
Abstract
Frontotemporal dementia (FTD) is second only to Alzheimer’s disease in individuals younger than 65 years of age. Behavioral variant FTD (bvFTD) presents with nonspecific symptoms such as disinhibition, apathy, or emotional blunting. Although neuropsychological testing and structural neuroimaging are not very helpful in diagnosing bvFTD in its initial stages, newer quantitative structural methods and functional neuroimaging have better sensitivity and specificity. Ms L presented with blunted affect, disinhibition, impairments in insight, planning ability and social comportment, changed dietary habits, and episodes of mutism. Her brain magnetic resonance imaging was normal whereas her single-photon emission computed tomography (SPECT) pattern was consistent with FTD. Her clinical presentation was consistent with bvFTD yet both the symptoms and SPECT findings reversed after 2 years of follow-up. We suggest that Ms L had a reversible phenotypic and brain function equivalent of bvFTD. The case highlights the limitations of our diagnostic tools and the complex relationship between clinical symptoms, neuroimaging, and etiology.
Keywords
Introduction
Frontotemporal dementia (FTD) comprises a group of neurodegenerative disorders whose incidence is second only to Alzheimer’s disease in individuals younger than 65 years of age, with an estimated population prevalence of about 15 patients/100 000 between 45 and 64 years of age. 1 In the first few years after the onset, patients usually present with nonspecific symptoms such as behavioral disinhibition, apathy, emotional blunting, loss of sympathy or empathy, perseverative or compulsive behaviors, mental rigidity, and change in dietary habits. 1 Neuropsychological testing is neither sensitive nor specific in the initial stage of the disease. When present, cognitive deficits are identified in executive functioning and episodic memory. 1 Similarly, visual inspection of structural neuroimaging may not identify any brain changes initially or may show frontal, anterior temporal, and basal ganglia atrophy. Newer quantitative methods, such as voxel-based morphometry or cortical thickness mapping, are much more sensitive and specific in identifying FTD and differentiating it from other dementias 1 but are still unavailable for clinical purposes in most settings. Serial imaging shows progression of atrophy over time. Functional neuroimaging such as positron emission tomography or single-photon emission computed tomography (SPECT) shows reduced radiotracer uptake in the frontal and temporal lobes, is sensitive in identifying FTD, and is specific in differentiating it from other neurodegenerative diseases such as Alzheimer’s disease. 1 Usually, the disease follows a progressively deteriorating course that eventually leads to complete loss of functional ability and death. Here, we present a case where the initial symptoms and functional neuroimaging were consistent with behavioral variant FTD (bvFTD), yet both the symptoms and the functional neuroimaging findings reversed on follow-up.
Case Report
Ms L, a 45-year-old married white female with major depressive disorder, was admitted to our university hospital psychiatry unit twice, in August to September and again in October to November 2004.
Although being treated with venlafaxine, ziprasidone, and mirtazapine as an outpatient, Ms L complained of increasing depression, anxiety, pacing, stiffness, tremors, slurred speech, temporomandibular joint pain, abdominal cramps, and sleeping only 4 to 5 hours per night despite being prescribed zolpidem. Her outpatient clinician started decreasing her medications but due to concerns for the severity of her symptoms, Ms L was admitted to the inpatient psychiatry service from August 19, 2004 until September 27, 2004.
The patient lived with her husband for 20 years and their 2 adolescent children. She worked as a bookkeeper in the family business. Over the few months prior to admission, she had been unable to work because of poor concentration and depression. She described the relationship with her husband as lousy and said that her husband was threatening to divorce her if her condition did not improve.
Ms L had been hospitalized 3 years prior and once during the year of admission for similar symptoms of anxiety, pacing, depression, sweating, and increased energy. Three years prior, the patient had suicidal thoughts with a plan to cut herself with a knife although she did not complete this act because her husband stopped her. At that time she complained of auditory hallucinations which she described as “mumblings with no clear understanding of what the voices were saying.” She never had visual hallucinations.
Family history was significant for a maternal grandmother who had received electroconvulsive therapy (ECT), although her diagnosis was unknown, a paternal greatuncle with schizophrenia who completed suicide some years ago, and a brother and an uncle with possible alcohol problems.
Ms L did not smoke or drink. She denied any history of abuse. She was born in Hartford, Connecticut, and grew up in a neighboring town. She was a high school graduate and received a 4-year accounting degree. She described that, all her life, she had very few friends.
Medications on admission included cenestin 0.625 mg tablets orally every day, clonazepam 1 mg orally thrice a day, Ortho-Novum, and venlafaxine. Ms L had a history of hypertension. She had a minor motor vehicle accident in 2001 during which she injured her back. She denied any loss of consciousness or head trauma during the accident. She was allergic to codeine, sulfa medications, and environmental allergens. Physical examination was normal, except for jaw stiffness, rigidity, and cogwheeling in both her upper and lower extremities. Her blood pressure was 150/109, pulse 72, temperature was 98, and respiratory rate was 16. Neurological examination showed intact cranial nerves II to XII, motor, and sensory examination. Mental status examination showed Ms L to be alert and cooperative, with mild difficulty speaking due to jaw stiffness. She described her mood as sad and anxious. Her affect was anxious, restless, and constricted. Her thought process was logical and goal directed. Associations were normal. Her thought content was negative for auditory or visual hallucinations and suicidal or homicidal ideas. Her insight and judgment were impaired.
Shortly after admission, medical reasons for Ms L’s symptoms were ruled out. Pheochromocytoma was ruled out. Her thyroxine was elevated at 13.5 but after further evaluation, thyroid dysfunction was ruled out. Because of low estradiol, normal follicle-stimulating hormone, and luteinizing hormone, the endocrine service thought Ms L may have hypogonadotropic hypogonadism. The magnetic resonance imaging (MRI) of the brain with pituitary protocol showed no pituitary mass or adenoma and was unremarkable overall. She was scheduled for outpatient follow-up at the endocrinology clinic.
On the inpatient unit, Ms L was anxious, paced around, though at times she played cards, and interacted with others. As Ms L’s anxiety and depression persisted despite medication treatment, the option of ECT was discussed with her and her husband. Right unilateral ECT at the rate of 3 treatments weekly was started on September 07, 2004, and continued until discharge. Venlafaxine was tapered and discontinued. Clonazepam and valproic acid were briefly tried but discontinued in preparation for ECT. She was started on lorazepam and sertraline.
Ms L displayed a number of bizarre behaviors in the hospital. On September 10th, she was lying in bed, appeared to understand what was being said to her but could not or would not speak. She was given a 1 time dose of Ativan 2 mg to test for catatonia but continued being mute. On September 12th, she was again mute, wandered around the unit picking up staff telephones and grabbing staff members’ food. Eventually, she admitted to the treating physician that she heard voices telling her not to speak. She denied hearing any command or self-deprecating hallucinations. She was treated with quetiapine up to 1000 mg/d but the auditory hallucinations persisted. Her verbal output and interaction with others fluctuated over time. Even when answering questions, there was a long latency of responses. With continued ECT, her symptoms improved—she appeared less bizarre, less anxious, less depressed, and more engaged with staff and fellow patients. During a second family meeting on September 27, 2004, her husband felt that she had improved substantially. She was discharged to the partial hospital program the following day, with continued outpatient ECT treatment twice per week.
Ms L’s discharge diagnoses were major depressive disorder, recurrent, severe, with psychotic features, anxiety disorder, not otherwise specified, dependent personality traits, nocturnal paroxysms, jaw stiffness, temporomandibular joint pain, and hypertension. Discharge medications were Cenestin 0.625 mg every day, Ortho-Novum 1 tablet every day, quetiapine 500 mg twice a day, sertraline 150 mg every day, propranolol 20 mg thrice a day, and zolpidem 10 mg orally qhs prn insomnia.
While at the partial hospitalization program, Ms L continued to display a number of bizarre behaviors. She wandered through the cash registers of the hospital cafeteria without paying and grabbed food from the grill and ate it. At times, she ate voraciously, without stopping. She ate before ECT, without explanation. She arrived to ECT without her shoes. She denied feeling depressed. She reported sleeping 8 hours each night, described an increase in appetite. She reported gaining 7 pounds over 3 weeks. She was not sure whether her concentration was impaired. She denied further auditory or visual hallucinations. She denied a lack of interest or helplessness. She reported that her energy was good. She denied suicidal or homicidal ideation. Because of her bizarre behaviors, she was readmitted to the medical psychiatry inpatient unit.
During the second admission examination, Ms L exhibited significant psychomotor retardation. Her speech was nonspontaneous but with normal rate and volume. She reported that her depression had gotten better with treatment. Her affect was blunted and guarded. Her thought process was slow, somewhat concrete. She did not elaborate on subjects and gave vague answers. Her short-term memory was intact. Abstraction was good. Her concentration was good. Insight and judgment were poor regarding the recent history of bizarre behavior.
Throughout this second admission, the patient denied feeling depressed. She attended groups, spent much time in the TV room, and remained socially interactive. Her affect remained blunted. She received additional medical workup and an evaluation for possible dementia was done.
Urine toxicology was negative, and laboratory studies including calcium, magnesium, and phosphate, were normal. Rapid plasma reagin was nonreactive. Lyme titers were negative. Prolactin level was within normal limits at 41.37. Antinuclear antibody (ANA) was positive, with titer of 1:40, in a homogeneous pattern. Rheumatology consult concluded that the abnormal ANA was not clinically significant, there was no evidence for cerebral lupus or vasculitis, and that no further testing was needed. A follow-up endocrine consult concluded that hypogonadotropic hypogonadism could not be diagnosed while the patient is on birth control pills. Urinary 24-hour free cortisol was 30.8, within the normal range (normal less than 45).
A functional occupational therapy assessment done on October 25, 2004, concluded that the patient can live independently with assistance in planning and organization.
A SPECT scan was obtained to further assess the possibility of a neurodegenerative disorder (see Figures 1 and 2, left side). The SPECT revealed mildly to moderately compromised perfusion of the mid-region of the anterior frontal lobe, extending into the prefrontal lobe, bilaterally, possibly due to an early degenerative process, Pick's disease, depression, and so on. There were 2 small subsegments of decreased perfusion noted within the right relative to the left temporal parietal cortex. The significance of this latter finding was uncertain. Perfusion within the remaining temporal lobes, parietal cortex, subcortical structures, and cerebellum was within normal limits.
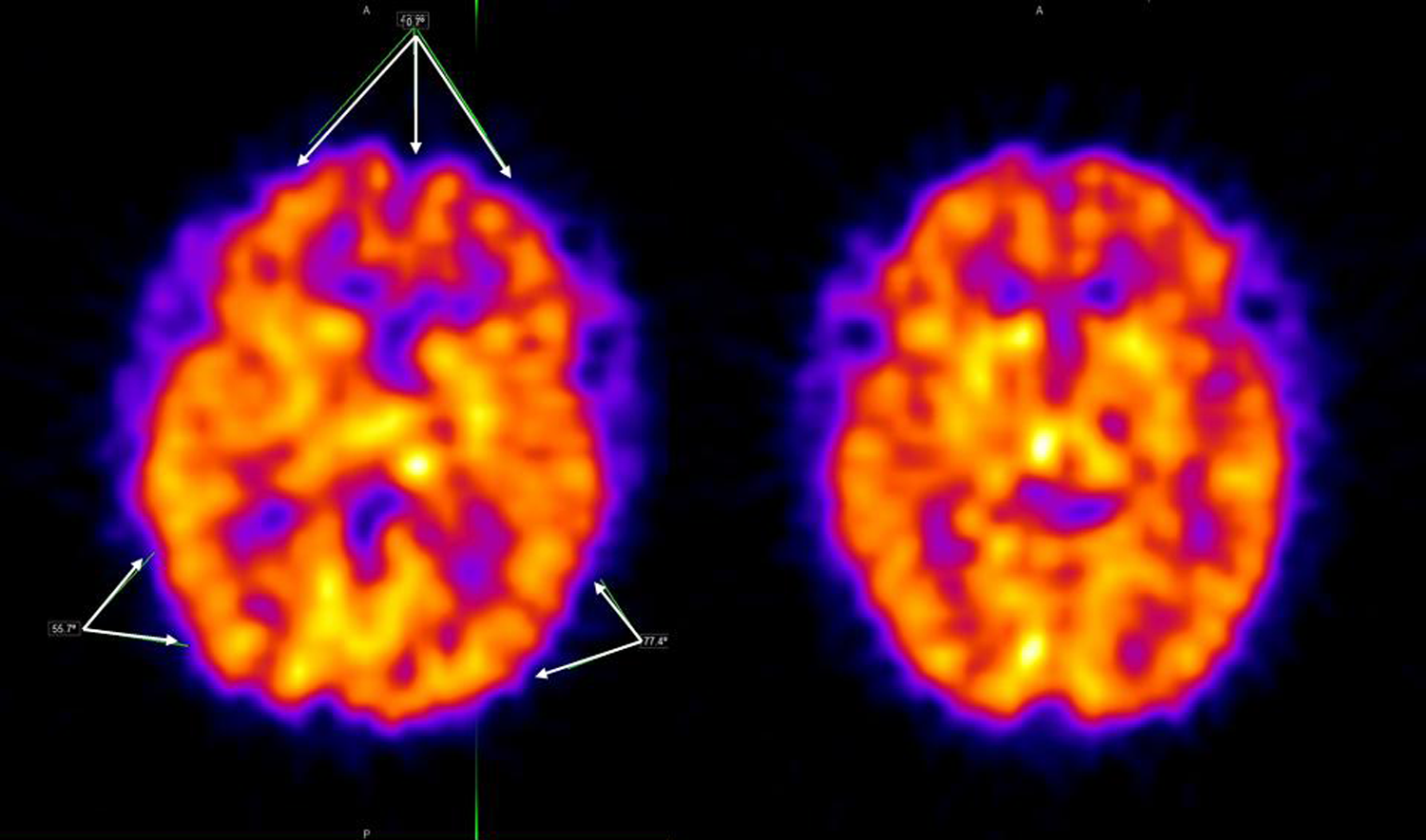
2004 axial SPECT images (left side) showing hypoperfusion in bilateral frontal lobes and in the right and probably in the left temporoparietal cortices (arrows). 2006 axial SPECT images (right) showing resolution with normal perfusion throughout the cortex. The SPECT images were acquired with special neurofocal collimation and corrected for attenuation. SPECT indicates single-photon emission computed tomography.
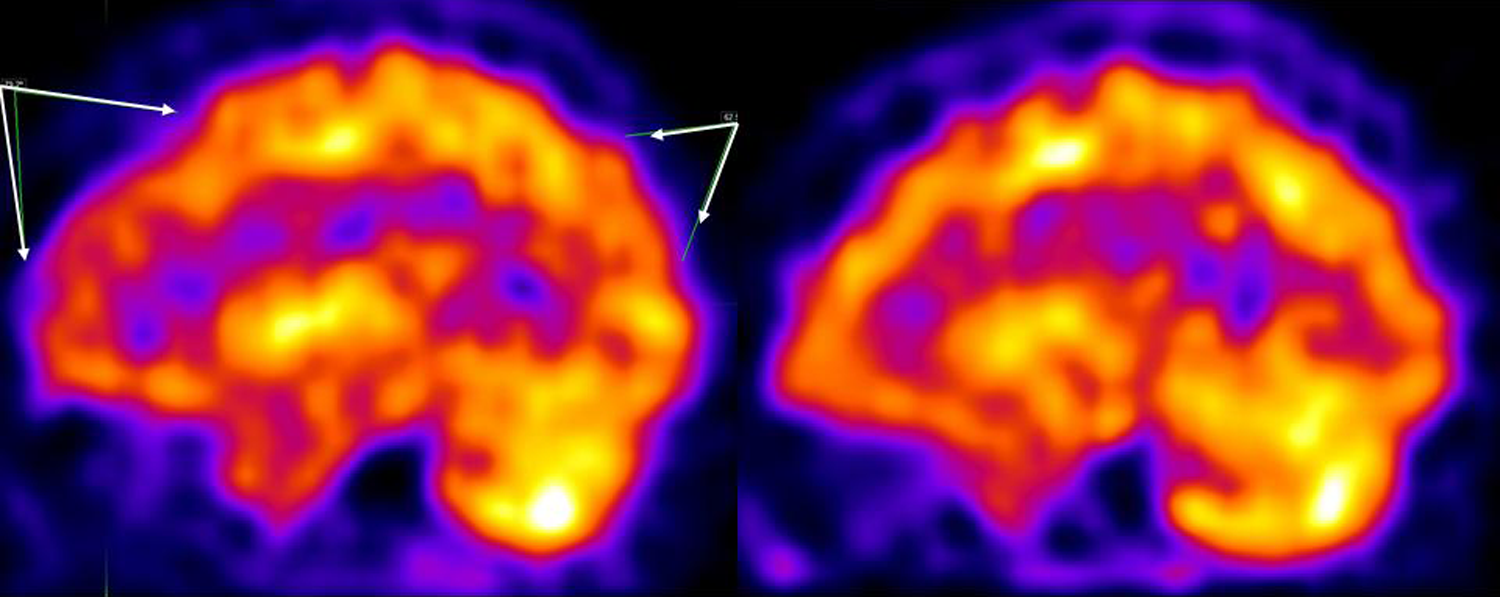
2004 sagittal SPECT images (left side) showing hypoperfusion in the right hemisphere frontal lobe and in the right temporoparietal cortex (arrows). 2006 sagittal SPECT images (right) showing resolution with normal perfusion in the same areas. The SPECT images were acquired with special neurofocal collimation and corrected for attenuation. SPECT indicates single-photon emission computed tomography.
During this hospitalization, quetiapine was tapered as it was thought it may be contributing to Ms L’s concentration problems. Bupropion was added at 75 mg q
By the end of the hospitalization, Ms L stated that she felt better, denied any symptoms of depression or anxiety and denied any suicidal or homicidal ideation. Her husband also felt that she was doing better. She was discharged on November 3, 2004.
Ms L’s discharge diagnoses after her second hospitalization were provisional dementia of the frontotemporal type with behavioral disturbance, major depressive disorder, recurrent, severe with psychotic features, rule out seasonal (summer) exacerbation, hypertension, temporomandibular joint syndrome, rule out hypogonadotropic hypogonadism, and minor motor vehicle accident in 2001 with no head injury or loss of consciousness. Discharge medications included sertraline 150 mg orally every day, propanolol 20 mg orally thrice a day, Modicon 1 tablet daily, quetiapine 200 mg orally twice a day with a recommendation to taper this medication, bupropion 75 mg orally q
Over the following 4.5 years, Ms L was followed by the first author in the outpatient neuropsychiatry clinic. Her clinical status did not substantially change. She continued reporting good mood and did not have a recurrence of depression. Her neurovegetative functions were good. She presented with euthymic but blunted affect. Over the course of the first 2 years of outpatient follow-up, her affect became less blunted and by the end of 2 years it was bright and stable. The patient’s speech was sparse, with normal rate and rhythm. Her thought process was logical and, while initially her ability to generate ideas was diminished, her thought flow improved by July 2005. Her thought content was without any of the psychotic symptoms she had experienced during her hospitalization. Throughout the time of her follow-up, she was consistently oriented to person, date, and place. The patient’s attention was adequate—she was able to spell “radio” forward and backward, repeat 7 digits forward and 5 backward. Her word generation improved over time—while in December 2004 she generated 11 “F” words and named 25 animals in 1 minute each, in April 2005 she generated 21 “F” words and named 26 grocery items in 1 minute each. Her short-term memory remained good throughout the follow-up period—she registered 4 of the 4 objects and remembered 4 of the 4 spontaneously after 5 minutes. Her long-term memory for baseball facts was excellent. Praxis was good—she was able to pantomime blowing out a candle, saluting like a soldier, or combing her hair on verbal command. However, she had difficulty in performing the Luria 3-step motor sequence (“fist-straight-flat”). In December 2004, she was unable to perform it after verbal instruction but was able to imitate it after a demonstration. In April 2005, she was able to do it after verbal instruction only, albeit with difficulty. Her abstraction ability was good throughout—she interpreted both learned and novel proverbs abstractly. She complained of increased sweating independent of the ambient temperature, which decreased over time but remained a symptom over the entire follow-up. She restarted working as a bookkeeper in her husband’s computer business 2 days/week. When her husband’s company moved, she applied for and was accepted as a full-time bookkeeper at another company. She was active, exercised several times per week.
Because Ms L’s clinical status, memory, judgment, and functional ability improved, we decided to repeat the SPECT scan (see Figures 1 and 2, right side). In March 2006, her repeat SPECT showed normal perfusion throughout the frontal, parietal, and right temporal lobe cortex, with mild hypoperfusion in the mid to anterior segment of the left temporal lobe cortex. Thus, the previously mildly to moderately compromised perfusion in the anterior frontal lobe, as well as that in the right temporoparietal cortex, was now within normal limits. The mild hypoperfusion within the left temporal lobe cortex was interpreted to be of questionable significance and likely within normal range. Perfusion within the subcortical structures (basal ganglia and thalamus) and cerebellum was normal.
Because the SPECT imaging results contributed significantly in validating the patient’s clinical symptoms and influenced our diagnostic impression, we will provide some detail on the SPECT’s technical aspects. The same radiopharmaceutical, Tc-99m-Ceretec (hexamethylpropyleneamine oxime [HMPAO]), was used for both studies. The dose that was administered was 28 to 30 mCi, within 10% between both studies. An intravenous line was placed, and HMPAO administered 5 minutes after its placement in a dimly lighted room. Acquisition of the images was started 45 minutes post the HMPAO injection. Neurofocal collimation was used, which increases sensitivity and magnification. There were a total of 120 projections, which equals 3° for each image set. The minimum data that were collected were 120 000 counts per image set, which is important for statistics. The acquisition radius was 13 to 13.5 cm, which is important for resolution. If needed, data were corrected for motion artifact. Image reconstruction was performed with filtered Back-Projection Butterworth Filter (Siemens). All images were corrected with Chang's attenuation. Realignment was done when needed. Both imaging results were read by the same nuclear medicine radiologist (the second author) and discussed with another nuclear medicine physician from the same department, as it was customarily done in the nuclear medicine department of our university.
We discussed the significance of the results with Ms L and her husband. Due to the patient’s functioning and the normalization of the SPECT results, we considered that FTD was no longer a possibility and that the patient had MDD, recurrent, severe, with psychotic features, currently in remission.
We attempted to taper her quetiapine, however, upon stopping it she experienced headaches during the day which stopped when she restarted it. The addition of glycopyrrolate for her sweating was discussed but was never started. Patient’s medications of last contact (February 2009) were bupriopion 75 mg q 7
Discussion
Symptoms at presentation were consistent with those seen in early FTD—bvFTD 1,2 or frontal variant FTD. 3 –5 Our patient was in her 40s, fitting a typical age at onset of FTD. Ms L presented with changes in personal and social comportment, disinhibition, and change in dietary habits—grabbing staff telephones, showing up at ECT without shoes, showing up at ECT having eaten, and grabbing food in the hospital cafeteria. Her affect was blunted. Although her language was preserved, she had periods of mutism. She had little insight into her actions. Ms L’s behavioral disturbances persisted after her depression and her neurovegetative signs had resolved. Ms L’s planning ability interfered enough with her daily routine that an occupational therapy function assessment recommended that she live in the community with supervision. Ms L’s structural MRI scan was normal whereas her SPECT scan was abnormal with a pattern consistent with an early neurodegenerative disease, such as FTD, or with depression. The SPECT scan was taken after she no longer felt depressed and after her neurovegetative functions had improved. Functional neuroimaging in general, and SPECT in particular, have been shown to be sensitive to early changes in FTD 1,3 and to be specific in differentiating FTD from Alzheimer’s disease. 3,6 Changes in cerebral blood flow (CBF) are not unique to neurodegenerative disorders as they can also be observed in psychiatric syndromes such as depression. However, CBF patterns are distinct in depression and dementia. Cho et al studied the SPECT patterns of 4 groups of patients—patients with depression having cognitive impairment, patients with depression without cognitive impairment, normal controls, and patients with Alzheimer’s disease. 7 Patients with depression had significantly decreased CBF in the left frontal region compared with healthy controls. Patients with depressive pseudodementia had significantly decreased CBF in both parietal regions compared with healthy controls. Patients with depressed pseudodementia also had significantly decreased CBF in the right temporal and both parietal regions compared with patients with depression without dementia. Patients with Alzheimer’s disease showed significantly decreased CBF in the right frontal, right temporal region, and both parietal regions compared with healthy controls. Patients with Alzheimer’s disease also had significantly decreased CBF in the right temporal region, both frontal regions, and both parietal regions compared to patients with depressive pseudodementia. Finally, patients with depressive pseudodementia had decreased CBF in the temporoparietal region, similar to that of the patients with Alzheimer’s disease and different from that of the depression group. 7 Additionally, CBF changes in depression do not seem to correlate with neuropsychological dysfunction. 8
Results of patient’s SPECT scan were consistent with her clinical presentation. The frontal lobes were the main site of decreased perfusion, and her behavioral syndrome comprised impaired impulse control, disinhibition, restriction of affect, poor judgment, and impaired social comportment. The persistence of the clinical symptoms beyond the period of depressive symptoms, in conjunction with her functional neuroimaging results, made us consider bvFTD as the etiology of her symptoms. According to the international consensus criteria for the diagnosis of bvFTD, she would meet criteria for probable bvFTD based on the clinical symptoms consistent with bvFTD, significant functional decline, and frontal hypoperfusion on SPECT 9 (Tables 1 and 2). Her subsequent symptom improvement and resolution of CBF changes in the follow-up SPECT proved that conclusion is wrong.
Ms L’s Symptom Fit to the Clinical Criteria for Establishing the Diagnosis of Frontotemporal Dementia. 2
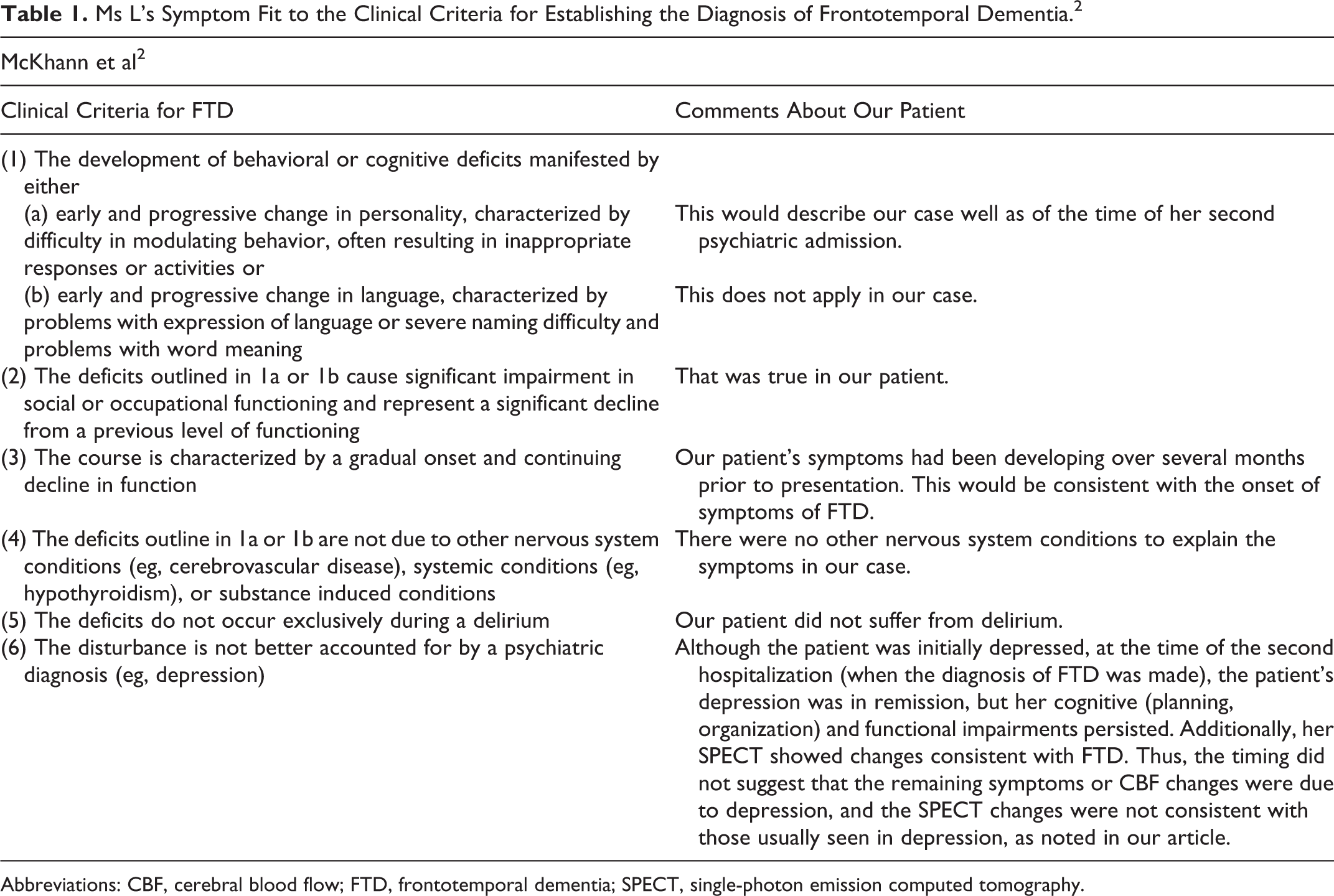
Abbreviations: CBF, cerebral blood flow; FTD, frontotemporal dementia; SPECT, single-photon emission computed tomography.
Ms L’s Symptom Fit to the International Consensus Criteria for Establishing the Diagnosis of Frontotemporal Dementia, Behavioral Variant (bvFTD). 1
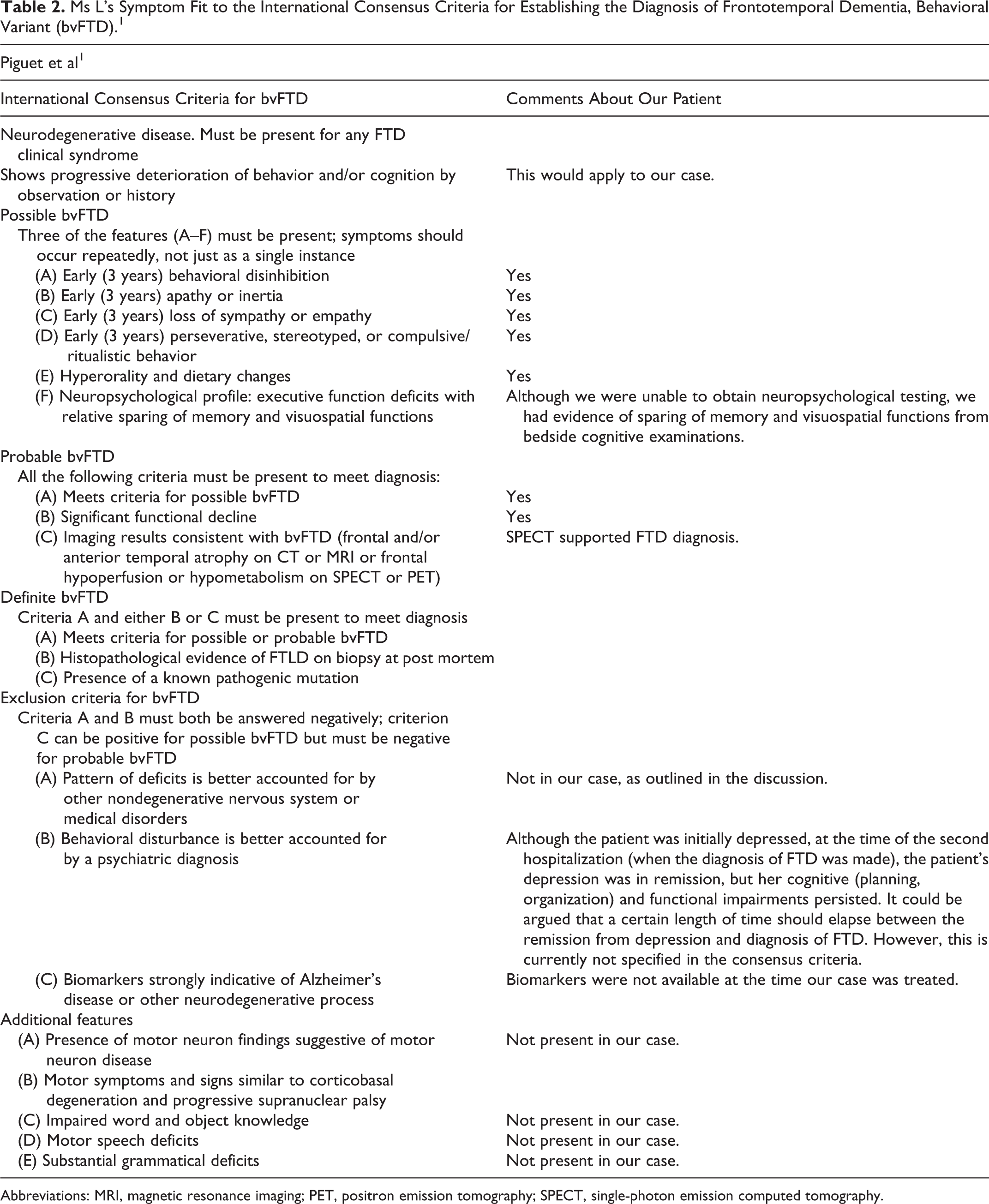
Abbreviations: MRI, magnetic resonance imaging; PET, positron emission tomography; SPECT, single-photon emission computed tomography.
Our investigation was limited by the fact that we were not able to obtain neuropsychological testing; however, standard neuropsychological testing is neither sensitive nor specific to FTD. 1 Therefore, had we obtained one, it would not have substantially supported or refuted the possibility that Ms L had FTD. We did not do any quantitative measurement of the patient’s structural MRI, which at the time of her treatment was not available to us. Also, we did not check CSF biomarkers, which at the time were not available. 1 Although cases of stagnant or reversible symptoms that initially mimic FTD (the bvFTD phenocopy syndrome) have been described, our case has some important differences. In bvFTD phenocopy, most patients are men, the clinical syndrome is that of bvFTD, the patients do not deteriorate or even improve over time, have normal or near-normal executive functions, have no signs of atrophy on structural neuroimaging, and have normal functional brain imaging. 1 In contrast, our patient is a woman, had significantly impaired planning ability, and abnormal SPECT scan.
We suggest that Ms L had a reversible phenotypic and brain function equivalent of bvFTD. This is important, since ultimate diagnosis of FTD relies on the combination of clinical symptoms and postmortem neuropathological findings, 1,2 and brain biopsies are not routinely carried out to diagnose dementia in a living person. Recently, novel quantitative neuroimaging techniques and CSF biomarkers have increased the sensitivity and specificity of our clinical tools. However, histopathological evidence of FTLD at postmortem brain biopsy remains 1 of the 2 threshold criteria for a diagnosis of definite bvFTD (the other one is the presence of a known pathogenic mutation). Without these criteria, we cannot definitively distinguish between the early stage of a neurodegenerative process and functional brain equivalents that are not neurodegenerative in nature. Reversible dementias have been described as a result of depression, 7 vitamin or mineral deficiencies, 10 infectious etiologies, intracranial lesions, 11,12 and others. However, this is the first report of which we are aware describing a patient presenting with a complex FTD clinical syndrome with functional neuroimaging supporting that diagnosis in which the patient’s clinical symptoms and functional neuroimaging subsequently improved. It is important in that it shows the complex relationship between clinical symptoms, neuroimaging, and etiology.
Although in principle the diagnosis of any progressive neurodegenerative disorder including FTD should be one of the exclusion of reversible causes of disease, the frontline clinician does not have the luxury of knowing the final outcome when making the clinical diagnosis of FTD. At best, the clinician can rely on consensus criteria to accurately classify the patient into categories of possible, probable, and definite FTD. According to these consensus criteria, our patient would have been classified as “probable FTD.” However, the consensus criteria may have to be further refined to increase their accuracy in identifying true FTD. One FTD criterion that may need to be reconsidered is the amount of time that needs to elapse between the resolution of a possible contributor to reversible FTD-like presentation (such as depression) and the diagnosis of a possible neurodegenerative disorder. Out tools have limitations. We have to keep in mind the possibility that, despite good clinical investigation, the processes we observe may evolve differently and have different etiology than we expect. This understanding of our limitations is important when educating and setting expectations for patients and their families.
Footnotes
Authors’ Note
Dr Tanev collected and interpreted the clinical data, drafted, and edited the manuscript. Dr Vento collected and interpreted the imaging data and edited the imaging part of the manuscript. Both the coauthors approved the final version of the manuscript as submitted for publication. Single case reports, in the opinion of the University of Connecticut Health Center IRB, are not “systematic investigation designed to develop or contribute to generalizable knowledge” and therefore do not require approval by the board.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.