
Abstract
Background:
In older adults with cognitive impairment (CI), decreased functional status and increased behavioral symptoms require relocation from assisted living (AL) to nursing homes. Studies support positive effects of pets on health/function.
Purpose:
Evaluate the effectiveness of the Pet AL (PAL) intervention to support physical, behavioral, and emotional function in AL residents with CI.
Methods:
Cognitively impaired AL residents randomized to 60-90 minute sessions [PAL (n = 22) or reminiscing (n = 18)] twice/week for 12 weeks. PAL interventionist encourages residents to perform skills with the visiting dog; reminiscing interventionist encourages residents to reminisce. Monthly assessment of physical (energy expenditure, activities of daily living), emotional (depression, apathy), and behavioral (agitation) function.
Results:
In linear mixed models, physical activity depressive symptoms improved more with PAL.
Conclusion:
Evidence supports that the PAL program helps preserve/enhance function of AL residents with CI. Additional study is required to evaluate the duration and predictors of effectiveness of the PAL intervention.
Keywords
Introduction
Dementia prevalence in assisted living (AL) ranges from approximately 42% to 67%. 1 -3 Assisted living residents with dementia are more likely to experience greater functional disability and neuropsychiatric symptoms than AL residents without dementia. 4,5 Functional impairment and increased emotional and behavioral symptoms lead to relocation of AL residents to more comprehensive and expensive care situations. 6
Depression is common and underrecognized among AL residents. 7 Approximately 25% of AL residents have significant depressive symptoms, and less than half of them are treated for their depression. 8 -11 Individuals with depression in dementia or cognitive impairment appear to have more motivational symptoms, 12 such as diminished goal-directed behavior and increased apathy, 13 -16 rather than depressed mood and suicidality, which in turn can predict higher levels of functional impairment. 9 Assisted living staff are particularly challenged by identifying and managing depressive symptoms among older adults with dementia or cognitive impairment. 10,17
Additionally, behavioral symptoms, including agitation, are common in AL residents; incidents of behavioral symptoms occur in approximately one-third of the residents each week. 18 Agitated behavioral symptoms further complicate the active involvement of individuals with dementia in functional and physical activities and often result in more rapid functional decline. 19
The majority of AL residents with dementia are inactive and have limited opportunities for physical activity. 20 Much recent research on improving physical function in AL residents with dementia focuses on motivating caregivers to change or modify their interactions when working with AL residents. 21 -23 Changing staff behavior to encourage physical activity in older adults with dementia leads to an improvement in the older adults’ physical performance. 24 -32 In several small randomized controlled trials, structured physical activity interventions in individuals with dementia led to improvements or slower decline in mobility, physical function, balance, muscle strength, mood, and behavior. 27,33 Successful interventions include walking programs, aerobic training, and various combinations of aerobic, resistance, and strength training. Effective physical activity interventions were implemented 2 to 5 times a week over 8 to 16 weeks. 27,34,35
Assisted living residents with cognitive impairment or dementia have several risk factors for functional decline and are likely to have complicating neuropsychiatric symptoms. This patient population can be challenging to engage and motivate to participate in activities of daily living and nonpharmacological interventions are needed that target both the motivational and behavioral symptoms.
The current study examines the use of animal-assisted therapy implemented as the pet-assisted living (PAL) intervention to directly increase physical activity and decrease depression, apathy, and agitation in AL residents with cognitive impairment. The PAL intervention was designed based on the theory of self-efficacy to increase physical function and improve mood and behavior among AL residents. The theory of self-efficacy clarifies and explains motivation for behaviors. 36 It suggests that the stronger the individual’s self-efficacy and outcome expectations, the more likely it is that he or she will initiate and persist with a given activity. Self-efficacy expectations are the individuals’ beliefs in their capabilities to perform a course of action to attain a desired outcome; and outcome expectations are the beliefs that a certain consequence will be produced by personal action. These expectations for physical activity are appraised and enhanced by (1) successful performance of the activity of interest; (2) encouragement that the individual is capable of performing the activity of interest; (3) seeing like individuals perform a specific activity; and (4) physiological and affective states such as pain, fatigue, or anxiety associated with a given activity. 37,38
The PAL intervention is expected to increase the AL resident’s physical activity and performance of functional tasks by performing difficult tasks with a canine visitor. Verbal encouragement, role modeling, mastery experiences, and decreasing unpleasant sensations are all ways in which the AL residents have been motivated to successfully change behavior to enhance function and physical activity. 39,40 The PAL intervention targets increasing motivation for physical activity and activities of daily living with verbal encouragement, role modeling, and mastery experience to encourage residents to perform activities with the dog that may be difficult or uncomfortable. It is anticipated that success in these activities will be generalized to other parts of the residents’ lives.
Social support motivates older adults to perform functional activities and exercise. Social support networks including family, friends, peers, and health care providers are important determinants of behavior, especially physical activity. 41,42 Social interactions influence self-efficacy and outcome expectations and slow the trajectory of functional decline from limitations to disability. Older adults who were more active were also more efficacious and had better physical function and fewer functional limitations. Only higher levels of self-efficacy were associated with less disability. 43
The PAL intervention has a great potential to increase social support for physical activity of AL residents. Companion animals facilitate social behavior and provide important sources of social support for older socially isolated individuals. Many AL facilities and nursing homes use pet visitation programs to enhance social interactions of residents, especially those with dementia. These programs, which generally include a short one-on-one visit from a person accompanied by an animal once or less frequently per week, increase residents’ social interaction. 44 Behavioral studies indicate that visits by a dog and handler increase social interaction in nursing home residents, especially those with dementia. 45 -49
Evidence supports the benefits of companion animals for preventing functional decline and improving health of older adults. A 6-month intervention similar to the PAL was effective at improving mobility, interpersonal contact and communication, activities of daily living, and general well-being of older institutionalized patients with schizophrenia. 50 Among community living older adults, pet owners experienced significantly less decline in physical and mental health and activities of daily living over a 1-year period than nonowners. 51
Previous research documents that dogs assist in motivating physical function and improving emotional and behavioral status in other populations. A unique study of motor skill task completion by preschool children supports the use of dog modeling for functional behaviors. Children completed a time relevant motor task faster when the task was modeled by a dog than by the handler. 52 Dog walking gives purpose to a walking program, providing a motivation for adherence. 53,54
Animal visitation programs have been effective at improving emotional and behavioral function. A meta-analysis of 5 experimental studies, including 4 conducted in nursing homes concluded that animal visits led to decreases in depression. 55 The interventions were both statistically and clinically significant. In 2 subsequent studies of nursing home residents, one of which was of residents with dementia, animal visits were more effective than people visits of equal duration at improving mood. 56,57 In several studies, both resident and visiting dogs reduced agitation of nursing home residents with dementia or cognitive impairment. 46,48,58 In a matched case–control study of nursing home residents with dementia, a 10-week animal intervention resulted in no change in agitation/aggression and depression, while the control intervention resulted in deterioration over the same time period. 59
No known study has examined the effect of structured dog visits on physical activity, mood, and behavior of AL residents with cognitive impairment. Therefore, this study was designed to evaluate the use of structured activities with a dog, the PAL intervention, to prevent deterioration of physical function (energy expenditure and activities of daily living), emotional (depression and apathy) and behavioral (agitation) function in AL residents with mild to moderate cognitive impairment.
Methods
A randomized clinical trial with repeated measures was conducted to examine the effect of the dog-aided functional intervention on emotional, behavioral, and physical function of AL residents with cognitive impairment consistent with mild to moderate dementia over a 3-month period. The 3-month intervention was chosen as a shorter duration that was likely to cause a benefit. 57,60,61 These AL residents were enrolled because this group is difficult to reach with more traditional recreational activities and have been reported to benefit from less structured forms of animal-assisted activities. 45 The study was approved by the institutional review board of the University of Maryland Baltimore and the ethics committee of WALTHAM®.
Sample Size
A prior power analysis for 3 repeated measures with correlations of .32, a medium effect size, α of .05, and power of 0.80 comparing 2 groups suggested a minimum sample size of 34. A sample of 40 was recruited to allow for loss of participants due to attrition or death over the course of the study.
Recruitment
Participants were recruited from 7 AL facilities from December 2010 through December 2012. A member of the AL staff identified residents who might meet the inclusion/exclusion criteria. Inclusion criteria included mild to moderate cognitive impairment (Mini-Mental State Examination [MMSE] score above 8 and below 23), 62,63 age 55 years or older, anticipated length of stay in the AL facility of 6 or more months, English speaking, and with either prior experience with or interest in interacting with a dog. Residents were excluded if they had known allergies to or fear of dogs, a physical illness like asthma that is exacerbated in the presence of a dog, or receiving hospice care, see Figure 1 for a consort diagram for the study.
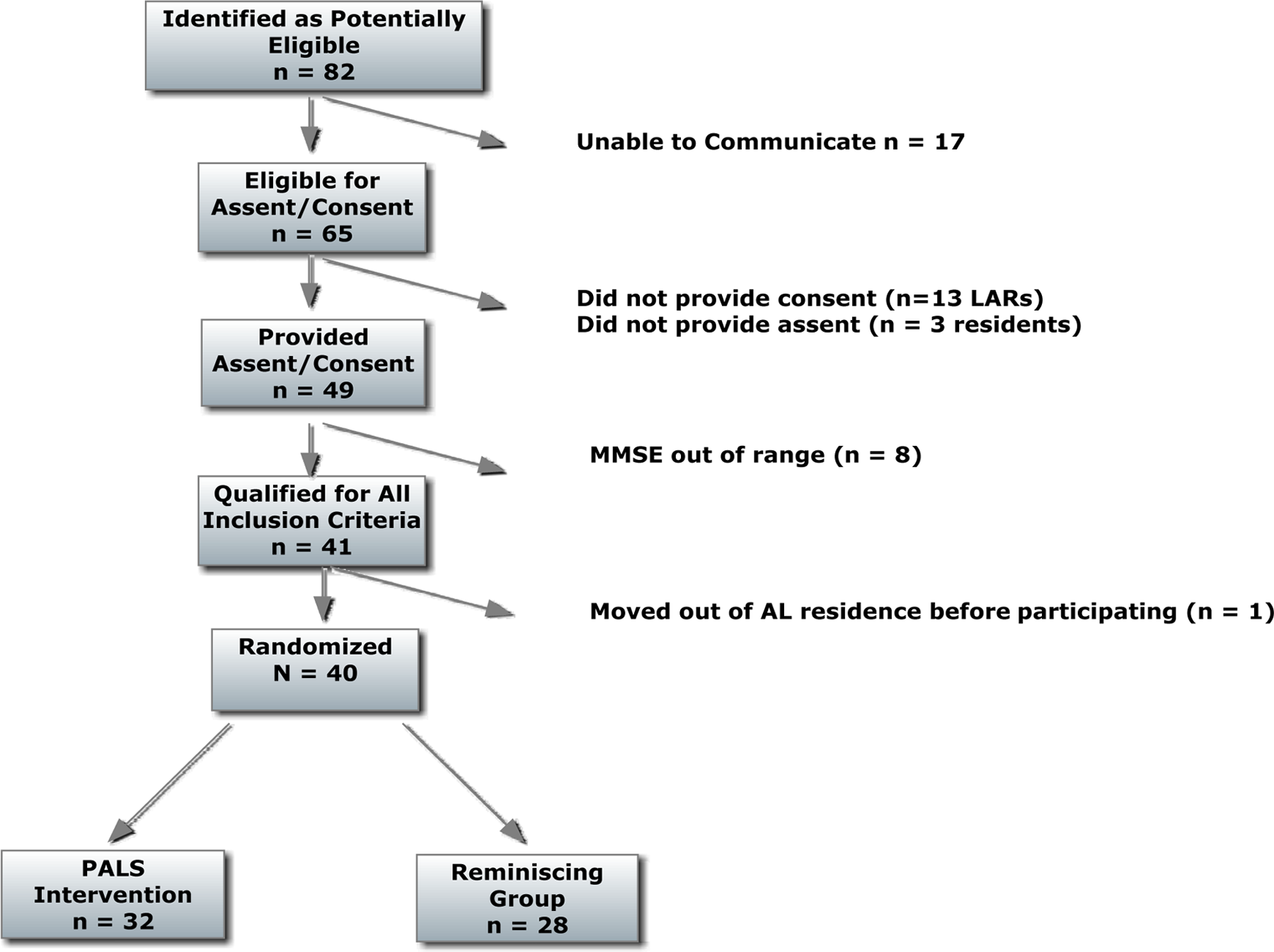
Consort diagram for enrollment in the pet-assisted living study (PALS). Abbreviations: LAR, legally authorized representative; MMSE, Mini-Mental State Examination.
A list of 82 potentially eligible residents was provided to the research team, 17 were unable to communicate; the remaining 65 were approached for participation. If the resident did not pass the Evaluation to Sign Consent, 64 he or she was asked to sign an assent to participate, and the legally authorized representative was contacted to complete the consent/HIPAA approval process. Eight residents did not qualify based on too high (n = 2) or too low (n = 6) scores on the MMSE. All legally authorized representatives (LARs) were contacted. A total of 13 eligible residents and 3 proxies refused to provide consent. One resident relocated from the participating AL residence prior to the beginning of the study. Thus, 40 AL residents participated in the study.
Setting
The study took place in residences that are part of a network of small family style AL residences located in suburban communities in Maryland. Each residence was home to 7 to 14 individuals. The residents spent most of the day in a family living room or dining area setting. Each residence was randomly assigned to 1 of the 2 interventions. Due to the varying numbers of participants at each residence, 4 facilities completed the PAL intervention and 3 facilities completed the reminiscing intervention. Residences were paired according to the number of residents, with the 2 smallest grouped to pair with the largest. For each pair, a coin was flipped to determine which member received each intervention. No other interventions or activity programs were being conducted at the facilities during the times they were participating in the study. One of the facilities assigned to the reminiscing intervention did have a resident pet but no program involving the residents with interacting with it.
Assessments
Participant demographics and health history were obtained from the residence records. Participant’s physical, behavioral, and emotional functioning were assessed prior to the intervention and at the end of every month of intervention. Assessments were completed by an independent nurse observer, who was not involved with the intervention. The residence staff member served as the informant for rating the resident’s emotional function with the 7-Item Apathy Evaluation Scale (AES) 65 and Cornell Scale for Depression in Dementia (CSDD), 66 the resident’s behavioral function with the Cohen-Mansfield Agitation Inventory (CMAI), 67,68 and the nurse rated the resident’s physical function with the Barthel Index. 69 The same staff member evaluated each resident on all occasions. The nurse applied an Actigraph Activity Monitor (Pensacola, Florida) to each resident’s chest to assess 24 hours of physical function.
Interventions
The PAL intervention consisted of 60- to 90-minute sessions with a therapy dog for residents participating in the program at each facility twice per week for 12 weeks. A 12-week intervention was previously effective for improving mood in patients with depression 70 and with psychiatric disorders. 71 The interventionist engaged each resident in dog-related activities during every visit. Skills taught/reinforced with different components of the dog visit program include: activities of daily living—feeding the dog, brushing the dog’s teeth, brushing the dog’s hair, and dressing the dog in a bandana; range of motion—throwing a ball, grooming the dog; small motor skills—adjusting a collar, hand feeding a treat, and petting the dog; sequencing events—opening a container of treats and then giving the dog a treat; and social skills—talking to the dog, talking about the dog to another person, giving the dog commands, and petting the dog. The dog used in the study was a Cardigan Welsh Corgi who was experienced at visiting nursing homes. The person conducting the intervention was a nurse practitioner familiar with working in the gerontological population. The intervention was conducted in a group living room environment with each participating resident taking turns with interacting with the dog and interventionist.
The reminiscing group was an attentional control intervention with equal amount of attention from the interventionist and the same schedule as the PAL intervention. Skills taught/reinforced in the reminiscing group included social skills—talking to the researcher and other residents and small motor skills—picking up pictures and showing them to others. The interventionist brought prompt material to the group meetings and encouraged conversation related to that topic and/or things that had been happening in the residence. The reminiscing intervention was conducted in a group living room or dining room environment with each participating resident encouraged by the interventionist to talk with the group.
Measurement
Physical function
Ability to perform activities of daily living was measured using the Barthel Index, a 14-item measure of physical function that assesses an individual’s ability for self-care. 69,72 Scores can range from 1 to 100. Higher scores indicate greater ability to perform activities of daily living, and a total score of 100 indicates complete independence in self-care.
Amount of physical activity was objectively measured for 24 hours using the ActiGraph an accelerometer that records activity with established reliability and validity. 73,74 The number of kilocalories expended by the resident in 24 hours was used as an index of activity level. The percentage of each resident’s time spent in moderate to vigorous physical activity during each 24-hour energy expenditure assessment was obtained from the Actigraph.
Emotional function
Depressive symptoms were measured using the CSDD, a well-validated 19-item survey designed to assess depressive symptoms in individuals with dementia. 66 Scores can range from 0 to 38. Scores of 6 or above indicate significant depressive symptoms, scores above 10 indicate a probable major depression, and scores above 18 indicate a definite major depression. 66,75
Apathy symptoms were measured using Zimmerman’s short version of the AES, a well-validated 7-item instrument. It rates a person's thoughts, actions, and emotions over the previous 4 weeks to measure motivation in older adults. 65 Scores range from 7 to 28, and lower scores indicate higher apathy.
Behavioral function
Agitated behaviors were measured using the CMAI, a survey of disturbing behaviors commonly found in long-term care residents with dementia. 76 The 14-item version of the CMAI (short form) uses a 5-point Likert-type scale to rate the frequency of behavioral symptoms in individuals with cognitive impairment and is based on the factor structure of the original CMAI inventory. Several studies have evaluated the psychometric properties of the CMAI and report evidence of reliability and validity. 68,76,77 Scores range from 14 to 70, and higher scores indicate higher agitation.
Demographic and health characteristics
Chart review was used to obtain demographic, diagnoses, and psychotropic medication (drug, dose, frequency of antipsychotics, antidepressants, anxiolytics, and sedative/hypnotics) data and date of admission to the residence. Medications and diagnoses were also obtained by chart review at the end of the intervention.
Data Analysis
Prior to data analysis, descriptive statistics were used to characterize the sample and evaluate the normality of the variables. Missing data analyses were used to evaluate randomness of missing data, there was no evidence that data were missing informatively (Little’s missing completely at random test = χ2(5) = 2.114, p = .833). Differences in preintervention levels of each outcome between the intervention groups were examined with t tests. Where normative data are available, separate chi-squares (χ2s) were used to assess differences in frequencies of categorization of participants in the 2 intervention groups at the beginning and at the end of the intervention. The square root transformation of depression and log transformation of agitation and energy expenditure were used to normalize data for longitudinal analyses. Intraclass correlations for the unconditional means models with nesting of participants within facilities (depression: 0.064, apathy: 0.019, agitation: 0.190, energy expenditure: 0.181, and Barthel: 0.00) and for the unconditional growth models with nesting of participants within facilities and sessions within participants (depression: 0.555, apathy: 0.477, agitation: 0.579, energy expenditure: 0.684, and Barthel: 0.813) confirmed the appropriateness of linear mixed models analyses. Two sets of linear mixed models were conducted separately for each outcome. The first set of analyses examined the independent contributions of intervention group and session as well as the interaction between the 2 predictors. The second set of analyses, stratified by the intervention group, was used to provide trajectories of changes in each measure of functional status on a monthly basis in the 2 treatment groups. All analyses were conducted with participants nested within facilities as well as sessions nested within participants. All tests were 2 tailed, despite directional hypotheses to address the possibility that the PAL intervention could lead to increased agitation. Analyses were conducted with SPSS 19.
Results
A total of 40 AL residents participated in the study, 22 in the PAL intervention group and 18 in the reminiscing intervention group. Participants ranged in age from 56 to 95 years with an average age of 81 (standard deviation [SD] = 9.1; see Table 1). The participants were largely female (72%) and almost all white (95%). Years of education ranged from 7 to 20 years. There were no significant differences in demographics (see Table 1) between participants in the 2 intervention groups.
Demographics, Diagnoses, and Medication Use of all Participants (N = 40) and of Participants in the Pet-Assisted Living (PAL) and Reminiscing Groups.a
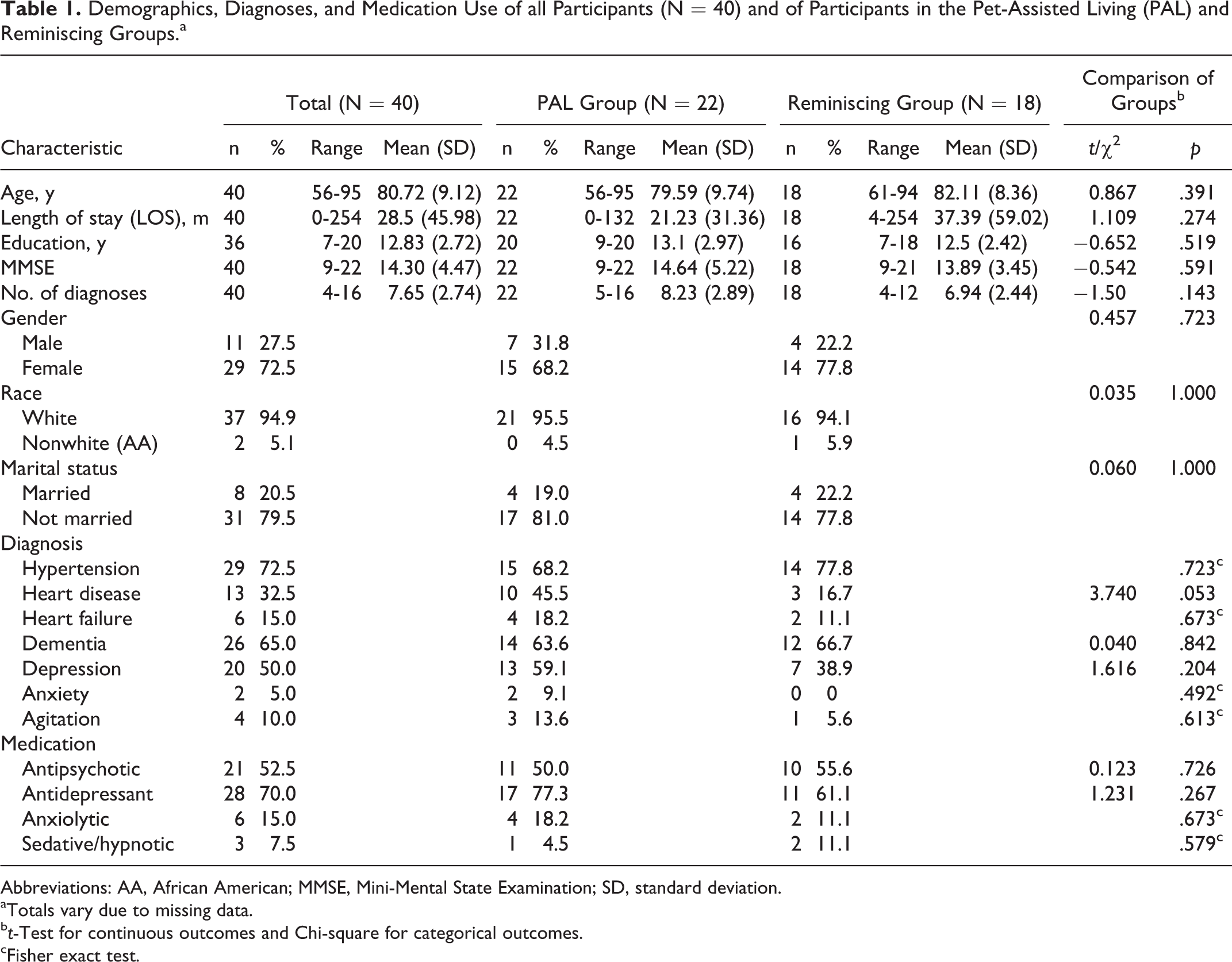
Abbreviations: AA, African American; MMSE, Mini-Mental State Examination; SD, standard deviation.
aTotals vary due to missing data.
b t-Test for continuous outcomes and Chi-square for categorical outcomes.
cFisher exact test.
Participants’ MMSE scores ranged from 9 to 22 with a mean of 14.3 (SD = 4.47; see Table 1). Scores on the MMSE did not differ significantly between the intervention groups. Participants’ times of residence in the AL facility ranged from 0 to 254 months with a median of 12 months. Mean length of residence in the AL facility did not differ significantly between participants in the 2 intervention groups, t 38 = 1.1, p = .274.
Health status indicators of the participants in the 2 groups did not differ significantly at initial assessment (Table 1). Participants had 4 to 16 diagnoses (mean = 7.65, SD = 2.74) at baseline. The number of diagnoses did not differ significantly in the intervention groups, t 38 = −1.50, p = .143. Sixty-five percent (26 of 40) of the residents had a documented diagnosis of dementia; however, all participants had evidence of mild to moderate cognitive impairment by history and by score on the MMSE. Additionally, 50% (20 of 40) of the residents had dementia with depression, 5% (2 of 40) with anxiety, and 10% (4 of 40) with agitation. Frequency of these psychiatric diagnoses did not differ in the intervention groups. Heart disease tended to be more common in the PAL group (45.5% vs 16.7%) than in the reminiscing group. Use of antidepressant, antipsychotic, anxiolytic, and sedatives/hypnotic medication at baseline also did not differ between participants in the 2 groups.
Two residents, both in the PAL intervention group, died due to preexisting conditions; heart failure and lung disease in 1 case and pneumonia in the other case, over the course of the study; and 1 PAL participant moved from the residence prior to the end of the study. The residents who died were 68 and 86 years old, the one who moved was 81 years old. They were the only participants who did not complete the study. Follow-up diagnoses and medications were not available for 1 participant in the PAL intervention group.
Changes in physical, behavioral, and emotional functioning in the PAL and reminiscing groups were described and examined for directional and statistical significance. Initial and end of intervention (3-month follow-up) scores for each dependant variables are provided in Table 2. In all analyses, significant variability in the outcome remained unexplained indicating that additional variables are needed to predict changes over time.
Functional Status Assessment of All Participants and Participants in Each Intervention at Initial Assessment (Baseline) and End of Intervention (3 Months).
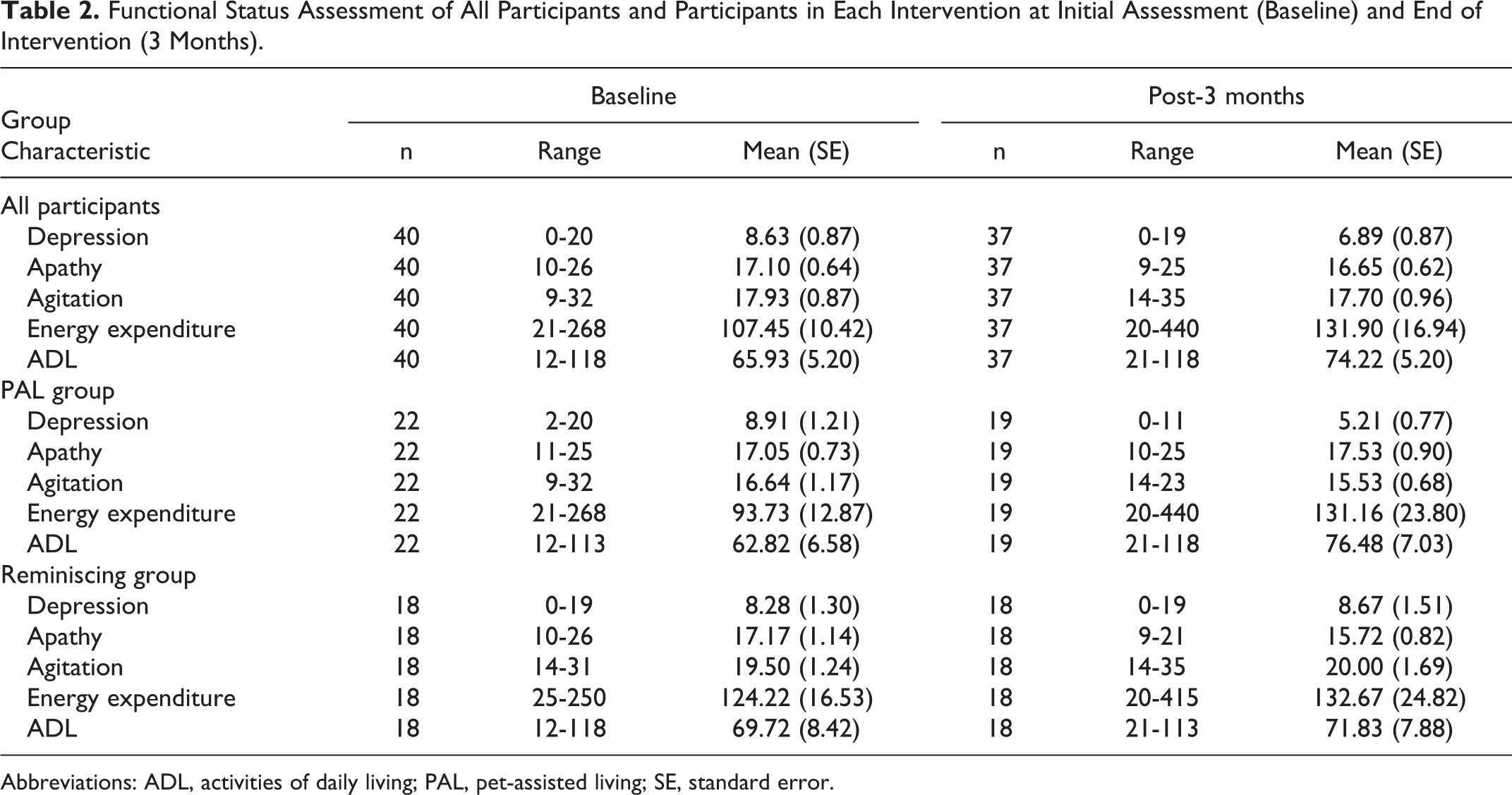
Abbreviations: ADL, activities of daily living; PAL, pet-assisted living; SE, standard error.
Physical Functioning
Changes in energy expenditure and physical activity as assessed with 24-hour activity monitors and self-care activities as assessed with the Barthel Index were used to examine changes in physical functioning over the 3-month period in the 2 treatment groups. At initial assessment, 40.9% of the participants in the PAL intervention group and 38.9% of those in the reminiscing intervention group spent less than 1% of their time in moderate or greater physical activity. After 3 months of intervention, 36.8% of the participants in the PAL intervention group and 37.5% of those in the reminiscing intervention group spent less than 1% of their time in moderate or greater physical activity.
At initial assessment, average energy expenditure beyond basal activity was 107 Cal/d. During the first 24-hour activity assessment, there was no significant difference in mean calories of activity between the 2 intervention groups, t 38 = 1.478, p = .148. In the first analysis of energy expenditure, there was a significant interaction, β = 0.06 (0.033), t 111.119 = 2.078, p = .040, between intervention and session; the effect size for the interaction was 0.19. Stratified linear mixed models analysis (Table 3) revealed that the slopes of changes in energy expenditure over time were in opposite directions although in neither intervention was the change significant (PAL: p = .306; reminiscing: p = .072). Physical activity increased slightly over time for the PAL intervention group and decreased for the reminiscing group over the course of the intervention period.
Summary of the Results of the Stratified Linear Mixed Models Analyses to Examine Changes Over Time in Emotional (Depression and Apathy), Behavioral (Agitation), and Physical (Energy Expenditure and Activities of Daily Living) Function of Assisted Living Residents With Mild to Moderate Dementia Who Participated in the Pet-Assisted Living (PAL) Intervention (n = 22) or a Reminiscing Intervention (n = 18) Twice Weekly for 3 Months.a
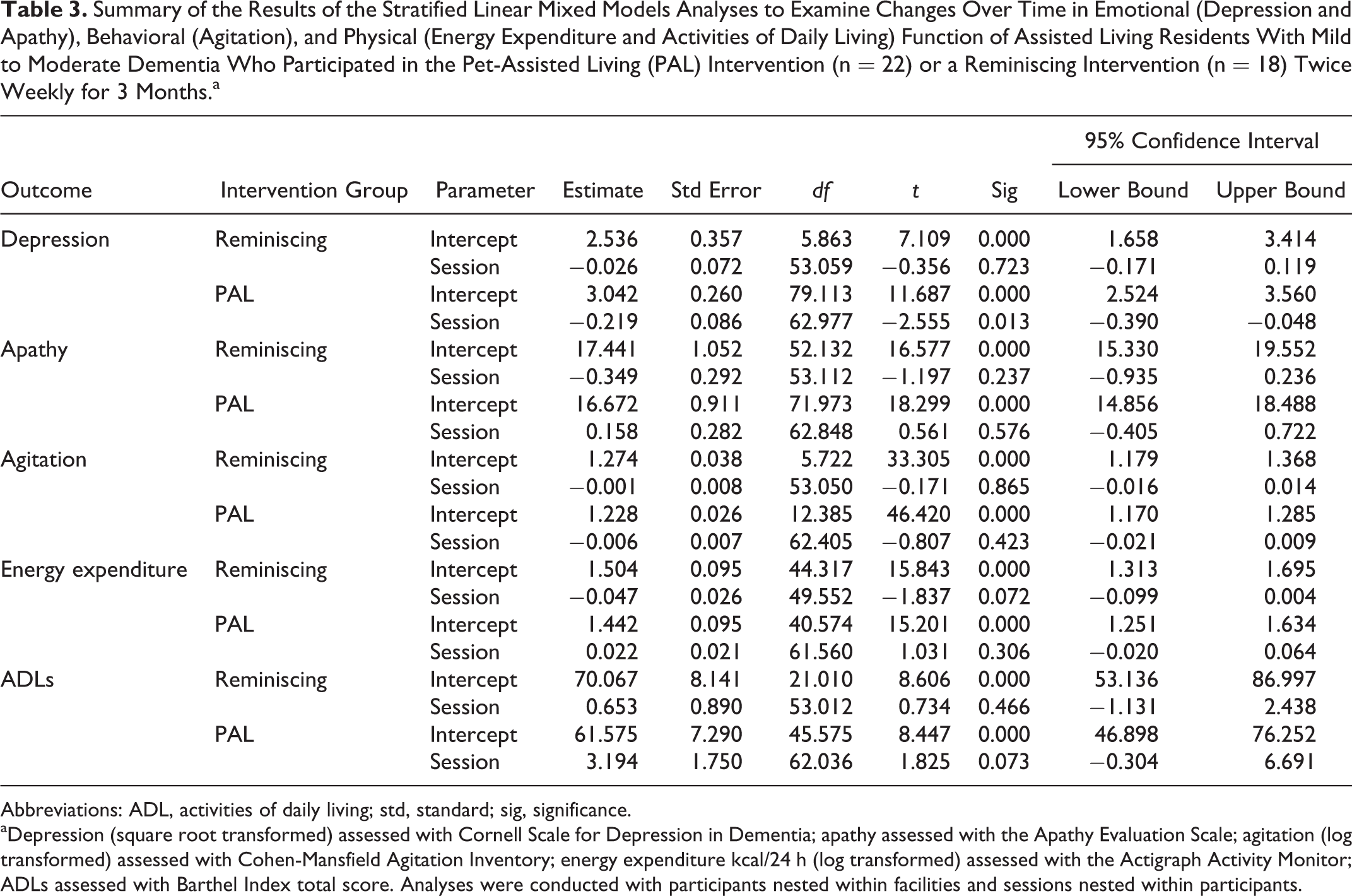
Abbreviations: ADL, activities of daily living; std, standard; sig, significance.
aDepression (square root transformed) assessed with Cornell Scale for Depression in Dementia; apathy assessed with the Apathy Evaluation Scale; agitation (log transformed) assessed with Cohen-Mansfield Agitation Inventory; energy expenditure kcal/24 h (log transformed) assessed with the Actigraph Activity Monitor; ADLs assessed with Barthel Index total score. Analyses were conducted with participants nested within facilities and sessions nested within participants.
At the initial assessment, only 1 person in each group did not require significant assistance with self-care, as indicated by a score of 100 on the Barthel Index. Similarly, 1 person in each group did not require assistance with self-care after 3 weeks of intervention. At initial assessment, the mean score on the Barthel Index was 65.93. Initial average activities of daily living (Table 2) did not differ significantly between the 2 intervention groups, t 38 = 0.656, p = .516. In the first analysis of Barthel Index score, there was no significant interaction, β = 2.548 (10.890), t 114.645 = 1.28, p = .215, between intervention and session; the effect size for the interaction was 0.08. In stratified linear mixed models (Table 3), activities of daily living (ADL) as assessed by the Barthel score tended to increase over time in the PAL group (p = .073) but not in the reminiscing group (p = .466).
Emotional Functioning
Changes in depression and apathy were used to examine changes in emotional functioning over the 3-month period in the 2 treatment groups. At the initial, preintervention assessment 62.5% (25 of 40) of the participants met the criteria for possible depression (score 6 or above) on the Cornell Depression in Dementia Scale. At baseline, rate of depression did not differ significantly between the PAL group (59.1%) and the reminiscing comparison (66.7%) group, χ2(1df) = 0.24, p = .622. After 3 months of intervention, the rate of depression tended to be lower in the PAL intervention group (36.8%) than in the reminiscing (66.7%) comparison group, [χ2(1df) = 3.29, p = .07. There was no change in frequency of antidepressant medication orders over the course of the study in either group (Table 4).
Medications Taken and Number of Diagnoses Present on Medical Records at Initial Assessment (Baseline) and End of Intervention (3 Months) for Participants in the PAL Intervention and the Reminiscing Comparison Group.a,b
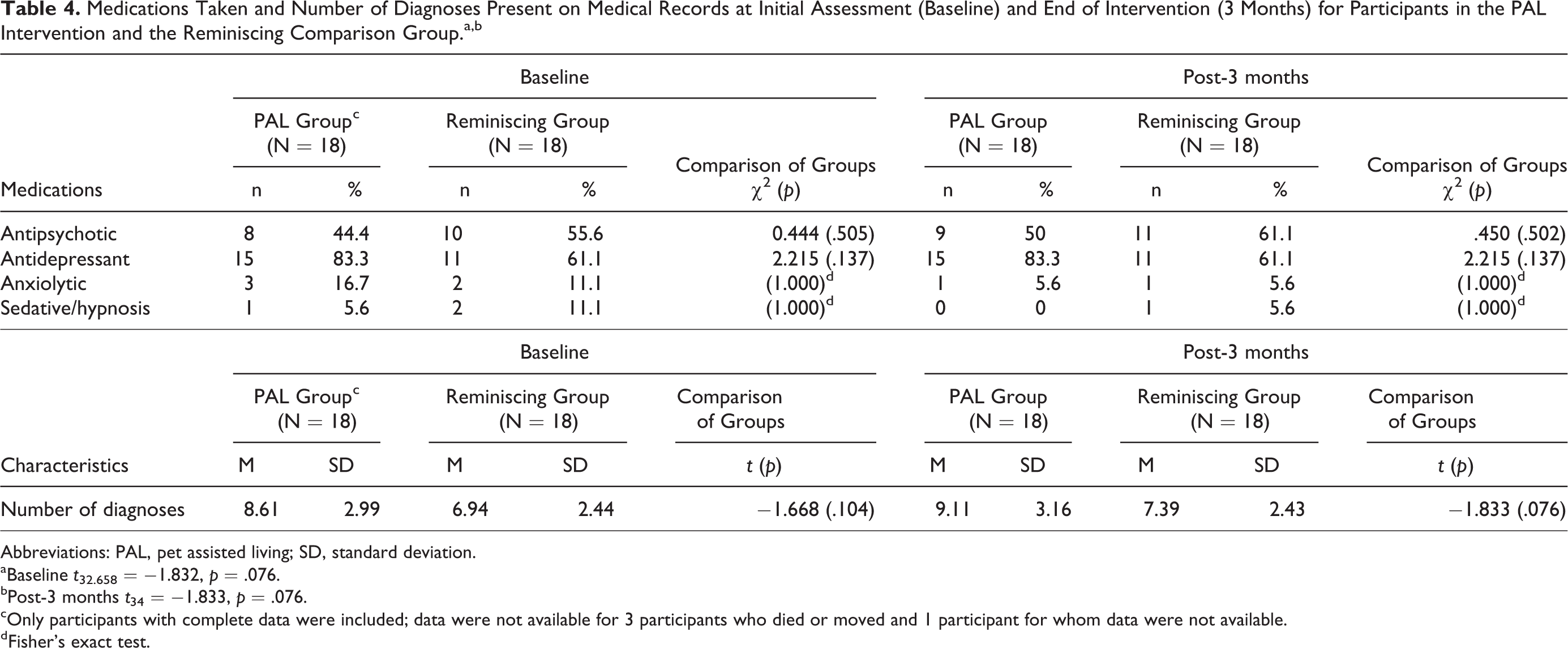
Abbreviations: PAL, pet assisted living; SD, standard deviation.
aBaseline t 32.658 = −1.832, p = .076.
bPost-3 months t 34 = −1.833, p = .076.
cOnly participants with complete data were included; data were not available for 3 participants who died or moved and 1 participant for whom data were not available.
dFisher's exact test.
Average initial depression scores did not differ significantly between the groups, Table 2; t 38 = −0.355, p = .724. In the first analysis of depression, there was a tendency for an interaction, β = 0.20 (0.11), t 115.4 = 1.757, p = .082, between intervention and session; the effect size for the interaction was 0.18. In stratified linear mixed models, depression decreased significantly over time (Table 3) in the PAL group (p = .013) but not in the reminiscing group (p = .723). Depression tended to decrease more over the course of the intervention in the PAL group than in the reminiscing comparison group.
Average apathy score at baseline was 17.1 of a possible 25. At the initial, preintervention assessment, average apathy did not differ significantly between participants in the 2 intervention groups, Table 2; t 38 = 0.092, p = .927. In the first analysis of apathy, there was no significant interaction, β = 0.503 (0.407), t 115.719 = 1.237, p = .219, between group and session; the effect size for the interaction was 0.12. Stratified linear mixed models analysis revealed that the slopes of changes in apathy over time were in opposite directions, although in neither case was the change significant (PAL: p = .576; reminiscing: p = .237). Apathy moved in an improved direction very slightly over time for the PAL group and in a worsening direction over time for the reminiscing group.
Behavioral Functioning
Changes in agitation were used to examine changes in behavioral functioning over the 3-month period in the 2 treatment groups. At initial assessment, no participants demonstrated significant agitation. Average initial agitation score on the CMAI was 17.9. Average initial agitation (Table 2) did not differ significantly between the 2 groups, t 38 = 1.675, p = .102. One member of the reminiscing group became agitated over the course of the study. In the first analysis of apathy, there was no significant interaction, β = −0.005 (.011), t 115.271 = −0.432, p = .666, between group and session; the effect size for the interaction was 0.12. A stratified linear mixed models analysis revealed that the slopes of changes in agitation over time were in opposite directions (Table 3), although in neither case was the change significant (PAL: p = .423; reminiscing: p = .865). Agitation decreased slightly over time with the PAL intervention and stayed the same over time with the reminiscing intervention.
Medication Use
Changes in medication use over the course of the study were examined to evaluate the potential for differences in changes in functional status between the intervention groups to be attributable to differences in changes in medication. Over half (70%) of the participants were receiving antidepressant medication, and over half (52.5%) of the participants were receiving antipsychotic medication prior to the interventions. Fewer (15%) of the study participants were receiving anxiolytic, and 7.5% were receiving sedative/hypnotic medications prior to the interventions. Changes in behavioral medication over the course of the 3-month treatment period were minimal. Antidepressants and antipsychotic medications were added for 1 participant in each group (Table 4), anxiolytic medication was removed from 2 members of the PAL group and 1 member of the reminiscing group, and sedative/hypnotics were removed from 1 member of each group over the course of the study. There were no significant differences in frequency of any type of medication between the 2 groups either at initial assessment prior to the interventions or at the final assessments after 3 months of intervention.
Discussion
The current study suggests that a PAL program can be effective at improving physical, behavioral, and emotional function in AL residents with cognitive impairment or dementia. All trajectories of change from pre- to post-PAL intervention were in the direction of improvement in the outcome as was expected.
Energy expenditure was extremely low in the residents studied, an average of 107 Cal above basal metabolic rate per day. This may be related to the AL small home type of residence, with very little room to move around compared with a more institutional facility with long corridors. This, in combination with the inability of many residents (70%) to walk without assistance, made it impossible to have the residents participate in dog walking, which would have been ideal. Despite this limitation, there was a difference in the trajectory of energy expenditure between the groups over the 3 months of the study. The PAL participants’ energy expenditure increased, while the reminiscing group participants' decreased.
Utilizing the theory of self-efficacy, the PAL intervention involved practicing and building confidence in physical tasks with the dog, for example, brushing its hair, that can be translated into self-care tasks. The Barthel Index was used to assess ability to complete activities of daily living. There is sufficient evidence for the reliability and validity of the Barthel Index when used with older adults, 69,72 individuals with progressive neurological conditions, 78 and when proxy-respondents reporting the functional abilities of dementia patients. 79 There was no significant improvement in the activities of daily living as assessed on the Barthel Index over the 3 months of intervention; however, the trajectories of changes over time tended to differ for the 2 intervention groups. These findings are in the expected direction; the Barthel Index improved over time in the pet assisted living (PAL) intervention group and deteriorated over time in the reminiscing group. Two additional studies did not support major changes in physical activity as a result of animal activities for elders with dementia. For individuals with severe dementia, increases in motion were similar in dog activities (similar to the PAL intervention) and comparison activities conducted over 3 months. 60 In a day care program for individuals with dementia, activities of daily living increased over the duration of the therapy period for participants who received dog therapy twice per week for 3 months and decreased for the reminiscing group, but the changes were small and not significant. 61
The PAL intervention as implemented in this setting with this population did not include a walking component. Many of the residents included in the sample had impaired mobility; 70% of residents used assistive devices to walk and 24% of residents could not stand without assistance. We acknowledge this less typical of many AL settings. Smaller ALs were used in this study and the philosophy of these sites was to maintain residents in AL setting as long as possible, even when residents were no longer able to ambulate safely. Additionally, residents with cognitive impairment were recruited to participate in this study, and half of the participants had a diagnosis of depression. The severity of both cognitive impairment and depression is a significant predictor of functional disability in AL populations. 9 An implementation that also encourages the residents to take the dog for a walk is likely to increase physical function more than occurred in this study.
Residents of the AL facilities in this study were more likely to be depressed (62.5% vs 14%) and to be cognitively impaired (100% vs 48%) than a large sample from a residential care and AL facilities population with length of stay comparable to the participants in the current study (median 12 months). 18 In the current study, the rate of depression and average depression scores after 3 months of intervention were significantly lower in the PAL group than in the reminiscing group, although they did not differ significantly at baseline. The high prevalence of depression in the participants in the current study was helpful for assessing the impact of the interventions. The lack of improvement in the reminiscing groups suggests that the changes seen in the PAL group were not a result of regression to the mean. These findings are consistent with those of 2 recent experimental studies of older adults with dementia. One group of nursing home residents with dementia, depression, and psychoses tended to experience more improvement in depression after 6, 90-minute weekly group sessions with several dogs than a comparison group. 57,80 In aged care residents, an 11-week dog intervention led to greater improvements in depression than person visits among residents with mild to moderate dementia. 57 In that study, depression improved more in the dog intervention than in the person-only intervention among residents who were more depressed. Depression also tended to improve in individuals with more severe Alzheimer’s dementia during 3 weekly group visits with several dogs but not after weekly visits with stuffed dogs. 60 In contrast, depression did not change among 8 nursing home residents with dementia who participated in activities with 2 dogs for an hour a day for 4 consecutive days. 47
The 7-item AES was used as a measure of emotional function. A strong correlation was demonstrated between the 18-item AES and the 7-item AES. Cronbach's α for the 7-item AES was .67. The AES is used to measure motivation in older adults. 65 Participants in the current study demonstrated low levels of apathy, despite their dementia. Although change was nonsignificant, apathy improved slightly for participants in the PAL intervention and worsened slightly for participants in the reminiscing group over the course of the study. These results contrast with the significant decrease in apathy among 8 nursing home residents with dementia who participated in activities with 2 dogs for an hour a day for 4 consecutive days. 47 The low apathy scores of the participants in the current study made it difficult to evaluate the effectiveness of interventions for decreasing apathy or increasing motivation in this population.
Residents of the AL facilities in this study were less likely to be agitated (0% vs 34%) than a large sample from residential care and AL facilities population with length of stay comparable to the participants in the current study. 18 In the current study, the low prevalence of agitation made it difficult to effectively evaluate the effectiveness of interventions for decreasing agitation. Agitation decreased slightly in the PAL group and remained constant in the reminiscing group. Several other studies without comparison groups also support reductions in agitation among nursing home residents with dementia, 46,60 long-term care residents with severe agitation, 58 and individuals with severe Alzheimer’s who attend day care programs. 48 Person centered care is focused on having caregivers use strategies that focus on nurturing, resident comfort, and individual preferences. 81 -84 Concerns that interventions that increase stimulation and physical activity for individuals with dementia may increase behavioral symptoms due to overstimulation were not supported. 40
Over half of the residents who participated in this study were receiving antipsychotic medication. This high frequency is more typical of dementia specific AL residences (67%). 85 -87 It is well recognized that antipsychotics have a significant side effect profile including sedation, falls, hypotension, constipation, CVA, pneumonia, and death. In the current study, improvements in physical activity in the PAL intervention group occurred despite and beyond the side effect profile of antipsychotics. Future research should assess the long-term impact of the PAL intervention on gradual dose reduction in psychotropic medications, particularly antipsychotics.
All the participants included in this study had cognitive impairment; however, only 65% of the participants were actually diagnosed with dementia. Previous research has demonstrated that dementia is underdiagnosed in AL settings. 2,5,88 When AL residents without a diagnosis of dementia were evaluated by neurologists and psychiatrists, the dementia diagnosis had been missed in 25% to 38% of the AL residents who were evaluated. 5,89 Assisted living staff was less likely to correctly recognize dementia among residents who did not have severe cognitive impairment or obvious behavioral symptoms and functional impairments. 2
The PAL intervention included both the interventionist and the dog. The reminiscing attentional control intervention was of the same duration and with the same interventionist as the PAL intervention. This supports the attribution of differences between the interventions to the integration of the dog into the PAL intervention. It is not necessary to completely separate out the contributions of the interventionist and the dog in the PAL intervention. All animal-assisted interventions integrate an interventionist and an animal. The interventionist is responsible for guiding the intervention and directing the animal to enact the activities as required for the intervention. The interventionist also monitors dog and participant activities to assure safety of both parties. 90 The PAL intervention is more complex including more elements. Both interventions include small motor and social/communication activities. The PAL includes additional activities of daily living and range of motion elements. It is possible that the diverse elements in the PAL intervention are partially responsible for the differences in the residents’ responses.
This study included only AL residents whose legally responsible representative indicated that they either had “prior experience” with dogs or had interest with a dog or indicated this themselves. Residents with these characteristics may react more positively to the PAL intervention than those without prior experience with animals. It is important to note that only people who are comfortable with animals are appropriate participants in any animal-assisted intervention or activity.
This study was limited due to the limited number and type of facilities included and the lack of the specific dementia diagnosis. The PAL intervention may perform differently in larger facilities with more programs available to the residents. Use of 5 different outcomes may have led to significant changes occurring by chance. The lack of significant agitation and apathy in this population also limited the likelihood that any improvement could be observed. Future work should include the specific type of dementia if it is known.
The PAL program may be effective for preserving/enhancing emotional and behavioral function in residents of AL with cognitive impairment consistent with mild to moderate dementia. Additional study in a population with more agitated and apathetic individuals is warranted to determine the basis of the differences in the trajectories in the current study.
The reduction in depression demonstrated by the PAL intervention would also tend to encourage improvement in physical function in this population. Examination of the effectiveness of a PAL intervention that includes walking will allow evaluation of the relationship between changes in depression and physical activity.
A variety of activities is useful for maintaining function, but some activities are not suitable for residents with cognitive impairment. 45 Both the PAL and the reminiscing intervention were well received by the residents of the facilities as well as by the staff. Several residents expressed distress when told that the interventionist would not be returning the following week.
The current study included a 3-month intervention because that is the minimal duration for which similar types of interventions have proven effective 57,60,61 and to minimize loss of participants due to death or relocation. Evaluation of longer duration is necessary to demonstrate longer term effectiveness.
The a prior power analysis used correlations between measures of .32 to estimate the required sample size. Actual intercorrelations (depression: 0.555, apathy: 0.477, agitation: 0.579, energy expenditure: 0.684, and Barthel: 0.813) were larger. On this basis, smaller sample sizes would be estimated for future studies. However, the effect sizes were smaller than the .25 estimated as a medium effect size. Using calculated effect sizes for the interactions (depression: 0.18, apathy: 0.12, agitation: 0.04, energy expenditure: 0.19, and Barthel: 0.08) led to post hoc power estimates indicating adequate power for depression (0.77) and energy expenditure (0.93) but not for the other measures (apathy: 0.35; agitation: 0.08; Barthel: 0.35). Larger samples and participants with more variability in apathy, agitation, and ADLs are necessary to draw conclusions about the effectiveness of the PAL intervention for improving these outcomes.
There were minimal changes in behavioral medication over the course of the study, and there were no significant differences in frequency of any type of medication between the 2 intervention groups at either initial or final assessment. Three months of follow-up is likely too short to evaluate the impact of the intervention on behavioral medication. Assessment of the long-term impact of the PAL intervention on gradual dose reduction in psychotropic medication, particularly antipsychotics, should be considered. Furthermore, much larger studies are required to investigate whether PAL interventions lead to reduced relocation to nursing home or improved survival.
Implications for Nursing Practice
Some of the factors that serve as barriers to engagement in physical activity among long-term care residents include apathy, boredom, lack of motivation, and anxiety. 91 -93 When traditional walking and exercise programs are offered in these settings, only a small number of residents are willing to participate, 94 and nurses may resign themselves to engaging residents in sedentary activities. Additionally, many long-term care facilities offer pet visitation or pet presence; however, many do not utilize these pet visits to overcome the motivational challenges and actively engage AL residents with cognitive impairment in physical activities. Using the PAL intervention, which makes use of self-efficacy based approaches, such as role modeling, eliminating unpleasant sensations, and encouragement, long-term care nurses have the opportunity to serve as facility-based champions to implement creative approaches to address a health promotion need of their residents and overcome motivational challenges, particularly for those with mild to moderate cognitive impairment.
Conclusion
The results of this pilot study are promising, suggesting the potential for the PAL intervention to lead to improvement in physical, behavioral, and emotional function. Further studies extending over longer time periods with larger samples are warranted to evaluate the predictors of effectiveness of the PAL intervention for each type of function and the duration of its effect.
Footnotes
Declaration of Conflicting Interests
Dr. McCune is employed by WALTHAM®. WALTHAM® provided Dr. Friedmann with travel funds to report research results at conferences.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was supported by an ISAZ/WALTHAM® Collaborative Research Award.