
Abstract
Background:
In response to the hurricane-related deaths of nursing home residents, there has been a steady increase in the number of facilities that evacuate under storm threat. This study examined the effects of evacuation during Hurricane Gustav on residents who were cognitively impaired.
Methods:
Nursing homes in counties located in the path of Hurricane Gustav were identified. The Minimum Data Set resident assessment files were merged with the Centers for Medicare enrollment file to determine date of death for residents in identified facilities. Difference-in-differences analyses were conducted adjusting for residents' demographic characteristics and acuity.
Results:
The dataset included 21,255 residents living in 119 at risk nursing homes over three years of observation. Relative to the two years before the storm, there was a 2.8 percent increase in death at 30 days and a 3.9 percent increase in death at 90 days for residents with severe dementia who evacuated for Hurricane Gustav, controlling for resident demographics and acuity.
Conclusions:
The findings of this research reveal the deleterious effects of evacuation on residents with severe dementia. Interventions need to be developed and tested to determine the best methods for protecting this at risk population when there are no other options than to evacuate the facility.
Introduction
In the wake of the Hurricane Katrina and in response to hurricane-related deaths, there has been a steady increase in the number of nursing homes that evacuate under storm threat. 1 –5 Within the same storm-affected region in 2005, the number of nursing homes evacuating in advance of the storm more than doubled within a 1-month period; from 30 nursing homes prior to Hurricane Katrina to 72 facilities in advance of Hurricane Rita. 2 There was a 4-fold increase 3 years after Hurricane Katrina, when 119 facilities evacuated prior to Hurricane Gustav. This increase has been accompanied by considerable public debate about the appropriateness of a universal evacuation policy for nursing home residents. 3 To address this concern, recent research examined the differential morbidity and mortality associated with evacuation versus sheltering in place for nursing home residents. Dosa and colleagues found that evacuation, and not storm effects experienced while sheltering in place, contributed significantly to increased rates of hospitalization, morbidity, and mortality of nursing home residents. 2,6
Nationwide, of the approximately 1.6 million adults who live in nursing homes, an estimated 50% to 70% carry a diagnosis of Alzheimer’s disease or a related dementia. 7,8 It is well recognized that impaired memory and reasoning severely limit a person’s ability to independently and adequately respond to complex, evolving, and dangerous situations. 9 Although people with dementia are recognized as a vulnerable population during disasters, it is unknown if this diagnosis confers increased risk for disaster-related hospitalization and mortality for those who are evacuated.
Nursing home evacuation in response to a storm threat is typically done en masse with staff who may not know the residents. Supplies, equipment, and transportation are prepared in the hours leading up to the departure. Across studies examining relocation-related stress and transfer trauma, it appears that time spent preparing residents for a move reduces negative consequences and supports successful adjustment. 10 –13 However, it is unknown what types of intervention, if any, are currently used to build resilience and prepare residents for this type of move, particularly given the limited time available prior to a storm. It is probable that residents with cognitive impairment may not adequately grasp what is occurring and understand why daily schedules are disrupted while staff are preparing for evacuation. It is also unknown whether nursing home residents with dementia fare worse during evacuation than those who are cognitively intact. To elucidate this issue, this study examined the effects of evacuation during Hurricane Gustav on residents diagnosed with Alzheimer’s disease and related dementias.
Background
On August 27, 2008, as Hurricane Gustav approached the southeast United States, the Governor of Louisiana issued a Statewide Declaration of Emergency. In response to the storm’s magnitude at sea and the uncertainty of the storm track, more than 2 million people evacuated in advance of the hurricane. After Action reports suggest that government officials and response agencies were extremely vigilant and determined to be proactive in the days leading up to Hurricane Gustav’s landfall because of the devastation wrought by Hurricane Katrina 3 years earlier. 5,14,15 To protect their residents, approximately 119 nursing homes evacuated in response to Hurricane Gustav’s threat. Although the National Hurricane Center predicted with 45% certainty that Hurricane Gustav would make landfall on September 1, 2008, as a category 3 storm or greater, it struck Louisiana as a weak category 2 storm and quickly fell to category 1 intensity. 14
Although Hurricane Gustav caused an estimated $4.5 billion in economic losses, the overall damage to buildings and physical infrastructure outside of rural coastal areas of Central Louisiana was minimal relative to other major hurricanes. As such, Hurricane Gustav provides a unique opportunity to examine the effects of evacuation on nursing home residents because of the minor storm effects. That is, because residents evacuated in advance of the storm, most nursing home evacuees were never directly exposed to the hurricane; did not return to damaged, uninhabitable buildings; or experience relocation to a new facility after the storm.
Methods
Data Sources
Institutional review boards at the University of South Florida and Brown University approved this research. Data were drawn from multiple sources to capture the storm effects, location of nursing homes, and residents exposed to the storm. For the current study, we first identified all nursing homes in counties in the path of Hurricane Gustav (Figure 1) using the Online Survey Certification Automated Record to identify the facilities’ address, ownership, staffing, and size. To identify residents in nursing homes in specified at-risk areas for Hurricane Gustav during the 2006 to 2008 period (Figure 1), we used the Minimum Data Set (MDS). The MDS resident assessment includes nearly 400 data items providing information on residents’ cognitive functioning, physical functioning, diagnoses, health conditions, treatments, and outcomes. 16 The MDS data were merged with the Centers for Medicare and Medicaid Services enrollment file to determine date of death for the residents in the at-risk facilities.
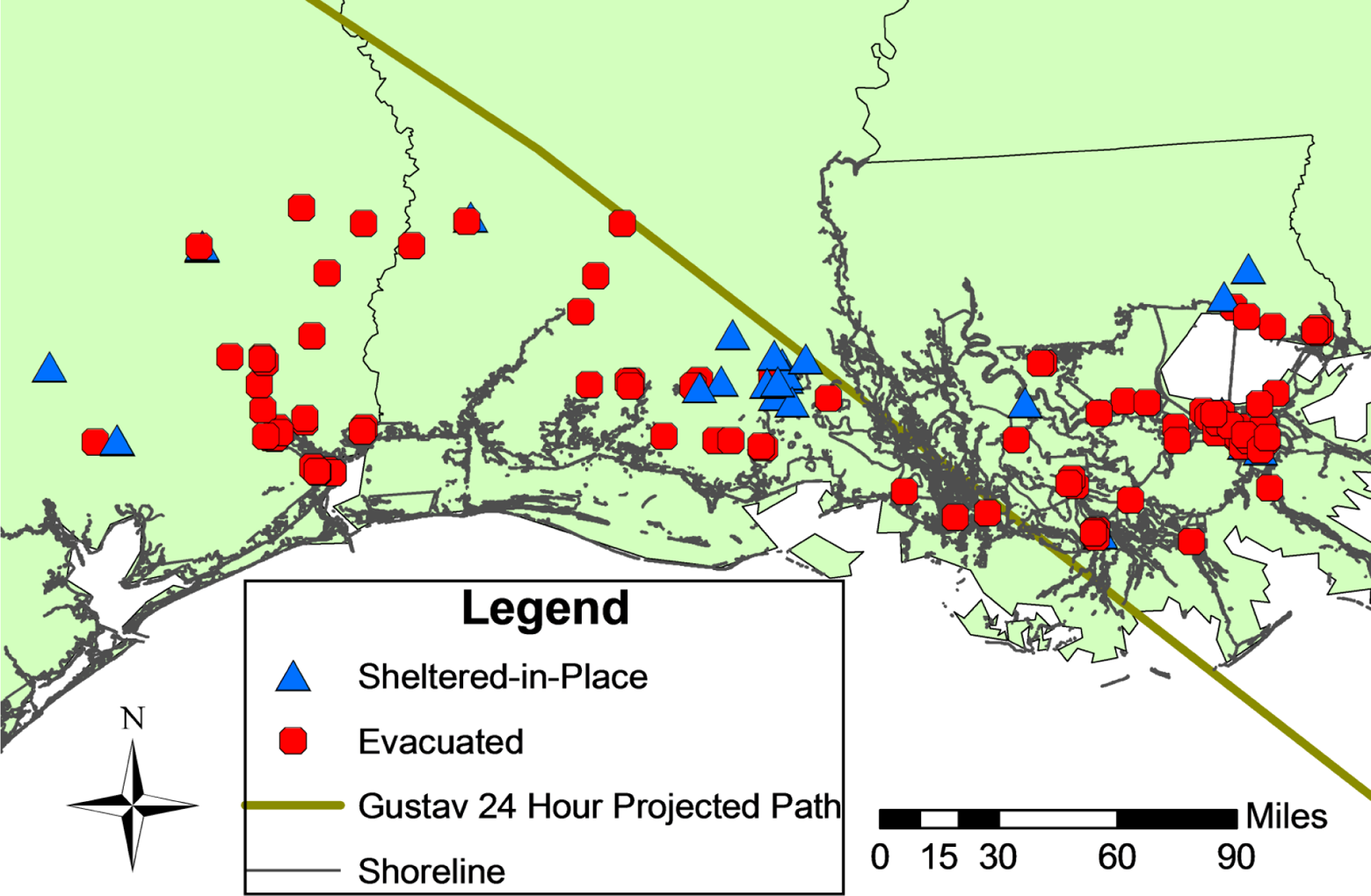
At-risk nursing homes for Hurricane Gustav that evacuated and sheltered in place.
Sample
We evaluated long-stay (>90 days), Medicare eligible, nursing home residents who resided in an at-risk nursing home for at least 3 months prior to the date of landfall. At-risk nursing homes were defined as those homes geographically located in parishes or counties that were included in the National Weather Service’s initial hurricane watch at 48 hours and the subsequent warning zone at 24 hours. Additional nursing homes were included if they were located in parishes or counties where at least 1 nursing home was known to have evacuated based on information provided by the state nursing home association. Nursing homes from counties or parishes where there were no known evacuations and those without 3 years of consecutive data were removed.
Dependent Variables: Morality at 30 and 90 Days
Information on the date of death was determined from the Medicare denominator file. Using data from Medicare files, the prehurricane period (3 months prior to landfall to 4 days prior to landfall), 30-day, and 90-day mortality rates were established for exposed patients. A date 4 days prior to each storm was selected due to potential morbidity and mortality associated with evacuations that commenced on or after that date but before storm landfall. To our knowledge, no nursing homes evacuated for Hurricane Gustav prior to this date. The exposure group was then compared to a control population residing in the same nursing homes during the same period of time for the 2 nonhurricane years.
Independent Variables: Cognitive Status and Evacuation
Residents with seriously impaired cognitive status were identified as those with a Cognitive Performance Scale (CPS) score greater than 5 (a score of 5-6 indicating severe cognitive impairment). The validity of the CPS to detect cognitive impairment in long-term residents has been established. 17 The CPS uses 5 MDS items (comatose status, decision making, short-term memory, making self-understood, and eating) to categorize the cognitive status of nursing home residents. In the identification of cognitive impairment, the CPS demonstrates substantial agreement with the Mini-Mental State Examination, with a reported sensitivity and specificity of .94 (95% confidence interval [CI]: .90-.98) and .94 (95% CI: .87-.96), respectively.
Residents were considered to have evacuated if they resided in facilities that completely evacuated prior to Hurricane Gustav’s landfall. Data on a facility’s evacuation status were obtained from the Louisiana Department of Health and Hospitals. Telephone confirmation with individual facilities was made whenever questions existed as to whether nursing homes completely evacuated. Nursing homes that evacuated after landfall for any reason were considered to have sheltered in place for the purposes of this analysis.
Control Variables Analyses
We used a difference-in-differences model to estimate the impact of evacuation on each outcome. 18 This approach is valid only under a restrictive assumption that changes in the outcomes of both groups would have followed similar trends over time in the absence of the evacuation. 19 Although such an assumption cannot be definitively tested, because no change in mortality was reported for the 2 previous years (2006-2007), we assume that would have continued on for 2008.
Independent 2-group t tests were conducted to compare the evacuated and nonevacuated groups at baseline in terms of demographic characteristics and resident acuity. We conducted unadjusted difference-in-differences analyses, and then examined difference-in-differences effects after adjusting for residents’ demographic characteristics and acuity. The multivariate difference-in-differences model is as follows:

where Outcomeit is the major outcome of interest (mortality at 30 and 90 days). CPS is a dummy variable for high CPS score, and B 1 captures the potential differences between those with a high CPS score and those who have a CPS score less than 5. The dummy variable Evacuation represents whether or not the resident resided in a facility that evacuated for Hurricane Gustav, and B 2 captures the change in outcomes of interest if the resident was in a facility that evacuated in 2008. The coefficient B 3 is the parameter of interest: B 3 measures the effect of evacuation status on the residents with a high CPS score (ie, difference-in-differences). X is a matrix of covariates, including year dummy variables, and a number of other resident characteristics that the literature has shown to be related to mortality: resident characteristics (male, Black, and age), and indicators of resident acuity (body mass index, cancer, congestive heart failure, diabetes, feeding tube, CPS score, Changes in Health, End-stage disease, and Signs and Symptoms Scale score, percent ambulatory, and acuity index). Given the size of our data set, least-squares models estimations of linear probability regression models are presented. Although this approach does not recognize the binary nature of the mortality measure, it facilitates the tractable estimation of these models, which are based on a large number of observations and an expansive set of regression controls. We include facility fixed effects to control for time-invariant differences in mortality between facilities; robust standard errors are clustered at the facility level.
Results
Sample and Baseline Characteristics
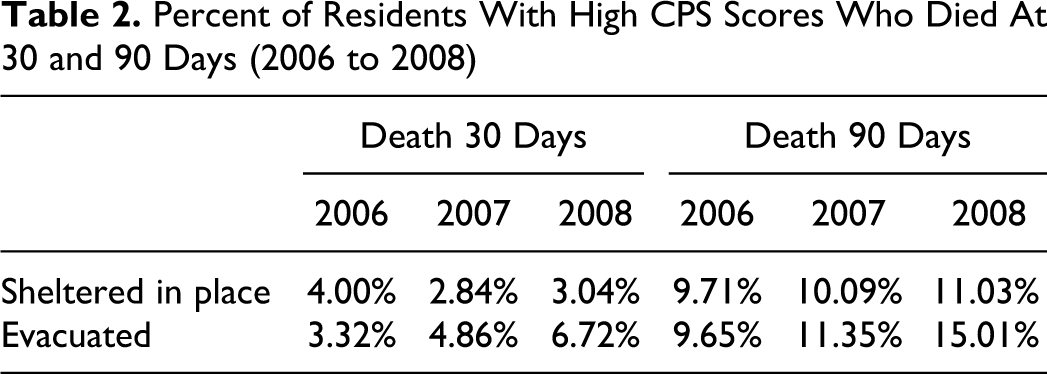
The data set included 21 255 residents of 119 at-risk nursing homes over 3 years of observation. Of these, 18% (3745 residents) were severely cognitively impaired (Table 1) and a total of 5036 residents (82% of nursing homes) evacuated for Hurricane Gustav. Over the study period, approximately 2.4% of residents died at 30 days and 6.7% of residents died within 90 days and death rates were higher in 2008 compared to the 2 prior years (Table 2). Results from a series of 2 sample t tests indicate that there were no significant differences at baseline in resident characteristics and acuity between facilities that evacuated and those that sheltered in place (results not presented).
Variable Description, Aggregated Over 2006 to 2008 (N = 21 255 Individual-Years from 119 Freestanding Nursing Homes)
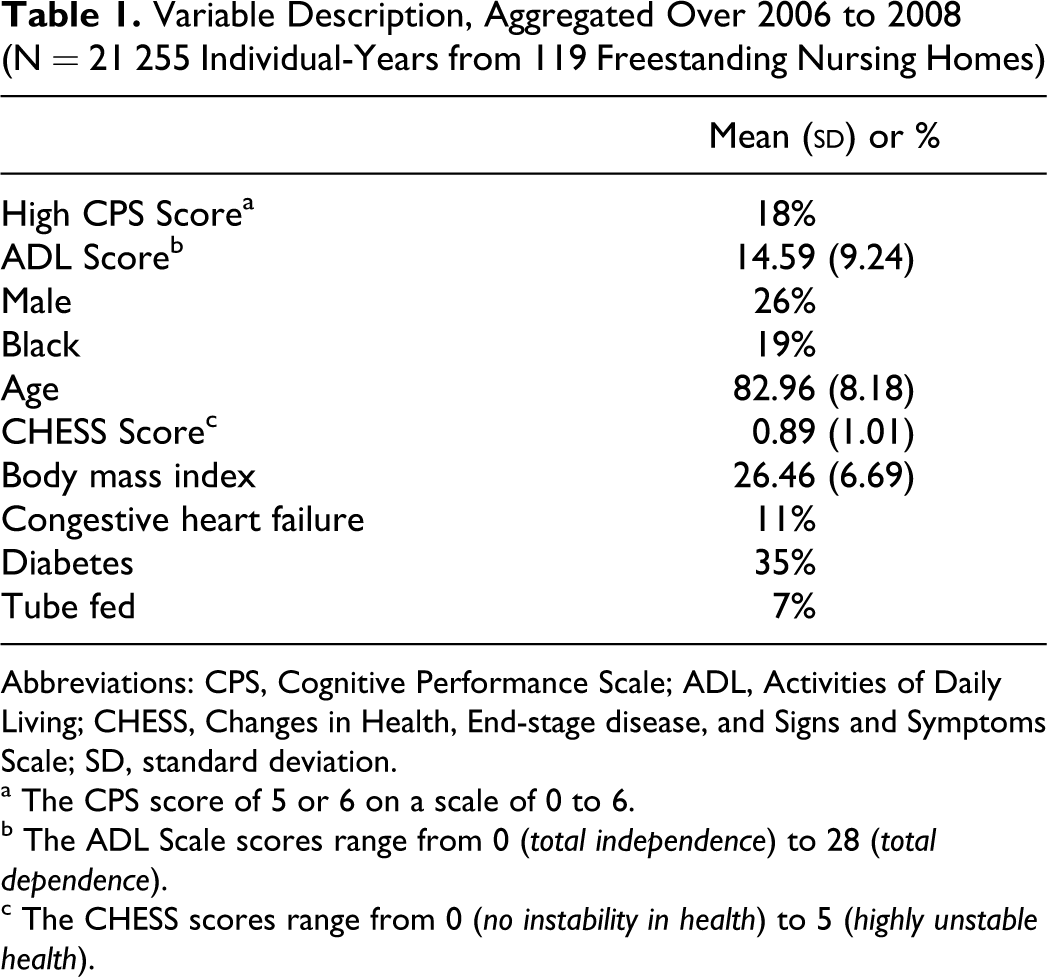
Abbreviations: CPS, Cognitive Performance Scale; ADL, Activities of Daily Living; CHESS, Changes in Health, End-stage disease, and Signs and Symptoms Scale; SD, standard deviation.
a The CPS score of 5 or 6 on a scale of 0 to 6.
b The ADL Scale scores range from 0 (total independence) to 28 (total dependence).
c The CHESS scores range from 0 (no instability in health) to 5 (highly unstable health).
Percent of Residents With High CPS Scores Who Died At 30 and 90 Days (2006 to 2008)
The difference-in-differences estimator (evacuated × high CPS score, which is indicative of severe cognitive impairment) indicate there is a 2.8% point increase in death at 30 days for residents with high CPS scores who evacuated for Hurricane Gustav, controlling for resident demographics and acuity (Table 3). When benchmarked against the average nursing home resident rate of death at 30 days, this finding translates into a 218% increase in mortality at 30 days for individuals with high CPS scores that evacuated for Hurricane Gustav. Thus, if all residents with a high CPS score were evacuated, there would be approximately 1400 additional deaths over the period of study. Results from the difference-in-differences regression modeling the outcome resident death at 90 days, indicated there was a 3.9% point increase in the mortality rate at 90 days for individuals with a high CPS score that evacuated for Hurricane Gustav (Table 4). If all nursing homes evacuated their residents with high CPS scores, a 158% increase in mortality at 90 days relative to the dependent variable mean over the study period would occur. This would translate into approximately 2250 additional deaths at 90 days over the period of study.
Evacuation and 30-Day Mortality, Regression Results a
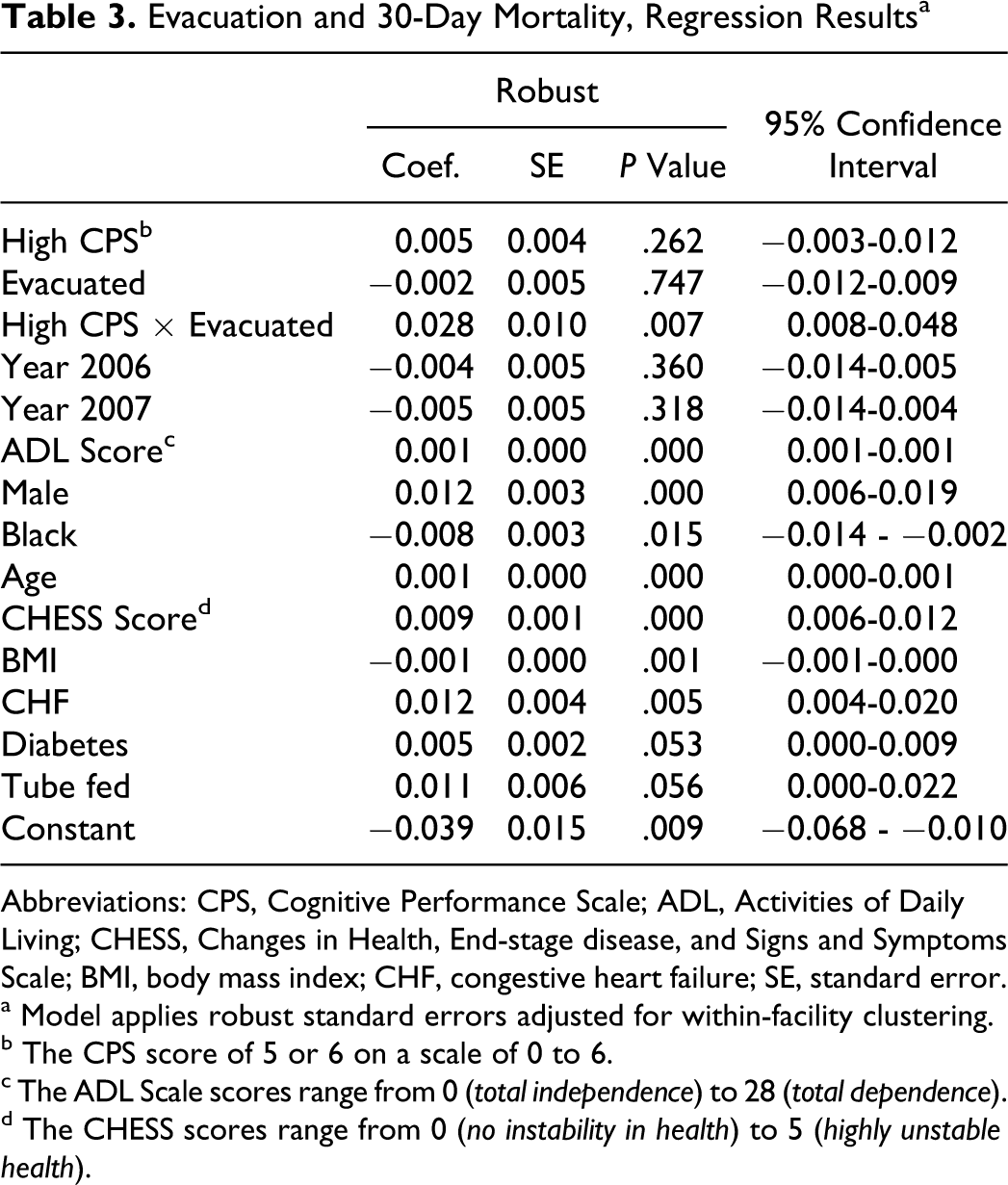
Abbreviations: CPS, Cognitive Performance Scale; ADL, Activities of Daily Living; CHESS, Changes in Health, End-stage disease, and Signs and Symptoms Scale; BMI, body mass index; CHF, congestive heart failure; SE, standard error.
a Model applies robust standard errors adjusted for within-facility clustering.
b The CPS score of 5 or 6 on a scale of 0 to 6.
c The ADL Scale scores range from 0 (total independence) to 28 (total dependence).
d The CHESS scores range from 0 (no instability in health) to 5 (highly unstable health).
Evacuation and 90-Day Mortality, Regression Results a
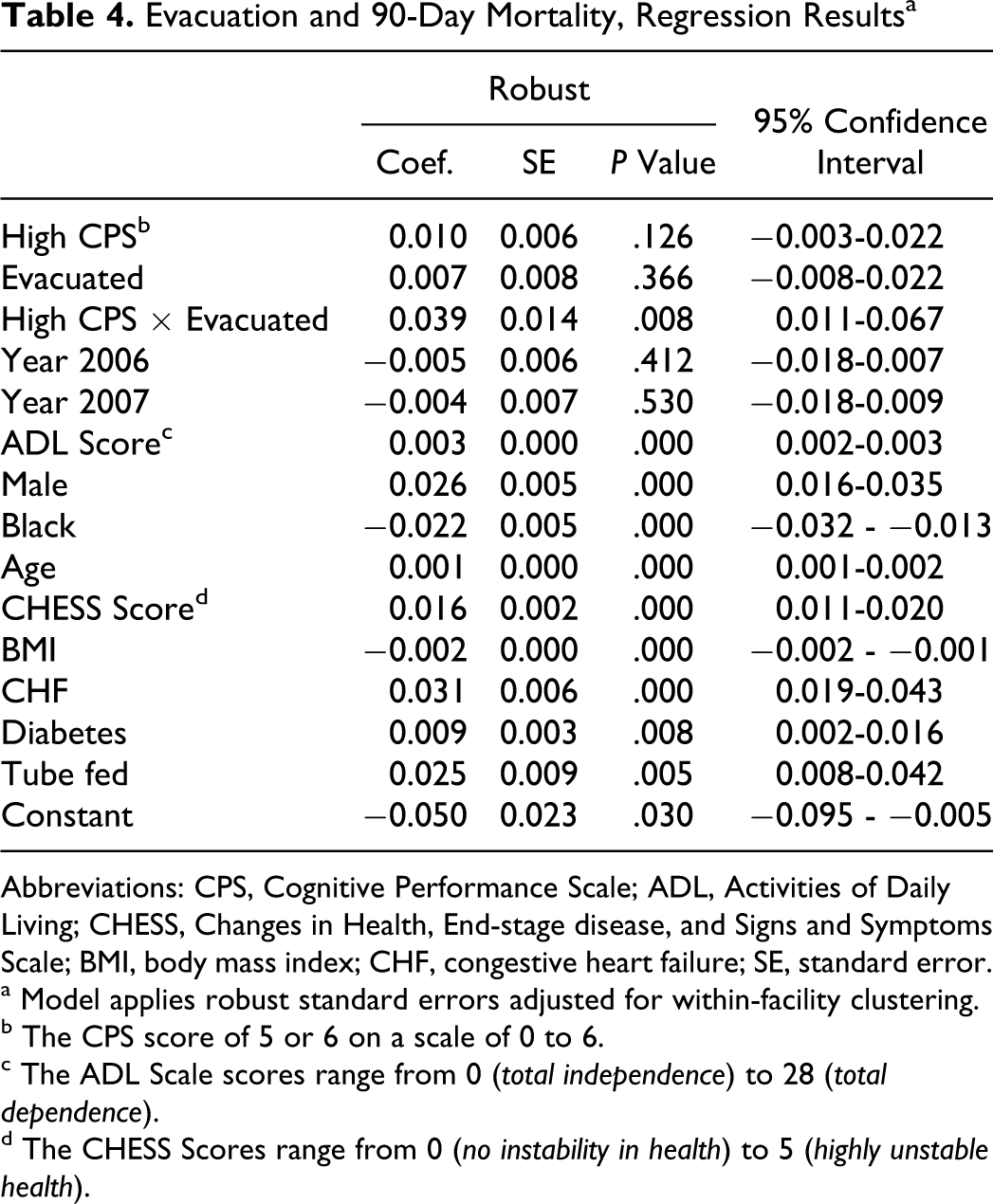
Abbreviations: CPS, Cognitive Performance Scale; ADL, Activities of Daily Living; CHESS, Changes in Health, End-stage disease, and Signs and Symptoms Scale; BMI, body mass index; CHF, congestive heart failure; SE, standard error.
a Model applies robust standard errors adjusted for within-facility clustering.
b The CPS score of 5 or 6 on a scale of 0 to 6.
c The ADL Scale scores range from 0 (total independence) to 28 (total dependence).
d The CHESS Scores range from 0 (no instability in health) to 5 (highly unstable health).
Discussion
Nursing home staff encounter unique challenges when providing care to residents during hurricanes. 20 –27 For nursing home residents, it is documented that existing physical and mental health conditions are exacerbated by disaster-related activities such as evacuation to another facility and disruption of day-to-day activities. Additionally, they face increased risk for adverse outcomes, such as morbidity, mortality, and hospitalizations. 28 –31 This study reveals that residents with severe cognitive impairment who are evacuated are at increased risk of death at 30 and 90 days post-move.
The findings from this study are important for several reasons. As our population ages and an increasing number of older adults live with dementia, it is reasonable to anticipate that use of nursing home services for the later stages of dementia will likely increase during the next 3 decades. Moreover, to reduce Medicaid costs for nursing homes and to respond to consumers’ requests to remain in the community, both the federal government and states have launched programs to “rebalance” long-term care services. Under such programs, individuals with personal care needs that qualify them for nursing home benefits, receive Medicaid payments for home and community-based services in lieu of nursing home care. 32 Many of these programs have reduced the costs of caring for frail elders and disabled individuals who may now live in the community. However, reducing the numbers of low-care residents increases the average acuity of the remaining long-stay nursing home residents. 33
Although hurricanes are just one type of disaster, we speculate that the findings of this research are generalizable to other types of disasters with some advance warning, such as floods, fires, and tornados. By identifying residents who are at greatest risk during catastrophic events and by developing policies, programs, and training that might serve to protect the most vulnerable, long-term care providers, clinicians, public health workers, and emergency responders will be better equipped to prepare for and respond to the needs of this subgroup.
For example, if evacuation is imperative, it may be beneficial for at-risk residents to be moved into the homes of family members where temporary care can be provided in an environment that may be less chaotic. It is unknown whether earlier evacuation, under more calm conditions, would be advantageous for people with severe dementia. On the other hand, managing the environment to reduce stressors can include simple actions that have potentially profound effects. For example, a study conducted with nursing home residents after the terrorist attacks on September 11, 2001, showed the adverse effects of prolonged TV viewing of the event. The investigators speculated that because intentional death and harm is considered especially heinous, it elicits strong reactions that appear to enhance retention of information, even in residents diagnosed with Alzheimer’s disease. 34 Although when compared to cognitively intact residents, those with dementia were more likely to remember personal (eg, how they heard the news) rather than factual information (eg, details of the attack); these 2 groups did not differ in their level of emotional intensity (ie, sadness, anger fear, frustration, confusion, and shock). 34 It is possible that turning off the TV or limiting exposure to disturbing programming may reduce residents’ psychological distress when their facility is under hurricane threat. Constantly viewing the trajectory of the “cone of uncertainty” and listening to animated descriptions of where the storm might make landfall, does little to calm those who have limited ability to independently take action or fully understand the imminent danger.
A study of nursing home administrators and directors of nursing found that nearly 90% would be interested in providing some type of predisaster, resilience intervention to residents if a program was made available. 35 At present, the emphasis is on maintaining the physical safety of residents and not on training staff to meet their mental health needs during disasters. Yet, numerous studies have consistently demonstrated that physical and mental health are closely intertwined. 36 Although a growing body of research shows that evidence-based programs to build resilience are effective, 37 –39 a number of constraints hinder the formal development and testing of a resilience building interventions within long-term care settings. There are no regulations that require this type of training, no reimbursement for staff providing resilience building interventions, and limited recognition of the potential value of implementing such a program. Moreover, the development and testing of a new, evidence-based predisaster resilience intervention is costly and time consuming.
Two programs, both in the public domain, maybe useful to nursing home staff who would benefit from training on managing the adverse mental health effects of disasters on residents postdisaster. Psychological first aid techniques can be used by all staff, not just licensed clinical practitioners, to enhance resident adaptive coping and resilience when evacuating or sheltering in place. The psychological first aid manual for nursing homes also includes behavioral interventions that are appropriate with residents with moderate-to-severe dementia. 20 An e-learning tool, “Frailty, Dementia and Disasters: What Health Care Providers Need to Know” increases the awareness of factors that contribute to vulnerability of residents and guides staff on how to help make the environment safer for older adults during emergencies and disasters. 40 Although additional research needs to be conducted to better understand how these programs are used during disasters and to explicate what types of mental health and quality of life benefits are derived by residents, both programs show promise and have been well received by staff.
Beyond mental health care, programs that generally prepare nursing homes for disasters include Mather LifeWays’ PREPARE 41 program and the Emergency Management Guide for Nursing Homes: National Concepts and Practices for All-Hazards Planning, developed by the Florida Health Care Association and the University of South Florida. 42 Both programs provide essential information needed for facilities to develop all-hazard plans, train staff in preparedness activities, including disaster drills and table top exercises, and recommend ways to recover after the event. These preparedness programs were developed in response to the post-Hurricane Katrina nursing home resident deaths and the highly critical Department of Health and Human Services’ Office of the Inspector General report that charged nursing homes with having inadequate disaster preparedness plans. 43
In response to the report, the Center for Medicare and Medicaid Statistics recommended new emergency preparedness checklists for nursing homes, but did not promulgate any new rules. Consequently, the Office of the Inspector General in a follow-up report indicated that many of the gaps identified after Hurricane Katrina, such as poor collaboration with local emergency management agencies and unreliable transportation contracts, remained problems for nursing homes. 44 This report also reinforced the importance of more attention to the preparedness activities of nursing homes when caring for their frail and cognitively impaired elders during disasters.
This research has several limitations. First, partitioning out mortality and morbidity-related storm effects versus other disruptions is not possible. Second, our research assumed that all residents in a nursing home evacuated together (in groups dispersed to various other facilities) and remained together during the hurricane. Because of the lack of data about the precise location of individual residents during the days of the storm, it is possible that some residents were temporarily sheltered by local family or friends instead of evacuating to another facility and were returned to the nursing home after the storm without ever having been discharged from MDS. However, even if some residents remained with family during the storm, they still evacuated, and our study captures the impact of relocation for these residents as well as for residents who relocated to less familiar surroundings.
Despite these limitations, this study is the first to quantify the deleterious effects of evacuation on residents with severe dementia. Although additional research needs to be done to fully understand the impact of evacuation on residents, our findings offer a cautionary warning to disaster planners, policymakers, and long-term care administrators. Research needs to be conducted that determines the optimal time for evacuation of residents that is based on cognitive status and health conditions, identification of best methods and conditions for transporting those who are at high risk, modifications to the environment that could prove beneficial in reducing resident distress, and refinement of psychological first aid techniques to enhance coping and resilience. Interventions need to be developed and tested to determine the best methods for protecting this at-risk population when there are no other options than to evacuate the facility.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institutes of Aging (RO1AG030619-01A2); John A. Hartford Foundation (#2006-0172).