
Abstract
This article explores how dyads of 186 community-dwelling individuals with a diagnosis of Alzheimer’s disease or a related disorder (ADRD) and their caregivers (dyads) plan to respond to hurricane evacuation warnings in South Florida. Predictors of dyad evacuation for a category 1-3 storm include (1) a younger age of the person with an ADRD diagnosis, (2) the caregiver living in a different residence than the person with ADRD, (3) lack of hurricane shutters, and (4) lower income. A dyad is more likely to evacuate in a category 4 or 5 hurricane if there is (1) a younger age person with an ADRD diagnosis, (2) a more recent diagnosis of ADRD, (3) a residence in an evacuation zone, and if (4) they report needing a shelter. Emergency management teams, especially those who assist with special needs shelters or other outreach programs for people with cognitive disabilities, can use these guidelines to estimate service usage and needs.
Introduction
In the United States, disaster planning places emphasis on individual preparedness. For example, families are expected to have a personal escape or evacuation plan and compile a disaster kit in case of emergency. 1,2 This article reports on the personal disaster plans of families affected by Alzheimer’s disease or a related disorder (ADRD), who live in South Florida, a region that faces comparatively regular evacuation warnings.
Risk Perception During Disasters
As Lupton has noted, there are 2 kinds of risks (1) environmental (such as toxic waste, radiation, or a hurricane) over which the individual has little control and (2) risk behaviors resulting from lifestyle choices, such as smoking. 3 Although the second category assumes that the risk is something over which the individual has control, the former does not, making an examination of decision making, and its implications such as formal disaster planning, especially important. This places emphasis on individual preparedness, resulting in a shift from society to the individual. Public health campaigns seek to educate individuals about potential risks, assuming that, armed with knowledge, people will avoid those risks. During Hurricane Katrina in 2005, for instance, people were frequently blamed for not evacuating after they were warned to do so. 4 Although they did not have control over the strength or path of the hurricane, it was assumed that people had control over their own location during the hurricane. On the other hand, scholars have pointed to a range of factors, such as socioeconomic status, which might influence a person’s risk-taking or risk-reduction choices during hurricanes. 5–7
Public health professionals and anthropologists have argued that individuals must believe that a threat actually exists (risk identification) and believe that protection is needed (risk assessment) before they are willing to engage in risk-reducing behaviors, such as formulating a disaster plan. 3,8 In order for individuals to work through these steps, they must believe that the information provided by the experts and the authorities is valid and that the safeguards they depend upon will be in place. For example, citizens must believe that a hurricane warning is legitimate and poses a true risk to their well-being before they decide to heed warnings. Those who plan to evacuate to shelters must believe that the government will adequately provide a safe and reliable sanctuary. According to Giddens’ theory of modernity, this trust may not always exist, and when individuals are skeptical of experts, they may choose to ignore the risk entirely. 9 If citizens do not trust experts who determine, for example, the direction and severity of a hurricane and who determine evacuation zones, they may not identify it as a risk nor evacuate. Indeed, we are routinely bombarded by risks in the world around us—the air we breathe, the water we drink, and even the sun we walk under all have the potential to cause us harm. 10 People must face risks and hazards on a daily basis, whether it is breathing toxic air, driving a car, or planning for a potential storm. From a long list of such hazards, people must decide which to prioritize so that they can mitigate, prepare, and respond to them as necessary. Conflicting information about hurricane prediction can be overwhelming for citizens and has been cited as a reason for poor evacuation trends before Hurricane Katrina. 4 More specifically, expert scientists and public authorities issued multiple “false alarms” during previous storms, lessening their credibility. 4
The implication of these social trends is that it is difficult for individuals to determine exactly when to act (or what to do) when threatened with a hurricane. Nichter, in his exploration of harm reduction, notes that while in epidemiology risk “refers to a calculated probability, the odds that something will occur (not occur) within a given population,” many individuals do not perceive themselves at risk, even if the statistics indicate this to be the case. 8 A major role of public health professionals and emergency managers is to inform the public of its level of risk and to convince its members to adopt risk-reducing strategies, such as hurricane plans. 2,5
The existence of preparations and plans for mitigation can also impact the outcomes of a hazardous event and ultimately determine whether it will be labeled as a true “disaster” or not. 11,12 The public health impact of hurricanes include storm-related mortality, injury, infectious disease, psychosocial effects, displacement and homelessness, damage to the health care infrastructure, disruption of public health services, transformation of ecosystems, social dislocation, loss of jobs and livelihood, and economic crisis. 13 An increase in communicable diseases after hurricanes is notable among vulnerable populations, including the elderly individuals. 13–15
Evacuation Decision Making
Prior research on evacuation decision making in Florida found that families with young children were more likely to evacuate before a storm. 7 This same research also found that people living in “risky environments,” specifically in mobile homes or flood zones, were more likely to evacuate than other populations. Similar trends were discussed by Peacock, Brody, and Highfield who found that Florida homeowners in expert-designated risk areas (ie, evacuation zones) reported higher levels of risk perception. 16 Conversely, people who owned their homes or who had pets were less likely to evacuate than others. 7
Whitehead et al represent one of the few research teams that explored how storm severity (eg, category, as measured by the Saffir-Simpson Wind Scale) impacted evacuation decision making at the household level. 17 Indeed, they found that storm severity was the single biggest factor in a household’s decision to evacuation.
In these prior studies, caregiving for a frail elder or a person with a disability (cognitive or otherwise) was not taken into account when examining factors affecting decision making. Findings from Eisenman et al 18 consider how elderly individuals might influence a family’s evacuation decision making. They suggest that elderly individuals may refuse to evacuate before a storm and therefore adult children and caregivers also choose to stay behind with them. 18 Differential risk perceptions within families can influence decision making in the wake of a storm.
Studies have shown that older individuals who might have survived past hurricanes unscathed tend to believe they can survive storms in their own home. 19–23 For instance, many elderly individuals in the New Orleans area who survived previous storms (eg, Hurricanes Betsy or Camille) believed they could also survive Hurricane Katrina. 24 Many had evacuated for Hurricane Ivan unnecessarily and therefore did not evacuate for Katrina. Another age-related factor that might have influenced their decisions includes an inability to leave prior to obtaining their monthly social security check. 4,25 Finally, another study by Cherry, Allen, and Galea on why elderly populations did not evacuate for Hurricane Katrina found, in addition to the sense of security that came with having survived previous hurricane experiences, such as Hurricane Camille in 1965, other “possible physical and cognitive limitations that might interfere with successful evacuation.” 21
Socioeconomic Status
The ways in which a hazard impacts a population are determined by several structural factors, including socioeconomic status (eg, minority group membership, income level, and age). 26 The concept of “vulnerability” is central to the understanding of disproportionate disaster impacts. Particular populations, such as those with lower socioeconomic status, marginalized minority groups, and the elderly individuals, tend to be more vulnerable to the deleterious effects of the hazard. 6,26–31 Most of the casualties of Hurricane Katrina fit into one or all of these categories. 24,32–34 The concept of vulnerability in disaster research refers to certain subsets of the population that bear an undue burden of the impact due to their lower socioeconomic status or preexisting health conditions. 11
Lower income can have a negative impact on families both before and after a hurricane. For example, lower income might make it difficult to afford the full range of disaster preparedness materials, including safe housing in safe locations, hurricane shutters or impact-resistant glass, transportation, or generators. 35 Lack of these supplies and resources might increase a person’s sense of risk and increase a desire to leave. Conversely, lack of funds for a car or its fuel (and, potentially, for a hotel room) might restrict a family’s ability to evacuate to a safe location. 4,25 Lower income may apply to those who are on a fixed income, such as older individuals who primarily rely on social security. 4,21 Most research has found that lower income is associated with sheltering at home rather than evacuating. 7,19,36,37
How ADRD Impacts Risk Perception
Although there is ample research on elderly individuals residing in nursing homes during disasters such as hurricanes, very few studies have explored how caregivers of community-dwelling persons with ADRD make decisions when faced with natural hazards. 38–45
Dementia of the Alzheimer’s type is a progressive disease, which affects decision-making capacity and performance of functional activities of daily living over time. One of the hallmarks of the disease is the decline in executive functions that lead to poorer decision-making capacity and diminished judgment. 46,47 These abilities are crucial in planning response to risk. 48–50 The ADRD impacts disaster planning because when executive functioning is impaired so is judgment when deciding how to respond to the risks associated with an upcoming hurricane. 35,48,51
Those who have caregivers living with them are likely to have assistance in making decisions about whether to evacuate or to shelter in place. Informal caregivers providing this assistance might have a range of preexisting relationships with the person with ADRD: spouse, adult child, other family member, or friend. They may or may not physically live with the person with ADRD. It is important to note that many caregivers have their own physical or mental health challenges. 52 Caregivers might also contend with a lack of resources, contributing to their own vulnerability. 53–56 Regardless of the relationships, all families must consider their risk, their resources, and their abilities (or lack thereof) when making decisions about whether to evacuate for an impending hazard, such as a hurricane, or to shelter in their own homes.
The following research was guided by the following research question: “Which factors influence caregiver's decisions to evacuate during moderate and severe storms?”
Methods
The analysis reported here is part of a larger study that included participant observation, semistructured interviews (n = 20) with informal caregivers, professional caregivers (n = 8), disaster plan reviews (n = 259), and a semiquantitative survey (n = 253). 35 Each methodological component informed an anthropological understanding of the experience of sheltering people with dementia during a hurricane and, when possible, contextualized these results. These data were collected with the assistance of the staff from a partnering organization, Alzheimer’s Community Care (ACC), which serves approximately 1000 families per year in South Florida. The ACC is a 501 (c) (3), providing community-based services, such as specialized adult day care and case management for families affected by ADRD. It serves families in an area that was impacted by multiple hurricanes during the 2004 to 2005 hurricane seasons. The focus of this article is on the disaster plan review and a caregiver survey administered in May 2011 and the disaster plan review from June 2011.
Sample
All caregivers who have a family member participating in specialized adult day care through ACC have a basic disaster plan on file in their charts. There were 186 caregivers who participated in both the caregiver survey and the follow-up disaster plan review and who were included in the final analysis.
Disaster Plan Review
The ACC requires that all families receiving services have a basic disaster plan on file with the organization. This disaster plan is recorded on the ACC “disaster plan checklist” that documents the family’s planned location during a storm. In 2011, initial caregiver interviews revealed that caregivers had different plans depending on the category of the storm. The ACC disaster plan checklist was updated to capture the distinction in caregiver disaster plans for category 1-3 storms and category 4-5 storms. When the form was modified, a follow-up disaster plan review was conducted to determine how many caregivers planned to shelter in their homes versus evacuate based on severity of the storm. Thus, the revised document captured whether individuals (1) planned to evacuate, (2) required formal shelter (ie, Red Cross or special needs shelter), or (3) planned to stay with a family member or friend.
Survey Instrument
To augment information in the disaster plan review, a caregiver survey was created to capture demographic information and other factors that might influence a caregiver’s decision to evacuate or not (eg, having hurricane shutters, a relationship to the person with dementia, previous hurricane experience, and socioeconomic status). The survey tool was informed by 20 interviews with caregivers and 8 interviews with ACC staff members and then piloted with a subsample of 5 respondents.
The structure of the survey had 4 domains (1) demographic information about the person with an ADRD diagnosis (6 questions), (2) information about the caregiver (10 questions), (3) questions about disaster preparedness and vulnerability to a storm (11 questions), and (4) information about factors that could impact disaster recovery (5 questions).
The first domain (demographics of person with ADRD diagnosis) considered (1) age, (2) sex, (3) year of receiving a formal diagnosis and whether it took place during the highly active 2004 to 2005 hurricane season, (4) place of residence and whether the patient was living with a caregiver during the 2004 hurricane season, and (5) mobility status.
Caregiver characteristics considered in the second domain (caregiver information) included (1) age, (2) sex, (3) relationship to the person with dementia, (4) stress level, and (5) social support.
The third domain, which considered factors that might influence a dyad’s vulnerability, included (1) having a disaster kit, (2) perception of risk about the likelihood of a hurricane hitting that year (ie, risk perception), (3) having hurricane shutters on the home, (4) access to a generator, (5) housing structure (cinderblock or wood frame), (6) whether they rented or owned their home, (7) whether they lived near a body of water (including Lake Okeechobee, the intercoastal waterway, canal, or the Atlantic Ocean), and (8) the year the home was built.
The final domain included inquiries into a family’s disaster recovery potential. This domain was centered around economic capacity, such as whether they had (1) the capacity to repair damage to their home if it lost its roof, (2) homeowners’ or renters’ insurance, (3) flood insurance, (4) a wind protection policy, and also asked about (5) yearly income.
Information from the survey was recorded in a Microsoft Excel spreadsheet. The data were linked with the data from the disaster plan review for analysis. The file in was then exported to SPSS version 19 to perform a logistic regression. 57
Procedure
The survey was administered by the first author (J. C. C.), ACC nurses, and 1 ACC volunteer. It was completed via telephone, concomitantly with the yearly disaster plan intake. Although the disaster plan intake is a mandatory part of the ACC procedures, verbal consent was obtained from caregivers before the survey was administered. Data were deidentified to protect participant confidentiality. This study was reviewed and approved by the institutional review board of the University of South Florida.
Analysis
When a hurricane approaches, caregivers must decide between 2 discrete options, (1) evacuate or (2) remain at home. For the purpose of analysis, these decisions were recorded as “yes, to evacuate” or “no, to shelter at home.” A logistic regression offers an analytical framework for modeling discrete outcomes. The resulting models are based on household responses to the survey and the required disaster plan. 58
Descriptive statistics for each variable were created, and normality was tested. Nonnormal variables were transformed. Student t test, chi-square test, and Mann-Whitney U test were used where appropriate for variable comparison.
Two logistic regression models were created, 1 with a dependent variable of evacuation in a category 1-3 storm and 1 with a dependent variable of evacuation in a category 4-5 storm. For both, a stepwise method and adjusted odds ratio with a 95% confidence interval was used. Significance was determined at P < .05.
Although all values were considered (including models that included variables by domain), the models discussed here were selected because they were parsimonious, included significant values, and had the highest predictive outcome. We sought the most parsimonious model so that planners could focus on significant variables when predicting how many ADRD-affected families might evacuate for a hurricane. These models only contain significant predictive values; therefore, nonsignificant variables are not discussed in depth.
Results
One hundred and eighty-six dyads were included in the sample. As revealed in caregiver interviews, the category of storm (Saffir-Simpson Scale) influenced a caregiver’s decision to evacuate or not (described in Christensen). 35 In addition to storm severity, several other socioeconomic factors and physical conditions influenced a caregiver’s decision to evacuate or shelter at home before a storm. This research considers what factors might influence a caregiver’s decision to evacuate or shelter in place in less- and more-severe hurricanes.
Demographics and Descriptive Statistics
The average caregiver age was 61.6 years. The youngest caregiver reported being 27 years old, while the oldest was 94 years old. The average age of the person with a diagnosis of ADRD was 81.7, with the youngest being 47 years old and the oldest 111 (see Table 1). Most of the caregivers (75% or n = 139 of 185) were female (1 survey was missing these data). The vast majority (90%) of caregivers reported having experienced a hurricane during the highly active 2004 to 2005 hurricane seasons (n = 168 of 186). The majority (95% or n = 175 of 186) of the caregivers and persons with an ADRD diagnosis were living in the same dwelling as they had been at the time of the survey in 2011. However, only 65% (n = 120) were living in their same dwelling during the 2004 to 2005 hurricane season. During the 2004 to 2005 hurricane season, only 38% (n = 71) of the individuals had been diagnosed with ADRD. In 2011, 77% (n = 144 of 186) of the families reported having hurricane shutters on their homes. Some dyads (20%; 37 of 183) reported they were aware of living in an evacuation zone (3 dyads had missing data). There were 35 (19%) caregivers who, according to their disaster plans on file with ACC, self-identified with “needing shelter” if a hurricane were to threaten them in 2011. This designation indicates that the caregiver did not feel safe in their home but without a specific evacuation plan.
Participant Demographics.
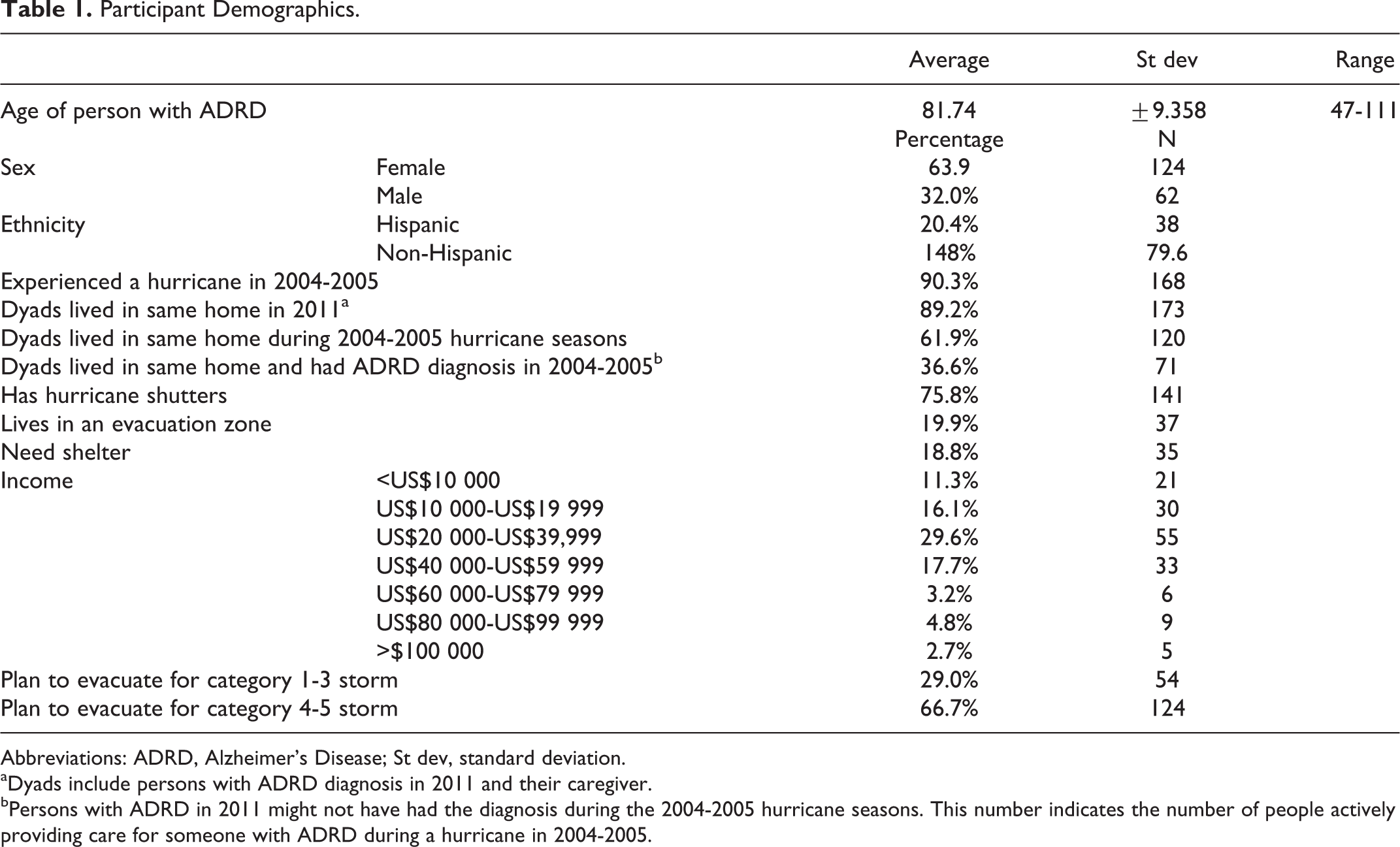
Abbreviations: ADRD, Alzheimer’s Disease; St dev, standard deviation.
aDyads include persons with ADRD diagnosis in 2011 and their caregiver.
bPersons with ADRD in 2011 might not have had the diagnosis during the 2004-2005 hurricane seasons. This number indicates the number of people actively providing care for someone with ADRD during a hurricane in 2004-2005.
Income (combined based on the caregiver and person with ADRD income) was broken into 6 categories, 1 = less than US$10 000 per year (n = 27); 2 = between US$10 000 and 19 000 (n = 30); 3 = between US$20 000 and 39 000 (n = 55); 4 = between US$40 000 and 59 000 (n = 33); 5 = between US$60 000 and 79 000 (n = 6); 6 = between US$80 000 and 99 000 (n = 9); and 7 = over US$100 000 (n = 5). Unfortunately, as several (n = 27; 15%) caregivers declined to provide this information, data were obtained for only 157 participants. The most commonly reported income was between US$20 000 and US$30 000 per year (34%, 55 of 159). In total, 70% of this sample made less than US$40 000 per year. Overall, 29% (n = 54 of 186) of the families predicted that they would evacuate if their home were threatened by a category 1-3 hurricane. The number of families who stated they would evacuate jumped to 67% (n = 124 of 186) if they were threatened by a more intense category 4 or 5 hurricane in the same year.
Predictors of a 1 to 3 Hurricane Evacuation: Model # 1
Predictors of dyad evacuation for a category 1 to 3 storm include (1) a younger age of the person with an ADRD diagnosis, (2) whether the caregiver and person with ADRD live in the same home, (3) lack of hurricane shutters, and (4) lower income. This model attempts to predict whether a person will evacuate his housing in a category 1-3 hurricane. Each variable significantly contributes to the model except for “age of person with dementia.” This variable (age of person with dementia) approaches significance (P =.055) and was determined to be theoretically important in other research. 7,21,24,59
As Table 2 illustrates, a person is more likely to evacuate during a category 1 to 3 hurricane if they are younger, if the caregiver and person with dementia do not live in the same home, if they do not have hurricane shutters, and if they have a lower income. This model is able to predict evacuation 76.5% of the time (see Tables 2 and 3).
Observed Versus Predicted Evacuation for Category 1-3 Hurricane (n = 158).
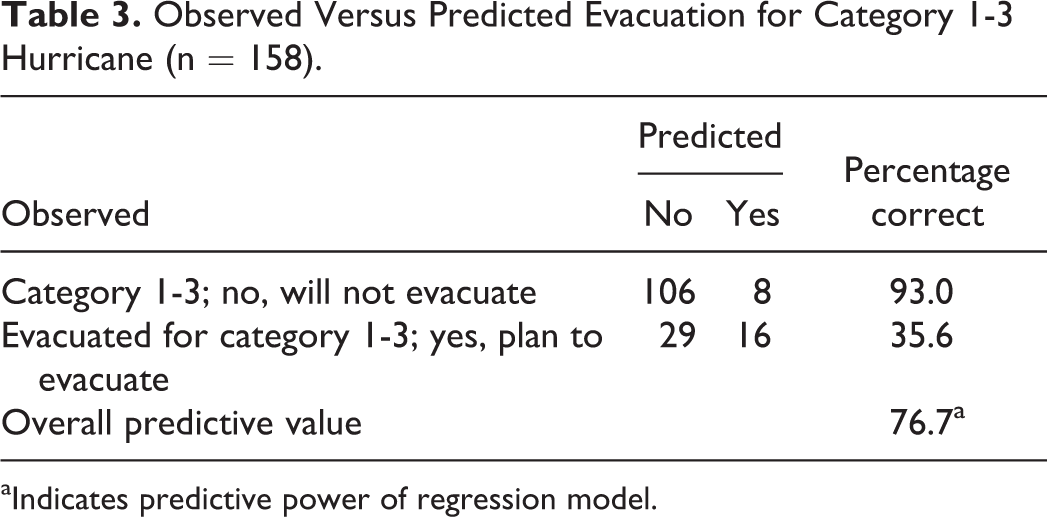
aIndicates predictive power of regression model.
Predictors of Evacuation for Category 1-3 Hurricane (n = 158).
Abbreviation: CI, confidence interval.
aWith every 1 year increase in age.
bReference Category: Yes, plan to evacuate (1).
cWith every increase in income category (<10k per year; 10k-20k per year; 20k-40k per year; 40k-60k per year; 60k-80k per year; 80k-100k per year; >100k per year).
Predictors of a 4 to 5 Hurricane Evacuation: Model #2
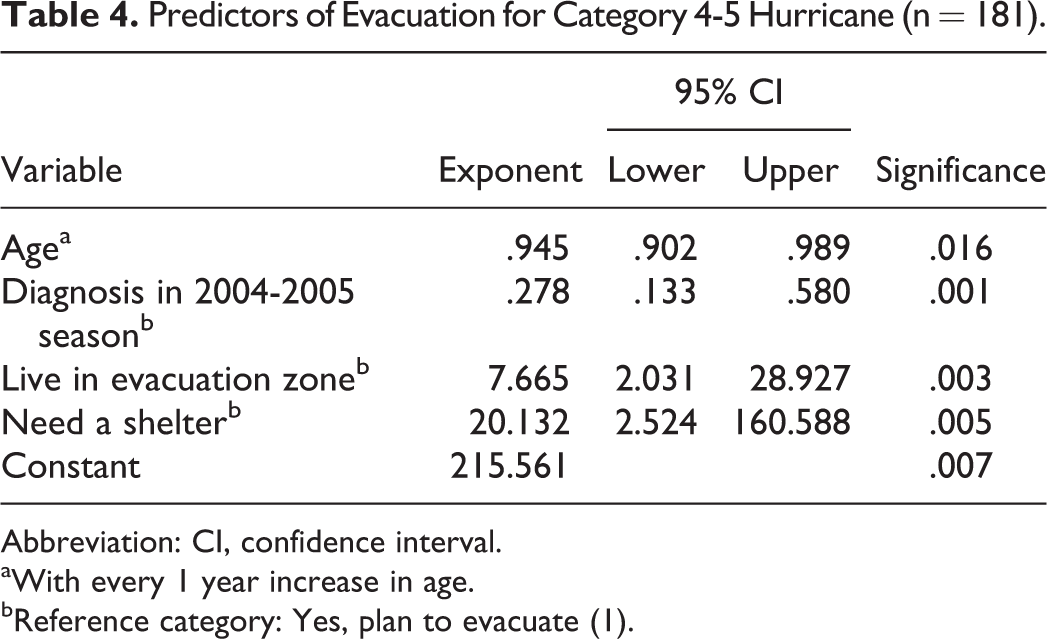
A dyad is more likely to evacuate in a category 4 or 5 hurricane if (1) the person with a ADRD diagnosis is younger, (2) they have been more recently diagnosed with ADRD, (3) if the dyad lived in an evacuation zone, and (4) if they reported needing a shelter. This model attempts to predict whether a person will evacuate during a category 4 to 5 hurricane. Each variable contributes significantly to the model.
As Table 4 illustrates, a person is more likely to evacuate in a category 4 or 5 hurricane if they are younger, did not have an ADRD diagnosis during the 2004 to 2005 hurricane season, if they live in an evacuation zone, and if they reported needing a shelter. Living in an evacuation zone and needing a shelter are particularly important. If a person identifies with needing shelter, they are over 20 times more likely to evacuate than someone who does not think they are in need of a shelter. If a person lives in an evacuation zone, they are 7.7 times more likely to evacuate. This model is able to predict evacuation 75.8% of the time (see Tables 4 and 5).
Observed Versus Predicted Evacuation for Category 4-5 Hurricane (n = 181).
aIndicates predictive power of regression model.
Predictors of Evacuation for Category 4-5 Hurricane (n = 181).
Abbreviation: CI, confidence interval.
aWith every 1 year increase in age.
bReference category: Yes, plan to evacuate (1).
Discussion
These analyses show that a dyad’s decision to evacuate or shelter at home during a hurricane is complex, and the driving factors vary depending on storm severity. Both the decision to evacuate and shelter at home can hold unique risks for families affected by ADRD. Caregivers have to weigh their own abilities, the abilities of the person they care for, the safety of their home location, and their capacity to recover from a hurricane should their home sustain damage. Understanding how these variables work together to create evacuation outcomes can help to inform emergency planners and, ultimately, to assist in keeping vulnerable individuals safe during complex, rapidly progressing emergency situations. The models presented here elucidate the factors that play the largest roles in predicting whether a caregiver plans to evacuate or shelter at home.
Age of Person With ADRD Diagnosis
Both models (for hurricanes category 1 to 3 and category 4 to 5) indicated that the age of the person with an ADRD diagnosis played a role in whether a dyad would evacuate or not, older ADRD age indicated that a family was less likely to evacuate for any category of storm. This supports the literature, which has noted the reluctance of older people to evacuate. 18,21,59 It is unclear why, specifically, the age of the ADRD plays a prominent role in the model since other indicators, such as impaired physical mobility, did not significantly contribute to the predictive value of the model. This is an area that needs further research.
In addition, caregiver age and health did not significantly contribute to the predictive value; therefore, these were not included in the model. One assumes that the caregiver is making most of the disaster-planning decisions and, therefore, their strength and stamina would play a large part in how the dyad responded to disaster. However, it did not significantly contribute to the model. This might be a result of their risk perception, that is, caregivers might not consider themselves to be at risk.
Increasing rates of ADRD of advanced severity can increase the challenge to professionals in charge of risk communication. 51,60 Since some caregivers are quite elderly themselves (in our sample, the eldest was 94 years old), one might assume that their health and levels of social support would factor into disaster decision making. This research did not find caregiver age to be a factor; however, further research on this topic is warranted.
Other Important Factors for Hurricanes Category 1 to 3
If families feel it is necessary to evacuate for a category 1 to 3 hurricane, this suggests they do not feel their home would be safe during any storm. This model suggests that a family is more likely to evacuate its home, even for less intense hurricanes if (1) the person with ADRD is younger, (2) the caregiver and person with dementia do not live in the same home, (3) the family does not have hurricane shutters, and (4) the family has a lower income.
Living Arrangement
When a caregiver and person with ADRD do not live together, there is a greater chance of evacuating for a category 1 to 3 storm. This may mean that the caregiver will evacuate the person with ADRD from where they live to the caregiver’s home.
Low Income and Hurricane Shutters
This research found that caregivers were more likely to evacuate if they had lower incomes. This contradicts much of the literature, which indicates that lower income prevents a family’s ability to evacuate when faced with a disaster. 26,61 Lower income families might be more likely to live in older, less expensive housing that might not be up to current building codes; additionally, they might not be able to afford protective devices such as hurricane shutters. For example, Christensen found that caregivers living in Federal Housing and Urban Development (HUD) housing were not provided hurricane shutters and, by virtue of the fact that they qualified for HUD housing, could not afford to install them on their own. 35 If homes are not designed to withstand severe weather, residents are at a higher risk of injury or death if they remain in their homes during a hurricane. 62 Our findings indicate that lower income residents appear to perceive themselves to be at higher risk and opt to evacuate even for lower intensity storms. Housing type was considered as a factor but was not found to significantly contribute to the model, whereas lower income levels and lack of hurricane shutters did.
Evacuation can be an expensive endeavor, often requiring access to a vehicle, money for gasoline, and possibly a hotel. It is noteworthy that 70% (112 of 159) of this sample made less than US$40 000 dollars a year, perhaps making it difficult to afford the full range of disaster preparedness materials. These necessities can be mitigated through social networks (staying with friends or families) or taking advantage of the resources, such as an emergency shelter (run by the American Red Cross) or the special needs shelters (run by the counties). 35,62 We can posit that lower income can be correlated with the perception of higher risk, leading to a decision to evacuate, but further research is needed to explore this factor.
Important Factors for Hurricane Category 4 to 5
A person with ADRD is more likely to evacuate in a category 4 or 5 hurricane if (1) they are younger, (2) they did not have a diagnosis of ADRD during the 2004 to 2005 hurricane season, (3) they lived in an evacuation zone, and (4) the caregiver reported needing a shelter.
Diagnosis During Previous Hurricane Experience
A dyad including a person with a more recent diagnosis of ADRD (ie, the individual did not have a diagnosis during the 2004 to 2005 hurricane season) was more likely to evacuate. Conversely, people who had previously been caring for a person with dementia during a hurricane were less likely to evacuate. People with a more recent diagnosis of ADRD are more likely to be in the earlier stages of the disease and their caregivers are less likely to be experienced.
Some people who have successfully cared for people during past hurricanes might not feel that future evacuation is necessary. This might be related to the results that “older age” and “previous hurricane experience” predict against evacuation. 21 This decision might be problematic because diseases that cause dementia, like Alzheimer’s disease, are often progressive and change over time, making it difficult for people caring for a person with dementia to anticipate the needs of a person with ADRD during future hurricanes. 46,63–65
Evacuation Zones
This analysis suggests that caregivers are taking the official designation of “evacuation zones” seriously and that caregivers do respect the official designation of risk. As noted earlier, people must believe that risk exists before they engage in risk-reduction procedures, such as creating disaster plans. 3,8,66 They must also believe the information provided by the authorities is valid and that safeguards will be in place. Many people do not perceive themselves as at risk even if they have a high probability of being impacted by an illness/disaster event. However, this finding suggests that caregivers who are aware they are living in a designated evacuation zone do take it into consideration when deciding whether to evacuate or to shelter in place.
In the larger study, however, not all caregivers were certain whether or not they lived in an evacuation zone. 35 This question was part of the disaster plan on file at the ACC specialized day care centers, and there was no option for responses such as “I don’t know.” The staff was expected to probe and help the caregivers determine whether they lived in an evacuation zone or not. However, it is unknown whether this happened in practice. This lack of knowledge might preclude caregivers from deciding to evacuate even if they are at risk. 5,67 It remains important that evacuation zones are well publicized so that caregivers can make educated decisions about whether to evacuate for a hurricane or not.
Risk Perception “Needing Shelter.”
The question relating to a family needing a shelter plan was meant to identify families that required assistance in finding alternative shelters during the storm. Needing shelter indicates that the caregiver assessed his or her situation and did not feel that the family home would be safe during higher impact storms (category 4 to 5) but was unsure where to go. In other words, they had a higher perception of risk and needed assistance securing a safe location. 3,68,69 It is not entirely clear which factors, other than living in an evacuation zone, might have influenced the caregivers’ risk perception because in this model lacking hurricane shutters, for example, did not appear as predictive factors for higher intensity hurricanes. Future research should further investigate understandings of the construct of “risk” among this population. Although qualitative data were used to develop the factors included in the survey, the importance of the variable, caregiver needs shelter, could use more explanation. Ideally, another round of qualitative interviews could help researchers better interpret the trends found in this analysis.
Limitations
There are several limitations of this study that should be considered. The first limitation is the relatively small sample size of 186. Although this sample is sufficient overall, once it is subdivided into groups (such as those based on income) it becomes quite small, affecting the integrity of the prediction.
Some of the variables collected in the data asked caregivers to reflect on past hurricane experiences. In Florida, the last direct hurricane to impact the area was in 2005. This means that there was a 6-year lapse between experience and data collection, making some of the responses vulnerable to recall bias.
Although this article is based primarily on caregivers’ plans for future hurricanes, hypothetical evacuations are different from actual evacuations. Hypothetical evacuation rates are usually higher than the number of people who actually evacuate. 19
It is difficult to capture complex phenomena such as “risk perception” in quantitative data. Although qualitative data were used in this research to inform the creation of the survey and assisted in explaining some of the factors in the model, additional follow-up interviews would be useful for better understanding the trends.
Some factors, such as social support, have been reported as important elsewhere but were not significant in this analysis. Further investigation is necessary to understand variation seen in the body of research related to disaster preparedness and evacuation among older adults.
It is possible that this research is not reflective of the average caregiving population because the population in this study received basic disaster planning services through the partner organization. The larger study found that this population tended to be better prepared than the average American, based on the existence of both disaster kits and having basic disaster plans. 35 More research is necessary to test the findings presented here in a more representative population.
Conclusions and Significance
Predictors of caregiver and person with ADRD (dyad) evacuation vary for category 1 to 3 and category 4 to 5 hurricanes. Previous experience, age, living situations and locations, emergency supplies, and sheltering needs contribute to whether a dyad expects to evacuate and under what circumstances. This research can give emergency managers insight into what factors might influence the ultimate utilization of services. These models can assist in predicting the number of personnel and supplies that may be needed before, during, and after a hurricane, depending on the strength of the storm. For example, planners might consider the age of the person with ADRD when estimating the number of people who will ultimately utilize their shelter and other services.
Risk perceptions (or proxies of risk perception) play an important role in a caregiver’s disaster planning. Our study indicated that caregivers do take the government-designated evacuation zones into consideration when deciding whether to evacuate or shelter in place during severe storms. However, for caregivers to assess their risk they must first be aware that they are living in an evacuation zone. Caregivers’ education is essential so that they can be aware of other factors that might influence their safety and security during a hurricane as well as those affecting resources available to them in the event of an emergency.
Income levels play a complex role in the decision-making process. Our research suggests that caregivers with lower income feel more at risk and are, therefore, more likely to evacuate. This is especially true if they live in an evacuation zone and lack hurricane shutters. Income plays a complex role in the model, especially because our finding that lower income is associated with higher evacuation rates contradicts most other research on this topic. This requires further research.
Considerations for Further Research
The qualitative data collection and analysis were part of the larger research study. Although the details of the mixed-method study are described in depth elsewhere (due to space constraints), they remain important for providing context to these findings. The qualitative components, including staff and caregiver interviews and participant observations, shaped the survey questions. Ideally, another round of qualitative analysis could help us better interpret the trends found in this analysis.
Organizations serving community-dwelling families affected by ADRD should take an active role in disaster preparedness education with their clients. Educational tools, such as specialized disaster kits, can be used to help families critically consider their risks, needs, and options before a disaster strikes.
Several factors were considered, such as social support and comorbidities, which did not appear in the model; however, this does not mean that they do not play an important role in disaster planning. The authors suggest that these and other issues, such as tracking evacuation expectations to actions during a hurricane, be considered in future research.
Footnotes
Acknowledgment
We extended our gratitude to Melanie Mouras for her assistance with editing the text of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.