
Abstract
Introduction:
The study was undertaken to evaluate the postganglionic sympathetic sudomotor function employing the quantitative sudomotor axon reflex test (QSART) in tauopathies Alzheimer’s disease (AD) and behavioral variant of frontotemporal dementia (bvFTD).
Methods:
Patients were recruited in a prospective pilot study. A structured history was taken and QSART was recorded.
Results:
In all, 15 patients with AD (7 female) and 14 patients with bvFTD (9 female) were included. Mean age (±standard deviation) of patients with AD and bvFTD was 74 ± 9 and 71 ± 10 years, respectively. Severe sudomotor dysfunction (Composite Autonomic Severity sudomotor score 3) was present in 3 (20%) patients with AD and 0 (0%) patients with bvFTD (P = .037). The upper extremity was only involved in 1 patient with AD and 1 patient with bvFTD. Sweat results of the 4 recording sites did not differ between both groups. Patients’ history correlated with severe autonomic symptoms as assessed with QSART.
Conclusion:
Postganglionic sudomotor involvement in AD and bvFTD is most likely not part of the disease.
Keywords
Introduction
Autonomic dysfunction in Alzheimer’s disease (AD) was in focus of interest in a number of studies. These studies mainly focused on cardiovascular autonomic dysfunction. Allan and coworkers in 2007 reported, that in 39% of patients with AD pathologic cardiovascular autonomic tests were observed, 34% suffering from orthostatic hypotension (OH). 1 A relationship between cognitive impairment and OH was reported, although the causal relationship remained unclear. 2 A number of authors have found signs of cardiovascular dysfunction in patients with AD such as reduced 30/15 ratio, 3 impaired sympathetic response to standing, 4 or depressed baroreceptor reflex sensitivity. 5
In contrast to cardiovascular autonomic studies, until recently, there was little attention paid to the sudomotor autonomic nervous system in tauopathies. In fact, there is evidence that amyloid β may directly impair cholinergic transmission. 6 In addition, an AD mice model, more vulnerable to amyloid β by additional p75 deficiency, proved severe sudomotor dysfunction and reduction in sympathetic postganglionar target organ innervation. 7 In humans, data are lacking on whether deficits in sympathetic function are of central or peripheral origin. 7
Recently, the sympathetic sudomotor function was investigated in patients with AD using the Sympathetic Skin Response (SSR) test; a research article by Zakrzewska-Pniewska et al 8 observed a pathologic SSR latency in 26% of their patients with AD. Negami et al reported an abnormal SSR in a small minority of their cohort, although only the amplitude of the SSR was evaluated and the latency was not reported. 9
The SSR is a polysynaptic reflex with a suprabulbar, bulbar, spinal, and peripheral components. 10 Articles employing the SSR are methodically unable to identify the anatomical site of lesion (central or peripheral sympathetic neurons). The SSR in addition is a surrogate measure, and patients with congenital absence of sweat glands (ectodermal anhidrotic dysplasia) show SSR responses. 11
Given the current data on sudomotor dysfunction in patients with AD, the question arises whether the peripheral sympathetic neurons or sweat function might be involved in tauopathies in analogy to the in vitro mouse model. 7 A method to evaluate the postganglionic sympathetic sudomotor function is the quantitative sudomotor axon reflex test (QSART). 12 A pathologic QSART reveals postganglionic sympathetic dysfunction.
Current data are limited to AD and do not include other tauopathies. For behavioral variant of frontotemporal dementia (bvFTD), there is no sudomotor data available so far but preganglionic sudomotor dysfunction was demonstrated in a kindred having pallidopontonigral degeneration with N279K mutation. 13 This is to our knowledge the first pilot study to evaluate the sympathetic postganglionic sudomotor neuron in patients with tauopathies AD and bvFTD.
Methods and Participants
Patients
Autonomic function tests were performed in a prospective pilot study at the Autonomic Unit, Department of Neurology and Psychiatry, Johannes Kepler University, Linz. Alzheimer’s disease was diagnosed according to the McKhann criteria. 14 Behavioral variant of frontotemporal dementia was diagnosed according to the revised criteria by Neary et al. 15 Patients and their relatives gave written informed consent to be enrolled in this study. The study was approved by the Ethical Committee of the province of Upper Austria.
Clinical Assessments
All patients received an extensive medical assessment including medical history, indirect history, and investigation of concomitant diseases; clinical neurological examination including Unified Parkinson’s Disease Rating Scale, Tandem-walk performance, Timed Get Up & Go, and Tinetti Test; full neuropsychological assessment including Frontal Assessment Battery, CERAD-Plus, Stroop Word-Colour Test, aphasia status; and cerebral imaging employing 1.5 Tesla MRI. Significant medical causes for secondary dementia were excluded. Clinical follow-up was performed every 6 months. Patients and caregivers were asked to fill out an autonomic symptoms scale 16 Results to question 5 (“Is sweating in your feet decreased compared to the rest of your body?”) and 6 (“Is sweating in your feet decreased or absent (for example, after exercise or during hot weather?”) were compared to QSART results. In addition, if these data were not provided, a standard autonomic history chart was applied including the question “Is sweating reduced in feet?” 17
Patients were rested in supine position 15 to 20 minutes before the test. Recordings were performed in an acclimatized room kept on a stable controlled temperature of 23°C. The QSART, which quantitatively evaluates the postganglionic sympathetic cholinergic sudomotor axon, was measured with the Q-Sweat device (WR Medical Electronics Co Maplewood, MN, USA). It was routinely recorded from the following 4 sites: medial forearm three-fourths of the distance from the ulnar epicondyle to the pisiform bone; proximal lateral leg, 5 cm distal to the fibular head; medial distal leg, 5 cm proximal to the medial malleolus; and proximal foot over the extensor digitorum brevis muscle.
A multicompartment chamber was filled with 10% acetylcholine. The acetylcholine compartment is separated from a second compartment continuously measuring humidity. 12 Iontophoresis of acetylcholine into the skin was performed by passing a 2 mA of constant current across the skin. The postganglionic sympathetic sudomotor axon terminal is consecutively activated by the acetylcholine and the impulse travels antidromically, reaches a branch point, and then travels orthodromically to release acetylcholine from the nerve terminals, evoking the sweat response. Sweat production below the sweat compartment was continuously measured by circulating air connected to a high precision hygrometer (Figure 1).
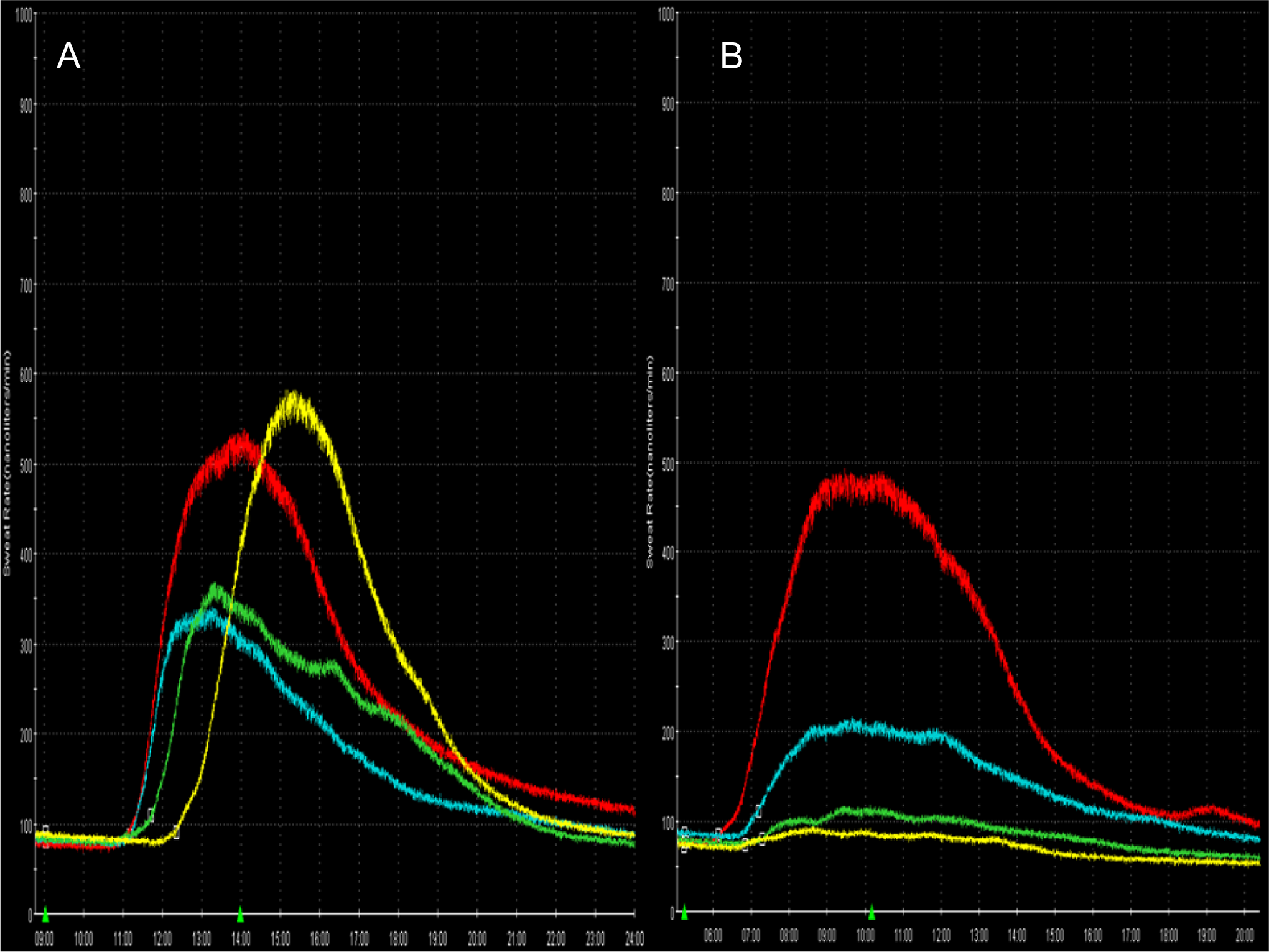
A, Normal QSART and (B) pathologic QSART with length-dependent decrease in sudomotor function. First green triangle: iontophoresis start, second green triangle: iontophoresis stop, red trace: arm, blue trace: proximal leg, green trace: medial distal leg, yellow trace foot.
Medications, which might have an influence on autonomic test results (eg, β-blockers and antidepressant drugs), were stopped at least for duration of the double half-life before testing.
Sudomotor volume results were interpreted according to the sudomotor score of the Composite Autonomic Severity Score (CASS), 18 including the interpretation of length-dependent patterns as pathological if the foot volume was one-third or less of the proximal leg volume.
Exclusion Criteria
Tests showing artifacts (eg, sweat compartment leakage) were excluded.
Statistical Analysis
Single factor variance analysis or independent t test was used to compare differences across groups in normally distributed data. Fisher’s exact test was employed to detect the presence of differences across groups in the categorical baseline characteristics. All statistical tests were performed with SPSS version 20 (SPSS Inc, Chicago, IL, USA).
Results
In all, 15 patients with AD and 14 with bvFTD were included. No patient had to be excluded due to artifacts. Demographic characteristics are summarized in Table 1.
Comparison of Demographic Characteristics and Quantitative Sudomotor Axon Reflex Tests in Individuals With AD and bvFTD.a
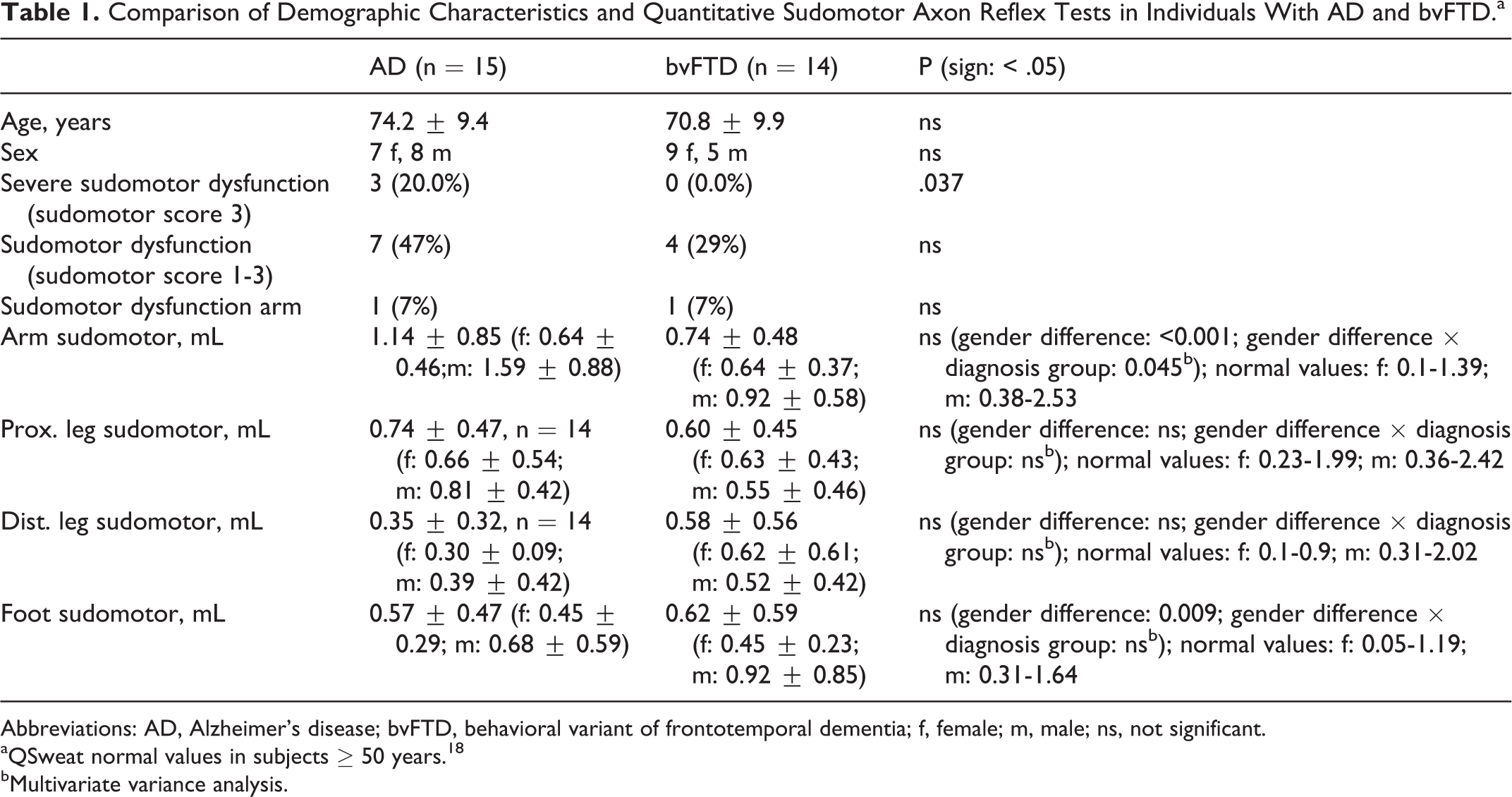
Abbreviations: AD, Alzheimer’s disease; bvFTD, behavioral variant of frontotemporal dementia; f, female; m, male; ns, not significant.
aQSweat normal values in subjects ≥ 50 years. 18
bMultivariate variance analysis.
In total, 3 cases with AD and 1 case with bvFTD were having diabetes mellitus (DM). A positive sudomotor score was found in 7 patients with AD (3 = severe, 1 = moderate, and 3 = mild) and 4 patients with bvFTD (0 = severe, 2 = moderate, and 2 = mild). One female patient with AD (aged 69) with a long-standing history of DM had all sweat recording sites but the hand reduced. All other cases with diabetes had no signs for autonomic neuropathy and a normal QSART. Sweat production in the forearm was reduced in 1 patient with AD (85% of normal value) and 1 patient with bvFTD (45% of normal value). All other patients had no reduction in sweat production in the forearm. There was no significant difference between sudomotor values of the 4 recording sides between both groups (Table 1). There was a significant difference between males and females in the hand and the foot. In the hand, this effect was also influencing a group difference analyzed by multivariate variance analysis (diagnosis and gender).
History taking with patient and caregiver was severely aggravated by AD and bvFTD employing structured autonomic history taking. 16,17 Only 67% of patients with AD and 71% of the patients with bvFTD were able to present a sound history on autonomic symptoms. In patients providing information for an autonomic history, data did not show significant group differences with the occurrence of sudomotor dysfunction of all grades but with the occurrence of severe sudomotor dysfunction (CASS sudomotor score 3; Table 2).
Cross-table of Sudomotor Symptoms and Sudomotor Signs Assessed With QSART.
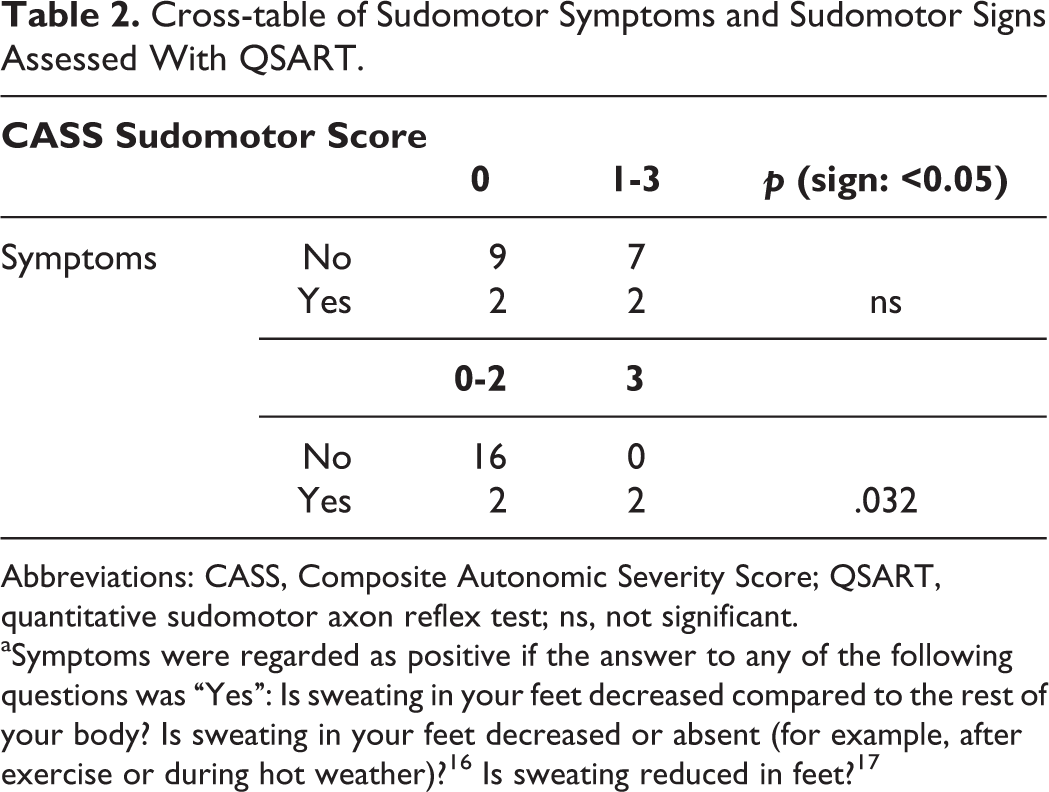
Abbreviations: CASS, Composite Autonomic Severity Score; QSART, quantitative sudomotor axon reflex test; ns, not significant.
Discussion
Severe sympathetic postganglionic sudomotor dysfunction is present only in a minority of patients with AD, sparing the hand, and absent in patients with bvFTD. Autonomic involvement is not a predominant clinical feature in AD and bvFTD. Nevertheless, sudomotor dysfunction in AD was recently reported in some patients employing the SSR. 8,9
A clear age dependency on SSR was previously demonstrated. The SSR declines with age and might not be seen in a number of patients older than 50 years. 19 Skin atrophy accompanies normal aging resulting in loss of skin small nerve fibers and sympathetic sweat glands innervation. 20 Sudomotor dysfunction might therefore be well expected in elderly patients. In contrast to the sudomotor surrogate measure SSR, QSART is a method to measure sweat production directly. QSART, like SSR, shows a clear age decline in sudomotor response in the leg but unlike SSR not in the arm. 21 Therefore, QSART testing of the arm is a valuable measure to elucidate sudomotor involvement in a geriatric cohort. In Parkinson’s disease, sudomotor involvement is known as part of the disease progress and found in up to half of the patients in the arm. 22 In addition, postganglionic sudomotor involvement could be demonstrated in 29 patients with multiple system atrophy. 23 If postganglionic sudomotor involvement was part of the disease process in tauopathies in analogy to synucleinopathies, sudomotor dysfunction would be expected at all recording sites including the arm in a reasonable number of patients. We could demonstrate severe sudomotor dysfunction only in the minority of patients with AD and not a single patient with bvFTD mainly of the foot sparing the leg. The arm however was only involved in 1 patient with AD and 1 patient with bvFTD. A strong gender effect of sudomotor response with higher sweat volumes in males was demonstrated previously and was also present in our data. 24
Based on the very low frequency of sudomotor involvement in the arm, we conclude that postganglionic sympathetic sudomotor involvement is most likely not part of the disease process in humans with tauopathies AD and bvFTD.
The first step to identify autonomic dysfunction is not autonomic testing but history taking. 25 We had severe problems to achieve a sound sudomotor history in patients with AD and bvFTD. Where a history was obtainable from the patient together with the caregiver, the history did not significantly differentiate between sudomotor signs of all grade but significantly differentiated between the occurrence of severe sudomotor dysfunction (CASS sudomotor score 3).
To summarize, severe peripheral sympathetic postganglionic sudomotor involvement is uncommon in AD and bvFTD and is most likely not part of the disease process. Autonomic history, if available, might help to identify patients with severe sudomotor dysfunction.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Bank of Austria (OeNB grant 13240).