
Abstract
This study utilized data from the Framingham Heart Study Offspring Cohort to examine the relationship between midlife and late-life alcohol consumption, cognitive functioning, and regional brain volumes among older adults without dementia or a history of abusing alcohol. The results from multiple linear regression models indicate that late life, but not midlife, alcohol consumption status is associated with episodic memory and hippocampal volume. Compared to late life abstainers, moderate consumers had larger hippocampal volume, and light consumers had higher episodic memory. The differences in episodic memory according to late life alcohol consumption status were no longer significant when hippocampal volume was included in the regression model. The findings from this study provide new evidence that hippocampal volume may contribute to the observed differences in episodic memory among older adults and late life alcohol consumption status.
Introduction
Light and moderate alcohol consumption during late life is associated with higher cognitive functioning among older adults 1 and a decreased risk of dementia. 2 Similar findings have been reported from prospective studies that have examined midlife alcohol consumption and cognitive functioning during old age. 3 Several explanations have been proposed for the observed benefits of moderate alcohol consumption for cognitive functioning later in life. Light and moderate alcohol consumption is associated with higher educational attainment 4 and lower prevalence of risk factors for dementia, such as cardiovascular disease 5 and stroke. 6 In the current study, we hypothesized that another mechanism that may explain the observed relationship between alcohol consumption and cognitive functioning is that light to moderate alcohol consumption contributes to preserved regional brain volumes, specifically the hippocampus, and frontal, temporal, and parietal lobes, which are important brain regions underlying memory and cognition.
The hippocampus is located in the medial temporal lobe of the brain and is a critical brain region for memory. 7 Hippocampal atrophy is a characteristic of patients diagnosed with Alzheimer’s disease, 8 and larger hippocampal volume is associated with better memory performance. 9 However, nonsignificant findings for a relationship between hippocampal volume and memory have been reported, 10 indicating that brain regions other than the hippocampus, such as the frontal, parietal, and temporal lobes, contribute to memory and overall cognitive function. The frontal lobe is located in the front of each cerebral hemisphere and is responsible for a number of complex cognitive tasks and behaviors including language, planning, decision making, attention, executive functioning, and goal directed behavior. 11 Frontal lobe atrophy is a characteristic of frontotemporal dementia (FTD), and clinical symptoms of FTD include impulsive behavior and deficits in language, decision making, and motor control. 12 The parietal lobe is the region of the brain posterior to the central sulcus and is involved primarily in tactile perception, 13 spatial orientation, 14 and visual perception. 15 Interestingly, there is evidence from neuroimaging studies that the parietal lobe is activated when performing memory tasks 16,17 and people with parietal lobe damage can present with impaired working 18 and episodic memory. 19 The temporal lobe is below the lateral fissure of the brain, and several brain structures involved in memory, in addition to the hippocampus, are located in the temporal lobe. 20 -22
Although the potential benefits of light to moderate consumption to cognitive functioning later in life have been consistently reported, prolonged periods of abusing alcohol, often defined as consuming 5 or more alcoholic beverages during a single drinking occasion, 23,24 is known to be harmful to the brain. 25 Wernicke-Korsakoff syndrome is a type of dementia that occurs disproportionately among adults with a history of abusing alcohol. 26 The dangerous effects of chronic alcohol abuse on the brain are well established, and previous studies have reported alcohol consumption during old age is associated with decreased total brain volume 27,28 and increased ventricular volume. 29 However, in a cross-sectional study of older adults between 60 and 90 years of age who did not abuse alcohol, investigators reported that as alcohol consumption increased, hippocampal and amygdala volumes also increased. 30 These findings suggest that alcohol consumption may contribute to preserved brain volumes in specific regions of the brain.
Previous studies that have examined the relationship between alcohol consumption and brain volume are limited in scope because alcohol consumption was assessed during only midlife or late life, and cognitive functioning was either not examined or not included in any analyses. Conversely, previous studies have not taken into account the brain volume when examining the relationship between alcohol consumption and cognition among older adults. The current study will address these limitations by using data from the Framingham Heart Study (FHS) Offspring Cohort to examine the relationship between midlife and late life alcohol consumption, regional brain volumes, and cognitive functioning among nondemented older adults who do not have a history of abusing alcohol.
Methods
Sample Population
This study utilized a cross-sectional design and was a secondary analysis of data collected from patients of the FHS Offspring Cohort. 31 The FHS Offspring Cohort was initiated in 1971, and a total of 8 clinical examinations have been completed between 1971 and 2008. Beginning in 1999, patients who were actively participating in the FHS Offspring Cohort were recruited to participate in a secondary study in which they received a comprehensive neuropsychological battery and magnetic resonance image (MRI) of the brain. 32 A total of 864 patients who were 60 years of age or older and absent of stroke, Alzheimer’s disease, or other type of dementia received the FHS neuropsychological battery and MRI of the brain. Patients who did not receive an MRI and neuropsychological battery within a 6-month period (n = 2), did not have data for apolipoprotein E (APOE) genotype (n = 121), or who had a reported history of consuming 5 or more drinks on an almost daily basis (n = 79; see Assessment of alcohol consumption section) were removed from the final sample, which consisted of 664 patients. The average ages of the final sample during the first and eighth clinical examinations were 41.8 and 74.7 years, respectively.
Assessment of Alcohol Consumption
Alcohol consumption was assessed during the first (representing midlife) and eighth (representing late life) clinical examinations using 3 open-ended questions that were administered as part of a medical history interview. (1) During the past year, how many 12-ounce bottles, cans, or glasses of beer did you consume per week? (2) During the past year, how many 4-ounce glasses of wine did you consume per week? and (3) During the past year, how many cocktails (ie, drinks containing 1 to 1.5 ounces of liquor) did you consume per week? There is evidence that using separate questions to assess the consumption of beer, wine, and liquor reduces the risk of underreporting the amount of alcohol consumed by the patients 33 and is a commonly used approach in studies that include self-reported measures of alcohol consumption. 34,35
Midlife and late life alcohol consumption was determined by summing the amounts of beer, wine, and liquor consumed per week as reported by patients during the first and eighth clinical examinations. This was done to limit the number of comparisons made between alcohol consumption categories and because we were interested in studying the number of alcoholic beverages consumed as opposed to beverage type. Patients were grouped into the following classifications to define midlife and late life alcohol consumption status: (1) abstainer, 0 drinks per week; (2) light, 1 to 6 drinks per week; (3) moderate, 7 to 14 drinks per week; and (4) heavy, 15 to 34 drinks per week. As part of the medical history interview administered during the eighth clinical examination, patients were asked: “has there ever been a time in your life when you drank five or more alcoholic drinks of any kind almost daily?” For the purposes of this study, patients who responded yes to this question were said to have a history of abusing alcohol. This definition of a history of abusing alcohol is consistent with previous studies that have studied alcohol abuse. 36 A total of 66 patients reported having ever consumed 5 or more alcoholic beverages on an almost daily basis. This measure was validated by cross-referencing the responses to the alcohol abuse question with the reported number of alcoholic beverages consumed during the first and eighth clinical examinations. An additional 13 patients who responded no to the alcohol abuse question reported drinking 35 or more alcoholic beverages per week during the first clinical examination and were identified as having a history of abusing alcohol. There were 0 patient who responded no to the alcohol abuse question but who consumed 35 or more alcoholic beverages per week during the eighth clinical examination. Patients (n = 79) who were identified as having a history of abusing alcohol were excluded from the final sample. These patients were younger upon receiving the FHS neuropsychological battery (P = .02), were more likely to be male (P < .01), be a current or former smoker during midlife (P < .01) and late life (P < .01), and were less likely to have a college degree (P = .01) compared to patients who did not have evidence for a history of abusing alcohol.
Assessment of Cognitive Functioning
A detailed description of the cognitive assessments included in the FHS neuropsychological battery and the methods of data collection have been previously described. 32,37 Briefly, the neuropsychological battery includes assessments that assess the following cognitive domains: (1) language (Boston Naming Test 38 ); (2) simple and complex attention (Trail Making Test [TMT] A and B 39 ); (3) visuoperceptual skills (Hooper Visual Organization Test 40 ); (4) motor speed (Finger Tapping Test 41 ); (5) premorbid intelligence (Wide Range Achievement Test [WRAT]-3 Reading 42 ); (6) subtests of the Wechsler Memory Scale 43 that assess verbal memory (Logical Memory Immediate and Delayed Recall), learning (Paired-Associate Memory Immediate and Delayed Recall), and visual memory (Visual Reproductions Immediate and Delayed Recall); and (7) abstract reasoning (Similarities 44 ). The TMT A and B are timed assessments that require a participant to connect a random alphabetic sequence (TMT A) and alphanumeric sequence (TMT B). A longer amount of time to complete these assessments indicates lower cognitive performance. An additional cognitive measure was obtained by subtracting the time to complete the TMT B minus the time to complete the TMT A (TMT B − A). This difference score accounts for the motor speed and visual scanning components of the TMT A and TMT B and has been shown to provide a reliable measure of executive function. 45
The outcome measures for cognitive functioning were 3 composite scores that represented episodic memory, executive functioning, and global cognition, respectively. The composite scores were calculated for each patient by first transforming the raw score of each assessment into a z score by subtracting an individual patient’s score minus the sample mean and dividing by the standard deviation. The z scores for TMT A, TMT B, and TMT B − A were multiplied by −1 so that a higher score reflected better cognitive functioning. The composite score for episodic memory was the average of the z scores for Logical Memory Delayed Recall, Paired Associates Delayed Recall, and Visual Recognition Delayed Recall. The composite score for executive functioning was the average of the z scores for TMT A, TMT B, and TMT B − A. The global cognition composite score was obtained by calculating the average of all the z scores with the exception of the Finger Tapping Test, which is a measure of motor speed, 46 and WRAT-3, which was included as a covariate (see Covariates section).
Assessment of Regional Brain Volumes
The methods used to obtain volumetric measures of the frontal lobe and hippocampus from participants of the FHS Offspring Cohort have been described elsewhere. 32,47,48 Briefly, patients received an MRI at the MetroWest Imaging Center in Framingham Massachusetts using a Siemens Magnetom 1-T field strength magnetic resonance machine using a T2-weighted double spin-echo coronal imaging sequence of 4 mm contiguous slices from nasion to occiput with a repetition time of 2420 ms, echo time (TE) of TE1 20/TE2 90 ms, echo train length of 8 ms, field of view of 22 cm, and an acquisition matrix of 182 × 256 interpolated to a 256 × 256 with 1 excitation. 47,48 The MRI data were sent to the University of California Davis (UCD), where images were analyzed on QUANTA 2, a custom-designed image analysis package operating on a Sun Microsystems Ultra 5 workstation. 47 Investigators were blind to any identifying information of the patients. Images were evaluated using a semiautomatic method in which nonbrain elements were removed manually by tracing the dura matter within the cranial vault. 49 Regional brain volumes for frontal, temporal, and parietal lobes, and hippocampus, were defined as follows. 49,50 Frontal lobe volume was determined by tracing all supratemporal brain regions in front of the aqueduct of Sylvius. Temporal lobe volume was obtained by tracing the anterior pole of the temporal lobe to the aqueduct of Sylvius. The parietal lobe was defined as all brain regions behind the aqueduct Sylvius and extending to the medial transverse fissure of the striate cortex. Hippocampal volume was obtained by analyzing the temporal horns of the lateral ventricles. Once the data were interpreted and regional brain volumes had been recorded, the data were sent from UCD to the FHS data management team in Framingham Massachusetts.
Covariates
Covariates obtained during the first and eighth clinical examinations included gender and smoking status. Smoking status was recorded during the first clinical examination as current smoker, never smoker, or former smoker. Smoking status was recorded during the eighth clinical examination as current smoker or nonsmoker. Educational attainment was assessed during the neuropsychological battery and was defined as less than high school, high school degree, some college, or college degree. The WRAT-3 performance was also included as a covariate in all regression models because this assessment provides an indicator of educational quality, which may not be accurately reflected by years of education. 51 Additional covariates that were included were age (in years) upon receiving the neuropsychological battery and APOE e4 allele status (e4+ or e4−). The APOE e4 allele is a widely accepted genetic risk factor for Alzheimer’s disease 52 and is also associated with brain atrophy. 53 Also, patients attended the eighth clinical examination an average of 6 years (range 1.5-8 years) after receiving the neuropsychological battery and MRI. Therefore, time (in years) between receiving the neuropsychological battery/MRI and attending the eighth clinical examination was included as a covariate in all regression models for late life alcohol consumption. Finally, total brain volume was included as a covariate in the multiple linear regression models that examined the relationship between alcohol consumption and regional brain volumes.
Statistical Analysis
Differences for age, gender, smoking, educational attainment, and APOE e4 allele status according to alcohol consumption status during midlife and late life were determined using analysis of variance for continuous variables and chi-square test for categorical variables. Hippocampal volume, frontal lobe volume, and cognitive functioning were the outcomes of interest in separate multiple linear regression models. Midlife and late life alcohol consumption was examined in separate multiple regression models. The models that examined the effects of midlife alcohol consumption controlled for age, gender, educational attainment, smoking status during midlife, WRAT-3 performance, and APOE e4 allele status. Total brain volume was included as a covariate when the outcome was hippocampal volume or frontal lobe volume. The models that examined the effects of late life alcohol consumption controlled for age, gender, educational attainment, smoking status during late life, WRAT-3 performance, number of years between receiving the neuropsychological battery/MRI and eighth clinical examination, and APOE e4 allele status. Total brain volume was included as covariate when the outcome was hippocampal volume or frontal lobe volume. A gender by alcohol consumption interaction term was included to account for potential differences for the effects of alcohol consumption for men and women. An interaction term between APOE and alcohol consumption was also included to determine whether the effects of alcohol consumption on cognition and brain volumes differed according to APOE e4 allele status.
Results
Sample Characteristics
The descriptive characteristics of the final sample according to midlife and late life alcohol consumption status are provided in Table 1. Of the 664 patients included in the final sample, 12 (1.8%) patients carried 2 APOE e4 alleles, 133 (20.0%) carried 1 APOE e4 allele, and 519 (78.2%) did not carry any APOE e4 alleles. During midlife, there were 72 (10.8%) abstainers, 363 (54.7%) light, 163 (24.5%) moderate, and 66 (9.9%) heavy alcohol consumers. The result of a paired t test indicated that there was a decrease in the average number of drinks consumed per week from midlife to late life (6.0 vs 3.8 drinks/wk; P < .01). There were 348 (52.4%) abstainers, 133 (20.0%) light, 152 (22.9%) moderate, and 31 (4.7%) heavy alcohol consumers during late life. Men were more likely to be heavy alcohol consumers compared to women during midlife (P < .01) and late life (P < .01). Late life abstainers were older compared to light (P < .01) and moderate (P = .02) alcohol consumers. Patients who were abstainers during late life were less likely to have more than a high school degree (P < .01) and were less likely to have been a current or former smoker during midlife (P < .01). In addition, there were significant differences in WRAT-3 performance according to midlife (P = .01) and late life (P < .01) alcohol consumption status. Midlife abstainers had significantly lower WRAT-3 performance compared to patients who were moderate (P < .01) or heavy (P = .01) consumers during midlife, whereas late life abstainers had significantly lower WRAT-3 performance compared to patients who were light (P < .01) or moderate (P < .01) alcohol consumers during late life. The significant differences in WRAT-3 performance according to late life, but not midlife, alcohol consumption remained statistically significant after controlling for the effects of educational attainment.
Demographic Characteristics of 664 Patients of the FHS Offspring Cohort According to Midlife and Late Life Alcohol Consumption Status.a,b
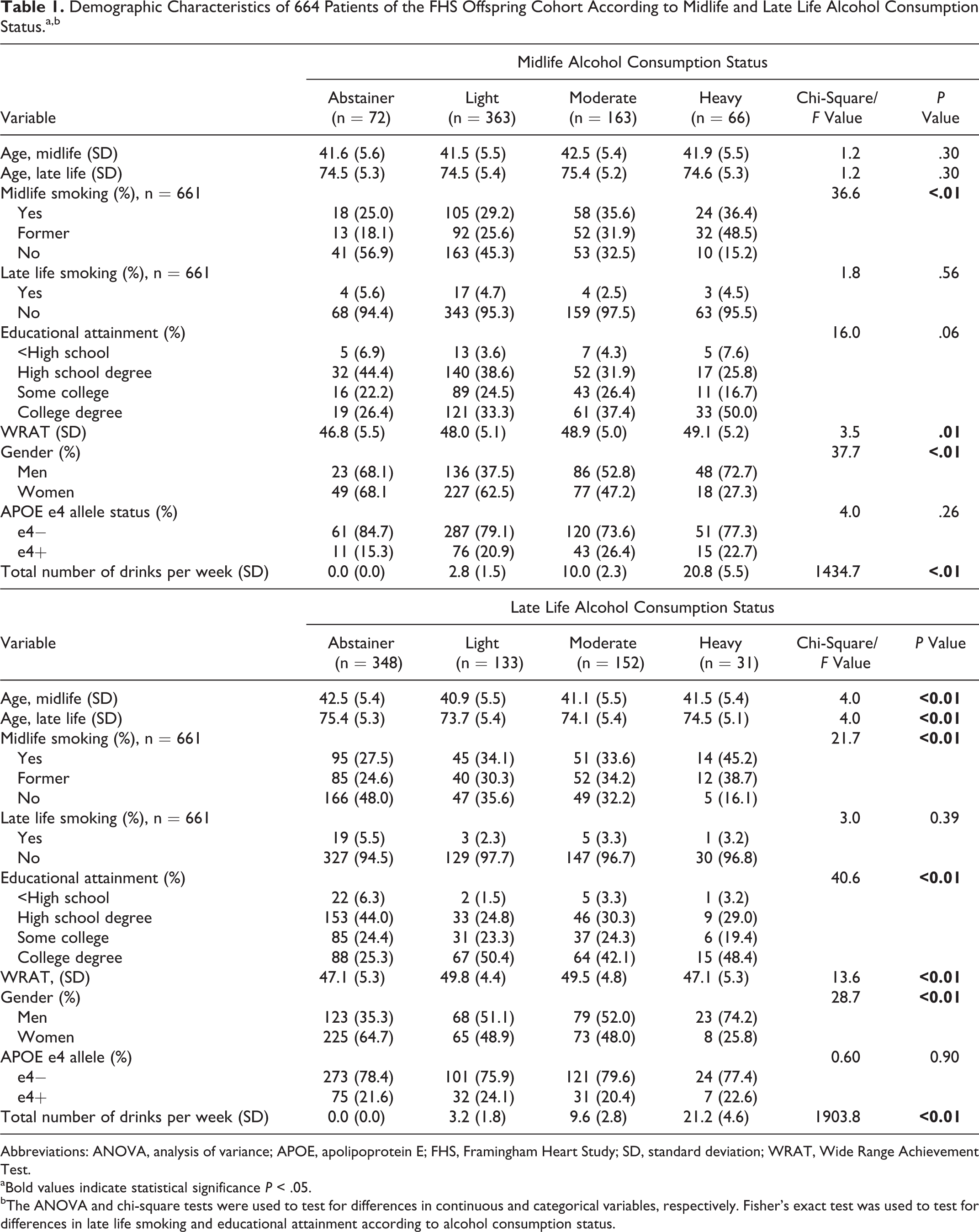
Abbreviations: ANOVA, analysis of variance; APOE, apolipoprotein E; FHS, Framingham Heart Study; SD, standard deviation; WRAT, Wide Range Achievement Test.
aBold values indicate statistical significance P < .05.
bThe ANOVA and chi-square tests were used to test for differences in continuous and categorical variables, respectively. Fisher’s exact test was used to test for differences in late life smoking and educational attainment according to alcohol consumption status.
Alcohol Consumption and Regional Brain Volumes
A summary (mean, standard deviation) of regional brain volumes according to midlife and late life alcohol consumption statuses is provided in Table 2. No significant differences for any regional brain volumes according to midlife alcohol consumption status were detected (Table 3). There were significant differences in hippocampal volume (P = .04), but not for frontal, parietal, or temporal lobe volumes, according to late life alcohol consumption status (Table 3). Specifically, patients who were moderate alcohol consumers during late life had larger hippocampal volume compared to late life abstainers (P = .01). There was evidence that the relationship between late life alcohol consumption and hippocampal volume differed according to APOE e4 allele status. When patients were stratified according to APOE e4 allele status, significant differences in hippocampal volume according to late life alcohol consumption status for patients who were APOE e4− were detected (F value = 4.8; P < .01), but not for patients who were APOE e4+ (F value = 1.9; P = .13). Moderate alcohol consumers who were APOE e4− had larger hippocampal volume compared to abstainers who were APOE e4− (
Mean Brain Volume According to Midlife and Late Life Alcohol Consumption Status.
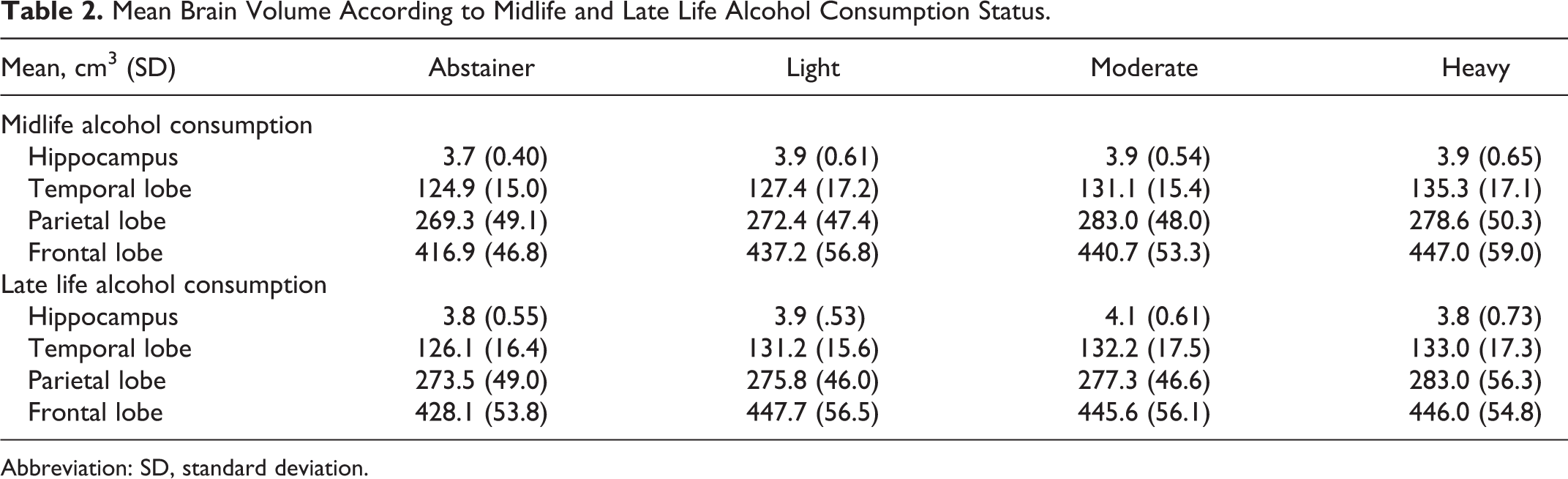
Abbreviation: SD, standard deviation.
Relationship Between Regional Brain Volumes and Alcohol Consumption During Midlife and Late Life.a,b,c
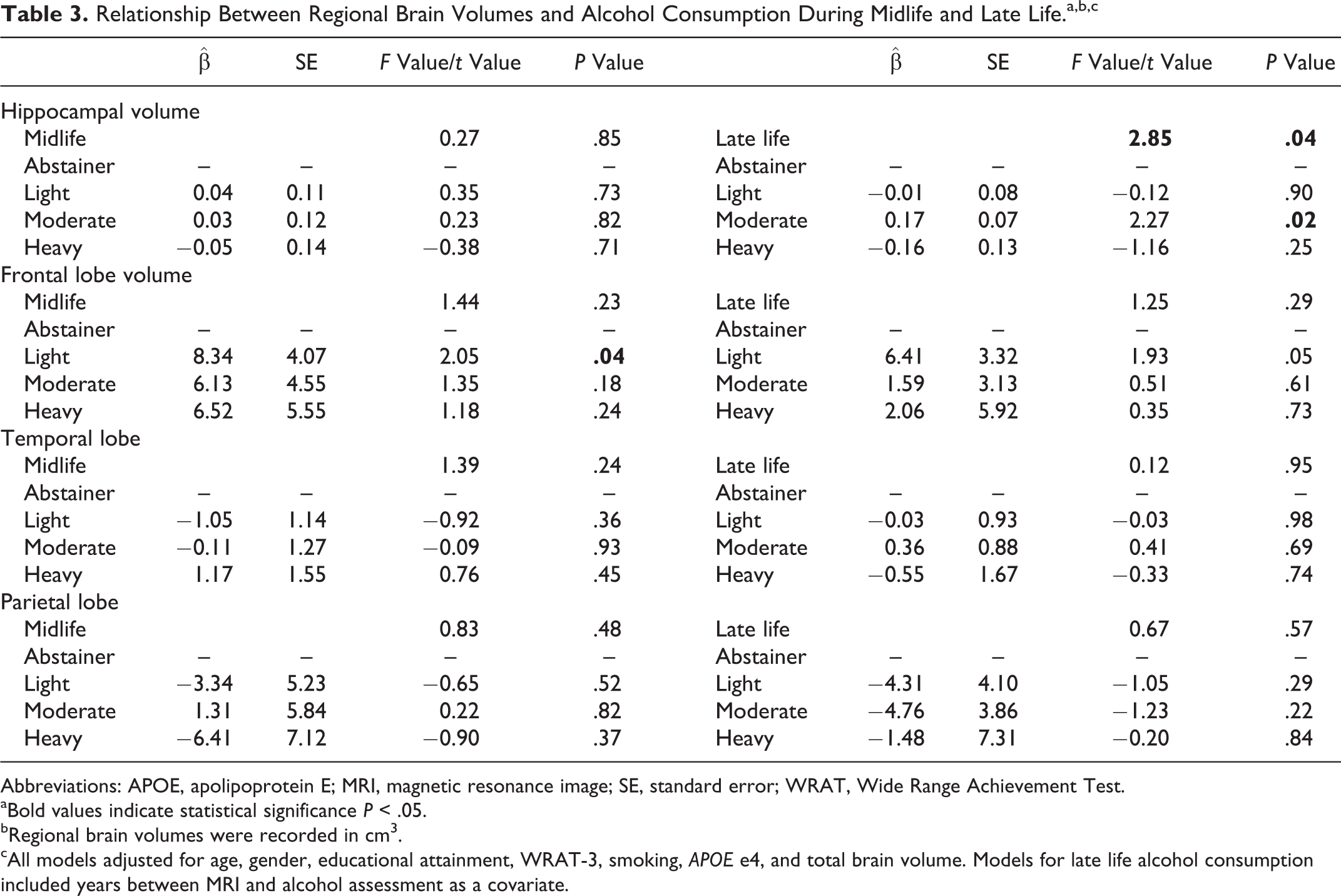
Abbreviations: APOE, apolipoprotein E; MRI, magnetic resonance image; SE, standard error; WRAT, Wide Range Achievement Test.
aBold values indicate statistical significance P < .05.
bRegional brain volumes were recorded in cm 3 .
cAll models adjusted for age, gender, educational attainment, WRAT-3, smoking, APOE e4, and total brain volume. Models for late life alcohol consumption included years between MRI and alcohol assessment as a covariate.
Alcohol Consumption and Cognitive Functioning
There were significant differences in cognitive functioning according to late life, but not midlife, alcohol consumption status (Table 4). Patients who were light alcohol consumers during late life had significantly higher episodic memory compared to late life abstainers, whereas no significant differences between moderate and heavy alcohol consumers were detected compared to abstainers. There were no significant differences in executive functioning or global cognition according to late life alcohol consumption. The relationship between episodic memory and late life alcohol consumption was not modified according to gender or APOE e4 allele status.
Relationship Between Cognitive Functioning and Alcohol Consumption During Midlife and Late Life.a,b
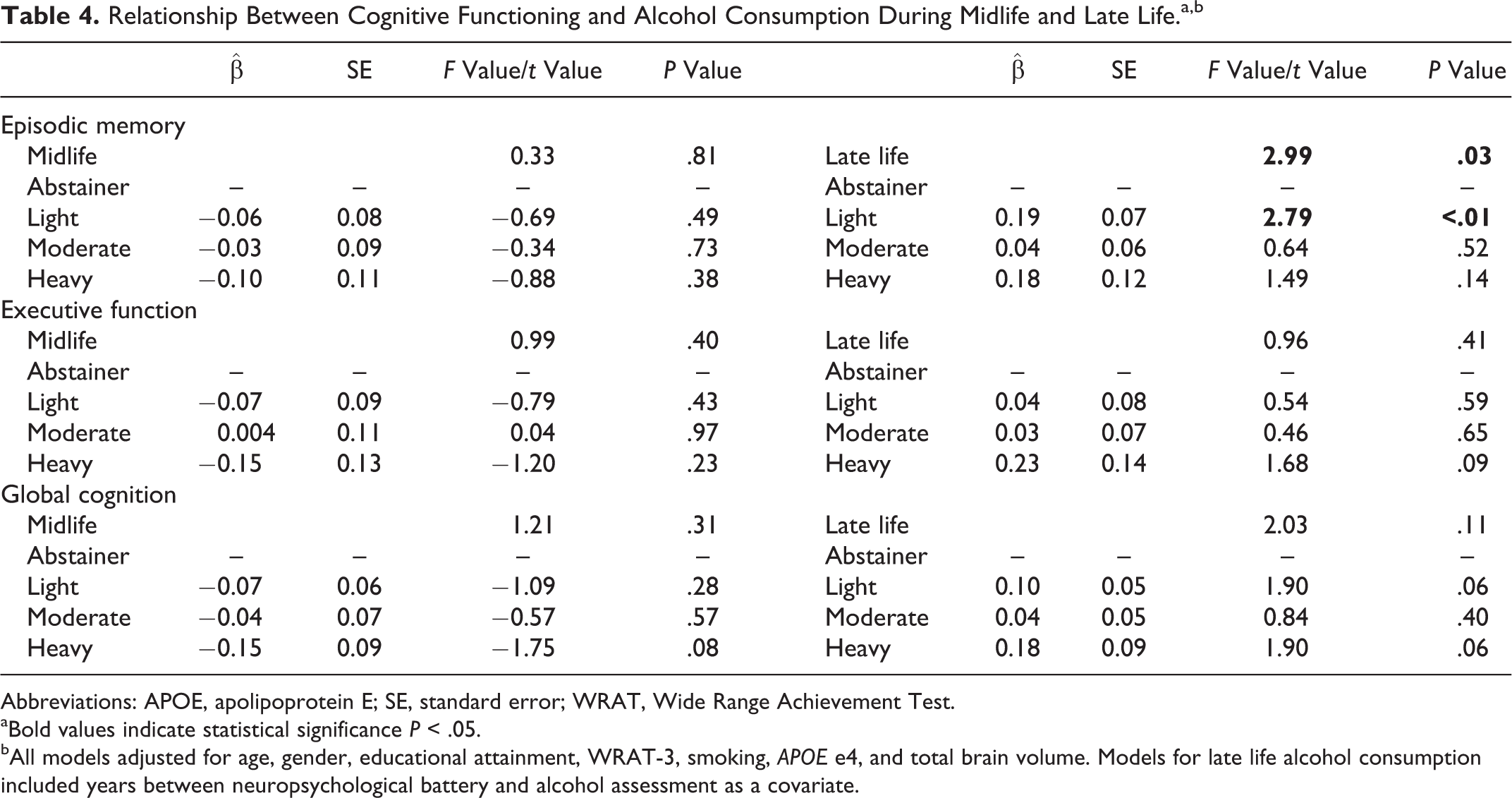
Abbreviations: APOE, apolipoprotein E; SE, standard error; WRAT, Wide Range Achievement Test.
aBold values indicate statistical significance P < .05.
bAll models adjusted for age, gender, educational attainment, WRAT-3, smoking, APOE e4, and total brain volume. Models for late life alcohol consumption included years between neuropsychological battery and alcohol assessment as a covariate.
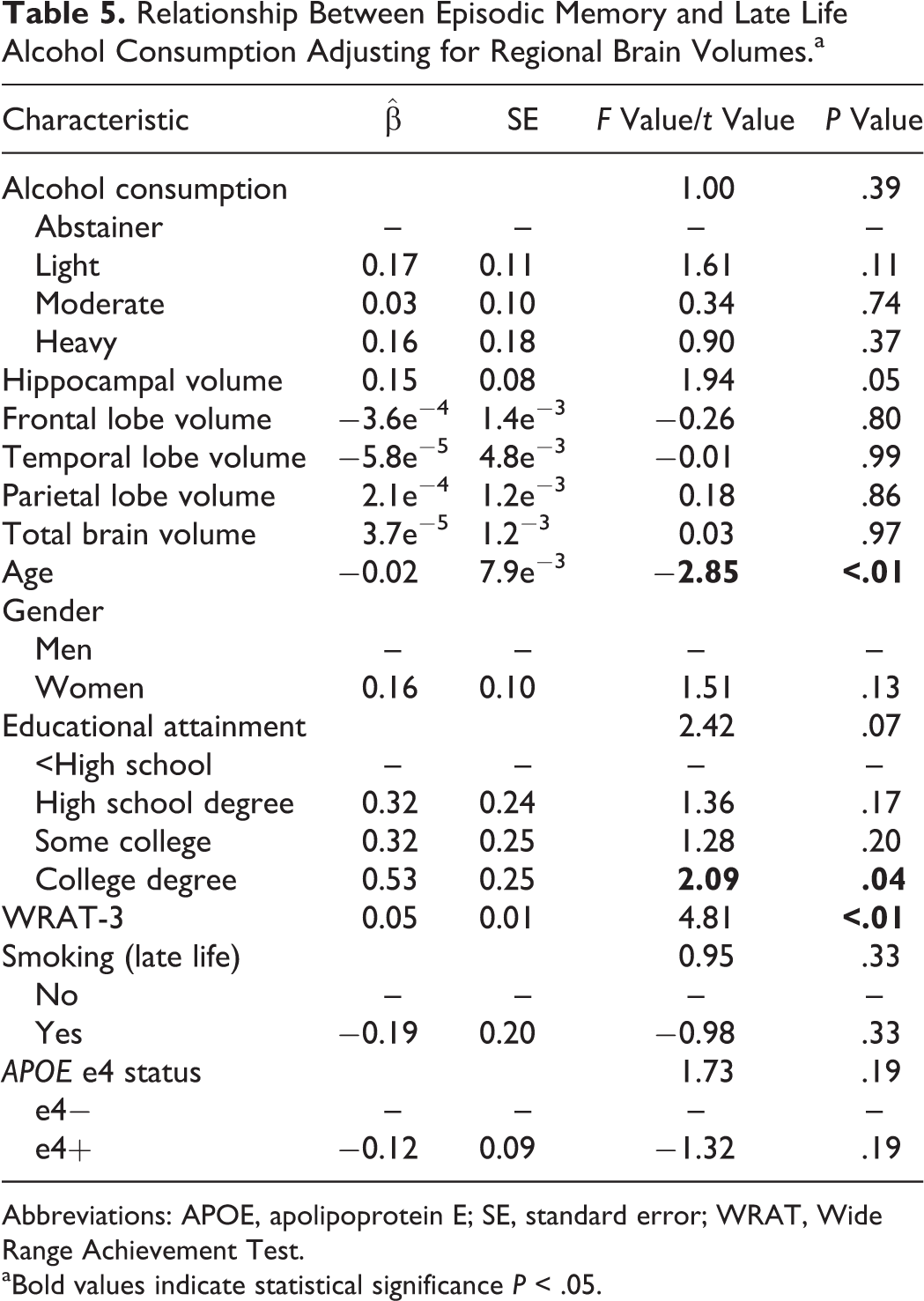
Relationship Between Late Life Alcohol Consumption, Episodic Memory, and Regional Brain Volumes
Regional brain volumes were included in the statistical models that examined the relationship between episodic memory and late life alcohol consumption to determine whether the relationship between late life alcohol consumption status and episodic memory remained statistically significant after controlling for the effects of regional brain volumes. Regional brain volumes were not included in the models that examined cognition and midlife alcohol consumption or late life alcohol consumption and executive function or global cognition because there were no significant differences in cognition according to alcohol consumption status in these models.
Hippocampal volume was the only regional brain volume significantly associated with episodic memory (
Relationship Between Episodic Memory and Late Life Alcohol Consumption Adjusting for Regional Brain Volumes.a
Abbreviations: APOE, apolipoprotein E; SE, standard error; WRAT, Wide Range Achievement Test.
aBold values indicate statistical significance P < .05.
Discussion
The findings from this study provide new evidence that light alcohol consumption during late life is associated with higher episodic memory, but not executive function or global cognition, after controlling for the effects of age, gender, educational attainment, WRAT-3 performance, smoking, APOE e4, and number of years between receiving the neuropsychological battery and eighth clinical examination. Additional factors identified to be associated with higher episodic memory during late life included higher performance on WRAT-3 and younger relative age. Also, older adults who consumed moderate amounts of alcohol had significantly larger hippocampal volume compared to older adults who did not consume alcohol. Finally, the relationship between episodic memory and late life alcohol consumption status was no longer statistically significant once hippocampal volume was included in the model. The findings from animal studies suggest that moderate alcohol consumption may contribute to preserved hippocampal volume by promoting the generation of new neurons in the hippocampus. 54 In addition, exposing the brain to moderate amounts of alcohol may increase the release of acetylcholine and other neurotransmitters that are involved in cognitive functioning. 55
A significant relationship between late life alcohol consumption status and educational attainment was detected. Specifically, patients who were late life abstainers were less likely to have received more than a high school degree. The relationship between lower educational attainment and abstaining from alcohol during late life has been documented 56,57 and is attributed to differences between abstainers and alcohol consumers in social, demographic, and health characteristics such as low socioeconomic status, limited access to health care, and overall poorer health. 58
There were no significant differences in cognitive functioning and regional brain volumes during late life according to midlife alcohol consumption status. This may be due to adults who are able to continue consuming alcohol into old age are healthier, and therefore have higher cognition and larger regional brain volumes, than people who had to decrease their alcohol consumption due to adverse health outcomes and become abstainers during old age. 59,60 There also may be an accumulative effect of alcohol consumption on cognitive functioning and regional brain volumes, meaning a person needs to consume alcohol, but not abuse alcohol, for several years or even decades before differences in cognitive functioning and regional brain volumes are observed. These potential explanations can be assessed by studying longitudinal trajectories of alcohol consumption to determine whether an increase, decrease, or consistent alcohol consumption from midlife to late life is related to cognitive functioning and regional brain volumes during old age.
A significant interaction between late life alcohol consumption and APOE e4 status on hippocampal volume was also detected in the current study. Moderate alcohol consumers during late life who were APOE e4− had larger hippocampal volume compared to abstainers who were APOE e4−, but there were no differences in hippocampal volume according to late life alcohol consumption status among APOE e4+ patients. The observed differences in hippocampal volume according to late life alcohol consumption status among APOE e4− patients are possibly due to the benefits of alcohol consumption on vascular health. Specifically, moderate alcohol consumption has been shown to be protective against atherosclerosis, 61 which has been associated with increased brain atrophy. 62 The lack of significant findings among APOE e4+ patients may be due to the low number of patients who were APOE e4+ and moderate alcohol consumers during late life and warrants further investigation using larger sample populations.
In the current study, higher WRAT-3 performance was associated with higher episodic memory and a relationship between increasing educational attainment and episodic memory approached statistical significance. Both high educational attainment and premorbid intelligence are associated with a decreased risk of dementia. 63 -65 A hypothesis for the decreased risk of dementia among older adults with high educational attainment and premorbid intelligence is these older adults may have greater levels of cognitive reserve, which allows them to withstand more brain pathology before cognitive deficits can be detected, compared to older adults with low education or premorbid intelligence. 64,66,67 Cognitive reserve is the ability to actively engage additional neural networks when performing a cognitive task 67 and is a plausible explanation for why older adults with high educational attainment are able to withstand greater accumulation of brain pathology before cognitive deficits are observed. 68,69 The benefits of educational attainment for cognitive reserve are supported by evidence that older adults with higher educational attainment activate additional regions of the brain when performing cognitive tasks compared to older adults with less educational attainment. 70,71 A study conducted by Cooper et al 72 reported that the relationship between moderate alcohol consumption and decreased risk of cognitive decline among older adults is due to higher premorbid intelligence among moderate alcohol consumers, and the authors suggest that higher cognitive reserve may explain the frequently reported benefits of alcohol consumption toward cognition among older adults. Our findings, however, provide evidence that factors in addition to premorbid intelligence and high educational attainment contribute to the larger hippocampal volume and higher episodic memory among older adults who are light and moderate alcohol consumers in the FHS Offspring Cohort.
There are limitations to this study that need to be acknowledged. First, patients included in the final sample may not be representative of the general population. Prolonged heavy alcohol consumption is associated with a higher rate of mortality 73 and older adults who were healthy enough to consume over 14 drinks/wk and still receive the FHS neuropsychological battery and MRI of the brain may have genetic, physiological, health, or other characteristics that make them less susceptible to the negative effects of heavy alcohol consumption, resulting in a healthy survivor effect among adults who consumed between 15 and 35 alcohol drinks per week. 74 This may also be a contributing factor to the observed association between heavy alcohol consumption during late life and high cognitive function. A second potential limitation is that self-reported measures for alcohol consumption and history of abusing alcohol were used to assess midlife and late life alcohol consumption. A limitation of self-reported measures of alcohol consumption is the risk of patients unintentionally or intentionally underreporting of the amount of alcohol typically consumed over a specified period of time. 75 The use of separate questions to assess beer, liquor, and wine consumption to calculate total alcohol consumption, as was done in the current study, has been shown to decrease the risk of underreporting compared to asking patients to recall the total number of drinks they consume without specifying beverage type. 33 There is also the potential for some patients to either not accurately recall or deny they have ever consumed 5 or more drinks at one time on an almost daily basis. This limitation was addressed by comparing the responses to the alcohol abuse question to the reported number of alcohol beverages consumed during the first and eighth clinical examinations. Patients who reported drinking 35 or more alcoholic beverages per week but responded no to the alcohol abuse question were identified as having a history of abusing alcohol. A third potential limitation of this study is the considerable time difference between when patients received the neuropsychological battery and MRI and the assessment of late life alcohol consumption during the eighth clinical examination. Although we controlled for this in all statistical models that included late life alcohol consumption, there is still possibility for reverse causality in which patients with higher cognition and larger regional brain volumes upon receiving the neuropsychological battery and MRI remained healthy enough to continue consuming alcohol. Finally, the current study did not control for hypertension, diabetes, heart disease, depression, and other factors that may confound the relationship between alcohol consumption, cognition, and regional brain volumes. There is evidence that these factors may contribute to poor cognition 76 and brain atrophy, 77,78 including atrophy to the hippocampus 79 -81 during old age. Future research on the relationship between alcohol consumption, regional brain volumes, and cognition that controls for vascular health and mental health is warranted.
In summary, the findings from the current study provide new evidence that late life alcohol consumption is associated with episodic memory and hippocampal volume during old age, but there is insufficient evidence to conclude that midlife alcohol consumption is related to cognitive functioning or regional brain volumes. The inclusion of both regional brain volumes and cognition revealed that the relationship between late life alcohol consumption and episodic memory was no longer statistically significant after hippocampal volume was included in the regression model. This suggests that the observed relationship between alcohol consumption and episodic memory and alcohol consumption during old age may be due to larger hippocampal volume. Future research on the relationship between changes in alcohol consumption with advancing age and cognitive functioning, the effects of alcohol consumption on cognitive reserve, and replication of our findings using larger sample populations can increase the scientific understanding of the relationship between alcohol consumption, regional brain volumes, and cognition during old age.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.