
Abstract
Clinicians often have difficulty distinguishing between various forms of dementia to achieve a correct diagnosis. Little research has been done to examine whether awareness of one’s cognitive deficits, or metacognitive monitoring, might differ between dementia diagnoses, thereby providing an additional means of differentiating between dementia subtypes. We review articles examining metacognitive comparisons between two of the most common dementia subtypes: Alzheimer’s disease and frontotemporal dementia. Greater monitoring deficits were apparent in frontotemporal dementia than in Alzheimer’s disease, and participants with frontotemporal dementia were less likely to utilize task experience to update and improve the accuracy of subsequent monitoring judgments. Results provide evidence for the utility of metacognitive measures as a means of distinguishing between Alzheimer’s disease and frontotemporal dementia.
Metacognition, or “cognitions about cognitions,” 1 can influence our everyday lives, as these cognitions play an important role in decision making. 2 –4 Metacognition consists of monitoring or assessing one’s knowledge and controlling or regulating this knowledge 3 . Monitoring and control of our cognitive processes may be involved in even the simplest of tasks. For example, suppose an individual needs to remember to purchase groceries on her way home from work. She might monitor her memory by deciding whether or not she is likely to remember these items. She could then use these monitoring judgments to control her memory (Nelson and Leonesio 5 but see Koriat, Ma’aayan, & Nussinson 6 ) either using strategies to modify her memory—such as rehearsing her grocery list aloud—or by choosing not to modify her memory at all. If these judgments were accurate, she is likely to remember the items on her grocery list. However, if monitoring is inaccurate, inaccurate decisions may be made. 5,7,8 Although forgetting to remember milk may be trivial, forgetting one’s medication, for example, is less so and can result in significant self-harm (for a detailed review of these implications, see the study by Cosentino et al 9 ). Up to 81% of individuals with Alzheimer’s disease (AD), the most frequent form of dementia, 10 have impaired awareness of their functional or cognitive impairments, or anosognosia, a symptom common to many types of dementia that has not yet been clearly defined or understood. 11 When individuals with dementia make decisions based upon inaccurate assessments of their impairments, these decisions are likely to be impaired as well. 12 Everyday behaviors such as medication management, traveling to doctors’ appointments, and preparing meals provide risks that could result in severe consequences. Anosognosia, therefore, poses a significant safety risk to affected individuals. 13
Frequently misdiagnosed as AD, frontotemporal dementia (FTD) is the second most common type of dementia 10 and may similarly hazard the safety of affected individuals. The necessity of achieving a correct dementia diagnosis is particularly important, as a common pharmacological medication for AD—anticholinesterase—often fails to benefit, and may even harm, individuals with FTD. 14 Individuals with FTD generally demonstrate a faster rate of cognitive decline than individuals with AD and shorter survival rates from initial diagnosis (4.2 vs 6.0 years 15 ), highlighting the importance of achieving proper diagnoses and treatment sooner rather than later. Unfortunately, although FDA-approved medications exist for AD, no FDA-approved medications currently exist for FTD, frequently resulting in the use of AD medications—including anticholinesterase—by individuals with FTD. 14
Although some research suggests an ability to differentiate between AD and FTD on a neural basis, such as through structural imaging, 16 these methods are expensive and time consuming. Such difficulties may be addressed through metacognitive assessment, a low-cost means of identifying cognitive deficits. In a recent review, Cosentino 17 discussed the advances made by metacognitive assessment in understanding awareness in AD. However, no review currently exists regarding metacognition in FTD or whether metacognition differs between AD and FTD. Accordingly, in the current article, we sought to review the literature comparing metacognitive awareness between individuals with AD and FTD. The primary purpose of this review is to identify differences in metacognition that can be used to differentiate between individuals with AD and those with FTD, aiding in correct diagnoses. As secondary purposes of this review, first, we aim to increase knowledge of anosognosia as a whole by understanding how anosognosia affects individuals with AD and FTD. Lastly, we are also interested in whether metacognition differs by the means in which these judgments were collected (ie, subjective vs objective measures). To be considered for inclusion, our review criteria required each study to include both individuals with AD and individuals with FTD and to possess some form of participant self-report or self-assessment regarding cognitions or behavior.
Methods
The 2009 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) review protocol guidelines were followed for this review (www.prisma-statement.org). We combined search results from the MEDLINE (PubMed; 1950-present), PsycInfo (1887-present), and ScienceDirect (1995-present) databases (through January 2015) using the terms metacognition and Alzheimer OR metacognition and frontotemporal dementia (404 articles). We limited these search results (see Figure 1) by removing articles which appeared in multiple searches (68 excluded), which were not written in English (34 excluded), which were review articles or book chapters (98 excluded), which did not include both individuals with AD and those with FTD (198 excluded), for a total of 6 studies remaining for review. Moreover, although review articles and book chapters were not included, we examined their references, in addition to the references reported in the included articles, to ensure we included any critical articles. This resulted in a total of 2 additional studies, for a total of 8 articles in our review. Given the specificity of our interests, we did not expect to identify relevant unpublished articles; therefore, our search was conducted only on published articles. Data from all articles were independently extracted by the first author and subsequently reviewed by the second author. When interpretations of data conflicted, the authors discussed the data in question to arrive at consensus.
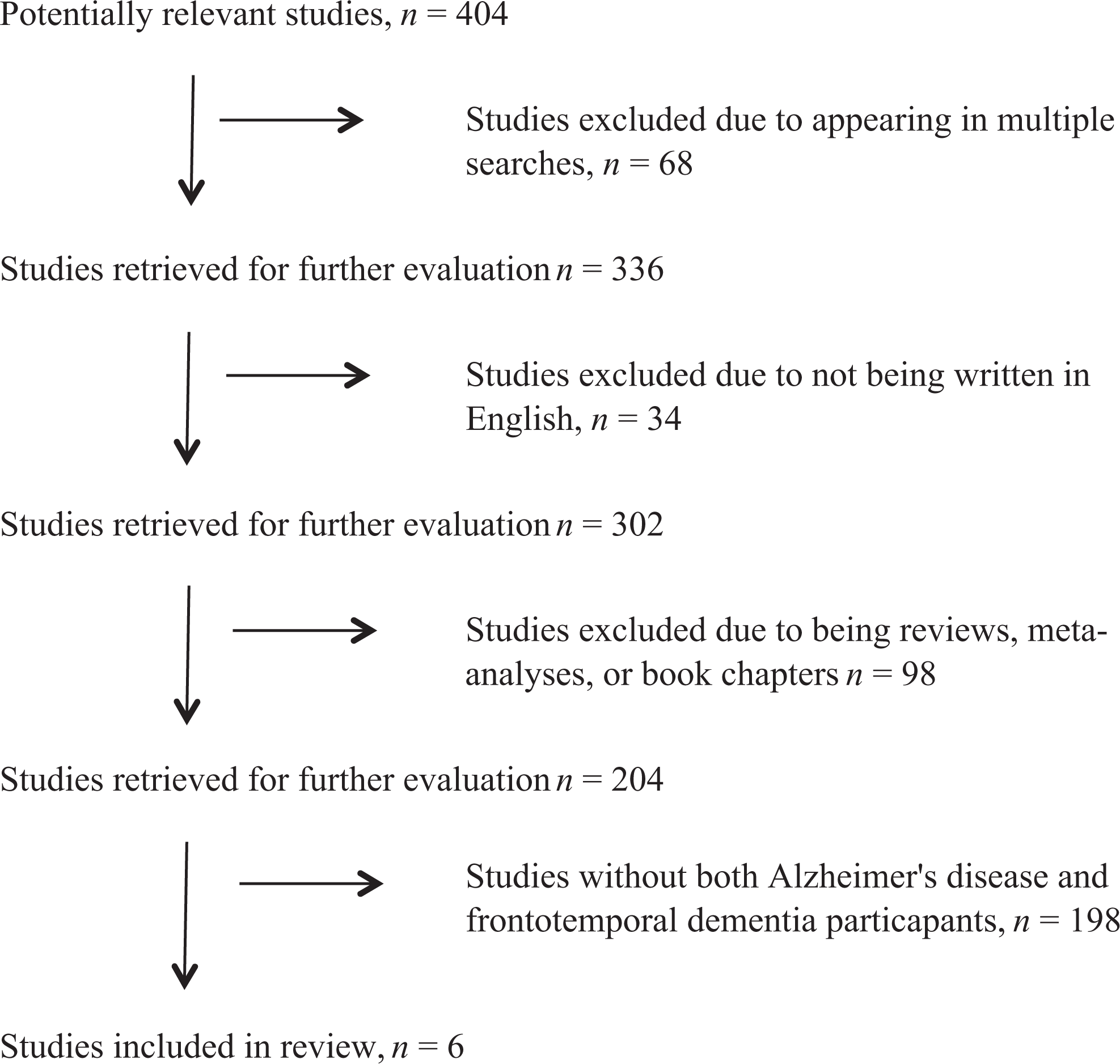
A study flow diagram of the review selection procedure.
Within these studies, FTD was primarily described either as a broad category or was further broken down into the 3 primary clinical FTD variants or subtypes: behavioral variant FTD (bvFTD), primary progressive aphasia, and semantic dementia (SD 18 ). Our review includes results for both FTD and all subtypes. No distinction is made among severity of AD diagnoses (eg, probable AD, mild to moderate AD, etc). Outcomes included awareness of changes in everyday behavior as well awareness of cognition. Measures of metacognitive awareness were collected through several methods: semistructured interviews, patient–informant discrepancies, and judgments of test performance. Principle summary measures consisted of differences in means: between individuals with AD and FTD and between both individuals with AD and FTD compared to older adult controls. Results were organized by the similarity of study design.
Results and Discussion
This review aims to identify metacognitive differences between individuals with AD and those with FTD. As metacognition is measured using different methodologies throughout the included studies (addressing such varied items as memory, behavioral changes, and tasks of everyday functioning), results are presented in the form of a qualitative review, in which only those measures and statistics relevant to the focus of this article are discussed. A total of 8 studies compared metacognition between individuals with AD and FTD, using a variety of techniques (see Table 1). Among these techniques, participant–informant discrepancy ratings were common, 19,20,21 in which both participants and their informant (typically a caregiver or spouse) provided assessments of the participant’s ability to function on a variety of tasks. Informant ratings were then compared to those of the participant, and discrepancies between these ratings indicated the severity of the participant’s anosognosia or the unawareness of his or her deficits. Another technique consisted of semi-structured interviews, 21,22 in which participants were interviewed regarding awareness of their deficits, according to a previously arranged series of questions. These interviews were then scored to provide a numerical assessment of the participants’ unawareness of deficit. Lastly, a third commonly used technique consisted of judgments of test performance. 16,19,21,23 –25 In this technique, participants were asked to make pretest or posttest judgments of their performance on a test. Rather than measuring test performance, the focus is placed on the accuracy of these test judgments as an indicator of monitoring awareness.
Summary and Quality Assessment of Empirical Studies That Met Inclusion Criteria.
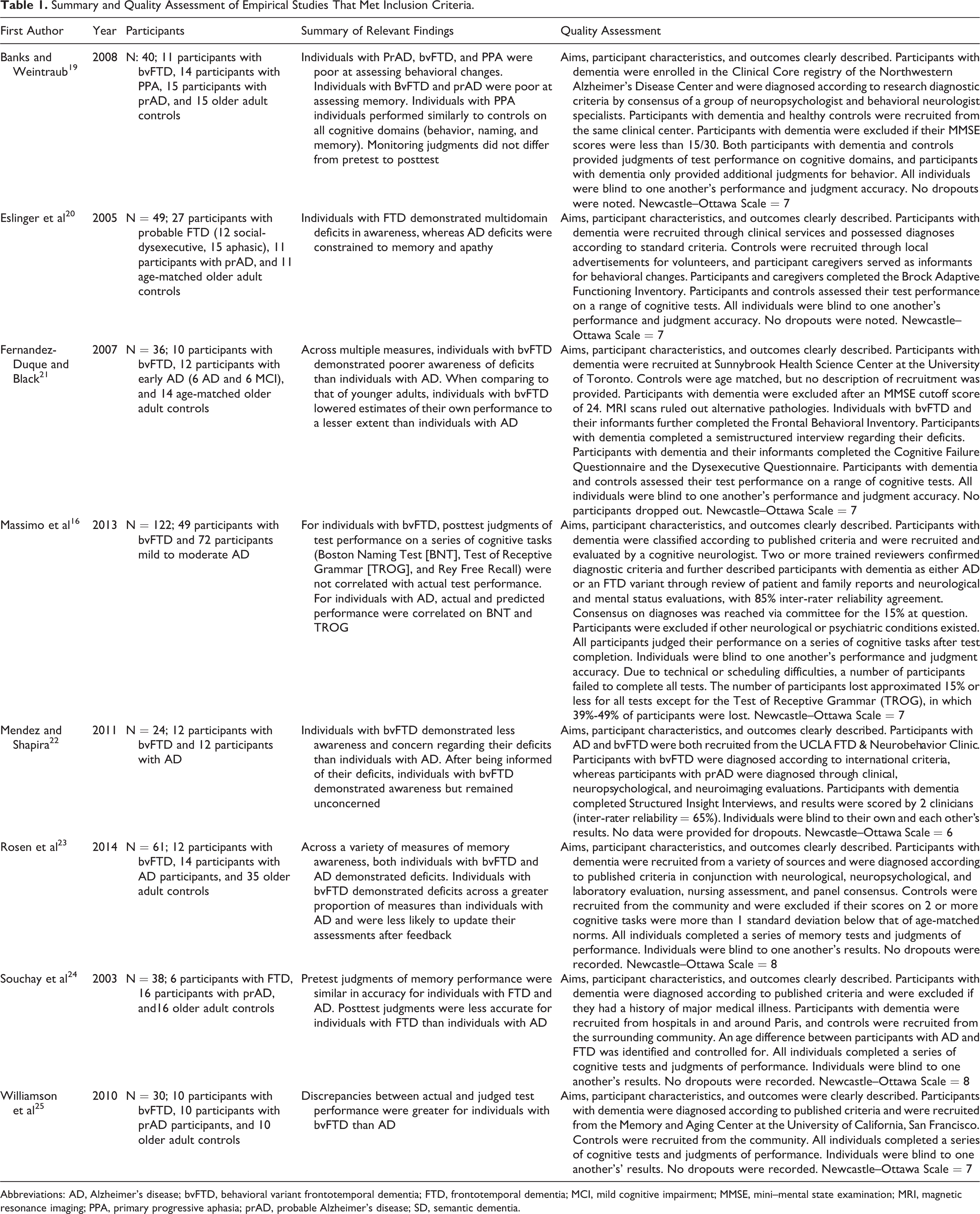
Abbreviations: AD, Alzheimer’s disease; bvFTD, behavioral variant frontotemporal dementia; FTD, frontotemporal dementia; MCI, mild cognitive impairment; MMSE, mini–mental state examination; MRI, magnetic resonance imaging; PPA, primary progressive aphasia; prAD, probable Alzheimer’s disease; SD, semantic dementia.
The objectivity of 2 of these 3 primary techniques has become a concern 16 (for a recent review, see Cosentino 17 ). For example, as noted by Massimo et al, 16 informants (typically caregivers or family members) may not be completely unbiased when providing an estimate of an individual’s awareness. Issues such as the difficulty (or ease) of caring for an individual may skew the informant’s rating of their abilities. Further, self-report scales cannot differentiate between participants’ overestimations and informants’ underestimations of the participant’s abilities. 26 In an effort to reduce this potential bias, Eslinger et al 20 compared participant–informant discrepancy ratings with those of controls and their informants. Only discrepancy scores differing significantly from those of the controls were included in further analyses of participants’ unawareness of deficit, in order to reduce informant bias. In addition to the issue of informant bias, subjective measures may be influenced by participants’ ability to use the rating scales. In an effort to address this potential problem, Banks and Weintraub 19 had participants and their informants additionally rate the self-related domains of weight and eyesight, which are not cognitively or behaviorally related but which may provide an idea of whether participants are capable of making self-relevant judgments. That is, if participants are unable to make accurate judgments of self, measuring these noncognitive and nonbehavioral domains may indicate whether factors other than anosognosia (eg, personal bias or difficulty utilizing the judgment scales) contribute to this inaccuracy. In contrast, if participants make accurate judgments for their weight and eyesight, researchers may be more confident that judgments indicating cognitive or behavioral anosognosia reflect anosognosia itself, rather than unrelated factors. As a final point of contention, it has been argued that interviews cannot provide a truly representative idea of an individual’s everyday deficits 16 (for a detailed discussion of potential confounds using clinical interviews, see Kaszniak and Edmonds 27 ). Therefore, recent work has touted the use of objective judgments of task performance as a means of examining metacognitive errors in impaired individuals. 12,23 In addition to being objective, such measures have been shown to relate to clinical measures of awareness, suggesting that while avoiding the pitfalls of subjective assessment, they additionally capture something specific to self-assessment. 12 Given these perspectives of prior methodology, this review is organized into subjective and objective measures of awareness, followed by an integrated discussion of these results.
Subjective Measures of Awareness (n = 5)
In one measure of awareness—discrepancy scores—both participants and informants (eg, caregivers and spouses) completed questionnaires rating the participant’s everyday performance. 19,20,21,25 For example, several of the studies 19,21 used the Frontal Behavioral Inventory (FBI 28 ), which is a 24-item behavioral questionnaire on items such as impulsivity, insight, distractibility, and so on. Informant ratings are then typically used as a control to compare participant ratings, against, as a measure of that participant’s monitoring deficits or changes in awareness.
When compared to their informants’ assessments, both individuals with AD and FTD were poor at assessing their everyday deficits. 20,25 Eslinger et al 20 gave participants and their informants a series of neurological assessment batteries surveying everyday cognitive, social, and emotional behaviors. Metacognitive accuracy was examined by subtracting each informant’s rating from the rating of their charge (same–different analyses). Consistent with the presupposition that healthy older adults possess relatively accurate awareness of their abilities, all control-informant discrepancy ratings failed to reach significance. Relative to their informants’ ratings of their abilities, individuals with FTD overestimated their abilities in 47% of the assessed domains, whereas individuals with AD overestimated their abilities in only 12% of the assessed domains. However, when FTD estimations were examined by subtype (described in terms of deficits, rather than clinically defined FTD variants), it was apparent that nonaphasic patients with social–behavioral and dysexecutive impairments (SOC-DYSEX) overestimated their performance in 59% of the assessed domains, whereas the other FTD subtypes (aphasic, composed of progressive nonfluent aphasia [PNFA] and semantic dementia [SD]) overestimated at levels comparable to those of individuals with AD (12% overall; 6% and 18%, respectively).
Similarly, Williamson et al 25 examined discrepancies between participant–informant ratings of everyday behavior (collapsed across individuals with AD and FTD; same–different analyses) and correlated these discrepancies with discrepancies between participants’ actual and predicted performance on tasks of everyday function from the Neuropsychological Assessment Battery (NAB). As participants judged their NAB performance both prior to and after completing the NAB (pretest and posttest judgments; discussed subsequently), this resulted in 2 correlations: participant–informant discrepancies on everyday behavior versus pretest NAB judgments and participant–informant discrepancies on everyday behavior versus posttest NAB judgments. Discrepancies between participant–informant responses were positively and significantly correlated with discrepancies between estimated and actual percentile rankings (r = .65 and .59 for pretest and posttest discrepancies, respectively). As noted by Williamson et al, 25 these correlations indicated that participants who were poor at estimating their performance on the NAB modules were also poor at assessing their performance in everyday life.
When compared to each other, individuals with FTD were worse than individuals with AD at assessing their everyday deficits, 20 although Williamson et al 25 reported these differences only as trends. Eslinger et al 20 found that, relative to their informants’ assessments, individuals with AD were able to detect changes in behavior, but that all individuals with FTD were poor at assessing changes in their behaviors, particularly within the SOC-DYSEX subtype. Banks and Weintraub 19 had participants assess performance on 2 cognitive domains (Boston Naming Test or Naming and Rey Auditory Verbal Learning Test or Memory) and one behavioral domain (FBI), both before and after completing each test (pretest and posttest judgments). In addition to the participants, each participants’ informant likewise completed the FBI to report their charge’s behavior, and this informant response was used as a measure of participants’ actual behavior. For both the cognitive measures (Memory and Naming), participant judgments of their performance were compared to their actual performance on those tests. For posttest judgments, or judgments made after each test regarding their test performance, individuals with bvFTD were poorer at assessing Behavior than Naming, whereas individuals with AD were poorer at assessing Behavior than either Memory or Naming.
Results of structured interviews again revealed that individuals with FTD were poorer at assessing their impairment than individuals with AD. 21,22 Mendez and Shapira 22 questioned individuals with AD and bvFTD on their awareness of having a disorder and its impact on themselves and on others. Participants were given corrective feedback after each of these 3 questions and subsequently completed an interview probing their awareness of this disorder. Individuals with bvFTD were less likely than individuals with AD to be aware of their disorder and, after corrective feedback, were less likely than individuals with AD to demonstrate either awareness or concern regarding the impact of their disorder upon themselves and others. Fernandez-Duque and Black 21 had individuals with AD, bvFTD, controls, and their caregivers complete a series of behavioral assessment inventories. Participants were then interviewed on their awareness of their deficits and any subsequent impact and concerns it had brought upon themselves or others. Individuals with bvFTD were less likely than individuals with AD to indicate awareness of their current deficits.
Objective Measures of Awareness (n = 7)
A frequent means of examining metacognition for memory performance is in terms of global or item-by-item judgments (see Dunlosky and Metcalfe 30 ). Global judgments are made as assessments of overall performance (eg, predicting the number of items that will later be recalled at test 31 ), whereas item-by-item judgments are made separately for each item (eg, predicting the likelihood of recalling a particular study item on a future test; for a review, see Rhodes 32 ). Global judgments have been examined extensively in metacognitive research on memory in AD 12 and to a lesser extent, in FTD. As such, we discuss global judgments first, as they comprise the majority of our results. Although few studies examined item-by-item judgments, we present them separately to highlight their importance.
Global judgments
Within the studies presented, participants were asked to judge or assess their overall test performance (e.g., number of items recalled or performance relative to others). Judgments made after a test reflect monitoring of task performance, 31 whereas judgments made prior to study reflect beliefs about memory and factors affecting memory performance. 24 Accuracy of prestudy judgments was poor, with both individuals with AD and FTD overestimating their memory performance, 19,24 whereas Eslinger et al 20 simply reported that results were highly varied, even among control subjects. These results suggest that beliefs about memory are inaccurate prior to test. Notably, however, both AD and FTD judgments demonstrated sensitivity to factors affecting memory performance. 21,23 That is, memory can be affected by cues inherent to the stimuli (intrinsic cues; eg, difficulty of the to-be-learned material) or by cues inherent to the testing (extrinsic cues; eg, type of test 31,33 ). Consistent with the common finding that performance is higher in recognition tests than in free recall, both individuals with AD and FTD utilized this extrinsic cue to accurately predict higher future performance for recognition than for free recall tests. 23 Similarly, consistent with the finding that memory performance deteriorates with age, when asked to judge the accuracy of their future test performance, both individuals with AD and FTD gave lower predictions when assessing their performance relative to that of younger adults, than relative to healthy older adult peers, although individuals with FTD lowered these predictions less than either individuals with AD or control participants. Thus, although both individuals with AD and FTD demonstrate inaccurate beliefs about memory, they also demonstrate an ability to utilize available cues to enhance the accuracy of their memory beliefs.
Most important, we examined the accuracy of posttest judgments, indicated by how closely these judgments reflected actual test performance (eg, correlations or mean difference). Overall, both individuals with AD and FTD made less accurate posttest judgments than older adult controls. 19,24,25 However, for judgments made immediately after study (but prior to test), Rosen et al 23 did not find the differences between groups to be significant. Notably, individuals with FTD made less accurate posttest judgments than individuals with AD. 16,20,23,25 For example, Massimo et al 16 reported that individuals with FTD (but not AD) failed to produce significant correlations between actual and judged test performance on all 3 tests of cognitive functioning administered. Further, individuals with FTD were poorer than individuals with AD at accurately adjusting their monitoring judgments, either as estimates of future performance or in relation to the performance of other individuals. 21,23 Relative to judging their performance to that of others their own age, when comparing their performance to that of younger adults, individuals with FTD lowered posttest judgments of their performance less than individuals with AD or controls. Similarly, when given explicit feedback on their test performance and then asked to predict their performance on a similar test in the future, Rosen et al 23 reported that individuals with FTD (but not AD) failed to make predictions commensurate with their test performance. Overall, these findings indicate that individuals with FTD demonstrate greater monitoring deficits than individuals with AD.
Item-by-item judgments
Only one study, by Rosen et al, 23 examined judged performance for individual items by individuals with AD and FTD; however, judgments were collected on 2 measures: feeling-of-knowing and retrospective confidence. For feeling-of-knowing judgments, participants rated the likelihood of recognizing individual word pairs at test, which they had previously failed to recall. After this recognition test, participants then rated their confidence in the correctness of their individual responses (retrospective confidence ratings). Feeling-of-knowing judgments were positively associated with recognition accuracy for controls and individuals with AD but not for individuals with FTD. Both individuals with AD and FTD demonstrated impaired feeling-of-knowing accuracy relative to controls, with the difference between individuals with AD and bvFTD approaching significance (p = .08). All adjustments for potential confounding variables revealed significant associations between judgments and performance for individuals with AD and control participants but no significant associations between judgments and performance for individuals with bvFTD.
Summary and Conclusion
In this review, we examined whether individuals with AD and FTD differ in their monitoring judgments. Awareness of deficit was reported either as subjective or objective judgments. Subjective measures revealed that individuals with FTD were less likely than individuals with AD to report awareness of their deficits and were less concerned by the effects of their deficits upon themselves and others. Similar results were found using objective measures. Most importantly, results from studies using objective judgments of awareness demonstrated a similar pattern in both global and item-by-item judgments. That is, individuals with FTD were less aware of their memory deficits than individuals with AD and less able to update the accuracy of their monitoring judgments, even after receiving explicit feedback. This failure to update suggests that in contrast to individuals with AD, individuals with FTD may possess a stability bias or a failure to sufficiently change or update their preexisting judgments when new knowledge is provided. 34
Although we have reviewed a number of studies, due to subtype variations within FTD, it is unlikely that these findings would hold for all variations in FTD. Although impaired insight is considered a primary feature of bvFTD, 35 it is less typically associated with the aphasia presentations of this disease (for a review of these differences across subtypes, see Snowden et al 36 ). As such, there may not be metacognitive studies documenting this association (but see Eslinger et al 20 ). In particular, Eslinger et al 20 reported metacognitive differences between individuals with FTD and AD but discovered this was driven by the results of one subtype of FTD, whereas all other examined subtypes performed similarly to individuals with AD. Accordingly, given the small number of existing studies (and the disparity of their means of metacognitive measurement), one possibility is that metacognitive performance in FTD may vary more (or less) than these studies indicate. Future research should continue to examine this as the literature grows. Additionally, further work should examine questions such as whether there is a specific cutoff in metacognitive performance that would be more indicative of FTD than AD or the reliability of metacognitive measures in distinguishing between FTD and AD (as confirmed by postmortem diagnoses). The current study, however, provides initial evidence for the use of metacognition measures as part of a larger assessment when evaluating the presence of dementia.
Footnotes
Authors’ Note
Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the National Science Foundation. We would like to thank Matthew Rhodes for helpful comments on a previous version of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science Foundation Graduate Research Fellowship Program under Grant No. DGE-1321845, Amendment II.