
Abstract
Inflammation may be associated with Alzheimer’s disease (AD). This meta-analysis aimed to compare the level of C-reactive protein (CRP) in patients having AD to healthy controls. A total of 10 cross-sectional studies (n = 2093) were identified from PubMed and EMBASE after systematic searching and evaluation. The combined standardized mean difference (SMD) of CRP level between the disease and control group was analyzed. In the meta-analysis, there was no significant difference in serum between the CRP level of patients with AD and that of healthy controls (SMD: −0.400, 95% confidence interval [CI]: −0.827 to 0.027, P = .066). However, when we stratified the studies by Mini-Mental State Examination (MMSE) scores, the level of CRP in the mild and moderate dementia subgroup (MMSE ≥ 10) was significantly lower than that in the control group (SMD: −0.582, 95% CI: −0.957 to −0.208, P = .002). Therefore, the diagnostic value of CRP for mild and moderate AD may be useful in clinical practice.
Introduction
Alzheimer’s disease (AD), the most prevalent dementia, is a progressive neurodegenerative disorder in the elderly population. The major pathological characteristics of AD includes senile plaques (SPs) formed by deposition of β-amyloid protein (Aβ) in the brain and neurofibrillary tangles (NFTs) formed by accumulation of abnormal tau protein. 1 In the past decades, a pile of evidence suggested the association between inflammation and AD. 2,3 Upregulation of inflammatory genes together with Aβ deposition and microglial activation was found even in the early stages of AD. 4 A neuroprotective effect of nonsteroidal anti-inflammatory drugs was also observed in some patients with AD. 5,6 In addition, inflammatory biomarkers may be associated with dementia risk. 7 Circulating level of several inflammatory mediators, including tumor necrosis factor-α, interleukin (IL) 6, and IL-1b, was found increased in patients with AD. 8
C-reactive protein (CRP), a well-known inflammatory biomarker, is a trace serum protein that markedly increases after acute injury, infection, or other inflammatory stimuli. Although usually CRP is synthesized in liver during an inflammatory reaction, CRP could also be produced by other cells, such as neurons. 9 Pathological studies have shown CRP to be associated with both SPs and NFTs in AD brain tissue. 10,11 Clinical studies have linked CRP levels to AD risk. Longitudinally, midlife elevations in CRP may increase the risk for late-life AD on a 25-year follow-up. 12 A recent meta-analysis that combined 7 retrospective or prospective studies (N = 5717) found an increased level of CRP before disease onset associated with an increased risk of AD (hazard ratio: 1.21; 95% confidence interval [CI]: 1.03-1.42). 13 For patients after disease onset, some cross-sectional studies revealed elevated CRP concentrations in the serum, cerebrospinal fluid, and brain tissue of patients with AD. 9,14,15 However, other studies showed inconsistent results. They found serum CRP levels appeared to be lower among cases with AD than age-matched normal controls. 16,17 This meta-analysis seeks to analyze the difference of circulating CRP levels in AD and controls and therefore provide the supporting data for the diagnostic value of CRP in AD.
Methods
We performed this meta-analysis following the guidelines of the Meta-analysis of Observational Studies in Epidemiology group (MOOSE). 18
Search Strategy and Quality Assessment
To identify the relevant studies, we searched through the online PubMed and EMBASE database from January 1966 to February 2015. Two key words were set during that process, namely “C-reactive protein” and “Alzheimer’s disease.” All articles included in the meta-analysis were hand searched after 2 stages. First, the researchers reviewed the title and abstract, followed by the full text. Studies were regarded eligible when they met the following criteria: (1) they identified the associations between AD and CRP; (2) they were designed as case controlled, which means that they compared CRP levels in both patients with AD and healthy controls; and (3) they were cross-sectional studies. Articles were excluded based on the following criteria: (1) non-English papers, (2) review articles or letters, and (3) absence of key information, such as sample size, Mini-Mental State Examination (MMSE) score, and CRP levels, including mean value and standard deviation. When duplicate studies were retrieved, the studies involving more patients (usually the latest) were included in our systematic review. Thus, the overlapping between cohorts and overestimation of the overall standardized mean difference (SMD) could be avoided. A flow diagram of the study selection process is presented in Figure 1.
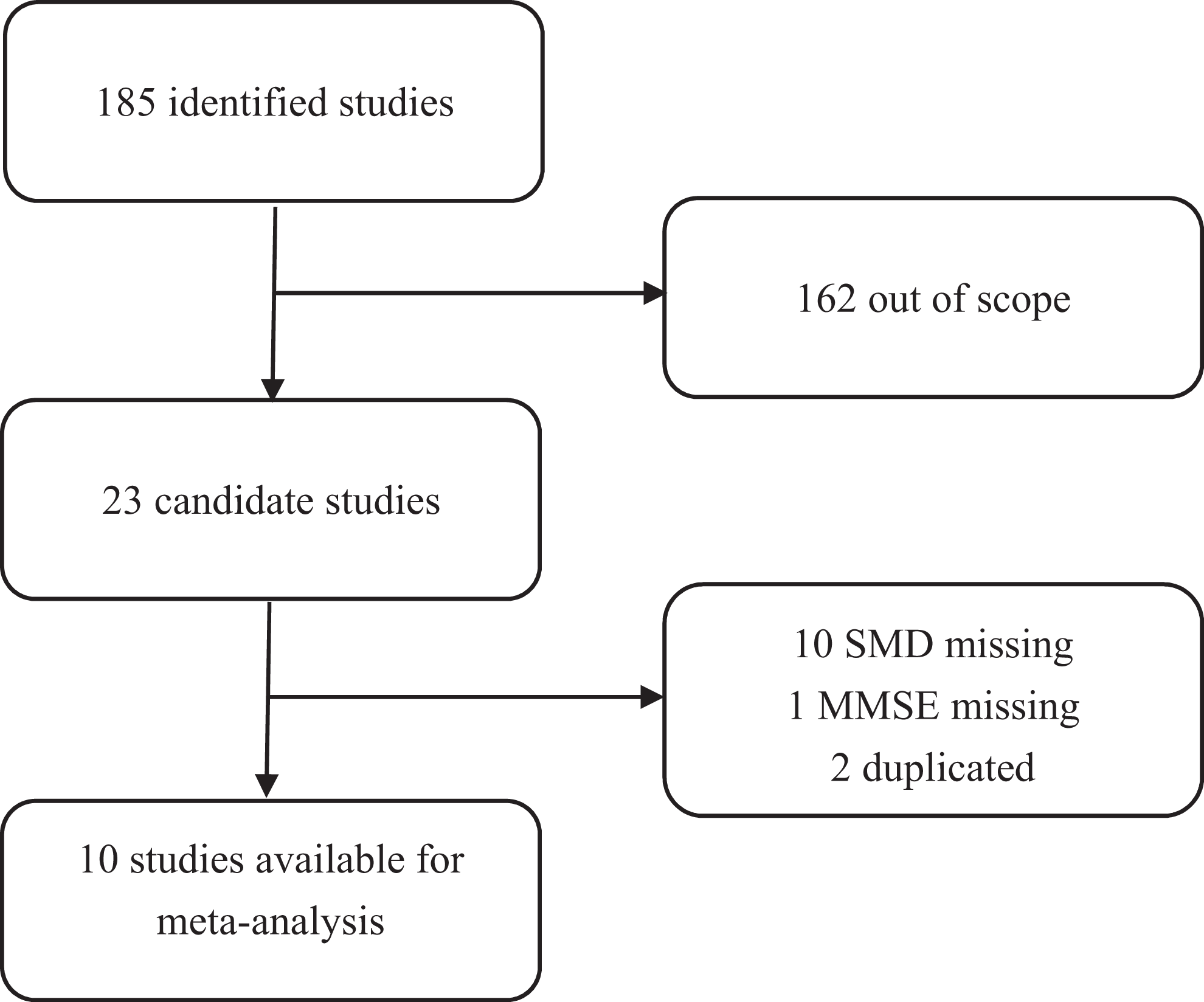
Flow diagram of the study selection process.
The studies were assessed for methodological quality independently according to the QUADAS (Quality Assessment of Diagnostic Accuracy Studies) criteria by 2 reviewers (C. G. and D. W.). 19 We used the SMD value to compare the difference between patients with AD and healthy controls, and there was no reference standard. Thus, 6 items concerned with reference standard were not included. Therefore, the remaining 8 items were used to assess the study quality, including (1) representative spectrum, (2) clearly described study criteria, (3) disease progression bias avoided, (4) partial verification bias avoided, (5) detailed description of index test, (6) availability of clinical data, (7) uninterpretable results reported, and (8) withdrawals explained. Each item was answered with “yes,” “no,” or “unclear” response. An answer of “no” or “unclear” indicated that the risk of bias may be high, and an answer of “yes” indicated that the risk of bias is low. An additional reviewer (Y. Z.) assessed all discrepancies, and the majority of opinions was used to resolve disagreements between the reviewers. The results of the methodological assessment for the included studies are summarized in Figure 2.
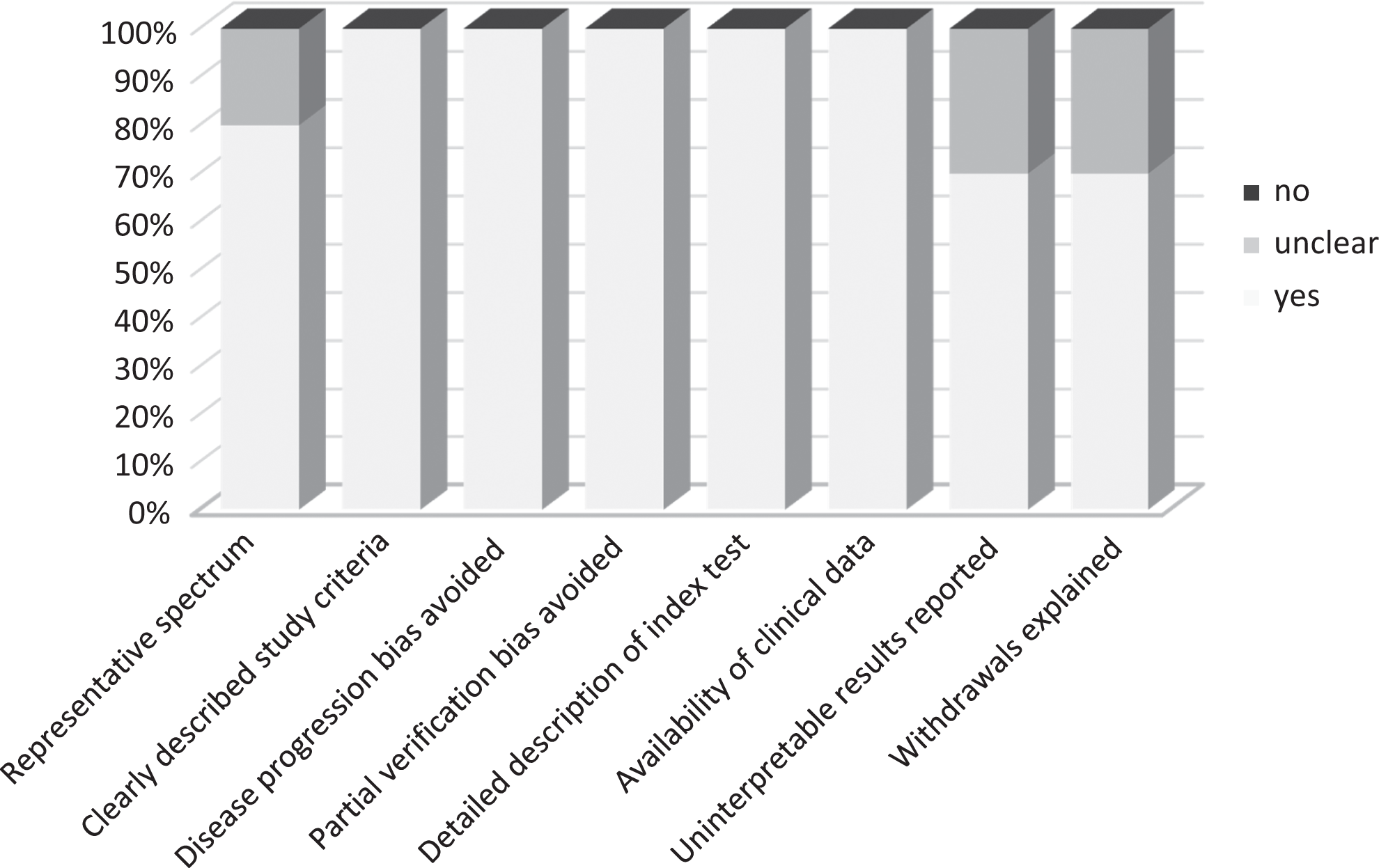
Proportion of Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool criteria fulfilled for the included studies.
Data Extraction and Statistical Analysis
The extracted data elements of this analysis included (1) publication details: first author’s last name, publication year, and origin of the studied population; (2) study design; (3) characteristics of the studied population: sample size, age, gender, and disease; (4) criteria of AD diagnosis and MMSE; (5) criteria of healthy control; and (6) method to detect CRP. The difference in CRP levels between patients with AD and controls was converted into SMD. According to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins JPT, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane-handbook.org), the formula for SMD is as follows:

A negative SMD less than 0 means lower CRP level in patients with AD as compared to the control group. Larger SMD absolute value indicates greater differences. The results could be defined as significant if the 95% CI does not include 0.
A test of heterogeneity of combined SMDs was performed using Cochran Q test and Higgins I-squared statistics. The random-effect model (Der Simonian and Laird method) was applied in the presence of between-study heterogeneity (P < .05), whereas the fixed-effect model was used if heterogeneity was not observed (P ≥ .05). Publication bias was evaluated using the funnel plot with the Egger bias indicator test. 20 All analyses were performed on “Stata: Data Analysis and Statistical Software” V12.0 (http://www.stata.com/).
Results
A total of 185 records for the level of CRP in patients with AD were identified from a primary literature search in PubMed and EMBASE. After manually screening the titles, abstracts, and key data, 162 studies were excluded because they were review articles, letters, not case–control studies, laboratory studies, or studies irrelevant to the current analysis. Of the 23 reports selected for detailed evaluation, 2 studies were excluded for being duplicated, and 11 others were excluded for lack of key data such as MMSE or CRP levels, including mean value and standard deviation. The final meta-analysis was carried out for the remaining 10 studies (n = 2093; Figure 1). The main features of the included studies are summarized in Table 1. The participants recruited were from the United States, Italy, the Netherlands, Yugoslavia, Trinidad, and Japan. All the studies applied criteria of National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) to identify AD. For MMSE, one study included patients with AD with a mean score of 4.5, and the others recruited patients with a mean MMSE ranged from 16.7 to 25.3. The methods for CRP detection included human multianalyte profile (human MAP), immunonephelometric assays (ITA), and enzyme-linked immunosorbent assay (ELISA). The quality assessment of all studies is presented in Figure 2. Totally, the quality of selected studies was high because most of them answered “yes” for most items. The quality of the studies by Davis et al, Lawlor et al, and Lepara et al was relatively lower because they answered “unclear” for several items.
Characteristics of the 10 Studies Included in the Meta-Analysis.
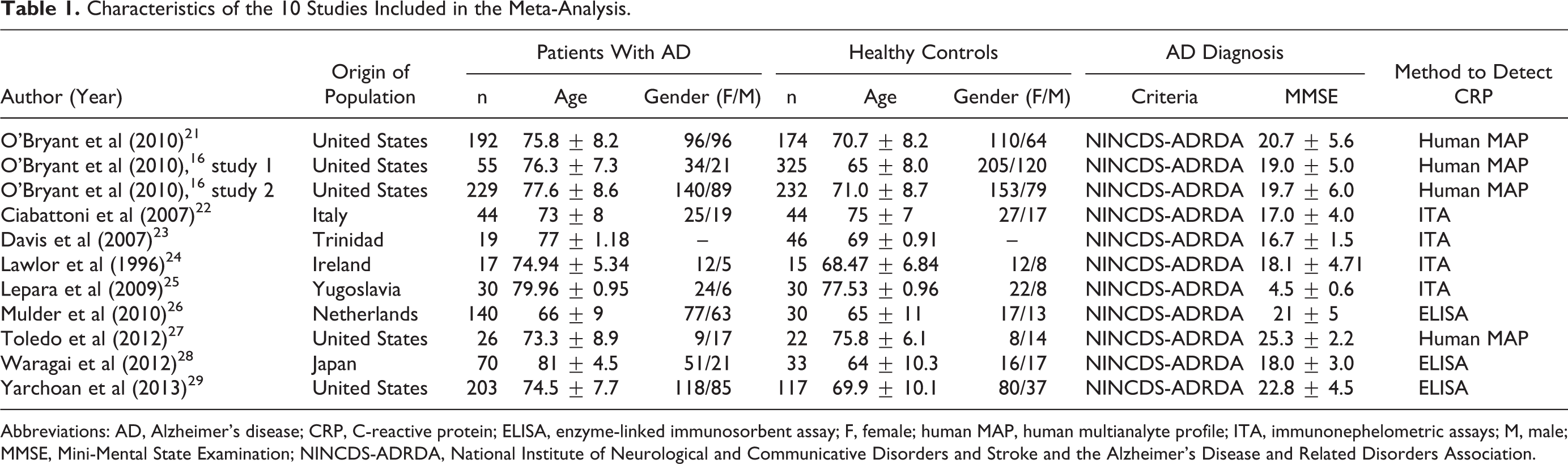
Abbreviations: AD, Alzheimer’s disease; CRP, C-reactive protein; ELISA, enzyme-linked immunosorbent assay; F, female; human MAP, human multianalyte profile; ITA, immunonephelometric assays; M, male; MMSE, Mini-Mental State Examination; NINCDS-ADRDA, National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association.
The following analyses were performed with a random-effects model for the evidence of Q-test and I2 test (case vs control: I2 = 94.1%, P < .001). In the meta-analysis, the difference of CRP levels in serum between patients with AD and healthy controls was not significient (SMD: −0.400, 95% CI: −0.827 to 0.027, P = .066). However, considering that the CRP level may be related to the dementia severity, 16 we stratified the studies by MMSE scores. 30 According to MMSE, mild, moderate, and severe dementia is defined as 21 to 26, 10 to 20, and 0 to 9, respectively. As shown in Table 1, patients with AD included in most studies were of mild or moderate dementia, with a mean MMSE ranged from 16.7 to 25.3. Only in 1 study, the patients were of severe dementia, with a mean MMSE of 4.5. Since this particular study was quite different from the others, we stratified severe dementia as one subgroup and the remaining as another. The result yielded significantly different estimate in CRP levels between the AD group and healthy group in the mild and moderate dementia subgroup (MMSE ≥ 10) (SMD: −0.582, 95% CI: −0.957 to −0.208, P = .002), and the severe dementia subgroup (MMSE < 10) has only 1 study, and therefore, no meta-analysis was performed (Figure 3).
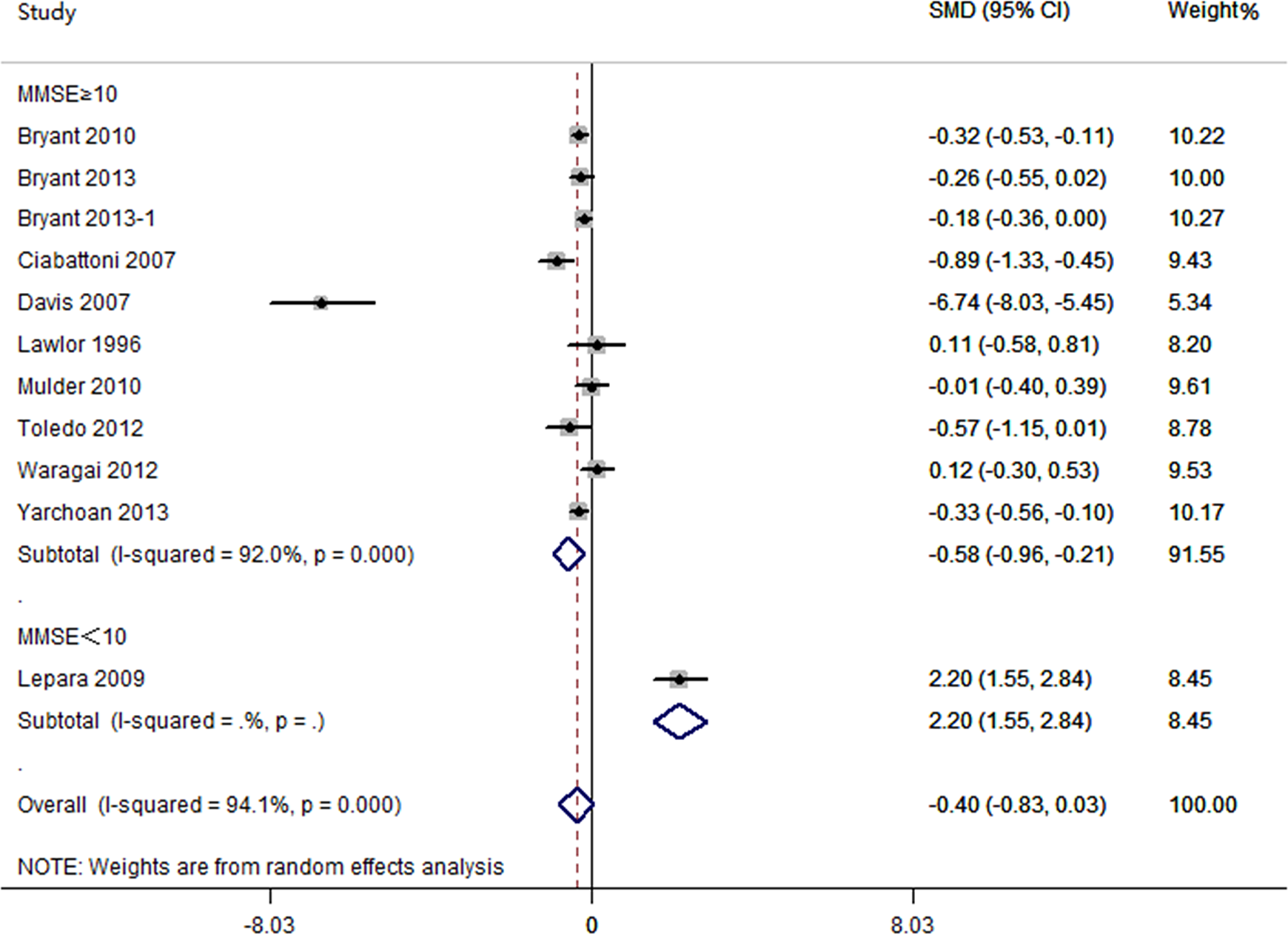
Meta-analyses for the difference of serum C-reactive protein (CRP) levels between patients with Alzheimer’s disease and healthy controls.
A sensitivity analysis was performed to determine whether review conclusion was affected by the choice of a single study. The finding revealed that no single study had effect on the pooled SMDs in the current meta-analysis (Figure 4). Finally, publication bias of the included studies was evaluated by funnel plots and Egger tests. As shown in Figure 5, there was no significant publication bias in the SMD meta-analysis, since its P values of Egger regression intercepts were more than 0.05 (P = .595).
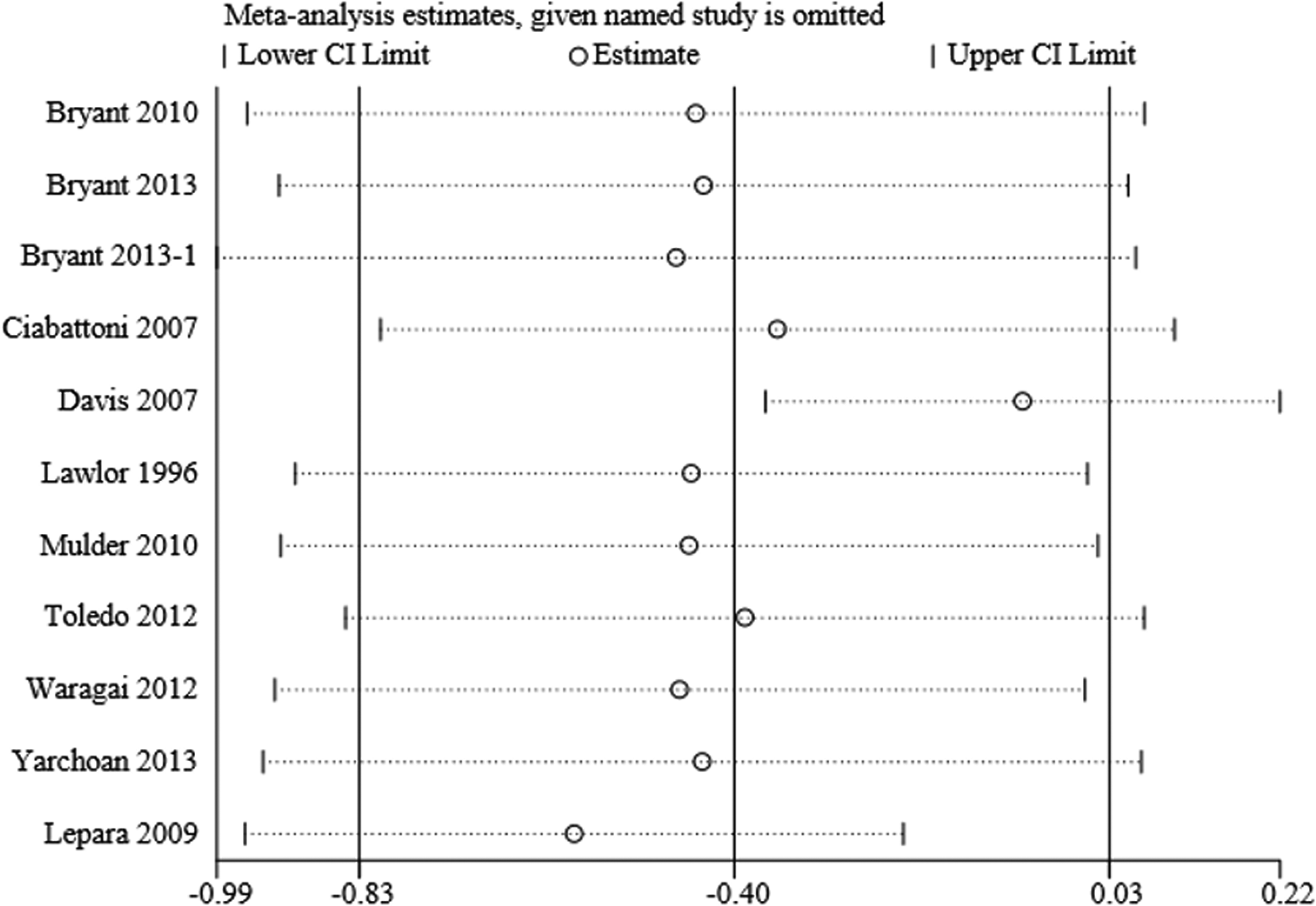
Sensitivity analysis of the difference of serum C-reactive protein (CRP) levels between patients with Alzheimer’s disease and healthy controls.
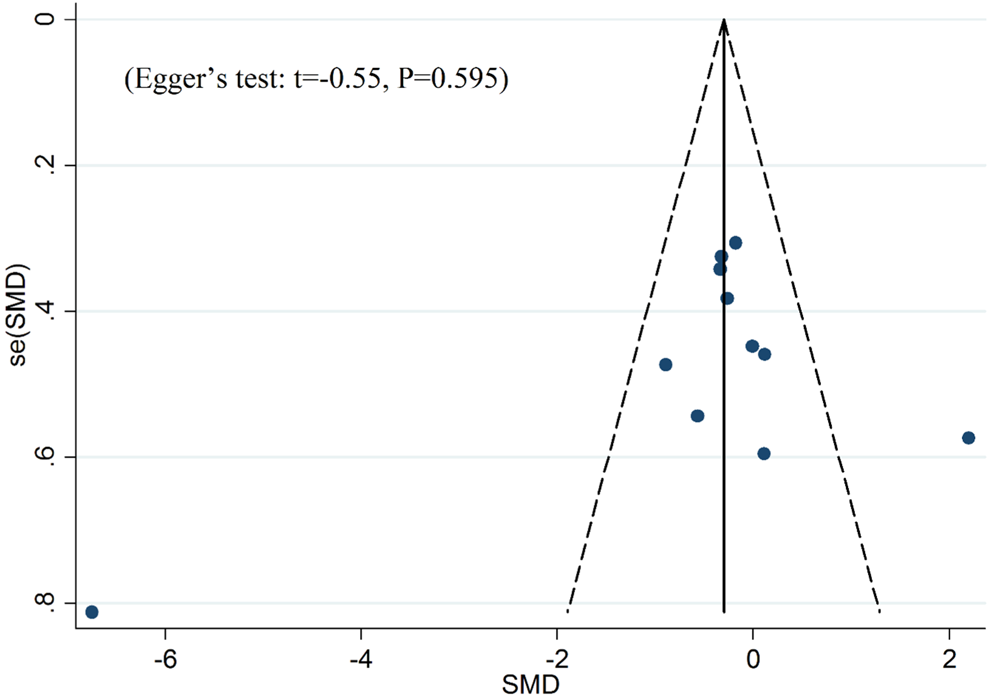
Funnel plot of publication biases on the difference of serum C-reactive protein (CRP) levels between patients with Alzheimer’s disease and healthy controls.
Discussion
This meta-analysis, recruiting 10 studies, showed no significant difference of CRP levels in serum between patients with AD and healthy controls. However, for the mild and moderate dementia subgroup (MMSE ≥ 10), the level of CRP in the AD group was significantly lower than that in the relative control group (SMD: −0.582, 95% CI: −0.957 to −0.208, P = .002).
C-reactive protein, as an inflammatory biomarker, has been widely used in clinical practice. Recent studies suggest CRP could be a predictor in a variety of diseases, including cardiovascular diseases, cerebrovascular diseases, metabolic diseases, cancers, and so on. 31 -35 Usually, elevations in CRP level may indicate worse outcome. For AD risk, a recent meta-analysis found higher CRP levels associated with increased risk. 13 This meta-analysis excluded cross-sectional studies but included retrospective or prospective studies, with follow-up periods ranged from 3.7 to 25.3 years. To date, most evidence suggested the diagnostic or prognostic value of elevated CRP for various diseases. However, several recent cross-sectional studies showed decreased CRP level in patients with AD as compared to the health controls. Although some other studies showed inconsistent or opposite results, this meta-analysis combined cross-sectional studies and found lower CRP level in the mild and moderate AD subgroup than that in the control group. The pooled data indicated the potential diagnostic of lower CRP level for AD. However, careful consideration should be taken before application in clinical practice. First, when also including 1 study for severe AD, the total SMD was not significant. The conclusion should be tempered because of the limit study number of severe AD, which is only 1. On the second hand, the data suggested CRP levels could be different in different stages. Considering immune fuction may be altered during AD process, it is possible for CRP to be decreased in mild or moderate AD and increased in the following severe stage. Second, midlife elevations in CRP may increase risk for late-life AD longitudinally. 12 Actually, O’Bryant et al found that midlife elevations in CRP were associated with increased risk of AD development. However, elevated CRP levels were not useful for prediction in the immediate prodrome years before AD becomes clinically manifest. 21 In fact, CRP levels were even lower in the early AD than the control group. Thus, it is reasonable to speculate the CRP curve throughout the life of patients with AD, which may be elevated decades before disease, decreased years before and just in the early stage of disease, and finally increased again in severe disease. Future studies should be performed to reveal the mechanism of such CRP curve. As compared to evaluating CRP once, routinely monitoring CRP levels is strongly recommended for patients with AD.
Clinical studies have demonstrated the diagnostic and prognostic value of CRP level in AD. However, it remains unclear whether the change of CRP levels is a cause or a consequence of AD. Some basic studies suggested CRP as a pathogenic factor in the progression of AD along with Aβ deposition. In rats, intracerebroventricular injection of CRP could cause learning and memory impairments. 36 In the rat adrenal pheochromocytoma cell line, CRP cytotoxicity was associated with Aβ formation and Aβ-related marker expressions, suggesting that CRP may trigger AD-like dementia. 37 However, to date, researchers focused on the effects of elevation of CRP, no studies were conducted to find the effects of decrease of CRP on AD. In addition, as compared to the healthy control, the CRP level was relatively lower in AD. However, its level was still in normal range, which is defined less than 10 mg/L. 38 In our opinion, normal CRP range should be refined by future studies.
Finally, this meta-analysis had several limitations, and the conclusion should be tempered. First, marked heterogeneity of participants existed in this analysis. The heterogeneity of the population was probably due to the difference in the characteristics of patients (age, gender, race or country, MMSE, etc), the detection method of CRP, and others. For example, considering the influence of CRP measurement to heterogeneity, we performed subgroup meta-analysis according to CRP measurement. Data of each group (human MAP, ITA, and ELISA) were comparable to the whole result. Although only the human MAP subgroup showed a significant difference (SMD: −0.259, 95% CI: −0.380 to −0.138), the trends suggested CRP level in the AD group was lower than that in the control. The heterogeneity was not existed in the human MAP and ELISA subgroups (P > .05) but only in the ITA subgroup (P < .05). To minimize the residual confounding effect caused by the heterogeneity within these studies, a random-effect model was applied. Furthermore, the total analysis includes 9 studies for mild and moderate AD and 1 study for severe AD. The results could be influenced by the study contribution, which is not well balanced. Somewhat, conclusion from the meta-analysis for mild and moderate AD may be more reasonable than the whole analysis.
In summary, our meta-analysis, representing quantified synthesis of eligible studies, showed decreased level of CRP in mild and moderate AD group as compared to the control group. It is necessary to assay CRP level in patients with AD, and routine monitoring is strongly recommended.
Footnotes
This article was accepted under the editorship of the former Editor-in-Chief, Carol F. Lippa.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: The analysis was supported by National Natural Science Foundation of China (NSFC 30800401).