
Abstract
While much of the literature on caregiver burden has focused on caregiving for people living with Alzheimer's disease (AD) there is little information on the experience of caring for a loved one living with amnestic Mild Cognitive Impairment (aMCI), the group most likely to convert to AD. A hermeneutic phenomenological approach was used to understand the organizing principles that give experiences of being form and meaning in the lifeworld. Study findings highlight the precarious nature of caregiver role acquisition and the heterogeneity that is present among informal care providers. Specifically, the findings suggest that the wearing of multiple situational masks is required by the carer to cope with accumulated progressive losses suffered as they continually adjust to their new and evolving carer identity. Support groups specific to the carers of those living with aMCI are needed in an effort to remove these masks and to validate this unique caregiving experience.
Literature on caregiver burden has tended to focus on caregiving for people with Alzheimer’s disease (AD). 1 The emphasis tends to be on later stage illness, where overburdened caregivers engage in multiple roles causing role strain and the inability to cope with stressors as interpersonal resources dwindle. 2 However, the stage in the dementia journey where caregivers form their new identity and begin to negotiate their new caregiver role with their existing social identities has received less attention in the literature. Specifically, the personal experience of caring for a family member before a formal dementia diagnosis is made is underresearched.
Those living with mild cognitive impairment (MCI), a diagnosis that differs from normal age-associated memory loss and dementia, 3 have a high rate of conversion to AD. On average, the majority of those living with the subtype amnestic MCI (aMCI) will convert from MCI to AD within 5 years. 3 -5 In Canada, the estimated prevalence of MCI is 17% among people who are aged 65 years and older. 6
Few studies address the factors that create barriers to diagnosis and support for people showing signs of MCI and their family members. 7 As well, care partners wait over 2 years on average before seeking a diagnosis for their loved one who is showing signs of cognitive impairment. 8 Yet studies suggest that early symptom detection and intervention may be beneficial to the health of both care partners and family members with aMCI. 9 When caregivers are unable to access the support they need while caring for a loved one with cognitive impairment, they can feel overtaxed and burdened. 10
Caregiver burnout is a complex and multifaceted concept that has a well-established literature base notably among dementia caregivers. 11 Burnout is not only the result of multiple losses 12 and having to cope with the multiple stressors associated with assisting with instrumental activities of daily living (IADLs) but also refers to the grief carers attribute to the decline in their loved ones health. 13 However, as noted by Adams, 14 more research on the early stages of caregiver identity formation with the intention of characterizing personal attributes of individuals who may be more prone to burnout is needed.
There are a number of gaps in current literature regarding what is needed to support the carers of those living with aMCI. First, the effect of long-term caregiving, and second, the effect of supporting someone who has received 2 diagnoses (aMCI and then AD), have not been explored. 15 In addition, research has yet to determine at what point caregivers transition into their new role and what opportunities there may be to support and educate carers during this transition. 16
A noticeable gap in the literature is the exclusion of the aMCI carers lived experiences and the absence of qualitative methodological inquiry, which explores the phenomenon of caring for a person with aMCI. As a result, no clear definition, social norms, or expectations can be ascribed to the aMCI carer role, which could result in difficulty with identity formation as aMCI carers lack of membership to a larger social group of caregivers. 17 This study seeks to gain a better understanding of the role of caring for a loved one diagnosed with aMCI.
Methodology
Hermeneutic phenomenology was used to understand the lived experience of those caring for someone living with aMCI. Phenomenology focuses on the structures of experience, that is, the organizing principles that give experiences of being form and meaning in the lifeworld. 18 The development of understanding takes place through a dialectical process, moving from descriptive inquiry toward interpretive contextualization, referred to as “hermeneutic understanding.” 19 This is achieved when the inquirer concentrates on the philosophical and historical meaning of an individual’s experience of a phenomenon and attempts to understand the meaning the individual gives to the experience while contextually situating the essence of experience in a social, historical, and cultural epoch. 20
Hermeneutic phenomenology moves away from description of a phenomenon toward an interpretation of the meaning individuals assign to a lived experience. 21 Hermeneutical phenomenology is particularly useful when there is a knowledge gap within the specific area one is interested in studying. 22 -25
Study Participants
Study participants were recruited through the Aging Brain and Memory Clinic (ABMC), an outpatient assessment and treatment clinic, at Parkwood Hospital, St Joseph’s Health Care, London. Patients referred to the ABMC with MCI, during the time of this study, were invited to participate in a larger study investigating the Memory Intervention Program (MIP) 26 and Taoist Tai Chi. The MIP program consists of 8 group sessions that include education about lifestyle factors affecting memory (i.e., diet, exercise, mental and social activity, and the negative impact of stress) and memory strategy training sessions. The aim of the program is to help people understand what MCI is and how it is different from AD. In addition, participants and their family members are educated on the risk factors associated with progression from MCI to AD. Family members are encouraged to attend concurrent support sessions facilitated by a social worker. In these sessions, family members were given tools to cope with and manage barriers in communication with their loved one as well as with other people in their social support system.
Typically, 10 to 12 people with aMCI take part in the MIP at any given time. Participants with MCI do not have to be accompanied by a family member to attend the program, and during the period investigated here, approximately half of the family members elected to attend along with their loved one. This is consistent with recommended sample sizes for phenomenological research, which suggest that a sample of 2 to 10 research participants 27 or “long interviews with up to 5 to 10 people” 28(p65) are sufficient to reach saturation.
Purposeful sampling was used to recruit participants. 25 Those eligible to participate in this study were family members of individuals who attended the MIP from September 2010 to August 2011. Participants were given a letter of information by one of the study coinvestigators (JF), the facilitator of the MIP group. Consenting participants were then scheduled for a face-to-face interview. Interviews ranged from 55 to 140 minutes in length.
Data Collection
Prior to each semistructured interview, participants completed a demographic questionnaire. To guide the interview, a semistructured interview guide was developed. To obtain carers’ prereflexive lived experiences, the interview guide focused on themes rather than specific questions. For example, probes such as “please tell me more about how you experienced that feeling/emotion/ reaction” were used. All interviews were audio-recorded, and each narrative was transcribed verbatim.
To fully understand the emergent essence of the experiences, both the transcripts and the audio-recording were reviewed multiple times. 20,29 Saturation was reached after multiple readings of the transcripts.
Analysis
To obtain a deeper understanding of the multiple components that help give meaning to the whole essence of the experience, wholistic, selective and line-by-line analyses were conducted. 20
Quality Criteria in Phenomenology
Study quality was confirmed through philosophical pedagogy, trustworthiness (study rigor), and representativeness or resonance. Through journaling, memoing, and analytical note taking, reflexivity was maintained. To maintain trustworthiness, a decision and audit trail was created to track the way themes and choices were made when collapsing themes from the selective analysis into themes that emerged from line-by-line analysis. Included in the decision and audit trail were interpretations that formed during journaling and reflexive note taking.
To ensure representativeness, the other researchers were asked to read the transcripts. 20 All study coinvestigators (MK, AZ, JF, and IG), who come from different lifeworlds, reviewed one of the transcripts and participated in a discussion about the possible themes. Reliability was achieved when main themes and the essence of the caring experience resonated with each study coinvestigator, and a shared understanding was realized by all.
This study was approved by The University of Western Ontario Ethics Board for Health Sciences Research Involving Human Subjects.
Findings
Five participants were included in the study. A sixth participant signed the consent form but withdrew from the study due to a health crisis. This participant did not differ in demographics from the other 5 participants (Table 1).
Participant Demographics.
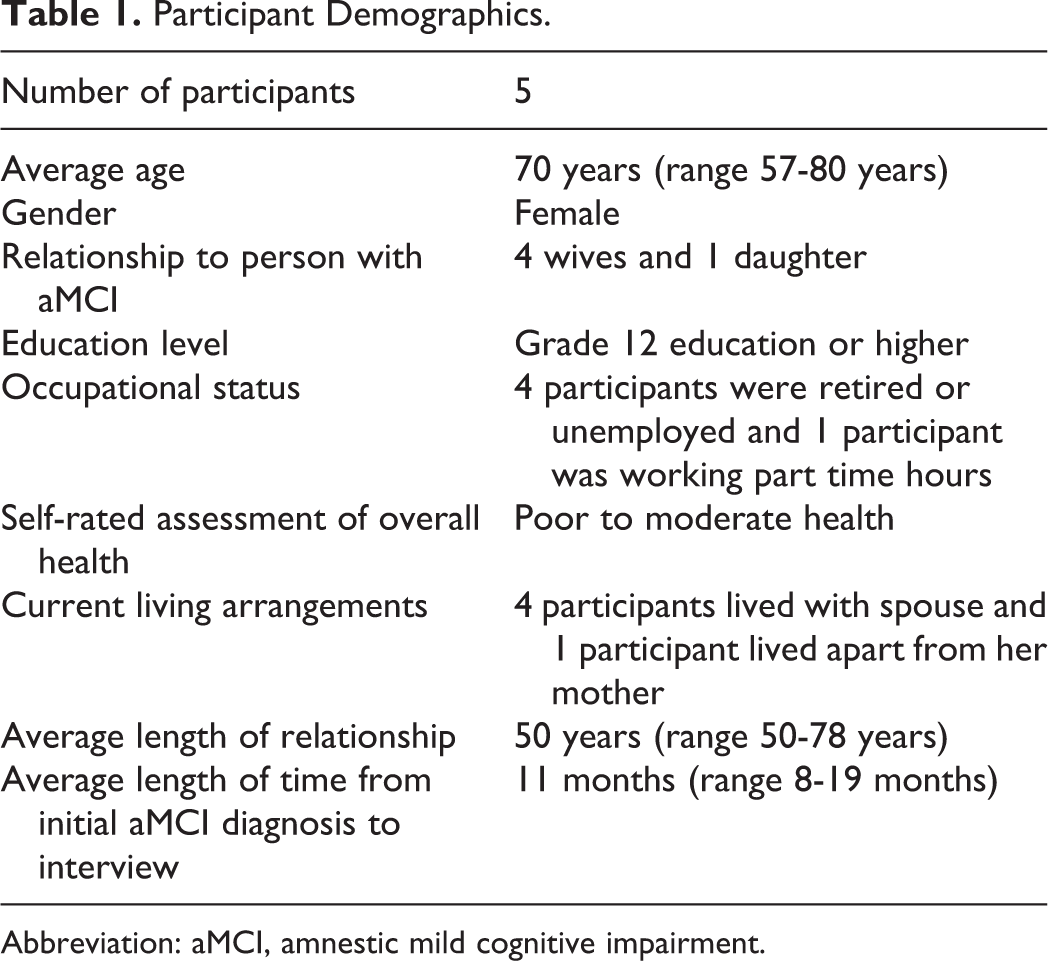
Abbreviation: aMCI, amnestic mild cognitive impairment.
The core essence of the caring experience that emerged from participant interviews was that of wearing masks. Masks were worn by carers for protection, both for themselves and to protect their loved ones. Participants experienced a need to know what mask to wear, given a particular lifeworld situation with their spouse/mother, family, friends, and others in the formal support system. Within the core essence of wearing masks, 3 specific subthemes emerged: wearing a mask: building protective identities, masking loss: multiple losses and anticipatory grief, and unmasking: validation of experience through shared understanding.
Wearing a Mask: Building Protective Identities
The carers in this study shared the experience of wearing a mask to camouflage, disguise, suppress, or protect themselves as they transitioned into new and unfamiliar roles with their loved one. Conversely, carers adorned these masks so that they may shield their loved ones from their own feelings of sadness, anger, and frustration. Participants acknowledged how challenging it was for them to appear happy and content while caring for a loved one with aMCI when their actual experience of happiness was waning. The experience of wearing a mask and selecting what mask to wear was largely dependent on the type of relationship carers had with care recipients. This experience is depicted in the following comment. [A challenge was] trying to control my own shortcomings because I would feel, I guess, that Fred (pseudonym) was doing this on purpose, you know that he wasn’t trying hard enough. You have to be understanding, you have to be patient because you do have shortcomings of your own … we care very deeply, one for the other. You know sometimes I think maybe I should just run away (she laughs); that’s not ever anything to think about.
Whether or not a loved one accepted their aMCI diagnosis had significant implications for the way the carer experienced taking on new roles and responsibilities. When these new roles did not fit with the preexisting roles a carer had filled in their life with their loved one prior to the diagnosis, the carer would start to mask their level of discomfort in this new role and wear the caregiver mask. Once a loved one had accepted that there was a problem, this allowed both the carer and the care receiver to begin to talk about their feelings of fear, frustration, and annoyance, and the carer was able to remove the mask and move into their new role of caregiver.
All of the carers experienced that until their loved ones were ready to admit that there was a problem, it was very difficult to accept this new role. Once care recipients validated that there was a change in their memory and functional ability, they also validated that this would alter the preexisting relationship they shared with their partner. I knew before James (pseudonym) was diagnosed that he had some type of impairment, but until he would recognize that and be willing to become involved with medical help, nothing was happening … it helps to know how to cope because before I used to get angry, and blame him …
When care receivers denied the diagnosis, they were also denying their need to be cared for. For the carer, this uncertainty about their own role caused resentment and frustration, as the care receiver did not validate or acknowledge the extra roles and responsibilities the carer was taking on. For those whose loved ones accepted the diagnosis, the acknowledgment made a significant contribution to the carer’s self-worth. For carers whose loved ones denied the diagnosis, the lack of validation and appreciation of the carer’s efforts caused sadness and anger.
The premorbid (prediagnosis) quality of the carer–care receiver relationship largely influenced the way the new role was experienced. Furthermore, respondents whose loved ones denied the aMCI diagnosis felt they were being lied to or deceived by their family member. All care providers made efforts to conceal their problem for as long as possible. One participant remarked that her spouse was like an alcoholic; friends and relatives were aware that there was a problem, but he believed he was hiding it so well that no one would notice. Another participant made an allusion to her husband “being in the closet” and only “coming out” once he was around other people who had a similar problem, an experience shared by the other participants. In our days you didn’t talk about “mental illness.” It was something that was hidden away. At first, he didn’t feel comfortable telling people about the diagnosis, probably because we were not really sure what it meant at first. I think it was after the first or the second session down here he met somebody who was just like him. He felt comfortable enough, he said, to come out and tell him.
They hid behind a mask of normalcy to protect themselves from the perceived judgmental gaze from outsiders who did not understand. With a poorly understood diagnosis such as aMCI, the carer themselves could not identify their place within this diagnosis. When carers experience their role as being valid, they shed this mask.
Masking Loss: Multiple Losses and Anticipatory Grief
All carers talked about some kind of loss. This loss was experienced in multiple ways, within temporal, corporal, spiritual and psychosocial contexts, and at different points of time, often at crucial transitions throughout the disease journey. The phenomenon of loss was pervasive and was experienced before, during, and after the loved one received their diagnosis. Participants described loss of identity, loss of control, loss of parent/spouse, and loss of hope for the future.
Loss of identity
Carers reported feeling that friends and family members did not validate their sadness regarding the multiple losses they were experiencing. In these instances, carers reported wearing different masks to cope. As well, all felt they no longer had a life of their own and often chose a mask of normalcy to wear to fulfill the obligations of caregiving.
Carers stated that assuming this new role took time and energy away from participation in their old life, which translated into feelings of lost self or identity. Carers also acknowledged a desire to get respite or to get away from their caring role, which created a feeling of dissonance as they experienced remorse about needing this time away. I’m probably resenting him because I’m having to give up a lot of my things because of course it takes time … You just all of the sudden feel like you don’t have any life, and that could maybe just be part of when you retire … I don’t know that, I just know … sometimes you just think, “oh, if I could only just get away.” If I could get away just so I could be me (she is getting teary-eyed) without thinking, “Now is that the right way to do that, or is that the right way to answer that?”
Loss of control
Loss of control, closely aligned with loss of identity, was complicated by the complex nature of the existing relationship prior to diagnosis. Participants commented that they felt less autonomous in their decision-making abilities, as the person with aMCI was often part of any decision made. For carers who had strained relationships with their loved one with aMCI prior to diagnosis, the ability to gain control in the relationship appeared to be an important and powerful experience. Perceived lack of control manifested itself through physiological stress responses, feelings of helplessness in carer’s ability to control the disease trajectory, and difficulty comprehending the ambiguous nature of the aMCI diagnosis. He flies of the handle for no reason at all … It’s terrible, it’s really, really terrible. Really hard and of course it doesn’t help my health either because with the strokes and heart problems, diabetes, I have a lot of things going on.
Loss of spouse/parent
For the carers in this study, both spouse and parent relationships were redefined. Carers felt they were no longer in the traditional dyads they had come to understand, but rather, they were now caring for their loved one in a manner similar to the way they would care for a child.
For the women in this study, the meaningfulness of their relationship changed. Their new carer role was no longer congruent with their wife/daughter role due to the newly formed “working” relationship. When communication remained open between the spouses, the loss was not as traumatic; however, the knowledge that they were going into the future without an equal partner to share both the positive and the negative aspects of a relationship with was frightening and overwhelming for these carers.
Loss of hope for the future: anticipatory grief
In addition to experiencing loss on both personal and psychosocial levels prior to and after their loved one was diagnosed with aMCI, participants also experienced loss for a future that was no longer obtainable for them, given their current lifeworld.
Participants often made comments that the gradual decline they experienced in their loved ones’ abilities served as a harbinger of continued decline and eventual transition into AD. Participants’ unmet expectations were the hardest to reconcile as anger and disappointment were conjoined with their want to be supportive and nonaccusatory, knowing it was unfair to blame their loved one for their inability to change the outcome of their diagnosis.
For some of the participants, looking forward and anticipating the future was too frightening to contemplate and negatively impacted their desire to care for their loved one at the present time. Carers often spoke of the need to take each day as it came, dealing with new issues or obstacles as they arose.
Unmasking: Validation of Experience Through Shared Understanding
Carers actively sought validation in different ways. While for some obtaining a diagnosis validated their experience, for others validation was obtained through discussion with others who had also experienced caring for someone with aMCI.
The journey from initial signs and symptoms to receiving the aMCI diagnosis differed among the study participants. However, for all 5 participants, this journey was disjointed, nonlinear, and problematic. As well, the journey from symptoms to diagnosis frequently caused both the carer and care receiver undue stress and strain.
Receiving the aMCI diagnosis came as a relief to these carers. The negative emotions the carers experienced were validated because they were able to forgive themselves for the anger and resentment they were internalizing and unable to express to their loved ones. Once a formal medical authority established the diagnosis, carers were able to reduce the level of blame they were placing on themselves. The experience of receiving the diagnosis was both validating and a relief.
Where this validation was most profound was through meeting other people and sharing similar lifeworld experiences. By meeting other people who had been through a similar experience, concealed and masked feelings of isolation, loneliness, and fear were validated. As a result, the carer felt less alienated and alone. If we got nothing (else) out of the course, (it) was meeting other people going through the same thing and being able to talk, not only for me, but for my husband. It’s been wonderful. Absolutely wonderful … the ladies here all understood exactly what I was saying and what I meant … and how can they know unless they have gone through something? … there are Alzheimer’s groups, I know that and if there is nothing else you can go there but, and I know it’s difficult, but if there is one, just for the one you are dealing with (meaning an MCI support group), it’s so much easier to go and acknowledge the other people and them acknowledge you and accept what you have to say and listen.
The masks worn by the carers to conceal their true feelings from friends, family members, and their loved one with aMCI were removed once they felt safe enough to allow their feelings to be validated. By meeting other people who had been through a similar experience, concealed and masked feelings of isolation, loneliness, and fear were validated, and the carer felt less alienated and alone. Carers also noted that the stories they heard from other carers during the MIP provided insight into what they could anticipate. Sharing experiences helped the carer experience less fear about the future and provided a feeling of encouragement that they would be able to fulfill their carer responsibilities. While the level of care being provided varied, carers acknowledged that the support group allowed them to be honest and open about their frustration and anger. Unmasking themselves and exposing their anger helped carers to feel connected to the others in this study.
Discussion
Wearing a Mask: Connecting Findings to Caregiving Literature
The notion of role transition has been well explored in caregiver literature. However, the attention paid to the early stages of caregiver role transition has only been investigated recently. 17,1,30 While the experience of “wearing a mask” was not a common finding that came out of the caregiving literature, it is supported in the discourse surrounding caregiver role acquisition and formation. Caregiver Identity Theory (CIT) 30 suggests that the career of caregiving is a series of transitions that result from the caregivers ever-changing care context (changes in dependency level of the care recipient and changing levels of activity and responsibility for IADLs).
The CIT proposes that caregivers not only change their behaviors but also change the way they see their role in relation to the care recipient. What this means and how it relates to the experience of caring for loved ones with aMCI is that carers are constantly undergoing a change in their own identity and self-concept. This identity change happens because of increased levels of dependence a care receiver begins to display. The care tasks that are required to support and maintain the health of the care recipient become inconsistent with the expectations the caregiver had from their initial relationship with the care recipient. The theory also maintains that other changes in the care context, such as decrease in the level of informal support and formal resources, may also create a change in the caregiver’s identity. 30
In their study of family caregivers who provided support to people dying in the home, Carlander and colleagues discovered that experiencing different life events, which the caregiver had not anticipated experiencing, forced the caregiver to form an alternate self or a new identity in order to manage the unexpected. 17 In this instance, one could assume that a person who is caregiving for their loved one at home is forming a new identity in order to shield themselves from the fear of the unknown, similar to the notion interpreted as wearing a protective mask.
This “modified-self” is continually reinvented in order to protect, transform, and support the care receiver as well as the caregiver. 17 The authors also proposed that forbidden “thoughts,” or rather those things that people think but are afraid to say because they are socially unacceptable are part of the process of self-modification. 17
For the women in this study, forbidden thoughts were often expressed. Comments such as “sometimes I’d like to just run away” and “I wish I could just shake him” or even “sometimes I don’t want to be there for her” would be considered forbidden thoughts. This uncomfortable experience of thinking forbidden thoughts and feeling guilty about these thoughts could be a by-product of entering into a new role which has socially accepted rules that are not yet accepted by the caregiver. However, the modified-self steps in to overrule the forbidden thoughts or rather a person wears a mask to prevent the care receiver from being hurt as a result of the disclosure of these thoughts. Future studies could focus on to what extent the carers modified self (or mask) is experienced while caring for a family member with aMCI and what social rules and norms are required for a carer to assimilate with this new role.
Multiple Losses and Anticipatory Grief: Connecting to Existing Literature
The experience of losing a spouse or parent was a theme that was pervasive among the women in this study. In addition, loss was experienced in different ways and at different points in time throughout the aMCI journey. When trying to interpret the experience and make references to previous scholarly literature on loss and grief among caregivers, the majority of the articles published deal specifically with caregivers of people with dementia. However, very recently, a novel research area has emerged looking at people who care for family members with a diagnosis of MCI. The overall finding from this research area is that carers in this specific context experience ambiguous loss. 31-33
Ambiguous loss is defined as “the process of experiencing the phases of normal bereavement in advance of the loss of a significant person.” 32(p159) This type of loss is experienced when a loved one is physically present but emotionally, psychologically, or spiritually absent. As emotional, psychological, and spiritual changes are frequently experienced among those living with ADOD and MCI, their carers may experience such a loss. The person with dementia or aMCI is still physically present, grief is static, but life does not go on in the fashion it once did. As a result, care providers have the constant reminder that their loved one will die before them. 33
When there is no validation of a point of death, a person caring for a loved one with aMCI or dementia is unable to reach closure, and there can be no resolution of their grief until their loved one passes away. The usual social recognition of death, such as a funeral or wake, which serves to commence the mourning of a loved one, is put on hold, and the caregiver continues to grieve and mourn the loss of their relationship with their loved one prior to their passing. 34 In her study of married couples coping with ambiguous loss as a result of MCI, Blieszner and Roberto asserted that care providers have “great difficulty in identifying and using effective coping strategies because of the psychological incongruence and confusion some people experience.” 34(p15)
In addition to experiencing loss and anticipatory grief, the carer can experience ambiguity and confusion around the MCI diagnosis. 35 The uncertain and fluctuating nature of MCI can simultaneously be comforting and disconcerting to both care provider and receiver. Carers in this study celebrated the fact that their loved one had not been given a diagnosis of AD. However, the multiplicative effects of fear of conversion, the uncertain length of time to AD diagnosis, the possibility of regression, and the lack of understanding from other people created perturbation among the carers in this study.
For the majority of the respondents in this study, the ambiguity of the diagnosis was also experienced prior to receiving a formal diagnosis, as the carers admitted to knowing that there was a problem with their loved one’s memory for quite some time. Carers responded that they were forced to seek out information on their own, looking to find an explanation in the form of some kind of answer that could cure their loved one. This was also a finding from Bleizner and Roberto. 34 In their study, care providers reported the experience of ambiguity prior to receiving the diagnosis as an uncertain loss which was further described as a need to make sense out of the change in their loved one. Yet by looking for an answer, they were further losing the expectations they had for the future.
The overall experience carers had in this study with regard to caring for their loved one long term was apprehension and ambivalence. Carers expressed concern about their ability to provide care on their own for an undetermined amount of time with the knowledge of what the future could be like for them. Findings from a study of 80 caregivers of people newly diagnosed with MCI echo the concerns the respondents in this study expressed. Carers were apprehensive of the future because they all intuitively held the knowledge of what losses they would face. They knew that the losses they had already endured would continue to be compounded going forward. 33 Losses identified in Holley and Mast’s study 33 included loss of personal freedom, loss of finances, loss of meaningful communication, loss of family cohesion, loss of emotional closeness, and loss of the person with MCI’s personality.
Anticipatory grief is a complex and multifaceted concept which captures the emotional response to an impending loss of a close friend or family member and the associated losses from the past, present, and future. 36 For the carers in this study, the multiple losses they experienced shaped their self-concept and made them question their ability to continue to provide support to their loved one long term.
This study highlighted the importance of shared understanding and communication with peers who occupy similar life world experiences, thereby validating the phenomenological approach to the study. Future research on aMCI and individuals who will be potentially providing long term caregiving to loved ones with AD could benefit from utilizing the unique expertise and recommendations from those individuals who have a clear understanding of the aMCI diagnosis and who can thoughtfully reflect on their experience. It is through coconstruction of meaning that these carers and I were able to come to better understand the experience of caring for a loved one with aMCI.
Study Limitations
When conducting the literature review for this study, it became apparent that phenomenology as a method for investigating the experience of those caring for a family member with aMCI is a novel research area. The existing literature strongly supports the findings of this study, a further check for resonance. Because this research is qualitative, and the focus was specifically on the experience of the participants in this study, there is no concern about the findings being generalizable. Nevertheless, the participants in this study were demographically homogenous. Each participant was caucasian, female, and older than the age of 50. While study findings cannot be generalized to people who fit these demographic characteristics, future studies would benefit from exploring and interpreting the experience of different social groups, specifically individuals who do not have access to specialist memory clinic services and specialized geriatric health care professionals.
Although this study group had the unique experience of attending the MIP, the study was able to explore the phenomenon of the caregiving experience for those caring for a loved one with MCI, and subsequently the carers in this study probably had above-average insight compared to a person who had not attended either the MIP or the caregiver support session. What this study captured was that understanding and validation come from shared experience.
Future Directions
Understanding the essential experience of wearing a mask and anticipatory grief among caregivers of people with aMCI has great potential to supplement future research. As a field of research, the “aMCI caregiver” has not yet been well developed in the current literature. Further research could benefit from exploring the carer role among those who care for individuals diagnosed specifically with aMCI. Because this group has the highest risk of converting to AD, care providers are an at risk group for developing caregiver burden and the negative health effects that are associated with caregiving.
Should future studies develop a better understanding of this phenomenon and should evidence-based strategies that mitigate the caregiver burden be identified, early placement into long-term care and the associated negative economic consequences for both the carer themselves and the health care system could be minimized. With the ever-increasing numbers of older adults over the next 20 years and with the increasing numbers of those with AD, finding a way to support carers over the long term so that they can support their loved ones who convert from aMCI to AD is of the utmost importance.
Another challenge is how to deliver the support to an undefined group of carers. If there is not a sufficient base of support for the aMCI carer, they will not go looking for the support programs and services until their loved one is much farther along in their disease trajectory. Future research could be conducted with the family doctor who often serves as the first line of contact for family members concerned about their loved one’s memory. Future research could focus on the identification of strategies that could close the knowledge gap that seems to exist between the family practitioner and exiting support services for aMCI care providers.
An area of research that could be helpful for this specific population of carers could identify aspects of peer support that are positive in reducing early LTC placement and reduce caregiver burden long term. Future studies could address what existing support groups are offered, what adult learning strategies are the most accessible for this population, and also how to deliver sustainable support programs in the community.
Conclusion
Using phenomenology to understand the lived experience of caring for a loved one with aMCI provided a deep and rich platform to investigate the meaning these carers gave to their newly formed identities. For the carers in this study, the transition from partner/child to care provider was demonstrated through the wearing of multiple masks to conceal feelings associated with the changing relationship with their loved one, especially when dealing with anticipatory grief due to multiple losses. These masks, in essence, became a coat of armor to help carers deal with the challenges of the social world. Caring masks were worn and interchanged depending on what coping strategy was contextually appropriate. Carers were able to shed these masks when they experienced validation from others caring for a loved one with aMCI.
Footnotes
This article was accepted under the editorship of the former Editor-in-Chief, Carol F. Lippa.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.