
Abstract
Background:
Increasing evidence suggests that gangliosides act as important mediators in both de- and remyelination. The scope of the present research was to investigate the presence of immunoglobulin (Ig) M antibodies against GM1, GD1b, and GQ1b gangliosides in the sera of patients with dementia and the possible connection with clinical parameters of the disease.
Method:
This research topic demonstrates the investigation of 103 patients with dementia and 60 healthy individuals using enzyme-linked immunosorbent assay for the presence of 3 antiganglioside antibodies in their sera.
Results:
The authors report a positive connection between IgM anti-GM1 and the age (P = .005) and the severity of dementia (P = .005). Most of the patients who revealed increased IgM anti-GD1b levels had Alzheimer’s disease (AD; P = .002).
Conclusion:
This study indicates that elevated IgM anti-GM1 may be connected with the neurodegeneration in older patients with severe dementia and that AD may also be associated with increased IgM anti-GD1b levels.
Introduction
Lipids play a potential role in the pathology of many neurodegenerative disorders of central nervous system like dementia and Alzheimer’s disease (AD). 1,2
Gangliosides are acidic glycosphingolipids of the plasma membranes which are mainly present in neural membranes (especially in presynaptic membranes). In addition to their role as surface markers in the outer leaflet of cell membranes, gangliosides are thought to have multiple biological functions. Due to their hydrophilic extracellular carbohydrate structure, they are capable of acting as an autoantibody target. 3,4
Gangliosides can act as receptors for viruses, bacterial toxins (eg, GM1 for cholera toxin and GQ1b for botulinum toxin), 5 -9 and have been thought to be the autoimmune targets in immune-mediated neuropathies (like Guillain-Barré syndrome) as well as other neurodegenerative diseases. 10 -12
Gangliosides are also known to be receptors for myelin-associated glycoprotein (MAG), an enhancer of axon–myelin stability, and also a potent inhibitor of axonal degeneration (after injury). 13 -15 Especially GT1b, GD1a, and GQ1bα appear to be potent support molecules for MAG, while GD3 does not bind. 13,16 Increasing evidence suggests that gangliosides act as modulators of cell functions including cell growth, apoptosis, and differentiation. 17
A pathological hallmark of AD concerns the eventual role that toxic aggregates of amyloid β (Aβ) protein play, as they are formed from their neurotoxic form.
Based on many research topics, ganglioside GM1 binds specifically to Aβ-peptide, in a cholesterol-rich environment, and it may inhibit its conformational changes. The GAβ complex activates microglia to produce antibodies and neurotrophic factors that disturb the myelin and may cause the neurodegeneration. 18 -24
In the present research, we investigated the levels of 3 antiganglioside antibodies (immunoglobulin [Ig] M type) in the sera of patients with dementia. Based on several studies, IgM gangliosides are detected in acute phases while IgG gangliosides in chronic phases of several demyelinating diseases.
Moreover, we focused on antibodies against GM1, GD1b, and GQ1b since they are the most widely with enzyme-linked immunosorbent assay (ELISA) studied ganglioside antibodies in the literature. Finally, we attempted to compare the results with the clinical parameters, to establish a possible correlation between them.
Materials and Methods
Patients
We examined 103 patients with dementia (35 men and 68 women), with a male to female ratio of 1:1.9, at a mean age of 71.1 ± 8.5 years for women and 71.9 ± 8.4 years for men and 60 healthy individuals (31 females and 29 males) with a mean age of 71.2 ± 6.3 years for women and 71.4 ± 8.6 years for men. The study patients gave informed consent for their participation; their anonymity was preserved.
We examined all patients and the control group for the presence of acute or chronic inflammatory or infectious disease, cancer, metabolic, or other severe pathological disorders. The controls were age-matched individuals with no history of immune or neurological disease. The patients had no prior history of peripheral neuropathy, and the neuropshysiological examination excluded current peripheral nerve disease.
The diagnosis of dementia, as well as the type of dementia, was based on the diagnostic criteria of Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition), National Institute of Neurological and Communicative Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association, the clinical, laboratory, and neuroimaging findings (computed tomography scan, brain magnetic resonance imaging [when necessary], and brain single-photon emission computed tomography). Moreover, we classified all patients referring to the gender, the age, the type of dementia as well as the grade of cognitive impairment.
We determined the clinical stage of dementia by neurological evaluation and neuroimaging as well as by the use of specific neuropsychological tests, like the Mini-Mental State Examination (MMSE) scale, which indicated the neurological disability of the patients in addition to the deficits of cognition. According to this scale, a mild cognitive impairment is characterized by a score of 20 to 25 of 30, a moderate cognitive impairment by a score of 15 to 20 of 30, and severe cognitive impairment by a score of <15 of 30, while scores between 25 and 30 of 30 are considered as normal. In the present research, the evaluated patients revealed a mean score of 20.7 ± 7.3 of 30, while the healthy individuals revealed normal scores (>28 of 30).
Referring to the types of dementia, 37 (36%) had vascular dementia, 24 (23%) had frontotemporal dementia, 18 (17%) had AD, 13 (13%) had mixed dementia, 9 (9%) had pseudodementia (dementia due to depression) and 2 (2%) had possible Lewy body dementia (LBDD).
Samples
We investigated the presence of IgM antibodies against GM1, GD1b, and GQ1b in the sera of the examined patients as well as of the healthy controls. We collected peripheral venous blood and centrifuged it for 10 minutes in 2000g; we separated the supernatants and froze in aliquots at −40°C. We determined serum concentrations of GM1, GD1b, and GQ1b-IgM using commercially available ELISA kits (IMMCO diagnostics Inc, New York, USA).
Anti-GM1 IgM, nti-GD1b IgM, Anti-GQ1b IgM Assays
Via ELISA we determined the presence of IgM antibodies against GM1, GD1b, and GQ1b gangliosides, using 96-well microtiter plates coated with the individual ganglioside, according to the manufacturer’s instructions.
Serial dilutions were made (1:50-1:200) and each sample was analyzed in duplicate. A positive and a negative control consisting of a serum sample, produced by the manufacturer, with high and low levels of IgM antiganglioside, respectively, were included in the assay. The negative control should be <20 EU/mL.
Levels of antibodies <20 EU/mL have been considered negative, while positive samples have had concentrations >25 EU/mL. Intermediate levels between 20 and 25 EU/mL were considered borderline.
Statistical Analysis
We chose to divide the patients in the following intervals: According to the age: group 1 (50-65 years), group 2 (66-75 years), and group 3 (76-86 years). According to the scores in the MMSE scale: group1 (1-18 of 30), Group 2 (19-25 of 30), and group 3 (26-30 of 30). For the correlation of the examined antibodies with the types of dementia, we separated the patients according to the concentrations of the antiganglioside antibodies: group 1 (8-19 EU/mL, negative), group 2 (20-25 EU/mL, intermediate borderline), and group 3: (>25 EU/mL, positive). The subdivision was given by the manufacturer.
We compared the results of antiganglioside antibodies of patients and those of the healthy controls using the Mann-Whitney U test of the SPSS 16.0. We evaluated the differences between antiganglioside antibodies versus age and MMSE scores with 1-way analysis of variance (2-tailed with the confidence interval at 95%). Finally, we compared the levels of 3 antiganglioside antibodies with the type of dementia via the chi-square analysis (confidence interval at 95%).
Results
Comparisons of Anti-GM1 IgM, Anti-GD1b IgM, and Anti-GQ1b IgM in Patients and Healthy Individuals
We examined the levels of anti-GM1 IgM, anti-GD1b IgM, and anti-GQ1b IgM in the serum of 103 patients with dementia setting the cutoff value of >25 EU/mL (Table 1).
Antiganglioside Antibodies of Patients With Dementia Versus Healthy Individuals.a
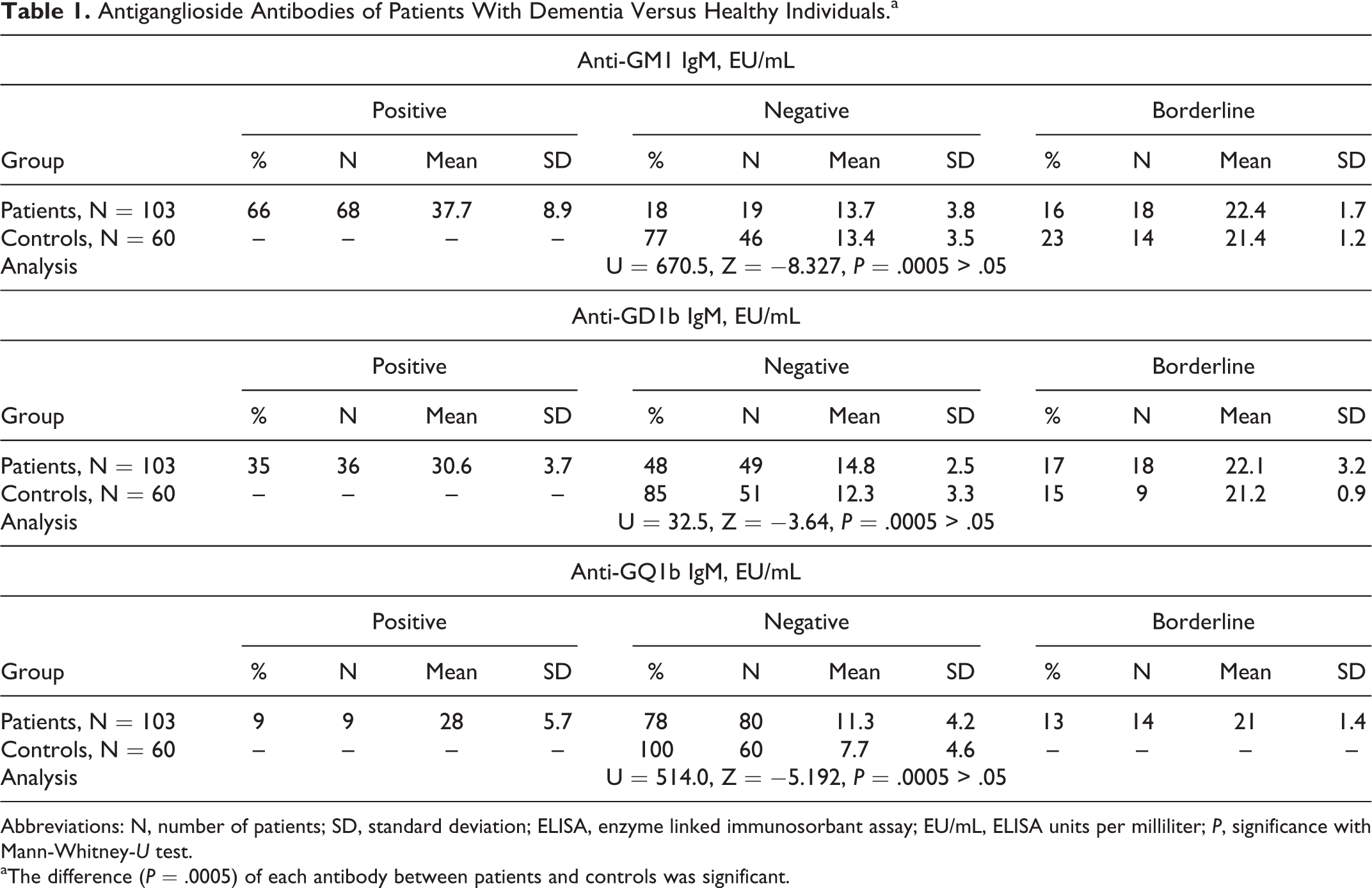
Abbreviations: N, number of patients; SD, standard deviation; ELISA, enzyme linked immunosorbant assay; EU/mL, ELISA units per milliliter; P, significance with Mann-Whitney-U test.
aThe difference (P = .0005) of each antibody between patients and controls was significant.
The concentrations of the positive controls were within the ranges indicated on the labels. Furthermore, our laboratory conducts anti-GM1, anti-GD1b, and anti-GQ1b studies in patients with Guillain Barrè and Chronic inflammatory demyelinating polyneuropathy (CIDP), confirming the accuracy of the test.
According to the present research, 66% of the patients revealed increased concentrations of anti-GM1 IgM (mean 37.7 ± 8.9 EU/mL), while only 18% were negative (mean 13.7 ± 3.8 EU/mL) and 77% of the healthy controls revealed negative anti-GM1 IgM (mean 13.4 ± 3.5 EU/mL), thus providing a statistically significant difference (U = 670.5, Z = −8.327, P = .0005).
Anti-GD1b IgM has also been determined in high concentrations (mean 30.6 ± 3.7 EU/mL) in 35% of the patients, while 49% revealed low levels of the examined antiganglioside antibody (mean 14.8 ± 2.5 EU/mL). Most of the controls (85%) demonstrated negative anti-GD1b IgM (mean 12.3 ± 3.3 EU/mL), with statistically important difference (U = 32.5, Z = −3.64, P = .0005).
Anti-GQ1b IgM assays revealed high levels in 9% of the patients with dementia (mean 28.0 ± 5.7 EU/mL), whereas 78% of them had a mean concentration of 11.3 ± 4.2 EU/mL. Anti-GQ1b IgM assay in healthy individuals demonstrated only decreased levels (mean 7.7 ± 4.6 EU/mL; U = 514.0, Z = −5.192, P = .0005).
The 3 examined antiganglioside antibodies demonstrated no pathological levels in the healthy control group.
Comparison of Antibodies Against GM1, GD1b, and GQ1b With the Age of the Patients With Dementia
According to our results, older patients with ages between 66 and 86 years revealed the most increased concentrations of anti-GM1 IgM (mean 28.1-37.0 EU/mL; F 2,101 = 30.6, P = .005 < .05; Table 2 and Figure 1). No statistical significant difference appeared between anti-GD1b IgM and anti-GQ1b IgM with the age of the examined patients.
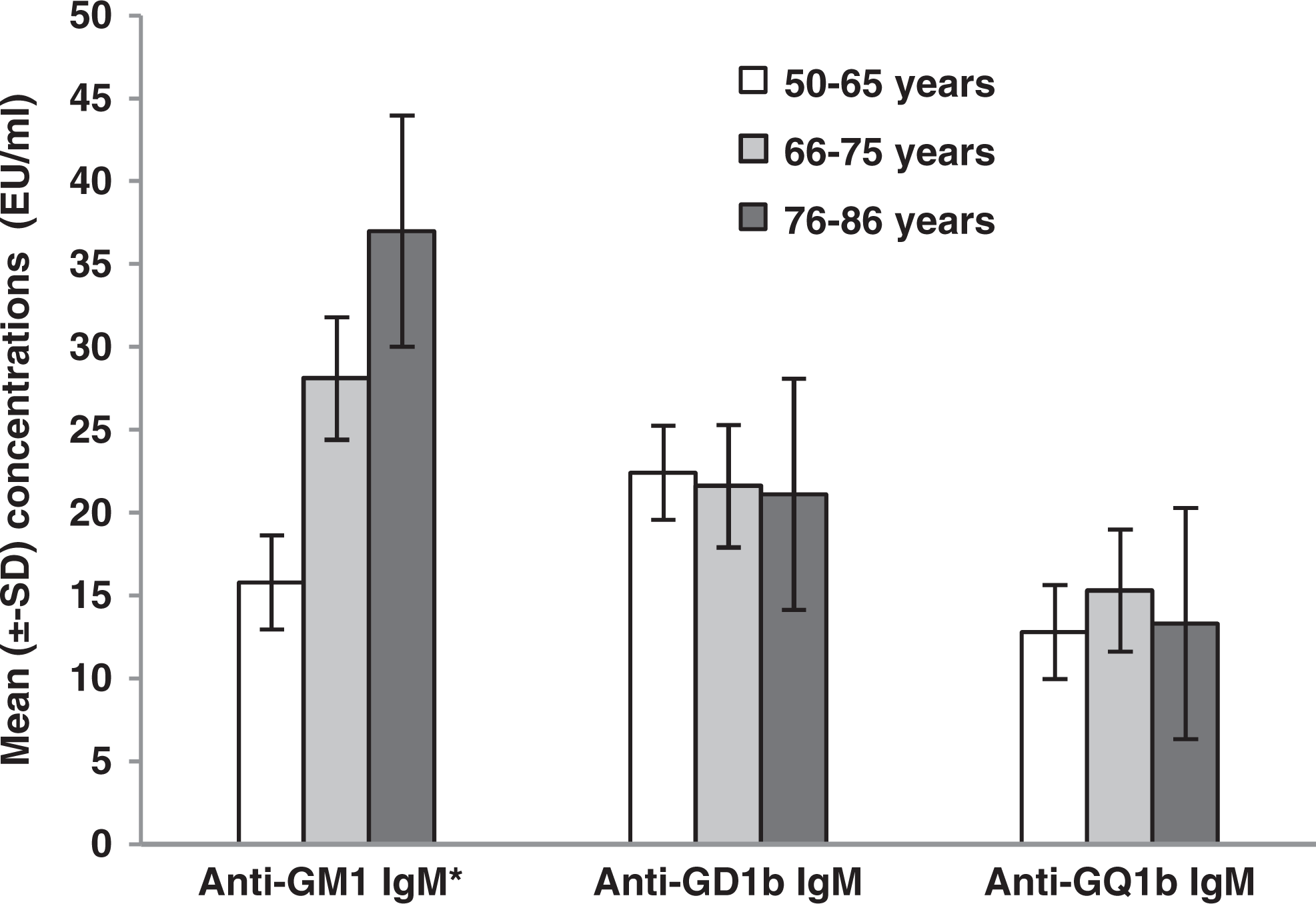
Comparison of the 3 antiganglioside antibodies with the age of the patients with dementia. Older patients (76-86 years) revealed higher levels of anti-GM1 IgM (F 2,101 = 30.6, P = .005 < .05).
Antiganglioside Antibodies Versus Age and Grade of Cognitive Decline of the Patients With Dementia.a
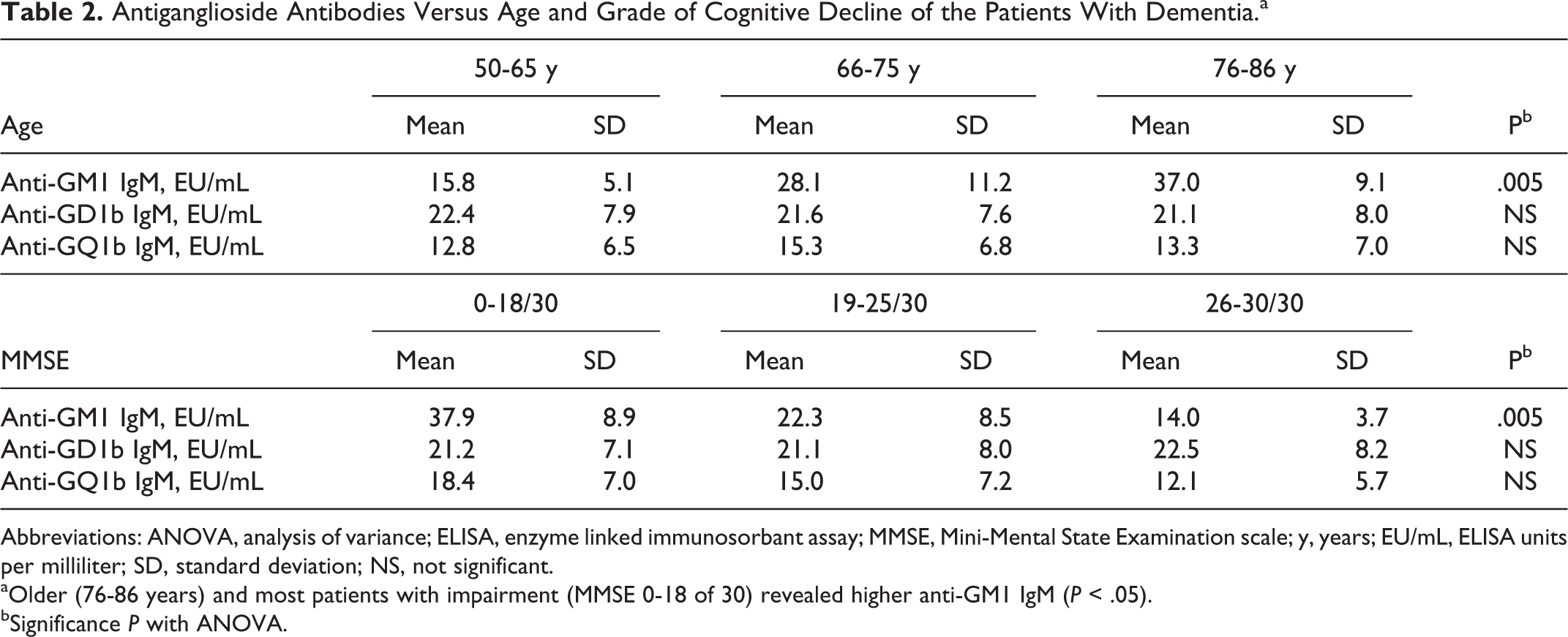
Abbreviations: ANOVA, analysis of variance; ELISA, enzyme linked immunosorbant assay; MMSE, Mini-Mental State Examination scale; y, years; EU/mL, ELISA units per milliliter; SD, standard deviation; NS, not significant.
aOlder (76-86 years) and most patients with impairment (MMSE 0-18 of 30) revealed higher anti-GM1 IgM (P < .05).
bSignificance P with ANOVA.
Comparison of the Antibodies Against GM1, GD1b, and GQ1b With the Grade of Cognitive Impairment
Based on the present results, most patients with dementia with scores of 0 to 18 of 30 in the MMSE scale revealed the highest levels of anti-GM1 IgM (mean 37.9 ± 8.9 EU/mL; F 2,101 = 83.3, P = .005 < .05; Table 2 and Figure 2).
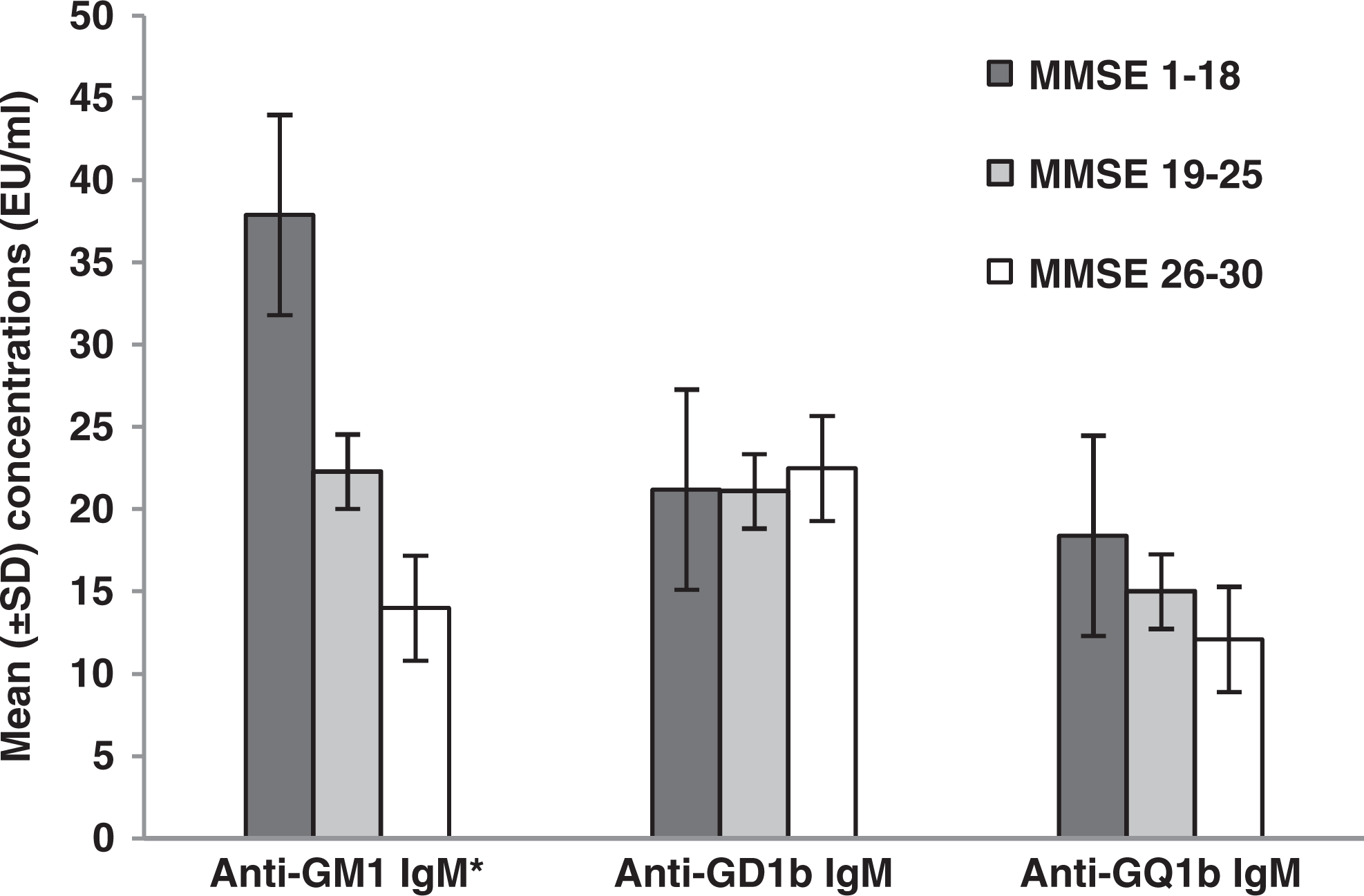
Comparison of the 3 antiganglioside antibodies with the grade of cognitive impairment of the examined patients. Most patients with dementia (MMSE 1 = 18 of 30) revealed the highest concentrations of serum anti-GM1 IgM (F 2,101 = 83.3, P = .005 < .05). MMSE indicates Mini-Mental State Examination; Ig, immunoglobulin.
Correlation of the Antibodies Against the Ganglioside GM1, GD1b, and GQ1b With the Types of Dementia
The patients have been separated into 3 groups according to the levels of antiganglioside antibodies (positive/negative/borderline). Due to the lack of cases, we excluded patients with LBDD and dementia due to depression (poststroke depression) from the statistical analysis.
There was an important difference between the levels of anti-GD1b in the sera of patients who had AD, MD, and VαD (F 4,99 = 4.46, P = .002 < .05). Patients with AD revealed the most increased concentrations of antibodies against the ganglioside GD1b (mean 27.4 ± 8.4 EU/mL), while patients with mixed dementia revealed a borderline concentration (mean 20.2 ± 7.3 EU/mL). Patients with vascular dementia had negative anti-GD1b IgM (mean 18.9 ± 6.1 EU/mL; Figure 3).
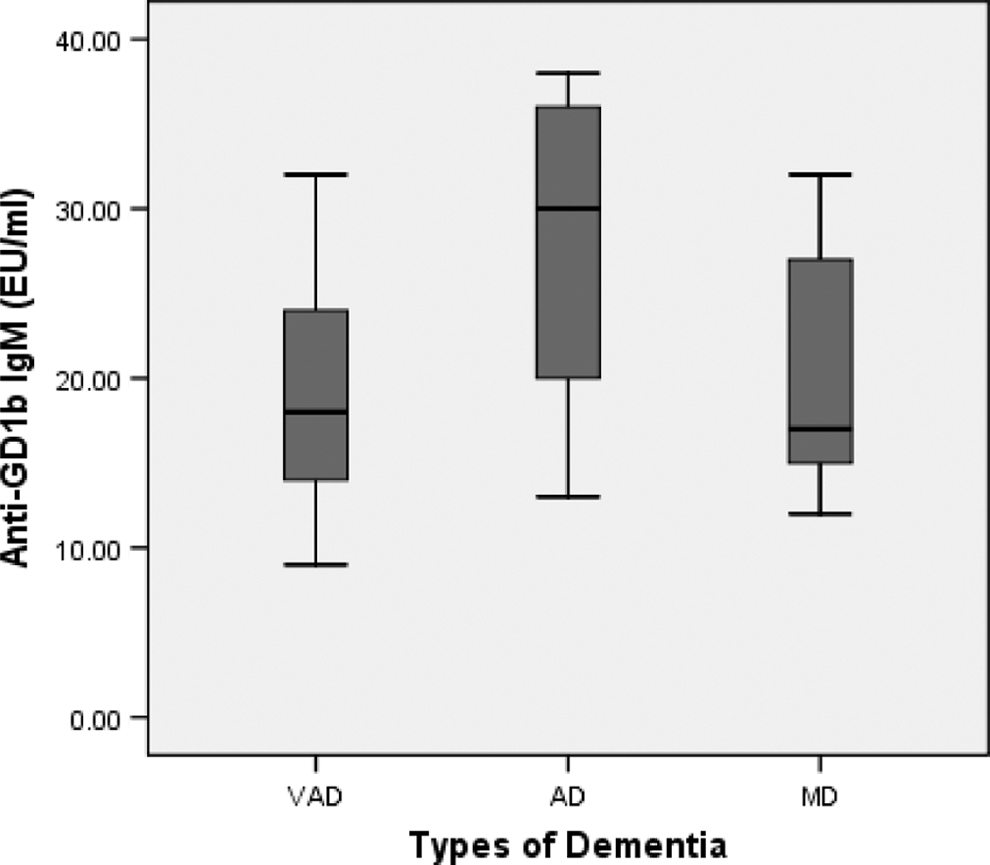
Comparisons of anti-GD1b IgM in patients with vascular dementia (VAD), mixed dementia (MD), and Alzheimer’s disease (AD). *Displayed are the mean (±SD) concentrations of anti-GD1b IgM that revealed an important correlation between VAD, AD, and MD. Patients with AD revealed the most increased concentrations of anti-GD1b IgM (27 EU/mL). There was a significant difference between increased anti-GD1b IgM and patients with AD (F 4,99 = 4.46,
Discussion
In the present research, we detected high levels of anti-GM1 IgM (37.7 ± 8.9 EU/mL) in the sera of 66% of the patients having several types of dementia mainly of VAD. In all, 35% of the patients had increased concentrations of anti-GD1b IgM (30.6 ± 3.7 EU/mL), whereas only 9% of them revealed high anti-GQ1b IgM (28.0 ± 5.7 EU/mL). However, healthy individuals demonstrated negative concentrations of the 3 antiganglioside antibodies. Both groups, patients (71.3 ± 8.5 years) and healthy controls (71.3 ± 7.4 years), were age matched. However, only the patients revealed higher concentrations of all the 3 examined antiganglioside antibodies (P = .0005). Our findings indicate the absence of high levels of antibodies in the sera of middle-aged to old healthy individuals (mean age ∼ 71 years) and second the possible correlation between anti-GM1 IgM and anti-GD1b IgM with the neurodegeneration presented in patients with dementia areprobably due to a stronger binding affinity of GM1 and GD1b gangliosides with the Aβ-peptide.
Previous studies also reported an increase of anti-GM1 in the sera of patients who had AD and also from other age-related dementias. 25 Chapman et al (2006) investigated the neurodegeneration in AD and have demonstrated the association with the presence of antiganglioside antibodies. Patients with AD revealed increased concentrations of anti-GM1 but not anti-GD1a, anti-GD1b, anti-GT1b, and anti-GQ1b, compared to age-matched healthy individuals. In addition, they mentioned high levels of anti-GM1 in the sera of patients with multi-infarct dementia and patients with Parkinson’s disease (PD) with dementia but not in nondemented patients with other degenerative disorders. 26 -28
The detection of anti-GM1 IgM in higher levels compared to the levels of anti-GD1b IgM and anti-GQ1b IgM may indicate the different binding affinity of Aβ-peptide to the 3 examined gangliosides. According to other researches, Aβ peptide (1-42) binds tightly to GM1, compared to the lower binding affinity for GD1b and GQ1b. 20-21
There have been several nuclear magnetic resonance (NMR) studies concerning the Aβ conformational changes. Based on NMR spectroscopic studies of Mandal and Pettergrew, 21 asialo-GM1 bound with Aβ peptide in a manner that could prevent β-sheet formation; ganglioside GT1b, however, did not show such a property.
They studied the interaction between gangliosides and Aβ-peptide, in a membrane mimic environment, dissolving the gangliosides asialo-GM1 and GT1b in sodium dodecyl sulfate solution. 21
Gangliosides present a hydrophilic oligosaccharide chain to which one or more sialic acids (N-acetylneuraminic acid) are attached and a hydrophobic ceramide, which binds the gangliosides to the plasma membranes. Gangliosides’ binding induces Aβ peptide oligomerization. The GM1 and GT1b have 4 sugar moieties in common; however, GT1b has 3 sialic molecules more compared to asialo-GM1 that doesn’t contain sialic rests. 29
According to this study, with the additions of sialic acid molecules, it is difficult to bind on the ganglioside-specific binding sites of Aβ-peptide. Asialo-GM1 and GM1 are able to bind Aβ and prevent the β-sheet formation by this binding. 21
Therefore, the loss of “protective” GM1 and the increase in “unprotective” GT1b during the aging 30 elevate the possibility of β-sheet formation and the resulting senile plaques. 29,31
Correlating the levels of the 3 investigated antiganglioside antibodies with the types of dementia, we found statistically significant association between anti-GD1b IgM and AD as well as with mixed dementia (P = .009) and vascular dementia (P = .004). Patients with AD revealed the most increased concentrations of anti-GD1b IgM (27.4 ± 8.4 EU/mL), indicating a probable correlation of these antibodies with the neurodegeneration.
In the present study, we also compared the levels of the 3 antiganglioside antibodies with the age of the examined patients. Based on the demonstrated results, patients older than 66 years revealed the most increased concentrations of anti-GM1 IgM (28.1 ± 11.2 EU/mL and 37.0 ± 9.1 EU/mL, respectively; P = .005). There was no statistically important association between age and anti-GD1b/anti-GQ1b IgM.
Correlating the severity of cognitive impairment with the levels of the 3 investigated antiganglioside antibodies; we detected a statistically significant association with the anti-GM1 IgM. Patients with dementia (MMSE 1-18 of 30) revealed the highest concentrations of anti-GM1 IgM (37.9 ± 8.9 EU/mL; P = .005), suggesting a probable correlation between anti-GM1 and neurodegeneration.
Additionally, we found that patients having PD with dementia demonstrated increased levels of anti-GM1 IgM (mean 33.3 ± 8.1 EU/mL; P = .003), as well as the patients having PD with a greater severity of the disease (UPDRS I > 4), strongly indicating the probable correlation of anti-GM1 IgM with neurodegeneration (P = .013).
Other researchers reported increased levels of anti-GM1 and anti-GD1b IgM in elderly patients with dementia. 1,32 Namely, anti-GM1 IgM seems to be connected to severe cognitive decline, announcing the initiation of activated neuroinflammatory process that results in demyelination and degeneration. Previous researchers have also demonstrated the pathogenic role of activated microglia and the resulting neuroinflammation in both AD and PD. 32 -34
The biological effects of gangliosides in several neurodegenerative diseases of the peripheral as well as of the central nervous system explain the interest of many researchers who propose them as possible therapeutics. In AD, the aim of the therapeutic strategies is to inhibit the aggregation of misfolded Aβ peptides into their neurotoxic forms.
The beneficial effects of intravenous treatment with GM1 was demonstrated in patients with AD. 35 -37 Neurotrophic factors and GM1 are used however only in experimental stage, as all the efforts highlight to prevent the formation of amyloid plaques.
The GM1-bound Aβ in blood is not able to cross the blood–brain barrier (BBB) and incorporate into plaques centrally. However, peripheral administration of GM1 may reduce amyloid aggregation in AD. 1 However, the difficulty is the low level of gangliosides that can enter into the brain (only 1% crosses the BBB). 38 For that purpose a synthetic GM1, known as LIGA-20, was used. Oral LIGA-20 seemed to protect neurons against the glutamate-induced neuronal death in mice 39 and without the side effects of glutamate receptors. All the above-mentioned researches refer to exogenous oral or intravenous administration of gangliosides especially of GM1.
The use of gangliosides as inhaled anesthetics could also be very interesting to investigate in the future. Previous studies demonstrate that the local anesthetics tetracaine and butacaine increased the fluidity of lipid dispersions, natural membranes, and intact ascites tumor cell membranes. The effect of the anesthetics appears to be due to an increased disordering of lipid structure. 40 Other evidence indicates that gangliosides can enhance the sensitivity of membrane lipids to the disordering effects of anesthetics, suggesting that the large ganglioside content of the outer leaflet of the lipid bilayer of neuronal membranes may render this membrane region unusually sensitive to anesthetic agents. 41
However, we need further studies in order to investigate the potential effects of inhaled gangliosides in the therapy of AD, at clinically relevant and safe concentrations.
In conclusion, our results indicate that older (>66 years) patients with dementia having moderate to severe cognitive decline revealed increased levels particularly of anti-GM1 IgM and anti-GD1b IgM and suggested a probable correlation between these antiganglioside antibodies and dementia as well as with the age. Additionally, we found a possible connection of anti-GD1b IgM antibodies with the type of dementia, since patients with AD revealed the most increased concentrations of anti-GD1b IgM. On the other hand, anti-GQ1b IgM did not seem to have any correlation with any clinical parameter at the present study.
Our results indicate antiganglioside antibodies (especially anti-GM1 and anti-GD1b IgM) in the serum of patients with dementia as probable biomarkers of neurodegeneration.
Footnotes
Acknowledgments
The present research was supported by the Greek Governmental Corporation of Bursaries (N5233).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Greek Governmental Corporation of Bursaries under the Grant N5233.