
Abstract
Background:
Apolipoprotein E (ApoE) ∊4 genotype is the most clearly documented risk factor for Alzheimer’s disease (AD). Epidemiological studies demonstrate an accelerated rate of progression to dementia and AD in patients with mild cognitive impairment (MCI). We assessed the ApoE allele and genotypes frequencies in Cuban patients with MCI.
Methods:
We performed ApoE genotyping of 74 Cuban patients more than 65 years old. Cognitive assessments included the Mini-Mental State Examination (MMSE) and a cognitive battery for evaluating memory, attention, perception, and executive function.
Results:
Cognitive impairments were characterized by amnesia and executive deficits in patients with MCI. The Apo ∊4 allele frequency was 0.196 in patients with MCI, 10-fold higher than that in the controls. Patients carrying the ∊4 allele exhibited poorer performance in MMSE and tests assessing executive function and short-term memory than noncarriers.
Conclusions:
The patients exhibited amnestic MCI multiple domains. Cognitive performance was worse in patients who carried the ApoE ∊4 allele.
Introduction
Mild cognitive impairment (MCI) is a syndrome that includes a set of cognitive disabilities atypical for age and educational level of patients without dementia. 1 –6 Individuals with MCI diagnosis have Alzheimer-type dementia at a higher frequency than the cognitively normal population. Consequently, Alzheimer’s disease (AD) and MCI might have a common genetic basis. Individuals could progress to dementia, have only MCI, or show an improvement in their condition. On average, 10% of individuals having MCI progress toward a form of dementia. Of these, 90% develop an Alzheimer-type dementia with an annual conversion rate of around 9% to 12%. 2,5,7
This conversion rate contrasts with that observed in the cognitively normal population, which is around 1% to 2%. 2,8 It is generally thought that the population diagnosed with MCI includes a heterogeneous group of individuals compared to the general population and are at increased risk of developing dementia. 1,9 Some authors suggest that patients with MCI and significant memory impairment (amnesic) in single or multiple domains (mds) represent a prodromal form of AD. 1,3 Recently, Albert et al defined diagnostic criteria for identifying the preclinical stage or symptomatic predementia phase of AD, using the term “MCI” due to AD. 4
These reports suggest that amnestic MCI (aMCI) 1 or MCI due to AD 4 and AD could have a common genetic basis. The apolipoprotein E (ApoE) gene has been associated with the sporadic form of late onset of the disease in a dose-dependent manner. 10 For that reason, correspondence between the particular genotypes of the ApoE gene and the cognitive profile of the individuals has been a topic of interest. 11 –14
In some studies, the ApoE ∊4 allele was found to be associated with deficits in cognitive performance in elderly healthy participants 11,12,15 as well as in patients with MCI. 13,14 An association of the ApoE ∊4 allele with dementia in the older Cuban population 16 and Cuban Americans has been reported, 17 but to the best of our knowledge, the possible association of ApoE ∊4 allele with cognitive deficits in Cuban patients aged 66 years and older has not been assessed. In the present study, ApoE was genotyped in patients between 66 and 85 years old with previous diagnosis of MCI. We assessed the patients using a battery of neuropsychological tests for examining different cognitive domains: memory, executive function, perception, visual/spatial process, and praxis. Our results suggest that the ApoE ∊4 allele is related to worse performance in cognitive function in patients with MCI.
Materials and Methods
Participants
Unrelated 46 patients with MCI diagnosis and 28 cognitively normal control participants more than 65 years old were randomly selected from the pool of recruited patients in “The Cuban Dementia and Alzheimer’s Study Playa (EDAP),” Havana City. 18 Written informed consent was obtained from patients, their corresponding informants, and control participants. The research protocol was approved by Cuban Neurosciences Center Ethic Review Board and the Ethic Committees of National Program for Attention to Disabled Persons.
The control sample consisted of patients neurologically and psychiatrically normal and without any cognitive deficit. All patients met the diagnosis of MCI according to the Petersen’s criteria 1 and included the following features: (1) a complaint of defective memory corroborated by an informant; (2) normal activities of daily living; (3) a deficit documented by performance on a battery of neuropsychological tests; and (4) absence of dementia according to the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) criteria for the dementia syndrome.
Exclusion criteria were thyroid diseases, vitamin deficiencies (B12), mental diseases, depression, substance abuse, or significant neurological or psychiatric antecedents. All participants had a normal clinical neurological examination. Blood samples, for DNA extraction and ApoE genotyping, were obtained from all patients and control participants.
Demographic variables of the the participants enrolled in this study are given in Table 1. The age of the participants was between 66 and 83 years, with a mean of 73.3 ± 4.1 years. There were no significant differences between participants belonging to control and MCI in age mean, sex, or race (P = .05). The educational level was however different between the 2 groups of participants (P[t] = .003; Table 1).
Demographic Variables of the Selected Participants.
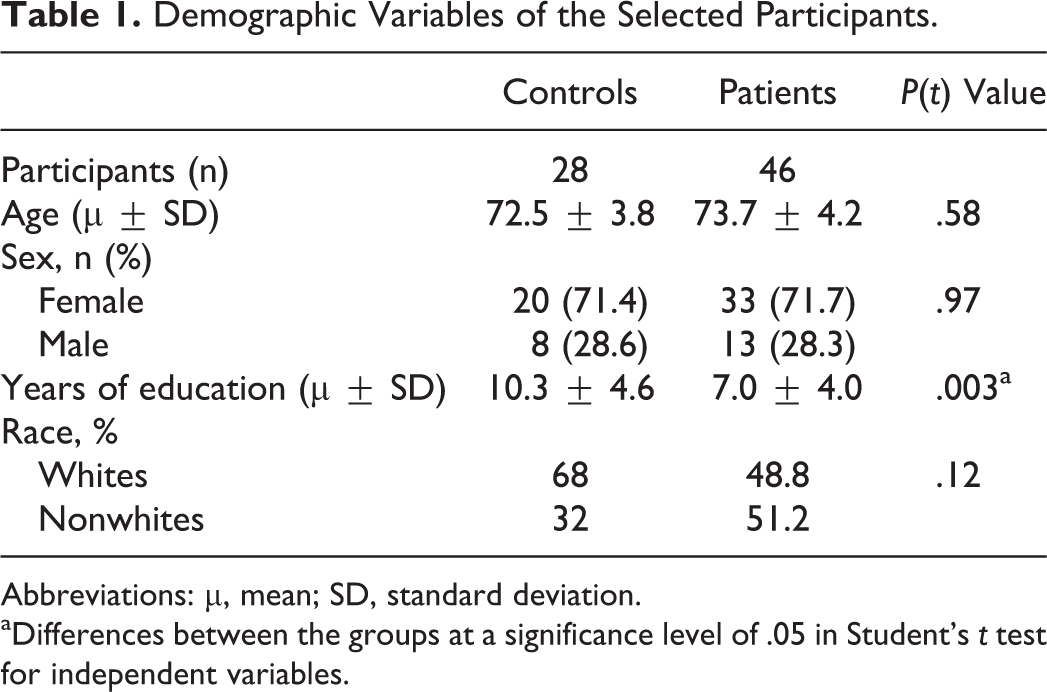
Abbreviations: μ, mean; SD, standard deviation.
aDifferences between the groups at a significance level of .05 in Student’s t test for independent variables.
Cognitive Tests
Neuropsychological evaluation of controls and patients was conducted by a neuropsychologist by means of a battery that included Mini-Mental State Examination (MMSE) and clinical dementia rating (CDR) scale. The battery also included tests for assessing the long-term memory (Word List Delayed Recal 19 and Rey Figure Delay Recall 20 ), the short-term memory (Digit Span 21 and Spatial span Corsi blocks 22 ), and other cognitive functions (attention, perception, executive function, praxis, and language) by means of token test, 23 Street’s completion, 24 verbal fluency (phonological), 25 trail making B-A, 26 attention matrix, 27 and constructional apraxia test. 28 We used the raw scores of the tests for performing the analyses because this neuropsychological battery is not normalized for Cuban population.
Procedure
Apolipoprotein E Genotyping
DNA molecules isolated from blood samples using genomic DNA purification kit (GFX; Amersham Biosciences, Argentina, S.A.) or from nonenzymatically treated immobilized blood in agarose gel 29 were used as template in the polymerase chain reaction (PCR). The fragment of 227 bp of ApoE gene was amplified using the oligonucleotide primers forward: 5′TCCAAGGAGCTGCAGGCGGCGCA3′ and reverse: 5′ACAGAATTCGCCCCGGCCTGGTACACTGCCA3′. 30 In the thermal reactor (Eppendorf Mastercycler, Eppendorf AG, Hamburg, Germany), an initial denaturation at 94°C for 5 minutes was followed by 40 cycles of denaturation at 94°C for 1 minute, annealing at 65°C for 30 seconds, and extension at 72°C for 1 minute, with a final extension at 72°C for 10 minutes. 30 Each reaction tube contained the 5 μL of DNA (GFX) plus 5 μL of 10× PCR buffer (100 mmol/L Tris-HCl, pH 9; 15 mmol/L MgCl2 and 500 mmol/L KCl; Amersham Biosciences, Argentina, S.A.), 50 pmol of each primer, 0.2 mmol/L of each deoxynucleotide, 5 μL of dimethyl sulfoxide, and 2.5 units of Taq DNA polymerase (Amersham Biosciences, Argentina, S.A.) in 50 μL final volume. PCR reaction mixture of 25 μL was incubated with 5 units of Hha I for 4 hours at 37°C and subjected to acrylamide 10% gel electrophoresis for ApoE genotyping. 30
Deviation from Hardy-Weinberg equilibrium was checked for ApoE genotypes. 31 Odds ratio value and 95% confidence intervals (CI95%s) for ApoE ∊4 allele were calculated. 32
Statistical Analyses
SAS Version 7.0 for Windows (SAS Institute Inc, Cary, North Carolina) was used for statistical analyses. The significance level was 0.05. Continuous variables (age and years of education) were compared through a Student t test for independent samples, while the dichotomous variables (race and sex) were compared using the chi-square (χ2) test.
Differential effects of diagnosis or ApoE ∊4 allele on each neuropsychological raw test scores were screened using analysis of covariance, adjusting the values by age and years of education, according to the general lineal model:
The multivariate analysis of the effect of ∊4 allele in the patient group with MCI or the diagnosis on the cognitive profile (considering all tests included in the neuropsychological battery) was performed using the Wilks test.
Results
Apolipoprotein E Allele and Genotype Frequencies in Patients With MCI and Controls
The ApoE genotypes and allele frequencies for patients with MCI and control participants are shown in Table 2. The sample was in Hardy-Weinberg equilibrium (χ2 = 4.62, P = .05). The ∊3 allele was the most abundant in our sample, with a frequency of 0.946 and 0.728 in cognitively normal participants and patients with MCI, respectively (Table 2). We also found that the ∊3/∊3 genotype was the most frequent in both groups (89% of controls and 54% of patients with MCI; Table 2). The ApoE ∊2 allele was the second more frequent in the controls, but it had a higher frequency in the MCI group, suggesting no protective effect of this allele. The ∊4 allele was the least represented in the population but appeared 10 times more frequently in patients with MCI that in the cognitively normal control participants. Only 1 control participant carried the ∊4 allele (Table 2). The frequency of the heterozygote patients with MCI for ∊3/∊4 was 24%, which was higher than that found in cognitively normal participants (Table 2). The odds ratio was 13.3 (CI95%: 1.6-105.5) for ApoE ∊4 allele, which suggests that it is a risk factor for cognitive deterioration.
Apolipoprotein E Genotypes and Allele Frequencies.
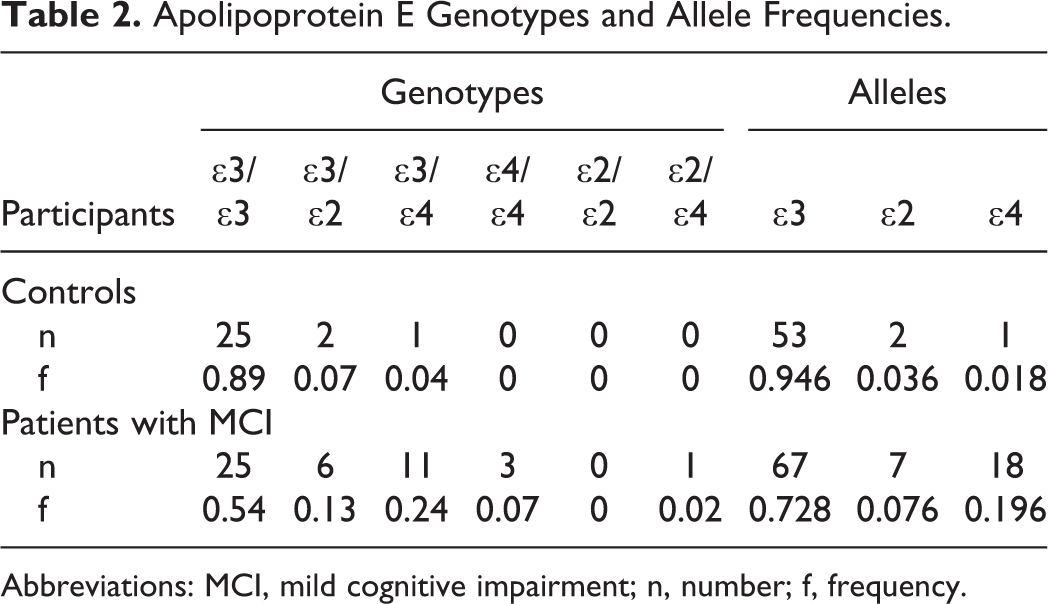
Abbreviations: MCI, mild cognitive impairment; n, number; f, frequency.
Cognitive Profile of Patients With MCI and Controls
All patients had a CDR scale score of 0.5, indicating a mild deficit in memory that was greater than that exhibited in the other cognitive domains or activities of daily living. All patients also scored ≥24 on the MMSE. The MMSE points were mainly lost on the memory and executive component of the test (delay recall and attention subscore), pointing out amnesia and executive deficits in the patients. For this reason and following the Petersen’s criteria, 1 our patients with MCI may be classified as aMCI + md.
The patients performed poorly and differently than controls on tests assessing long-term memory (delayed word list recall; delayed figure recall), attention and executive functions (attention matrix, trail making B-A, and phonological fluency), spatial and verbal short-term memory (spatial span and digit span), and praxis (constructional apraxia; Table 3). Visual perception as assessed with Street’s completion test was not significantly different between the 2 groups (P = .25). Just on Trail making, patients with MCI reached pathological mean scores (cutoff 1 : mean of control group ± 1.5 standard deviation [SD]), which indicated deficits in the executive function (Table 3).
Statistic of Neuropsychological Measure Scores Achieved by Patients and Controls.
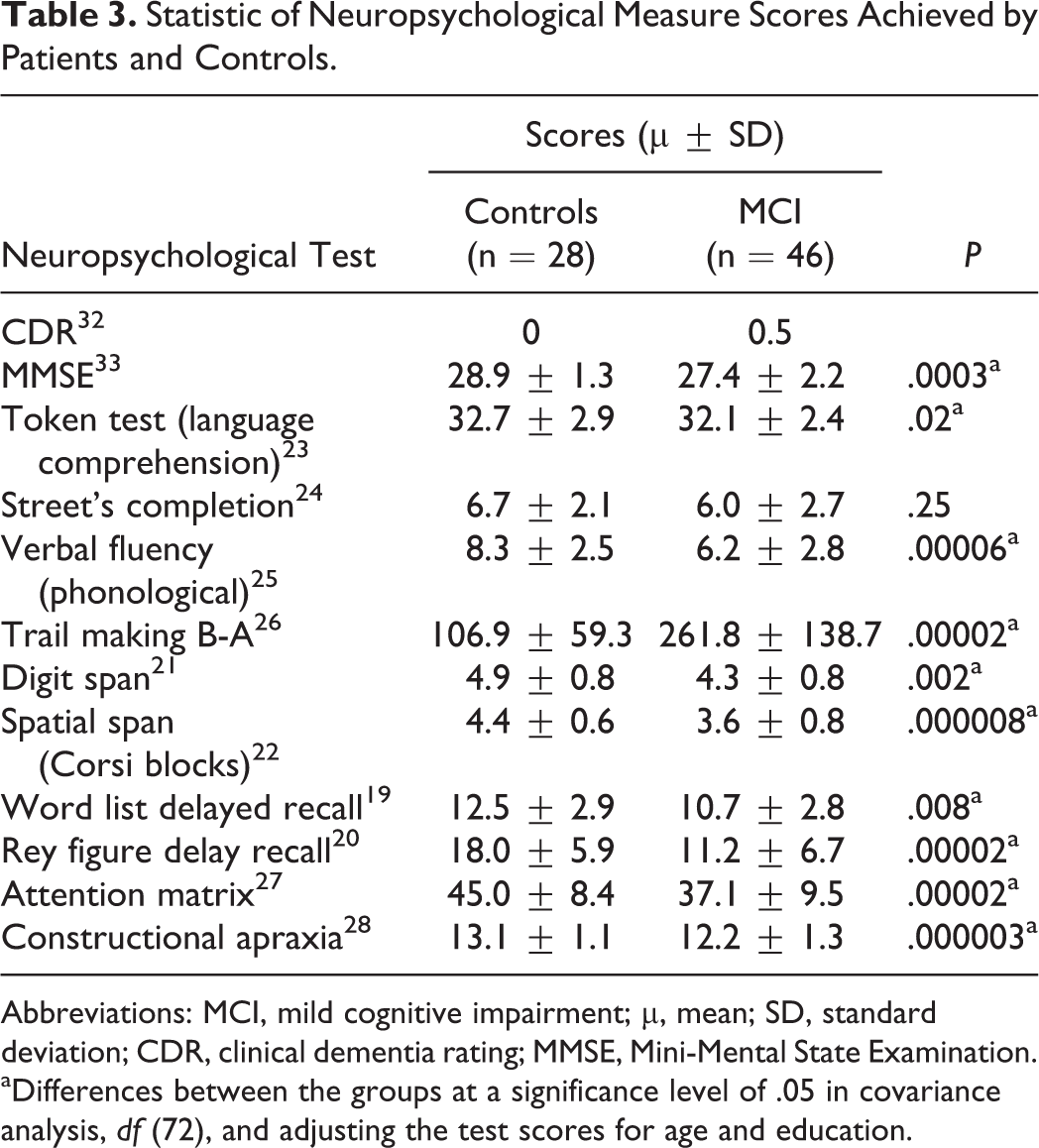
Abbreviations: MCI, mild cognitive impairment; μ, mean; SD, standard deviation; CDR, clinical dementia rating; MMSE, Mini-Mental State Examination.
aDifferences between the groups at a significance level of .05 in covariance analysis, df (72), and adjusting the test scores for age and education.
In contrast, control participants exhibited normal cognitive performance in all tests (Table 3). The multivariate analysis (Wilks’s test) revealed a significant overall effect of diagnosis (F = 5.7; P = .00005) across all neuropsychological functions and the overall effect of years of education (F = 4.4, P = .0001).
Cognitive Profile of ApoE ∊4 Allele Carriers and Noncarriers in the MCI Group
The 32.6% of patients with MCI carried at least 1 ApoE ∊4 allele (Table 2). Multivariate analysis of the results of whole neuropsychological tests did not show differences between the ApoE ∊4 allele carriers and noncarriers in the group of patients with MCI (P[F] = 0.3). However, ApoE ∊4 carriers exhibited poorer performances than noncarriers, with significant differences between means of MMSE and tests assessing executive function (verbal fluency, attention matrix, and constructional apraxia) and short-term memory (Corsi blocks; P ≤ .05). Interestingly, the ApoE ∊4 allele carriers in the group of patients with MCI showed a pathological mean score in Corsi block test that assesses short-term memory (3.4 ± 1.5 SD; cutoff 1 : mean of control group ± 1.5 SD).
Discussion
Apolipoprotein E alleles and genotype frequencies vary greatly according to the geographic localizations and ethnicity. 33 In this study, we found that ApoE allele and genotype relative distributions are in accord with those reported for other populations. 33 The ApoE ∊4 allele frequency in our control group is however lower than values reported for other populations and 4 times lower than that reported for Cubans without dementia. 16 This result may be due to 3 reasons: the small size of our control participant sample (n = 28; Table 1), possible sample stratification as a result of ethnic admixing of Cuban population and its strong known effect on ApoE genotype, 16 and the control participants included in our study are elderly individuals without any cognitive deficit. It is important to note that ApoE ∊4 allele frequency reported by Marcheco et al 16 was calculated for a group of elderly Cuban patients without dementia, which could include individuals with MCI. In contrast, we randomly chose the controls from a pool of screened unaffected individuals (supernormal controls) for this study, which has the potential to create significant bias. Although the use of supernormal controls is often recommended due to its higher power to detect association compared with a study using population-based controls, 34 some authors consider that this practice is inappropriate because the control exclusion criteria could be stricter than those applied to cases. 35
The frequency of the ApoE ∊4 allele found in our patients with MCI was higher than that reported for normal control participants 36 and 10 times higher than in our control group, and as a consequence we obtained a very high odds ratio (13.3 CI95%: 1.6-105.5) value for the ApoE ∊4 allele. This value is affected by the low frequency of ApoE ∊4 allele found in the cognitively normal participants. It should be noted that the ApoE ∊4 allele frequency found in our patients with MCI is similar to that reported for Cuban-Americans with AD or for Cubans with dementia. 16,17
Participants with MCI performed more poorly than cognitively healthy participants in 4 of the 5 cognitive domains evaluated (attention, executive function, memory, praxis, and language), with significant differences in overall performance (P[F] ≤ 0.05). This subtype of patients with aMCI md usually exhibits a high likelihood of progressing to AD. 1,37 In addition, the poorer cognitive performance of ApoE ∊4 allele carriers than the noncarriers in the patient group with MCI suggests a possible role of ApoE ∊4 allele in cognitive deficit.
Although the reports are controversial in relation to the association of the allele ∊4 with the deficiencies in cognitive performance, 11 –13,38,39 it is generally accepted that ApoE ∊4 is a risk factor for cognitive impairment. A meta-analysis carried out by Small et al in 2004 contrasting 38 studies where 8 cognitive domains were analyzed in healthy adults concluded that ApoE ∊4 had effects on global cognitive function, episodic memory, and executive functioning. 11 In each case, the ∊4 carriers performed more poorly than noncarriers. Another study conducted in 2005 by Greenwood et al, with healthy middle-aged adults, reported an ApoE ∊4 effect on attention and working memory, affecting only those homozygous for this allele, which indicated a gene dosage effect. 12
Recently, a retrospective study to evaluate the role of ApoE ∊4 in the clinical diagnosis of AD in patients with cognitive impairment revealed that ApoE ∊4 carriers had a higher percentage of AD diagnoses after a median 16-month follow-up than non-ApoE ∊4 carriers. These authors reported that ApoE genotyping may be helpful in diagnosing AD, particularly in patients presenting with early age of onset of cognitive impairment or presenting with atypical features of dementia. 40
Farlow and colleagues also analyzed the impact of ApoE ∊4 on the cognitive profile of aged patients with MCI. These authors found that the ApoE ∊4 genotype was associated in patients with MCI with worse performance in the domain of memory in a dose-dependent manner. 13 In our study, we obtained a pathological mean score in test assessing short-term working memory only for the ApoE ∊4 carrier’s subgroup (cutoff 1 : mean of control group ± 1.5 SD). This result corresponds well with reports where selective effect of ApoE ∊4 on cognitive performance in particular domains was found. 11 –13 In conclusion, our results suggest that ApoE ∊4 allele maybe a risk factor for cognitive impairment.
Limitations and Future Directions
A limitation of the present study is the small sample size. Consequently, the participants may not be representative of the general population. In addition, we did not assess the effect of ethnic identity and admixture of the participants.
Our investigation is also limited by its cross-sectional design. A larger confirmatory study and a longitudinal follow-up are needed to evaluate the predictive value of ApoE genotyping for the diagnosis and early detection of cognitive impairment.
Footnotes
Acknowledgments
We thank Dr David Sulzer and Dr Alina González-Quevedo for their critical reading of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a 2010 PNCT Grant of Cuban Academy of Sciences.