkins Verbal Learning Test–Revised, 28 the Brief Visual Memory Test–Revised, 29 Symbol Digit Modalities Test, 30 Trail Making Test Parts A and B, 31 and the WRAT. Participants performing below expectation on those cognitive tasks based on premorbid estimates were classified as MCI using Winblad criteria 32 and participants performing within or beyond expectations were classified as having normal cognition. Specifically, Winblad criteria for MCI involves the following: (i) the person is neither normal nor demented, (ii) there is evidence of cognitive deterioration shown by either objectively measured decline overtime and/or subjective report of decline by self and/or informant in conjunction with objective cognitive deficits, and (iii) activities of daily living are preserved and complex instrumental functions are either intact or minimally impaired. The result of this classification procedure was that participants with MCI exhibited at least an amnestic profile. Participants classified as having MCI possessed a delayed memory to premorbid intelligence discrepancy of 2.1 SD based on a mean delayed memory composite of SS = 76.8 (SD 17.7) compared to a mean premorbid intellectual functioning of SS = 108.6 (SD 12.8), and participants classified as having normal cognition possessed a discrepancy of 0.1 SD based on a mean delayed memory composite of SS = 112.0 (SD 7.5) compared to a mean premorbid intellectual functioning of SS = 111.2 (SD 4.6). Separate from the diagnostic categorization, participants were then administered the RBANS, CFQ, and GDS, for a total time of approximately 60 minutes of additional cognitive testing. All tests were administered using the standard protocol and scored/normed based on their respective manuals. Participants were invited back for a separate appointment and completed [18F]flutemetamol PET imaging in an average of 19.5 weeks (SD = 5.75) after completing the neuropsychological tests.
Data Analysis
As indicated above, participants were categorized into [18F]flutemetamol-positive or -negative status using a global composite threshold z score of 2.0 (Flute+ equals z ≥ 2.0, Flute− equals z < 1.99). 26 Analyses of variance (ANOVAs) were performed for the continuous demographic variables using the Flute+/Flute− group as the independent variable. For categorical demographic variables (gender and clinical diagnosis), χ2 analyses were performed using the Flute+/Flute− group as the independent variable. Significant demographic variables (education) were covaried in the primary analyses using multivariate analysis of covariance (MANCOVA), with Flute+/Flute− group as the independent variable and age-corrected cognitive performances, levels of depression, and subjective memory complaints as the dependent variables. For supplementary analyses, 2 separate multivariate ANOVA (MANOVA) were conducted for each diagnostic group with Flute+/Flute− group as the independent variable and the neuropsychological and behavioral measures as the dependent variable. Additionally, supplemental correlational analyses were conducted between [18F]flutemetamol z score uptake and age-corrected cognitive performances, levels of depression, and subjective memory complaints. Measures of effect size were expressed as Cohen d or partial η-square (η2) values. For all statistical tests, the α level was set at .05.
Results
Demographics
Table 1 displays demographic, neuropsychological, and behavioral data for the current sample. Eight participants were recruited from the clinic (100% classified with MCI), and 19 were recruited from the community (52% classified with MCI). Of the 27 participants, two-thirds were diagnosed with MCI (n = 18) and the other third was diagnosed with normal cognition (n = 9). Three-quarters of the sample were female. The mean age of the current study was 77.5 years, and the mean level of education was a college degree (16.3 years). Neither age nor education were significantly correlated with [18F]flutemetamol binding, r = −.16, P = .42, d = 0.32, for age and r = .32, P = .11, d = 0.68, for education. Overall, the mean premorbid intelligence of the sample was at the upper limit of the average range relative to normative peers, and within normal limits for peers on RBANS indexes of immediate memory, visuospatial/constructional, attention, learning, delayed memory, and total scale score (see Table 1). The mean raw composite value of [18F]flutemetamol uptake for the sample was 0.63 (SD = 0.18; range 0.41-1.09) and the mean composite [18F]flutemetamol z score was 2.97 (SD = 4.15; range −1.92 to 13.25).
Demographic, Neuropsychological, and Behavioral Variables Across the Total Sample.a,b
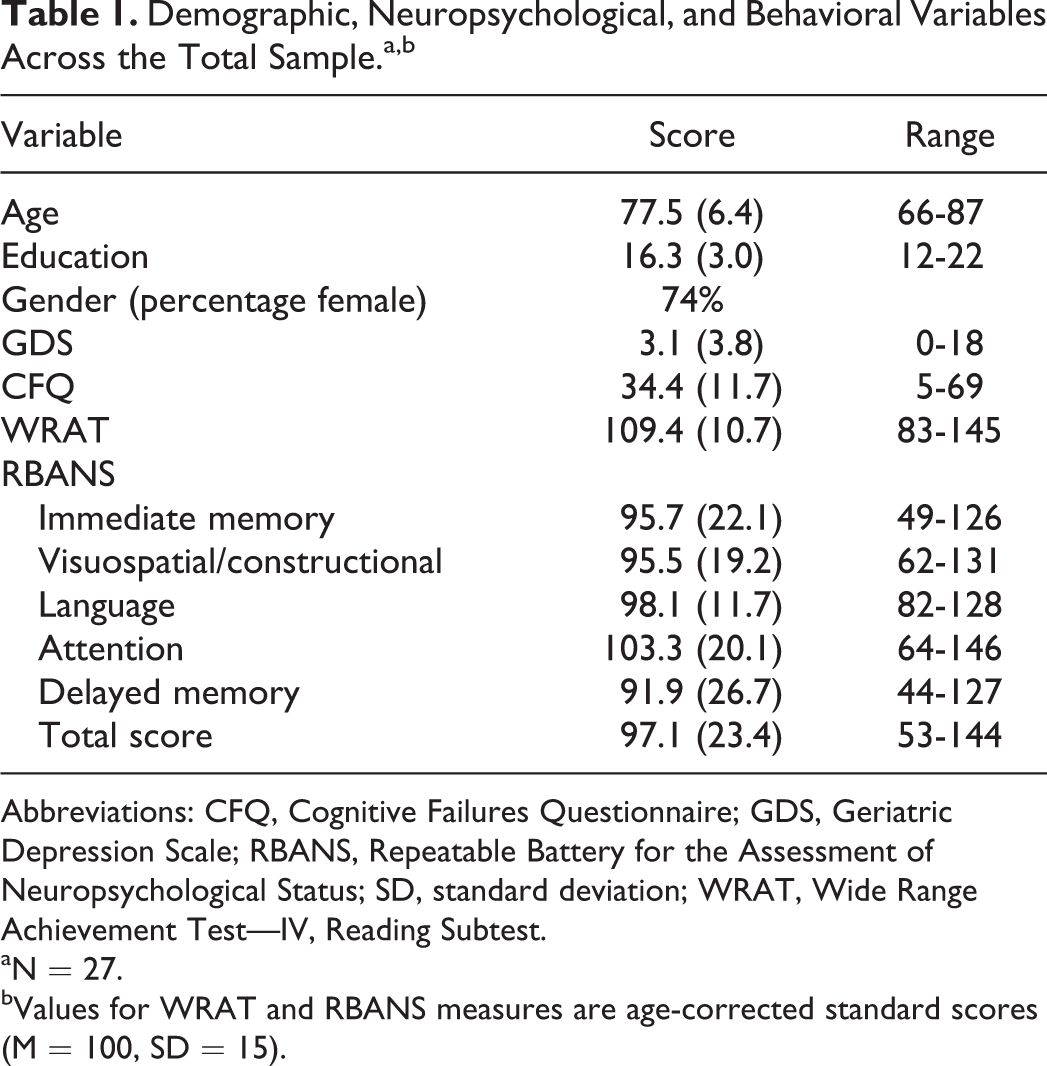
Abbreviations: CFQ, Cognitive Failures Questionnaire; GDS, Geriatric Depression Scale; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; SD, standard deviation; WRAT, Wide Range Achievement Test—IV, Reading Subtest.
aN = 27.
bValues for WRAT and RBANS measures are age-corrected standard scores (M = 100, SD = 15).
Cognitive Performances and Symptom Self-Report Based on [18F]Flutemetamol Classification
In the current sample, 13 participants were classified as having a positive [18F]flutemetamol-PET scan according to previous research, 26 and 14 were classified as having a negative [18F]flutemetamol-PET scan. No statistically significant differences were found among the [18F]flutemetamol groups with respect to age, gender, or premorbid intellectual functioning (all Ps > .05), however the flute+ group possessed a significantly higher level of education than the Flute− group, F(1, 26) = 4.65, P = .04, d = 0.16. Additionally, no statistically significant group differences were observed using χ2 analyses for diagnostic categorizations, χ2 = 1.19, P = .28; specifically, 10 (55%) of 18 participants who were diagnosed with MCI were Flute+, whereas 3 (33%) of 9 normal cognition participants were Flute+.
After controlling for education level, MANCOVA indicated that differences existed between [18F]flutemetamol groups with regard to neuropsychological and behavioral test performances, Wilk λ= .31, F9,16 = 3.95, P = .008, η2 = .69. Specifically, the Flute+ group performed worse than the Flute− group on RBANS indexes of immediate memory, F(1, 24) = 19.07, P < .001, η2 = 0.43; language, F(1, 24) = 7.90, P = .01, η2 = 0.25; delayed memory, F(1, 24) = 26.61, P < .001, η2 = 0.63; and RBANS total scale score, F(1, 24) = 15.32, P = .001, η2 = 0.39. No statistically significant group differences were observed for RBANS indexes of visuospatial/constructional, F(1, 24) = 2.34, P = .145, η2 = 0.09, or attention F(1, 24) = 3.52, P = .07, η2 = 0.13. See Table 2 and Figure 1. No statistically significant differences existed between groups on levels of depression, F(1, 24) = 0.01, P = .98, η2 = 0.00; or subjective report of cognitive difficulties, F(1, 24) = 0.60, P = .45, η2 = 0.03.
Demographics, RBANS, and Behavioral Variables for 18F-Flutemetamol-Positive (Flute+) and -Negative (Flute−) Groups.a,b
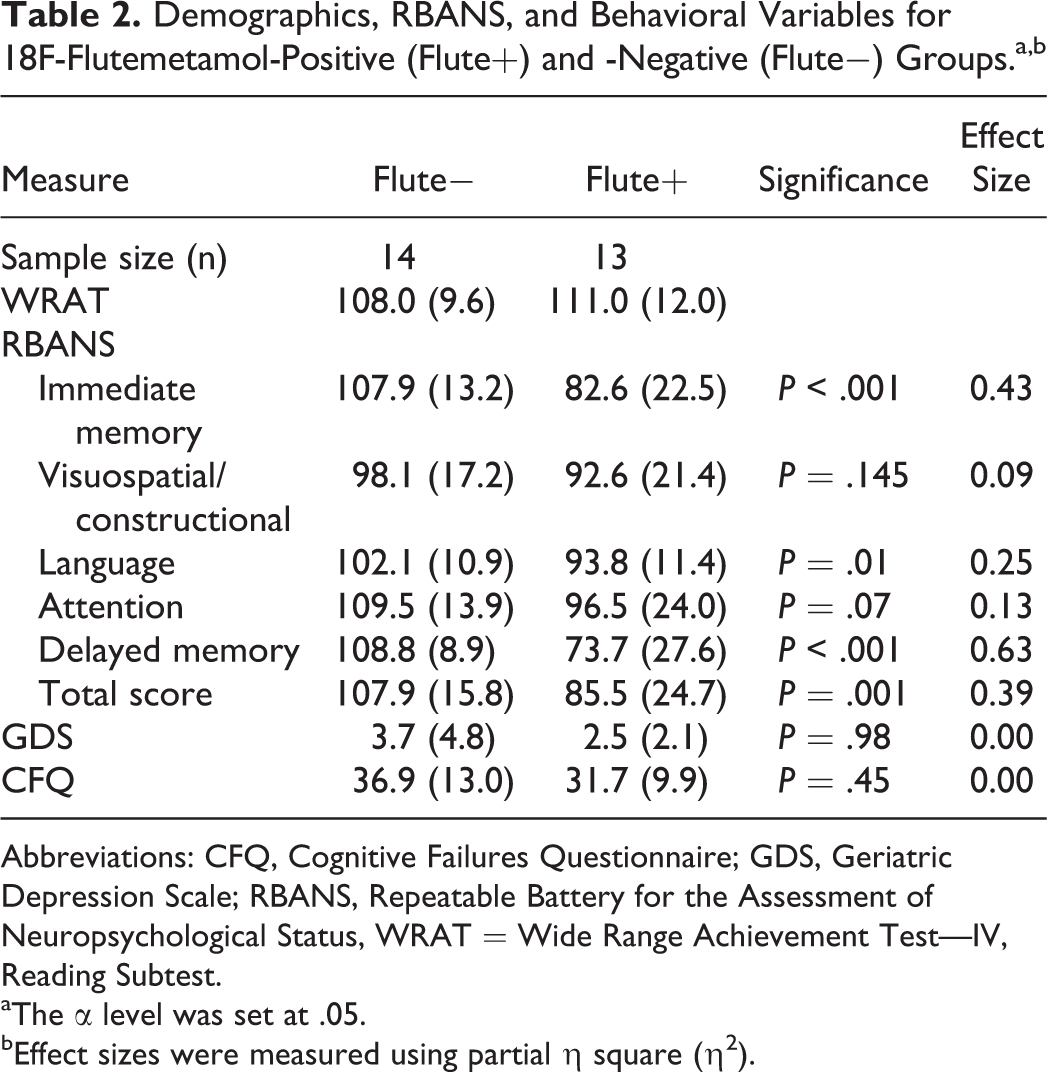
Abbreviations: CFQ, Cognitive Failures Questionnaire; GDS, Geriatric Depression Scale; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status, WRAT = Wide Range Achievement Test—IV, Reading Subtest.
aThe α level was set at .05.
bEffect sizes were measured using partial η square (η2).
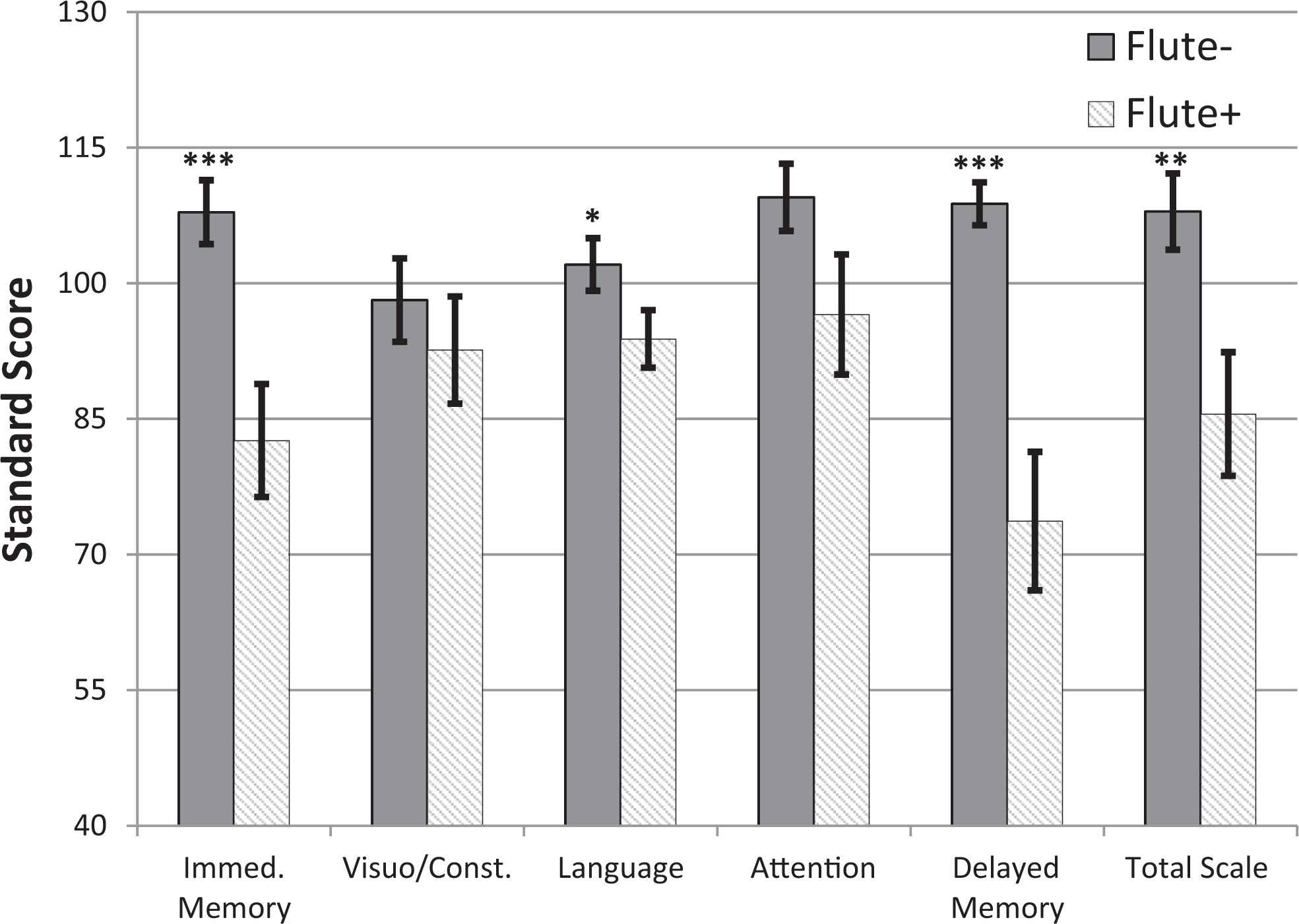
RBANS index performance between [18F]flutemetamol-positive (n = 13) and -negative (n = 14) groups. *Significant difference, P < .05. **Significant difference, P < .005. ***Significant difference, P < .001. Flute− indicates [18F]flutemetamol negative group; Flute+, [18F]flutemetamol positive group; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status.
Supplementary Cognitive Performances and Symptom Self-Report Based on [18F]Flutemetamol Classification Stratified by Diagnosis
Although the sample sizes within the MCI and normal cognition diagnostic categories were small, the value of examining performances on neuropsychological and behavioral tasks for these diagnostic groups based on Flute+ or Flute− status was felt to outweigh the limited conclusions to be drawn. When examining the 9 participants who were diagnosed with normal cognition, no significant differences existed between [18F]flutemetamol groups with regard to RBANS test performances or measures of premorbid intellectual functioning, depression, or subjective report of cognitive difficulties, Wilk λ = .09, F(1, 7) = 1.41, P = .57, η2 = .09.
When examining the 18 participants who were diagnosed with MCI, MANOVA indicated that differences were observed between [18F]flutemetamol groups with regard to neuropsychological and behavioral test performances, Wilk λ = .16, F(9, 8) = 4.64, P = .02, η2 = .84. Specifically, the Flute+ group performed worse than the Flute− group on RBANS indexes of immediate memory, F(1, 16) = 11.11, P = .004, η2 = 0.41; delayed memory, F(1, 16) = 25.33, P < .001, η2 = 0.61; and RBANS total scale score, F(1, 16) = 8.31, P = .01, η2 = 0.34. No statistically significant group differences existed in terms of RBANS indexes of visuospatial/constructional, F(1, 16) = 0.33, P = .57, η2 = 0.02; language, F(1, 16) = 1.32, P = .27, η2 = 0.08; or attention, F(1, 16) = 3.64, P = .08, η2 = 0.18. Additionally, no statistically significant group differences were observed on levels of premorbid intellectual functioning, F(1, 16) = 1.04, P = .32, η2 = 0.06; depression, F(1, 16) = 3.91, P = .07, η2 = 0.20; or subjective report of cognitive difficulties, F(1, 16) = 1.52, P = .24, η2 = 0.09.
Supplementary Analysis of the Correlations Between Neuropsychological and Self-Report Measures and [18F]Flutemetamol Imaging
Significant negative correlations existed between [18F]flutemetamol binding and RBANS indexes of immediate memory, r = −.69, P < .001, d = 1.91; language, r = −.42, P = .03, d = 0.93; attention, r = −.41, P = .03, d = 0.90; delayed memory, r = −.73, P < .001, d = 2.16; and total scale score, r = −.61, P = .001, d = 2.13. These results suggested that cognitive performance was significantly worse in those participants with higher [18F]flutemetamol uptake. Although a trend was present, no significant associations were observed between [18F]flutemetamol binding and the RBANS index of visuospatial/constructional, r = −.33, P = .09, d = 0.70. Additionally, no association was observed between [18F]flutemetamol binding and an estimate of premorbid intellectual functioning, r = −.07, P = .75, d = 0.13; depression levels, r = −.12, P = .66, d = 0.24; or subjective report of cognitive difficulties, r = −.09, P = .67, d = 0.17.
Further, no significant associations were observed between RBANS indexes and subjective report of cognitive difficulties (r = .04, P = .83, d = 0.08 for immediate memory; r = −.38, P = .05, d = 0.82 for visuospatial/constructional; r = .03, P = .89, d = 0.06 for language; r = −.09, P = .67, d = 0.18 for attention; r = .13, P = .51, d = 0.26 for delayed memory; and r = −.05, P = .80, d = 0.10 for total scale score) or RBANS indexes and depression levels (r = −.05, P = .82, d = 0.10 for immediate memory, r = −.30, P = .13, d = 0.63 for visuospatial/constructional, r = −.25, P = .20, d = 0.52 for language, r = −.12, P = .55, d = 0.24 for attention, r = .12, P = .54, d = 0.24 for delayed memory, and r = −.12, P = .57, d = 0.24 for total scale score). However, small sample size and restricted range of scores (on the GDS) may have reduced the power to detect subtle associations.
Discussion
The current study revealed that performance on a standard measure of cognitive assessment, the RBANS, 18 was related to in vivo cerebral amyloid deposition or accumulation. Nondemented participants underwent [18F]flutemetamol amyloid-PET imaging and were classified as being [18F]flutemetamol positive (Flute+) or negative (Flute−) according to the established criteria. 26 The participants were also administered a series of cognitive tasks, including the RBANS, along with measures of premorbid intelligence, mood, and subjective cognitive experience. Performance on these measures was analyzed based on [18F]flutemetamol group status, and supplementary analyses were conducted to assess for comparable effects between participants diagnosed with MCI and normal cognition.
The results of the current study suggest that participants possessing an abnormally elevated level of amyloid deposition using [18F]flutemetamol imaging (Flute+) demonstrated worse performance on RBANS indexes of immediate memory, language, delayed memory, and total scale score than participants with normal levels of amyloid accumulation (Flute−). These findings are consistent with previous research indicating that greater [18F]flutemetamol uptake was correlated with worse performance on RBANS indexes of visuospatial/constructional, attention, and delayed memory after controlling for premorbid intellect. 17 Our results also support the findings of previous studies using either [11C]PiB or [18F]florbetapir imaging agent, showing that greater amyloid biomarker imaging is associated with worse memory performance 33 –38 and also worse nonmemory cognitive performances (processing speed and attention). 33,35,39
Beyond this statistical significance, the magnitude of the difference in RBANS indexes of immediate memory and delayed memory between [18F]flutemetamol groups appears to be clinically meaningful. As seen in Table 2 and Figure 1, across the total sample, Flute+ participants performed approximately 25 SS points (1.7 SD) below their Flute− counterparts on immediate memory, and approximately 35 SS points (2.3 SD) below on delayed memory. Clinically, although the Flute− participants performed at the upper limit of the average range for their normative peer group on both indexes, the Flute+ group performed at the lower limit of the low average and borderline impaired ranges 40 for indexes of immediate and delayed memory, respectively. As the [18F]flutemetamol status groups were made up of both normal cognition and MCI participants, these results do not appear to be explained solely by diagnostic status. Additional supplementary analyses indicated that even among participants possessing a diagnosis of MCI, Flute+ participants performed significantly worse than Flute− participants on RBANS indexes of immediate memory, delayed memory, and total scale score. Specifically, the discrepancies in immediate memory and delayed memory indexes between Flute+ and Flute− groups for participants with MCI were comparable to or larger than the total sample, at 27 SS points (1.8 SD) and 43 SS points (2.8 SD), respectively. These results suggest that amyloid positivity may be a marker of more pronounced memory loss in older adults, particularly for those individuals with MCI-amnestic subtype. Our findings are consistent with AD neuroimaging initiative data showing worse memory performance among patients with MCI with greater amyloid burden relative to participants with MCI with minimal burden using [18F]florbetapir. 41 This is not necessarily surprising, given the typical clinical manifestation of AD or MCI due to AD, which begins with early and predominant anterograde episodic memory deficits associated with amyloid plaque accumulation and degeneration of the entorhinal cortex and hippocampus/medial temporal lobe. 42 –46 Because amyloid plaque burden is hypothesized to accumulate early in the disease process and then plateau, 1,47 our results suggest that increased amyloid deposition identified using [18F]flutemetamol-PET may contribute to substantial changes in cognition even early in the disease course. This sensitivity of detection raises the specter of [18F]flutemetamol-PET as a prognostic tool.
In our current study, 55% of participants classified as having MCI were Flute+ compared to 33% of cognitively normal participants. Our small sample size, especially for participants with normal cognition, likely limited our ability to find statistical significance in this analysis. Nevertheless, our respective proportions of participants possessing above-threshold amyloid accumulation are mostly consistent with rates found in the literature. For example, in a recent meta-analysis of 55 studies assessing the prevalence of amyloid positivity among individuals without dementia, Jansen and colleagues 48 found that for 75-year-olds (the mean age of our sample), the rate of amyloid positivity in individuals with normal cognition was 27.6% (95% confidence interval [CI]: 23.4-32.3) and the rate of amyloid positivity in individuals with MCI was 54.6% (95% CI: 50.2-59.0), which closely approximates our findings. The meta-analysis additionally identified that among all nondemented individuals, higher levels of education, but not differences in gender, were associated with amyloid positivity, 48 which also corresponds with our current results. This finding between higher education and greater amyloid positivity may at first glance seem counterintuitive, with the cognitive reserve hypothesis that individuals with higher education levels are less susceptible to dementia, 49 –51 though the association between these variables is not necessarily causal and highlights the important difference between the development of AD pathology and the onset of dementia. As indicated by our prevalence of amyloid positivity in 33% of individuals with normal cognition, the presence of amyloid pathology alone does not constitute dementia; as such, the onset of dementia due to AD occurs only after an individual has surpassed the threshold of brain pathology and lost efficiency of cognitive networks for which their particular level of cognitive reserve can compensate. 52 As has been suggested elsewhere, 53 there is no reasonable biological explanation for how higher levels of education could directly lead to an increased accumulation of amyloid, but rather our findings likely reflect that higher education and reserve in our sample may have raised the threshold of AD pathology needed for the development of dementia, permitting more participants to remain nondemented, while still possessing amyloid positivity.
The absence of an association between amyloid positivity and premorbid intellectual functioning contrasts with Duff et al’s 17 earlier study identifying that premorbid intellect possessed a mediational effect on the relationship between cognition and amyloid burden. As the current sample exhibited delayed memory and total cognition abilities approximately 1.0 SD and 0.5 SD lower than the participants in Duff et al’s previous study, 17 respectively, the differences in severity of impairment may account for these discrepant findings. In essence, our study may have contained more individuals whose memory difficulties were beyond the threshold of receiving a benefit from cognitive reserve, 52 thus reducing the mediational effect observed in Duff et al’s earlier study. Additionally, differences in statistical procedures used (regression vs MANCOVA, continuous vs dichotomous variables) may have also contributed to this discrepancy. This lack of association was particularly interesting, given that another proxy of cognitive reserve, education, was associated with amyloid burden. Such variability may be explained by differences in the nature of these proxy variables. Educational history is not influenced by cognitive declines in later life, but premorbid intellectual functioning based on sight-word reading skills is not entirely resilient to neurological insult, cognitive decline, or dementia. 54 –56 Consequently, as our participants’ memory skills declined, their sight-word reading skills may have also been impacted, influencing the potential relationship with amyloid accumulation. Taken together, our equivocal results suggest that more focused research on cognitive reserve in AD and the incremental contributions of each proxy variable will be beneficial in the future. For example, longitudinal evaluations of subclinical participants with varying levels of education and environmental enrichment/stimulation could be beneficial, as could obtaining archival school records or standardized testing results be used as a proxy for premorbid intelligence in future studies.
Additionally, the level of amyloid plaque burden on [18F]flutemetamol-PET was not related to levels of depression or subjective report of cognitive complaints. These results are consistent with a systematic review, 57 identifying a limited relationship between amyloid deposition and depression. Additional studies using [18F]florbetapir 58 or a collection of amyloid-imaging agents ([11C]PiB, [18F]florbetapir, [18F]flutemetamol) 59 have similarly failed to display an association between amyloid burden and levels of depression. Our results are also consistent with most literature suggesting a weak relationship between in vivo amyloid burden and subjective cognitive complaints. Although higher amyloid burden has been associated with worse subjective cognitive complaints in some studies, 16,60,61 other research has observed no relationship or inconsistent relationships when using individual subjective complaints questionnaires. 62,63 Overall, our findings are consistent with the literature suggesting a lack of clear evidence that depression levels or subjective cognitive complaints are early markers for increased amyloid burden.
The current study is not without limitations. First, our sample size may have limited our ability to find statistical significance for some analyses. Although future research on this topic using larger samples is encouraged, the cost of [18F]flutemetamol amyloid imaging may be a potential barrier in many smaller-scale studies. Second, the homogeneity of our sample related to education (mostly highly educated), ethnicity (Caucasian), and health status (able to receive a [18F]flutemetamol-PET scan) may have limited generalizability to the larger population possessing a wider range of demographics. Third, our sample reflected a restricted range of depression values that may have reduced the ability to observe a significant relationship between amyloid burden and depression, consequently a more thorough examination of [18F]flutemetamol binding and depression should be undertaken with participants possessing a wider range of depression scores before any definitive conclusions can be made about this relationship. Additionally, 4 participants in our study were prescribed cognitive-enhancing medications at the time of enrollment, which may have influenced their results on the cognitive tests. However, although these medications (donepezil, memantine) have shown modest relief for some patients with AD, 64,65 neither have prevented the progression from MCI to AD, 66 nor have been found to be disease modifying or impact amyloid burden. 67 Further, magnetic resonance angiogram or MRI was not available for the current study, therefore it is unknown what impact vascular burden would have had on the current results. This should be considered in future studies, given recent evidence of periventricular hyperintensities being associated with cerebral amyloid. 68
Finally, the current study utilized the RBANS cognitive assessment battery. Although the RBANS is being used increasingly in clinical drug trial studies as either a screening measure or an outcome measure, and thus possesses relevance from both clinical and research perspectives, it is not without its limitations. Specifically, the RBANS exhibits reduced sensitivity in identifying cognitive decline among participants with milder cognitive impairments 69 and also fails to assess cognitive domains related to executive functioning, which is known to be common in older adults with cognitive decline or neurodegenerative disease. Consequently, the current study cannot speak to the relationship between [18F]flutemetamol uptake and executive functioning, and future studies to examine this relationship using measures more sensitive to both milder cognitive impairments and executive dysfunction should be considered.
Despite these limitations, the current study possesses a number of contributions to the field. We have shown that nondemented community-dwelling older adults with abnormally increased cerebral amyloid burden on [18F]flutemetamol-PET performed worse on cognitive tasks of language, immediate and delayed memory, and total cognition on the RBANS relative to their negative amyloid status peers, regardless of their premorbid intellectual skills, subjective cognitive complaints, or endorsements of depression. The magnitude of these cognitive performance differences between our [18F]flutemetamol groups in both our primary and supplementary analyses also indicate that increased amyloid deposition identified by [18F]flutemetamol-PET may contribute to clinically meaningful changes in cognition even early in the disease course. Altogether, our findings suggest that earlier and more accurate predictions of cognitive decline in later life may be possible.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an anonymous foundation, a grant from GE Healthcare #GE067ISS, a grant from the National Institutes of Aging # 5R01AG045163, the Center for Quantitative Cancer Imaging at the Huntsman Cancer Institute, and the University of Utah Center for Alzheimer’s Care, Imaging and Research.