
Abstract
Introduction:
Previous studies have shown conflicting results on the association between smoking and cognitive function. This study aims to examine the relationship of smoking with cognitive function.
Methodology:
Data for the study, consisting of 2553 older adults aged 60 years and older, were drawn from a nationwide household survey entitled “Determinants of Wellness among Older Malaysians: A Health Promotion Perspective” conducted in 2010.
Results:
Current smokers had lower rates of cognitive impairment compared to never smokers (17.4% vs 25.9%), while cognitive function in former or ex-smokers was almost similar to that of the never smokers. Findings from multiple logistic regression analysis showed that current smokers were 37% less likely to be cognitively impaired, compared to the never smokers (odds ratio [OR] = .63; 95% confidence interval [CI]: .46-.86) while controlling for potential confounders. No difference in cognitive function was observed between former smokers and never smokers (OR = .94; 95% CI: .71-1.25).
Conclusion:
Although the findings indicated a negative association between cigarette smoking and cognitive impairment, we are unable to conclude whether this relationship is causal or affected by other unmeasured confounding factors, especially survival bias.
Introduction
With the rapidly aging global population, cognitive impairment in old age is a growing worldwide concern. 1,2 Since there is no absolute cure for cognitive disorders, 3 a growing body of research has been focusing on identifying modifiable risk factors contributing to the condition. In light of this, one of the risk factors that has been widely studied is cigarette smoking. Although there is evidence to support that cigarette smoking has considerable adverse effects on health and that smoking contributes to many age-related diseases, 4 -6 studies have produced conflicting findings on the association between smoking and dementia. 7 Observational studies suggest that smoking might be protective against Alzheimer’s disease (AD), 8 -10 whereas longitudinal studies have found that smokers have the same 11 -13 or increased risk of dementia and AD. 14 -16 For example, the findings from 2 meta-analyses of longitudinal studies concluded by Anstey et al 16 as well as Peters et al 17 have shown that current smoking is associated with an increased risk of dementia.
Although majority of the previous prospective studies have found that smoking increases the risk of dementia, surprisingly, the findings from a recent longitudinal study conducted by Wang and his colleagues 18 indicated that smokers were less likely to develop cognitive impairment compared to never smokers, after controlling for age, education, hypertension, diabetes, heart disease, and stroke at baseline. The study suggested that smoking might have protective effect for cognitive function.
In sum, a review of research focusing on the association between smoking and cognitive function shows apparently conflicting results, especially between cross-sectional and longitudinal studies. Several studies have found that smoking improves cognitive function; however, some other studies have found that smoking is associated with increased risk of dementia. Therefore, the impact of smoking on cognitive performance needs more clarification. 18 The current cross-sectional study aimed to examine the association between smoking and cognitive function among community-dwelling elderly individuals.
Methodology
Data for this cross-sectional study were drawn from a nationally representative household survey entitled “Determinants of Wellness among Older Malaysians: A Health Promotion Perspective” conducted in 2010. The methodology of the study has been previously published elsewhere. 19 Briefly, the survey used a 2-stage proportional random sampling technique to obtain a sample of 2562 older adults aged 60 years and older, with a response rate of 77%. The primary sampling units were Census enumeration blocks. The secondary sampling units were private households randomly selected from the list of all enumerated households in each block. All selected respondents were interviewed by trained enumerators. The final sample size after data cleaning was 2553 respondents.
Ethics and Approval
The study was approved by the Ministry of Health, Malaysia, and was in compliance with the Declaration of Helsinki and the World Medical Association guidelines. After providing a disclosure statement about the purpose of the survey, oral informed consent was obtained from all respondents before commencing the interview.
Measures
Cognitive Impairment
The main outcome variable was cognitive impairment, measured using with the Mini-Mental State Examination (MMSE). The MMSE assesses 5 areas of cognitive function including orientation, attention, calculation, language, and recall. The cutoff point 18 of 19 was used for detecting cognitive impairment in illiterate respondents and 24 of 25 was used for the educated. 20,21
History of Smoking
Respondents were asked whether they have ever smoked and whether they are still smoking. Based on the responses, respondents were classified into 3 main categories: never smokers, current smokers, and former smokers.
Chronic Medical Conditions
Chronic medical conditions (CMCs) were assessed using a checklist of self-reported chronic health problems including hypertension, heart disease, stroke, diabetes, cancer, visual problems, hearing problems, gastritis, asthma, kidney disease, joint pain (arthritis), and tuberculosis during the previous 12 months. The number of chronic medical conditions was categorized into 3 categories: zero, 1 to 2, and 3 or more.
Sociodemographic Factors
Sociodemographic characteristics, including age, education (in years), gender, and household income, were included in the analysis.
Statistical Analysis
The data were analyzed using SPSS version 21. A 2-step hierarchical logistic regression model was used to determine unique effect of smoking on cognitive impairment after controlling for potential confounders. Hosmer-Lemeshow tests were used to determine goodness of fit for the hierarchical logistic regression models. The P value criterion used for evaluating statistical significance was .05. Smoking status was entered in the first block. Sociodemographic factors and health factors were included in the second model, namely the variables on age, gender, educational attainment, household income, and CMCs.
Results
Table 1 presents the smoking status and demographic characteristics of the study respondents by their cognitive function. As can be seen from Table 1, 55% of the 2553 respondents who participated in the survey were women, and 40% of the respondents had no formal education. Less than one-fifth (15.9%) of the study participants indicated that they were current smokers, 17% were former smokers, and 67.1% reported having never smoked. The prevalence of cognitive impairment among current smokers was 17.4%. The former smokers and never smoked had a similar prevalence of cognitive impairment (24.5% vs 25.9%). A 1-way analysis of variance was used to test for differences in cognitive function among the 3 groups. Since the assumption of homogeneity of variance was violated (Levene Statistic = 14.94, P ≤ .05), the Brown Forsythe F ratio was reported. There was a significant difference in cognitive function among respondents by smoking history, F 2, 1248.13 = 20.84, P < .001. Tukey post hoc comparisons of the 3 groups indicated that the mean cognitive function score of the current smokers (M = 25.86, standard deviation [SD] = 4.68) was significantly higher than the former smokers (M = 24.43, SD = 5.56) and never smokers (M = 23.99, SD = 5.78).
Distribution of Study Variables by Cognitive Impairment.a
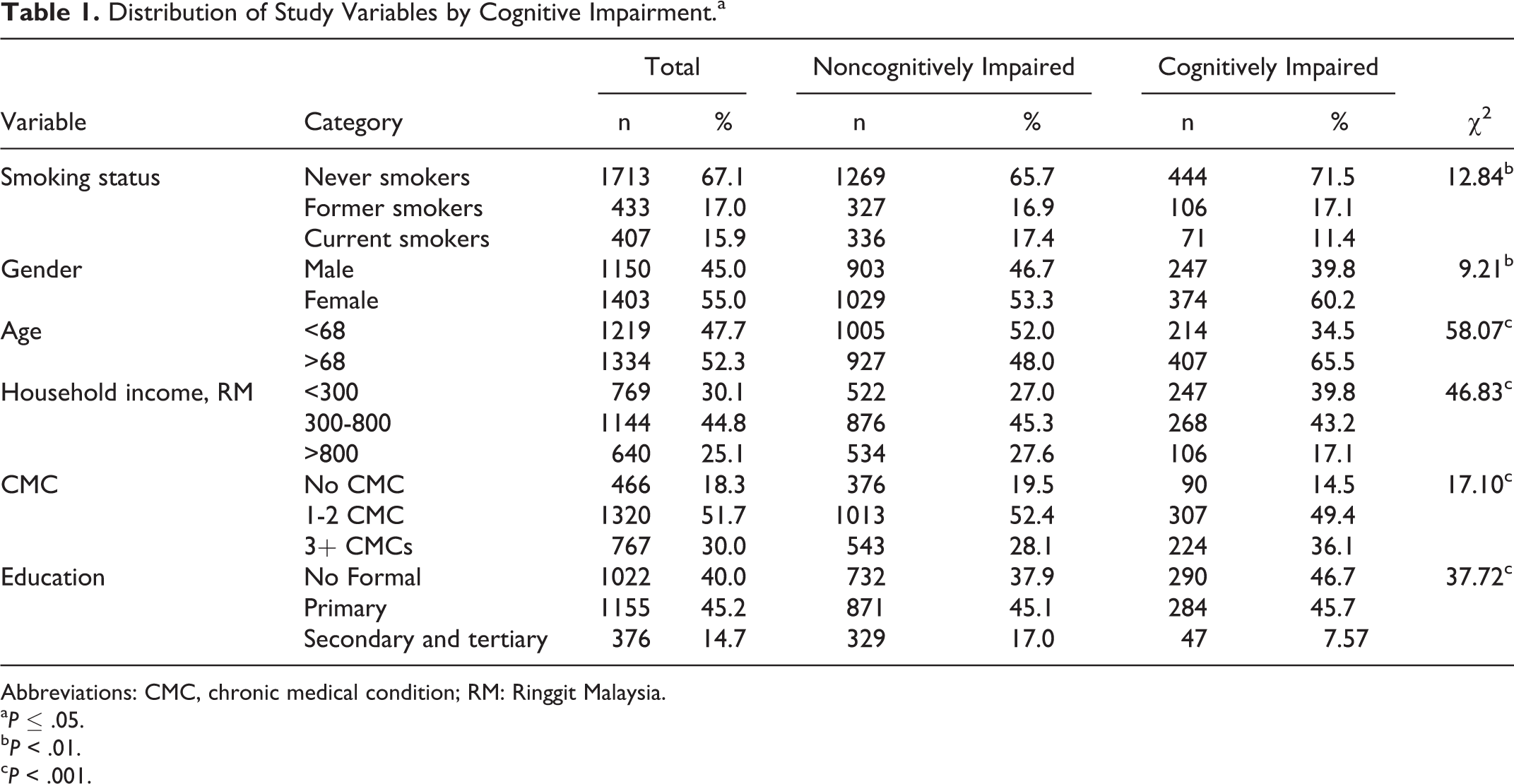
Abbreviations: CMC, chronic medical condition; RM: Ringgit Malaysia.
a P ≤ .05.
b P < .01.
c P < .001.
The results of chi-square analyses presented in Table 1 showed significant association between cognitive impairment with smoking status (χ2 = 12.84, P < .001), gender (χ2 = 9.21, P < .01), age (χ2 = 58.07, P < .001), household income (χ2 = 46.83, P < .001), CMCs (χ2 = 17.10, P < .001), and educational attainment (χ2 = 37.72, P < .001).
A series of chi-square analyses were also performed to examine the relationships between the sociodemographic variables and smoking status (see Table 2). The findings revealed significant associations between smoking status, gender (χ2 = 742.58, P < .001), marital status (χ2 = 97.99, P < .001), household income (χ2 = 24.20, P < .001), CMCs (χ2 = 27.38, P < .001), and educational attainment (χ2 = 36.81, P < .001).
Distribution of Study Variables by Smoking Status.a,b
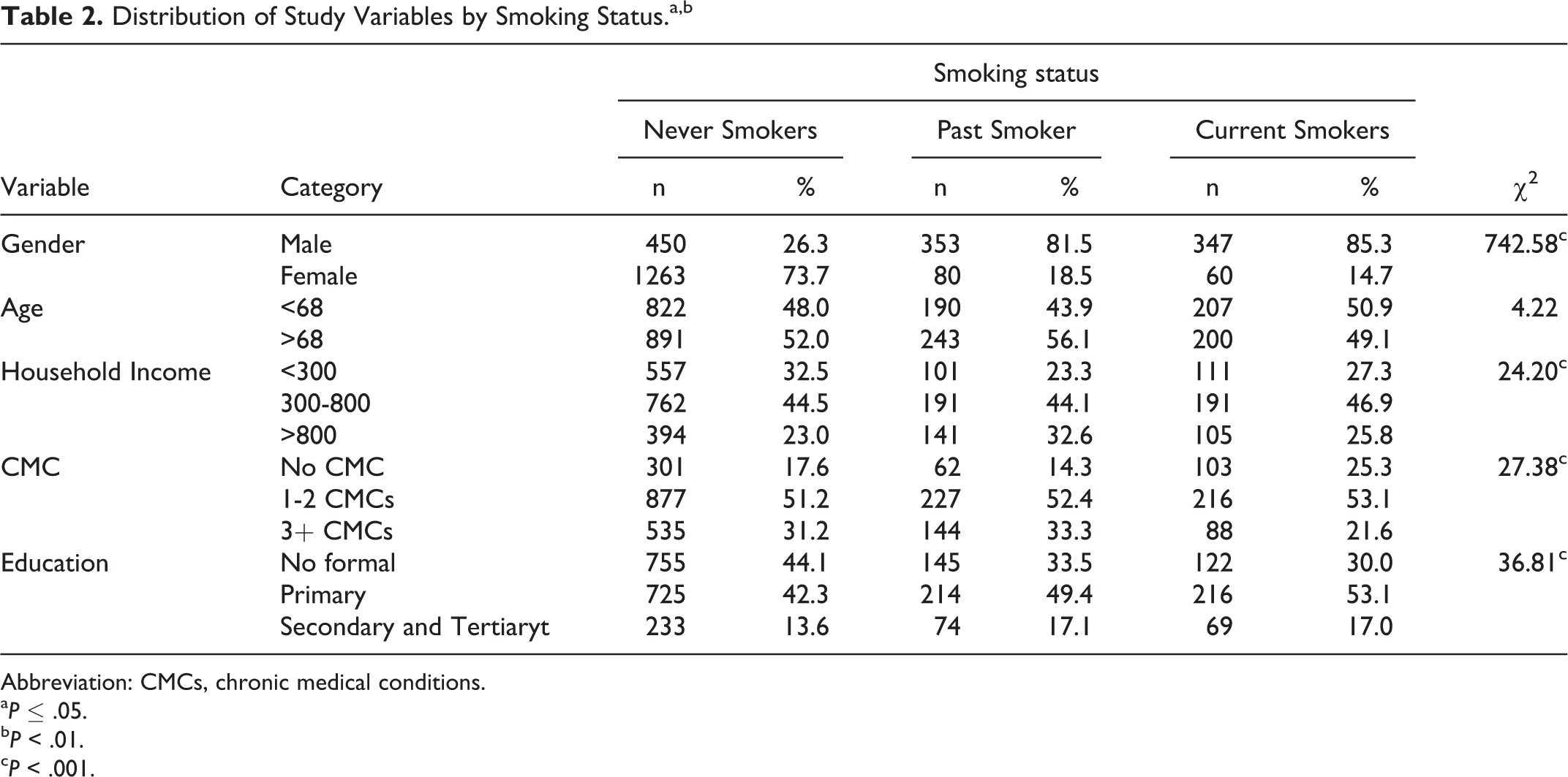
Abbreviation: CMCs, chronic medical conditions.
a P ≤ .05.
b P < .01.
c P < .001.
Hierarchical Logistic Regression
The first block (smoking history) was significant according to the model chi-square statistics. Current smokers had a lower risk of cognitive impairment than never smokers (odds ratio [OR] = .60; 95% confidence interval [CI], .46-.80). The findings from block 2 also revealed a significant model where smoking status remained a significant factor that contributed toward cognitive impairment at P = .01 while controlling for potential confounders such as age, gender, educational attainment, household income, and chronic medical conditions. Table 3 showed that there are no significant difference between former smokers and never smokers (OR = .94, 95% CI: 0.71-1.25).
Summary of Hierarchical Logistic Regression Model.
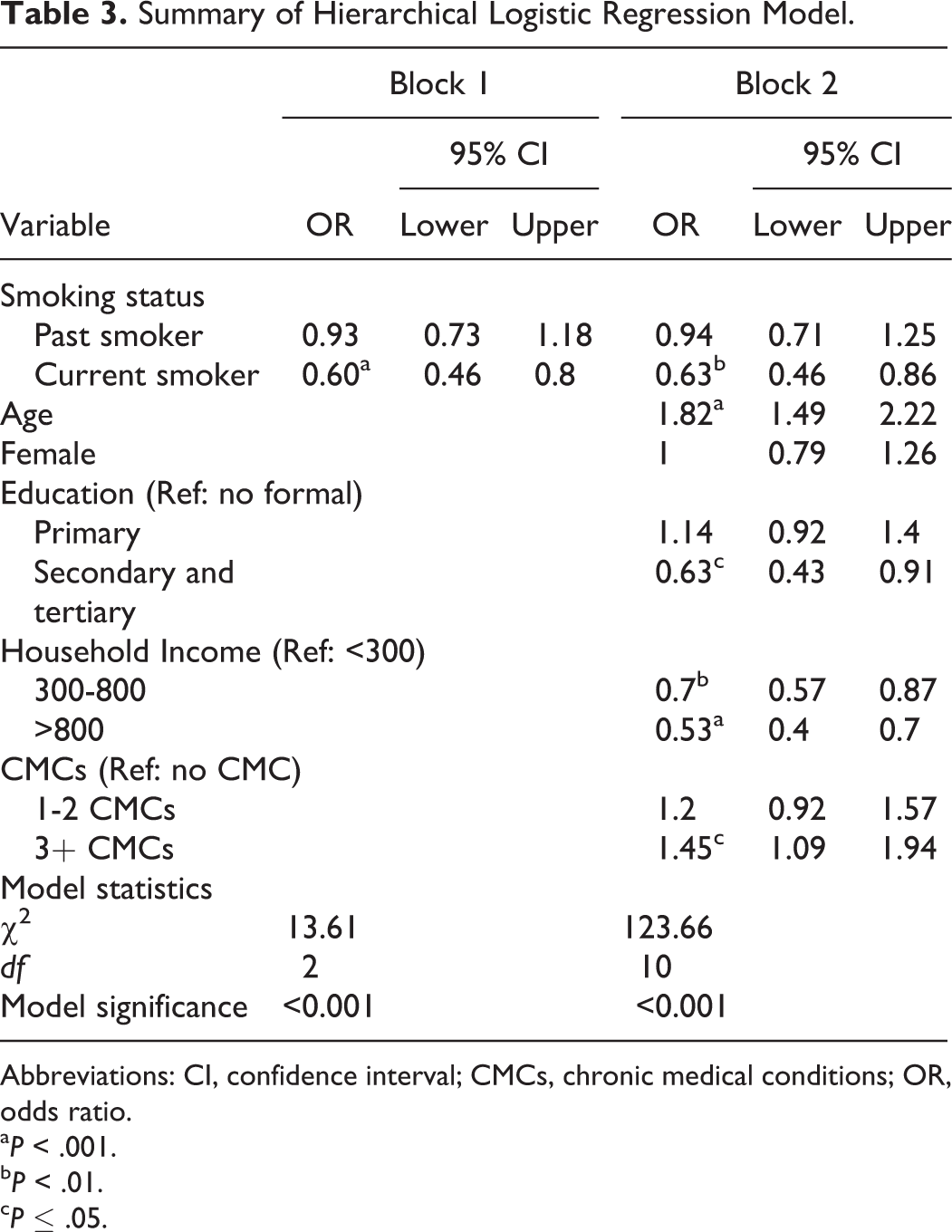
Abbreviations: CI, confidence interval; CMCs, chronic medical conditions; OR, odds ratio.
a P < .001.
b P < .01.
c P ≤ .05.
Discussion
The prevalence of cigarette smoking among older Malaysians aged 60 years and older in the present study was found to be 15.9% (30.2% among males and 4.3% among females), similar to the national prevalence rate of smoking among older adults. 22 The study provided evidence of a lower rate of current smoker status among cognitively impaired respondents compared to the respondents without cognitive impairment (11.1% vs 17%).
The main purpose of this cross-sectional study was to examine the association between smoking and cognitive function. Consistent with previous studies of similar research design, 18,23 we found an inverse relationship between smoking and cognitive impairment. The findings are inconsistent with a growing body of empirical evidence, particularly from longitudinal studies, which showed smoking increases the odds of cognitive impairment. 16,24 -29
The finding that showed no significant difference in cognitive function between former smokers and never smokers was consistent with several past studies. 28,30 However, there are other studies which linked smoking history to cognitive function and found that former smokers have better cognitive scores than never smokers. 18,31,32 For example, the findings from a prospective study among older Taiwanese respondent indicated that former smokers had a lower risk of cognitive impairment compared to never smokers, after controlling for age, education, diabetes, hypertension, stroke, and heart disease. 18 Conversely, the results of other studies provided evidence to the contrary where former smokers have a higher rate of cognitive decline. 16,29,33
Although the exact mechanisms by which cigarette smoking contributes to dementia have not yet been completely understood, it is believed that smoking damages the cardiovascular system and causes oxidative stress, the conditions that may increase the risk of dementia and AD. Smoking can increase the risk of AD and dementia through the cardiovascular system. 29 There was evidence that smoking is also a risk factor for hypertension. 34,35 It was found that hypertension is associated with an increased risk of Alzheimer’s disease and dementia through cerebrovascular pathology and Alzheimer’s disease pathology. 16,17,36
Oxidative stress is another mechanism that may explain the negative effect of smoking on cognitive function. Oxidative stress caused by cigarette smoking damages cells in the blood vessels and results in narrowing of the arteries and reducing cerebral blood flow. Consequently, reduced cerebral perfusion may account for cognitive impairment. 24,26 Recent studies showed that oxidative stress plays a significant role in the onset and development of Alzheimer’s disease. 37 -39
Another possible mechanism that may account for the contribution of smoking to cognitive function is through lifestyle factors. Studies have shown that cigarette smoking is associated with increased consumption of alcohol, 40,41 unhealthy body mass index, 42,43 and low physical activity, 44,45 conditions that are considered as leading causes of cognitive impairment. 46,47 Nonphysiological mechanism may also explain the association between cigarettes smoking and cognitive impairment. First, population-based studies have found an inverse association between socioeconomic status (SES) and smoking behavior, whereas people with lower SES are more likely to become smokers. 48,49 Second, several studies have shown that socioeconomic factors may have a role in dementia etiology. 50 -52 Therefore, the link between low SES and smoking habits may partly explain why smokers may be at greater risk of cognitive impairment.
In contrast, the potential biological protective effects of smoking on dementia has been attributed to nicotine. 53,54 Nicotine can improve short-term cognitive performance and inhibits amyloid formation. 16 It stimulates receptors in the brain that are important for thinking and memory. 55,56 Another explanation for negative association between cigarette smoking and cognitive impairment could be owing to the fact that cigarette smokers die at younger ages than nonsmokers, thus creating a survivorship bias. Consequently, fewer smokers are alive at the ages when dementia symptoms typically onset. 57 Therefore, lower rates of dementia among smokers may have little or nothing to do with any protective quality of smoking and actually be attributable to smokers dying early from other diseases before the onset of dementia. 58 For example, in their study, Sabia and colleagues examined whether the smoking–cognition association is underestimated owing to premature mortality among smokers and found that current smokers had a higher risk of dying during follow-up compared to never smokers, after controlling for age, socioeconomic status, and marital status among men and women. 57
Although, our study benefits from a large representative sample of Malaysian older adults 60 years and older, its cross-sectional nature limits causal conclusions. Another important limitation that should be highlighted is that smoking assessment was solely based on self-report. Some studies indicate that respondents tend to underreport socially undesirable behaviors, such as tobacco use, which may result in the underestimation of the association between smoking and cognitive function. The last limitation that should be acknowledged is related to the use of MMSE. Although the MMSE is widely used as an effective screening instrument for cognitive impairment, it relies heavily on the verbal response, reading, and writing. Therefore, nonformal educated respondents may perform poorly in spite of being cognitively intact. 59
Conclusion
The findings from the present cross-sectional research are in accordance with some previous studies which showed that cigarette smoking may be associated with a lower risk of cognitive impairment. It should be acknowledged that from the present study, we are unable to conclude whether the negative association between cigarette smoking and cognitive impairment is causal or due to other unmeasured confounding factors that require further study to identify the biopsychosocial mechanisms linking cigarette smoking to cognitive function.
Footnotes
Acknowledgments
The authors are thankful to the participants in the study, editor, and anonymous reviewers.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Science, Technology and Innovation which funded the research project (IRPA 06-02-04-0461PR0031).