
Abstract
Introduction:
Falls are one of the major problems among the elderly population. It has been established that people with dementia fall down more often. It is believed that this is a consequence of risky decision making by people with dementia resulting from cognitive deterioration. The aim of the present study was to evaluate the relationship between cognitive status and postural stability while standing.
Methods:
A total of 47 people, aged 71.6 years on average (±7.2), were divided based on results of the Mini Mental State Examination (MMSE) into a dementia group (MMSE ≤ 23) and a control group (MMSE > 23). Postural stability was tested using a force plate (with eyes open, with eyes closed, and with visual biofeedback). The parameters of movement of the center of pressure were analyzed.
Results:
Both in test with eyes open and eyes closed, significant difference was shown between the dementia group and the control groups. In visual feedback test, the dementia group showed 32% poorer performance than the controls.
Conclusion:
The falls experienced in dementia group may be caused by a disturbed balance control process of the central nervous system.
Introduction
The aging populations of developed countries and the developing world concomitantly bring some serious economic and social consequences, and thus constitute one of the greatest challenges of modern civilization. According to the Government of the United States, the total percentage of the population of the United States aged older than 65 is at 13% at the moment and by 2060 it is expected to increase to approximately 22%. 1 According to a report by the European Commission, the population of the European Union (EU) aged older than of 65 will increase from the current amount of 18% to about one-third of the population in 2060. An analogous situation exists in Poland, which is the fastest aging country in the EU. Currently, the percentage of people in retirement age is about 14%, but it has been estimated that within 50 years this figure will more than double. 2
There is a serious problem with cognitive impairments (CI) of different etiologies among the elderly population. Diseases such as Alzheimer’s and other types of dementia interfere with one’s ability to absorb information from the surrounding environment, process it, and use it to control one’s own behavior. Studies have shown that the percentage of people with dementia doubles every 5 years; in the population older than 65 years of age, it is 1%, which increases up to 45% of the population aged 90 to 95 years. 3 However, in specific populations, such as nursing homes or retirement villages, the prevalence of dementia ranges from 60% to 80%. 4
Falls, as well as their consequences in the form of orthopedic injuries, immobility, and disability, are another serious problem among elderly people. Among the psychological consequences, we talk about fear of another fall, a sense of helplessness, low mood, and reduced quality of life, also in terms of social functioning. 5,6 Therefore, preventing falls (and their consequences) is critical for a calm, peaceful aging process. 7,8 The effectiveness of prevention programs depends on accurate identification of risk factors in the particular population.
Studies have shown that there is an interaction between falls and the presence of CI in elderly people. The risk of falling among patients with CI is 2 times higher compared to those of similar age but cognitively intact. 9,10 It is also worth noting that the repercussions of falls in people with CI are much more serious than in their healthy peers. These people are 5 times more likely to end up in outpatient care units after a fall. 11 At the same time, the fall prevention programs for seniors with CI often turn out to be weak or ineffective. 12 -14
Until recently, it was believed that the problem of falls in this group of patients was solely attributable to the so-called “risky decision making” associated with the presence of CI. It has been shown that the decisions made by people with Alzheimer’s disease were more risky than choices made by healthy people. 15 However, in light of the latest knowledge, it seems that the problem also concerns the very process of balance control. People with CI exhibit a tendency of increased sway damping of the body’s center of gravity. It appears that damping delays the outset of movements aimed at correcting balance reflexes, which are necessary to counteract the falls. 16 Moreover, studies show a 5-fold increase in the likelihood of a fall in cases where the parameter of damping increases by a mere 10%. 17
Hauer et al 18 demonstrated that the necessity of performing concurrent cognitive tasks during a stabilographic test revealed a real problem in terms of maintenance of postural stability among people with CI, which generally cannot be detected during simple quiet stance tests. Nevertheless, knowledge of balance disorders in the elderly individuals with cognitive defects is still insufficient. Perhaps a better understanding of this problem will allow for the development of more effective programs to prevent falls in this group of patients.
Study Aim and Research Questions
The aim of this study was to evaluate the relationship between cognitive status and postural stability during standing.
Research questions: Does cognitive status correlate with postural stability as evidenced by force plate test results? Are there any differences in ways of maintaining balance during simple quiet stance tests on a force plate, between a group of people with dementia and a control group? Does cognitive status correlate with the performance on a force plate using visual feedback?
Methods
Participants
The tests on postural stability were conducted on 47 randomly selected patients (31 women and 16 men) who came to the mental health clinic for cognitive screening tests. Mean age of the participants was 71.6 years (±7.2), mean body height was 162 cm (±8.5), and mean body weight was 68.1 kg (±12.8). To assess cognitive status, a mini-Mental State Examination (MMSE) was used where a score between 30 and 27 indicated no CI, 26 and 24 indicated CI without dementia, 23 and 19 indicated mild dementia, 18 and 11 indicated moderate dementia, and 10 and 0 indicated severe dementia. 19 This was a screening study, where detailed diagnosis regarding the etiology of CI was not yet determined. Thus, each MMSE score should be treated as a general reflection of cognitive status and not as a medical diagnosis.
Participants were divided into 2 groups. The inclusion criterion for the test group (dementia group) was represented by a MMSE score equal to 23 points and below and, for the control group, participants with a MMSE score over 23 points were included. The criterion for exclusion from the study included the presence of Parkinson’s disease; major orthopedic, neurological, and rheumatologic ailments; and other diseases that may adversely affect posture and balance. Additionally, persons who did not understand the instructions in taking the visual feedback test were excluded from the study.
Studies were approved by the Scientific Research Ethics Committee at the University of Physical Education in Wroclaw. All participants gave their written consent to perform both the cognitive screening tests and the stabilographic tests.
Measurement Procedure
In order to perform the postural stability test, a force plate was used to register the center of pressure (CoP) in the sagittal plane (anterior-posterior [A/P]) and the frontal plane (medial-lateral [M/L]), during three 32-second trials of quiet stance on hard surface. The order of testing was as follows: quiet stance with eyes open, quiet stance with eyes closed, and a task with the use of visual feedback.
During a test trial examining postural stability using visual feedback, at a distance of 2 m from the force plate, a point appeared on the monitor screen at eye level, reflecting the participant’s CoP movement in real time during the test. Furthermore, in the middle of the screen, there was a square that had a 1 cm side. The respondent’s task was to try to keep the point on the screen, reflecting the CoP movement, for as long as possible within the designated field. The task was understood by each participant. In order to familiarize the respondent with the test, the main measurement was preceded by an additional test trial measurement, which was registered but not used in subsequent analysis.
The following parameters of the CoP movement were analyzed: variability (mm), total CoP path length (mm), mean velocity (mm/s), mean radius (mm), CoP sway (mm), and sway area (mm2). In the visual feedback test, a parameter that proved the quality of this task was the “performance” parameter (percentage of time in which the CoP was within the designated field). The sampling rate was 20 Hz.
Statistical calculations were performed using Statistica 10. The results were presented using descriptive statistics—the mean and standard deviation. Given a normal distribution of all parameters, the statistical significance of results of compared groups was examined using Student’s t-test for independent groups and set at a level of α < .05. The correlation of the results of MMSE scale with respect to the balance parameters was tested using Pearson’s linear correlation.
Results
Demographic ResultNineteen patients were qualified for the dementia group, with a mean age of 72.8 ± 7.1 years and a mean MMSE score of 16.4 (±5.3), while the control group included 28 people with a mean age of 70.7 ± 7.2 years and a mean MMSE score of 27.3 ± 1.6. Number of men and women in both the groups was comparable (P = .77). The 2 groups did not differ significantly with respect to age (P = .33; Table 1).
Participant Characteristic, Mean ± SD.
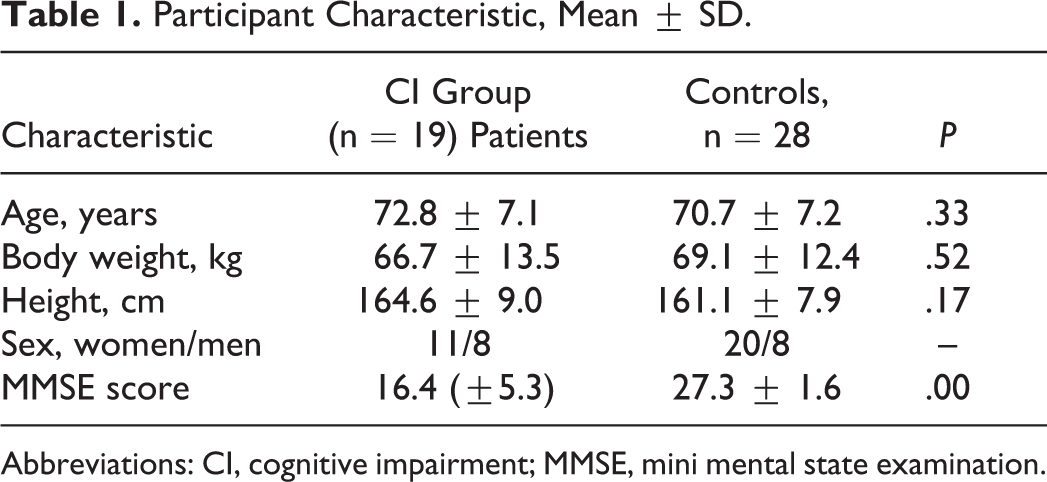
Abbreviations: CI, cognitive impairment; MMSE, mini mental state examination.
Eyes Open Test
In the test performed during a quiet stance, a significant relationship was observed between the MMSE score and the postural stability parameters in almost all studied characteristics. A strong, negative correlation was shown between the MMSE score and the mean CoP sway radius (r = −.49, P = .0004). A moderate relationship was also registered for the sway area (r = −.30, P = .04), total sway path length (r = −.31, P = .03), and mean velocity (r = −.30, P = .03).
Analyzing the values obtained for different planes, it was established that in the frontal plane, the MMSE score is negatively correlated with the sway path length M/L (r = −.30, P = .03) and with the mean sway velocity M/L (r = −.29, P = .04), whereas in the sagittal plane the MMSE score is only correlated with the mean velocity (r = −.30, P = .03). The parameter that least correlates with the MMSE score is the sway path length in the anterior–posterior plane (r = −.28, P = .053). The above-mentioned findings confirm the relationship of cognitive status with the CoP movement during a quiet stance with eyes open.
A comparison of people with dementia versus controls showed some important results. It was established that these groups differed significantly in almost all parameters that were studied. Most of the stabilographic parameters in people from the control group (Table 2) were more than one-third lower, indicating worse postural stability in people with dementia even during a quiet stance on hard surface with eyes open.
Comparison of Stabilographic Parameters (CI Group vs Control Group) During a Quiet Stance With Eyes Open.
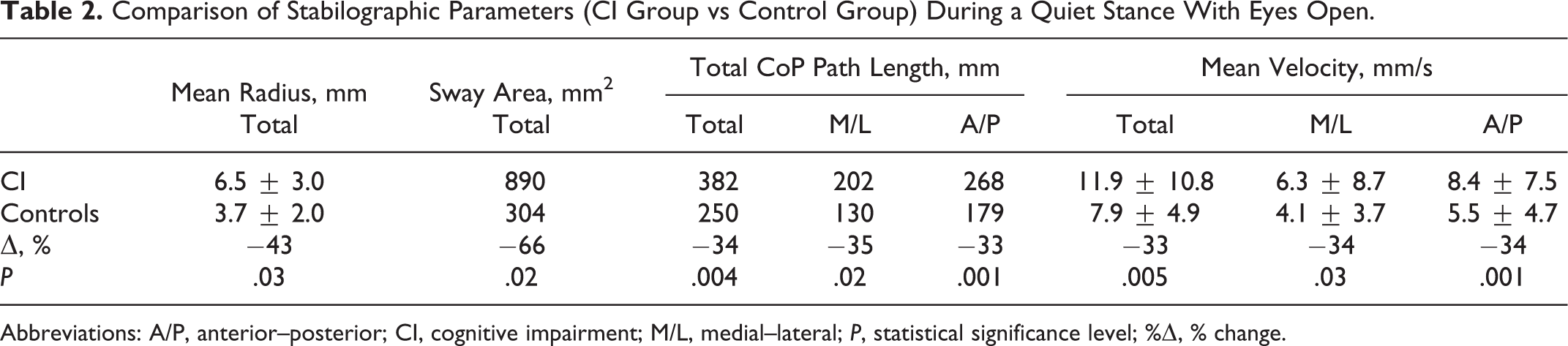
Abbreviations: A/P, anterior–posterior; CI, cognitive impairment; M/L, medial–lateral; P, statistical significance level; %Δ, % change.
Eyes Closed Test
Hampering the test by closing the eyes revealed a moderate, negative correlation of the MMSE score with balance parameters such as the total CoP path length (r = −.27, P = .04) and the CoP mean velocity (r = −.27, P = .04). A significant relationship was also demonstrated in the case of frontal plane CoP parameters. The length of the CoP movement in this plane clearly showed a negative correlation with the MMSE scale results (r = −.40, P = .005). A similar relationship was shown in the case of CoP mean velocity for the same plane (r = −.39, P = .007). Presented results confirm a relationship of cognitive status with CoP movement also in tests with eyes closed.
During a comparison of mean values of the parameters of postural stability in the dementia group and control group, significant differences were found in most of the studied characteristics. In the control group, the values of balance parameters were clearly lower. In this group, the path length covered by the CoP was more than 30% lower. Mean velocity, mean radius, and CoP sway area were significantly different as well. The study of postural stability conducted while standing with eyes closed indicated poorer postural stability in persons with dementia (Table 3).
Comparison of Stabilographic Parameters (CI Group vs Control Group) During a Quiet Stance With Eyes Closed.
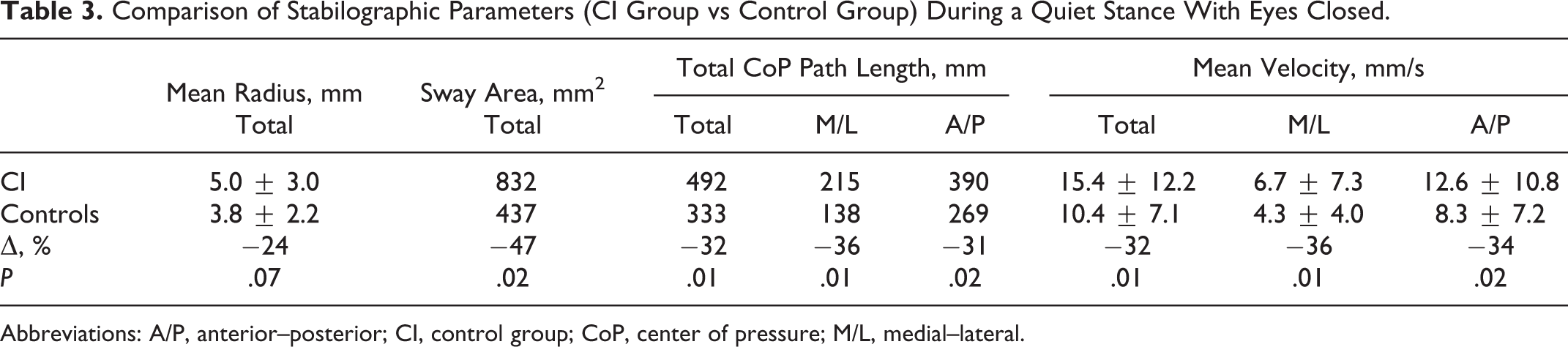
Abbreviations: A/P, anterior–posterior; CI, control group; CoP, center of pressure; M/L, medial–lateral.
Visual Feedback Test
A main parameter analyzed in this test was the performance parameter (percentage of time in which the CoP was within the designated field). The higher the score, the better the task was performed. In this test, a clear positive correlation was found between the MMSE result and the performance parameter (r = .43, P = .002). This means that the lower the MMSE score, the shorter the time the participant maintained their CoP within the designated field.
Comparing mean scores of balance parameters obtained in this test, we can observe a significant difference between dementia group and control group, namely, in terms of performance. Individuals from the reference group had managed to keep the point representing CoP within the designated field for a time longer by about 32%. In addition, significant differences were demonstrated between the mean sway area and the amount of CoP sway during the test. In dementia group, these parameters were significantly higher in comparison to the control group (Table 4).
Comparison of Stabilographic Parameters (CI Group vs Control Group) in the Test With Visual Feedback.
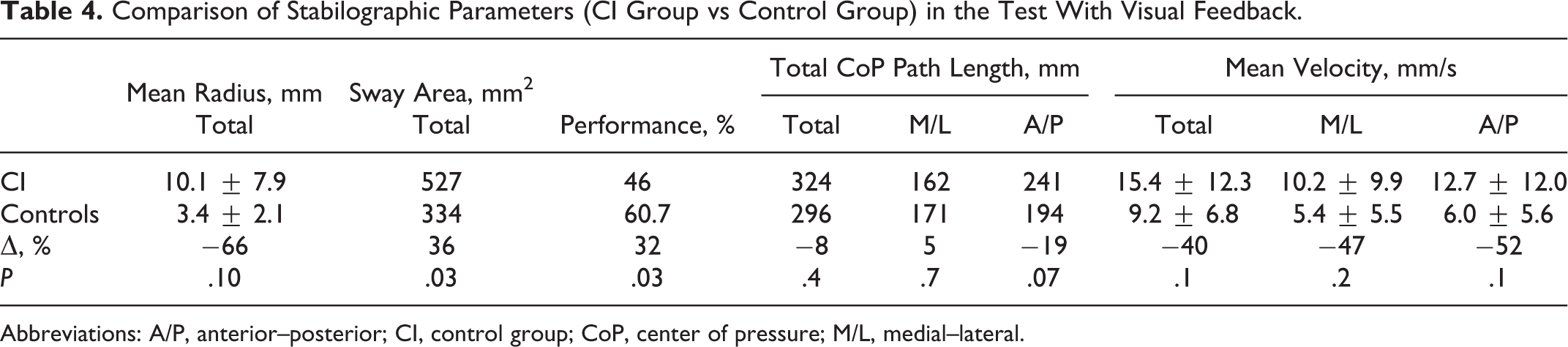
Abbreviations: A/P, anterior–posterior; CI, control group; CoP, center of pressure; M/L, medial–lateral.
Discussion
The aim of the study was to answer the question whether the presence of dementia is associated with postural stability in older people. The results showed that such a relationship does exist, since in both the quiet stance test with eyes open and in the eyes closed test, persons from the dementia group exhibited higher CoP sway when compared to the reference group in both the anterior–posterior and medial–lateral planes, which means poorer postural stability. A negative impact of CI on the process of maintaining balance was also confirmed by other authors with respect to people with mild CI and patients with Alzheimer’s disease. 20,21 It is therefore surprising that the results obtained in our study are contrary to reports by Hauer et al, 18 where no differences were shown between groups of patients with CI and those without CI in simple quiet stance tests.
A detailed comparison of the 2 research projects to some extent explains this difference. In these experiments, patients in the control group obtained a very similar mean MMSE score (approximately 27 points), but in the case of Hauer et al’s 18 research, people with CI obtained a mean MMSE score of 19 points, which indicates a mild degree of dementia; in our studies, it was 16 points, which indicates moderate dementia. Thus, it appears that the results of both experiments are not mutually exclusive but rather complementary. In their research, Hauer et al, 18 when comparing healthy individuals to patients with mild cognitive defects (mean MMSE score = 19), stated that simple quiet stance tests with eyes open and closed did not show differences in terms of keeping balance between the groups. It is not until you hamper the test in the form of an additional cognitive task that the problems of patients with dementia in keeping postural stability are revealed. In our study, where the dementia group exhibited greater deterioration of cognitive functions (mean MMSE score of 16 points), the differences between groups were visible even in the simple quiet stance tests on a force plate with eyes both open and closed.
The above-mentioned findings are additionally confirmed by the test that uses visual feedback, in which particpants received assistance in the form of a visual reflection on the screen showing the CoP movements of their own body. They were to use this information to stabilize posture and reduce CoP sway. The described task was performed far better by persons in the control group. In their case, the percentage of CoP being in the designated field was significantly higher when compared to dementia group (P = .03). At the same time, this study demonstrated that the biggest difference was in the length of mean CoP sway radius between dementia group and control group (66%) among all the samples. It turned out that the visual reflection of the CoP movements was helpful for patients from the control group, who in this test effectively stabilized their posture, and thus performed the task better. In the dementia group, on the other hand, this additional visual information had the opposite effect. A significant increase in the mean sway radius in relation to tests with eyes open and closed was observed. The resulting effect is therefore paradoxical. Visual feedback was supposed to help in completing the task; however, effectively, it worsened the postural stability of patients with dementia. This result may suggest that the cause of the problem with falls among elderly people with dementia lies in the disturbances of the body’s balance control in the central nervous system and is not just due to the so-called risky decision making arising from the presence of dementia as previously believed. These observations are confirmed by our team’s previous publications as well as by Hauer et al’s findings. 16,18
In recent months, very interesting research results were published together with conclusions that were complementary to our own observations. The study involved 139 cognitively intact and 56 cognitively deteriorated persons. This project did not apply additional cognitive tasks, or the visual feedback test, but hampered the process of maintaining balance in respect to specific positioning of each participant’s feet. In the first test, patients were asked to stand with their feet as closely together as possible. In the second test, they were asked to stand with the medial side of the heel of one foot touching the big toe of the other foot. In the third test, patients were asked to stand with both feet in line, while the heel of one foot touched the toes of the other foot. It was found that low cognitive status is associated with lower ability to maintain standing balance in more demanding standing conditions. 22 This very same project did not confirm a relationship between the CoP movement and the cognitive status in simple quiet stance tests. At the same time it should be clearly stressed that, as in the case of the experiment by Hauer et al, 18 patients with CI exhibited rather mild CI (mean MMSE score of 22 points).
Summing up the results of our research, it can be concluded that the presence of dementia negatively affects the process of maintaining balance in the elderly indiviuals. In turn, the summary of our research, together with results of other authors, can help in the observation of a certain principle—in the case of significant cognitive defects (moderate dementia), even simple quiet stance tests on the force plate allow one to identify problems with balance maintenance. On the other hand, in patients with minor cognitive deficits, it is not until the introduction of additional obstacles in the form of cognitive tasks, unstable surfaces, or more demanding standing conditions that the differences in ways of maintaining balance between people with dementia and those without moderate CI do show up. Further research in this area is still needed to better understand the interrelationships between CI and balance. It is only through better understanding of these mechanisms that programs aimed at preventing falls in patients with CI will be more effective.
Obviously we need to remember that falls usually take place during complex motor activities (turns, changing body position from sitting to standing or vice versa, and most often during walk). This is when complex interactions take place between many varieties of factors. In healthy elderly persons, gait disturbances are caused, among other things, by deterioration of the functioning of sensory organs that ensure postural stability (vision, hearing, and superficial and deep sense of touch). In addition, muscle mass content in the body decreases and the amount of fat tissue increases, which interferes with posture and hinders rapid response to unexpected situations of everyday life. This overlaps with degenerative changes in the lower limb joints, which is a common ailment of older people. Effectively, the step becomes shorter, double limb support phase takes longer, and the center of gravity moves forward, as a result of which body figure tends to lean forward. 23 Among those with CI, in addition to the aforementioned problems, there is also an improper, stiffening of the body figure and longer duration of response which, in the case of sudden loss of balance, increases the risk of falling. 16,24
Unfortunately, in many research projects that evaluated the effectiveness of fall prevention programs, the presence of CI was a factor excluding the patient from participating in the experiment. Among the 111 research projects conducted from 1992 to 2012, only 12 studies involved cognitively impaired older adults. 25 This fact shows that the professionals involved in the analysis of gait and postural balance are reluctant to take up studies involving people with CI, and at the same time it is in this group of patients that we observe the greatest risk of falls. Therefore, there is a need for further research in this area and for the creation of interdisciplinary research teams, in which kinesiologists, biomechanical specialist, and physiotherapists, as well as psychologists and psychiatrists who deal with cognitive problems in the elderly, could all work together
The limitations of the research project have been complemented. The main problem of this project is a small sample size of the study group, which limits the possibility of generalizing the results. This also gives rise to a small number of respondents within the actual groups of men and women, which makes a reliable analysis of postural stability in patients with dementia by gender impossible. Therefore, further research is needed so that there are reports that healthy female volunteers exhibit lower postural stability than those of men.
Footnotes
This article was accepted under the editorship of the former Editor-in-Chief, Carol F. Lippa.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.