
Abstract
Objectives:
In certain health care facilities, the staff commonly wear uniforms for dementia care. Wearing uniforms are often believed to improve the well-being of institutionalized people with dementia (PwD) by facilitating orientation and preserving hygiene. However, when studied more thoroughly, it appears that their use counters to person centeredness. This study aims to investigate the impact of wearing uniforms on the quality of life (QoL) of institutionalized PwD.
Method:
A natural experimental design was operated in 4 special care units (SCUs) in France. Two SCUs served as an experimental group (caregivers wearing street clothes except when performing hands-on physical care; N = 13) and 2 served as a comparison group (caregivers wearing uniforms; N = 14). The QoL of PwD was measured using the QoL-Alzheimer’s Disease scale, and focus groups were carried out with caregivers.
Results:
Overall and significantly enhanced QoL scores were observed for the experimental street clothing staff group when compared to the uniform group. Caregivers also reported subjective impressions of overall beneficial outcomes for PwD when the caregivers were not wearing uniforms and reported feeling more at ease when interacting with them.
Conclusion:
Results are discussed in terms of intergroup relationships, living and working conditions, and ethical issues.
Introduction
It is common to encounter caregivers wearing uniforms in special care units (SCUs) for people with dementia (PwD). But the rationale for wearing such attire is not evident. Dementia can in no way be considered a contagious or infectious disease; consequently, such hygienic measures that are found in hospital-like environments are not necessarily suitable for care of PwD unless specific medical care is needed.
A Brief History of Nurse’s Uniforms
Uniforms appear to be central to the perception of nursing. Although the use of uniforms in nursing originates from religious orders and military influence in the 19th century, Pearson and collaborators 1 note that the continued support for uniformity in attire can be attributed to a strong influence of tradition within nursing. These authors trace the earliest references to uniforms in modern nursing date from the Deaconesses at Kaiserworth, from whom Florence Nightingale received her initial training. Nightingale played a significant role in sanitary control in the 19th century, especially at the time of war. Stubbs and colleagues point out that until the early 1980s uniforms had only undergone minor changes since Nightingale’s time. 2 Until the 1980s, medical studies concerning uniforms mainly focused on their relation to hygiene, durability, mobility, and patient handling. 3 – 5 According to Dolan, 6 nurses’ uniforms and their ornaments (badges, capes, medals), like military uniforms, served as indicators and symbols of hierarchy and power relationships within the medical staff.
From the early 1960s onward, questions about social processes related to attire began to appear, especially in the psychiatric fields. 7,8 Attire has generally been considered a contribution to professional image and representation of hierarchy in the medical corps among staff, students, and patients in hospital-like environments. 1,9,10 In psychiatry, greater concern was focused on the quality and quantity of relationships between psychiatric staff and inpatients when wearing uniforms or street clothes. 11
Social Processes Involved in Attire
McNeill, Kreuter, and Subramanian,12(p1011) quoting the Institute of Medicine, 13 emphasize the fact that the social environment in which individuals evolve influences their behaviors by “shaping norms, enforcing patterns of social control, providing or not providing environmental opportunities to engage in particular behaviours, reducing or producing stress, and placing constraints on individual choice.” The transactional approach, as defined in environmental psychology and socioecological models, emphasizes that both physical and social environment are powerful influencers of behavior. They either reduce stress in uncomfortable situations leading individuals to adopt healthy and adapted behaviors or they are perceived as obtrusive, leading to maladaptive behaviors. 14,15
Although several studies have shown how attire could positively affect perception of professional image, skills, and professionalism, 9,16,17 other studies have shown deleterious impacts of attire. In any case, it is important to understand the social processes involved in wearing uniforms in a community service context, taking into account the situation, symbolic meaning, and the expectations of peoplewith or without dementia and their families.
As emphasized by McNeill et al, 12 research in social cognition demonstrates the importance of addressing behavior at multiple levels of influence, considering how interacting social and physical environmental factors simultaneously shape behaviors. These authors also suggest that these factors may also influence health and behavioral outcomes by influencing supportive or unsupportive behaviors when people are faced with daily stressors or stressful events.
Identity and Competency
Frank et al 18 demonstrate how sports uniforms can affect the identity and behavior of persons wearing them and the expectations of the persons perceiving them. They emphasize that in different contexts these variables may have different meanings. The social processes revealed in their study can help us understand the mechanisms involved in wearing uniforms in care contexts. These processes primarily refer to the malleability of the self-concept, social judgment theory, and behavioral adjustment. If we extend the observations of Frank et al 18 to the context of care, the fact that a person wears a uniform of some kind may help that person fit a professional identity and the respective behavioral competencies required of that position. Employing similar mechanisms, attire is also likely to affect social judgment and perception of the person wearing the uniform and thus provide cues to others who relate to that person in a care context to adjust their behavior accordingly.
Several articles suggest that in a psychotherapeutic context not wearing uniforms promotes interpersonal skills among staff when dealing with patients by attenuating the symbolic authoritative value of the attire. Although there is little research to confirm or invalidate this hypothesis, some authors suggest that wearing street clothing may facilitate staff’s therapeutic commitment and empathy processes. 8,11,19,20
Obedience and Authority
Milgram’s 21 well-known experiment on the impact of wearing uniforms on obedient behavior in a mock experimental setting is also instructive. Although Milgram did not investigate whether wearing uniforms influenced obedience to authority directly, one of his experimental conditions suggests it implicitly. In Milgram’s experiment, subjects were asked to administer electric shocks to their peers according to whether or not their peers answered certain test questions correctly. Obedience drastically decreased to 20% when the experimenters making the request were presented as ordinary civilians, whereas it reached over 60% when experimenters were presented as scientists—scientists wore white coats, whereas civilians wore casual clothing. Furthermore, Bickman’s 22 experiment on making a request to people in the street shows that requests are more often complied with when the experimenters making the request wear a uniform representing authority than when they are not in uniform. Three conditions were tested: civilian clothing, a milkman’s uniform, and a guard’s uniform. These experiments suggest that uniforms can lead to obedience when perceived as authoritative.
Both concepts—authority and obedience—can be observed in medical contexts and organizations. In similar contexts, they can prove useful in maintaining the order and hierarchy needed for medical procedures to be carried out efficiently and effectively. In a study on the impact of nurses’ uniforms on perceptions of nurse professionalism, Albert and colleagues 16 show that pediatric populations and their adult visitors did not judge competencies of nurses based on their attire, although, in a medical context, warmth of the attire was preferred. All these studies suggest that the impact of uniforms must be carefully considered before uniforms are worn in a caring, educational, or even pedagogical context.
Uniforms and Dementia Care
People with dementia are particularly vulnerable and can easily be overwhelmed by unfamiliar and disorienting contexts. Current trends in dementia care emphasize the need to promote person-centered approaches as described by Kitwood, 23 requiring fulfillment of 5 basic needs: attachment, identity, comfort, occupation, and social integration.
Although the trend among care providers is to promote person-centered care and the use of social relationships between staff and PwD, when questions about wearing uniforms in SCUs for PwD are discussed, hygiene, care, and ethics are the issues raised. Preconceived ideas and false beliefs about wearing uniforms for dementia care commonly target ease of orientation, environmental cuing, and body care. Reluctance of caregivers to street clothing during working hours is common in community services for PwD. According to the authors’ experience with caregivers in SCUs, concerns for hygiene are the most frequently given explanation for continuing to wear uniforms.
Although some authors question the utility of uniforms for professional caregivers in community services for PwD and the congruence with person-centered care, no research has been conducted concerning the perception of uniformed staff by PwD, nor its impact on quality of life (QoL) and behavioral and/or cognitive symptoms. A simple publication concerning uniforms in dementia care was a correspondence in The Psychiatrist, suggesting that staff wearing uniforms were more reassuring for PwD receiving care. 24 Results of googling “dementia” and “uniforms” on the Internet mainly refer to discussion forums where individuals voice opinions in local newspaper articles on community services that have introduced some sort of staff uniform or which have, on the contrary, dispensed with uniforms, or health care equipment retailers selling “dementia care tunics,” “scrubs,” or “tabards” as if dementia care required specific equipment of this kind.
Eval’zheimer is a psychosocial model of intervention developed by the Fondation Médéric Alzheimer, in France. It is intended to fit caring practices and environmental design to institutionalized PwD. 25 This model is based on the general assumption that nonpharmacological factors such as interior design and care practices can help reduce symptoms of people with Alzheimer’s disease (AD). 26 The model not only adopts a person-centered care and personhood approach 27 but also incites caregivers to consider PwD as elderly individuals’ alter egos that need to be supported more thoroughly throughout daily life. During the evaluation of the model of intervention, care practices such as shared meals 28 and night shifts 29 were assessed. For the present study, caregivers in the 2 SCUs independently decided not to wear uniforms, hypothesizing that not wearing uniforms would be more congruent with a domestic environmental design. Thus, the experimenters hypothesized that not wearing uniforms would positively influence the quality of care and therefore the QoL of residents in SCUs.
Designs and Methods
Procedure
The study was conducted in 4 French nursing homes’ SCUs—2 in Paris suburbs, 1 in Vienne (250 miles from Paris), and 1 in Nevers (150 miles from Paris)—were included in this study. The 4 units were a subset of 8 SCUs in which a larger randomized control trial was conducted to evaluate a training program coupled with an environmental design intervention involving 8 units in 8 different nursing homes across France. In the larger study, units were randomly assigned to the experimental group or the comparison group. All 4 units of the present study were part of the experimental group. In all the 4 units, the staff participated in a 12-session training program on dementia care conducted by a single trainer, including supervision sessions and workgroups. In addition, an environmental design intervention was implemented in each SCU to improve residents’ orientation and well-being. The environmental design interventions, homogeneous between groups with a budget limited to 7000 Euros, mainly consisted of changes concerning the use of space (eg, space arrangement, furniture, decor, linen, etc). External evaluators were hired to collect quantitative data and were not provided with the purpose of the study in order to preserve blindness.
During workgroups in the training program, the staff members of 2 of the 4 units independently chose not to wear uniforms. This decision was mainly taken so that the social environment would be consistent with the residential and domestic character of the physical environment. Staff members of both the groups also expressed their desire to try a different direction in their care practice that was related to residential care rather than hospital care. This sets the stage for the natural experiment that is the subject of this article. The units with staff not wearing uniforms served as the experimental group, while the other 2 units were chosen to serve as comparison groups. These decisions regarding uniforms and the fact that all 4 of the units participated in the same larger study enabled a framework to be set for a “natural” experimental design.
Description of the Intervention
Two sets of identical measures were administered to the residents for the purpose of the general study, one before the training and environmental interventions and one 3 months after it. Whether or not to wear uniforms and when to wear uniforms were discussed in order to reach consensus among the staff members. The experimental group decided to wear uniforms in the morning when helping residents with showering and dressing and to wear street clothes when these tasks were completed. However, if a resident needed hands-on body care during the day, they decided they would wear overblouses.
Measures and Data Collection
The Mini-Mental Status Examination (MMSE) 30 is a widely used screening tool that provides a descriptive view of the participant’s cognitive functioning. This test includes simple questions and problems concerning orientation to time, orientation to place, registration, attention and calculation, recall, language, repetition, and complex commands. The MMSE provides a total score ranging from 0 to 30, with lower scores indicating a greater cognitive impairment. The MMSE was administered once at the beginning of the study. It was not possible to administer the MMSE with some participants.
The French version of the Quality of Life-AD 31 – 33 (QoL-AD) was used for this study. The QoL-AD is a brief, 13-item measure designed specifically to obtain a rating of the patient’s quality of life from both the patient and the caregiver. It uses simple and straightforward language and responses and includes assessments of the individual’s relationships with friends and family, concerns about finances, physical condition, mood, and an overall assessment of QoL (Table 1). Patients with MMSE scores of 10 or higher can usually complete it with no problems; and in patients with scores below that, the caregivers can continue to complete it. For this study, caregivers completed the measure as a questionnaire about their patients’ QoL. The 13 items of the QoL-AD are rated on a 4-point scale, with 1 being poor and 4 being excellent. Total scores range from 13 to 52.
Description of the Items of the QoL-AD. 32
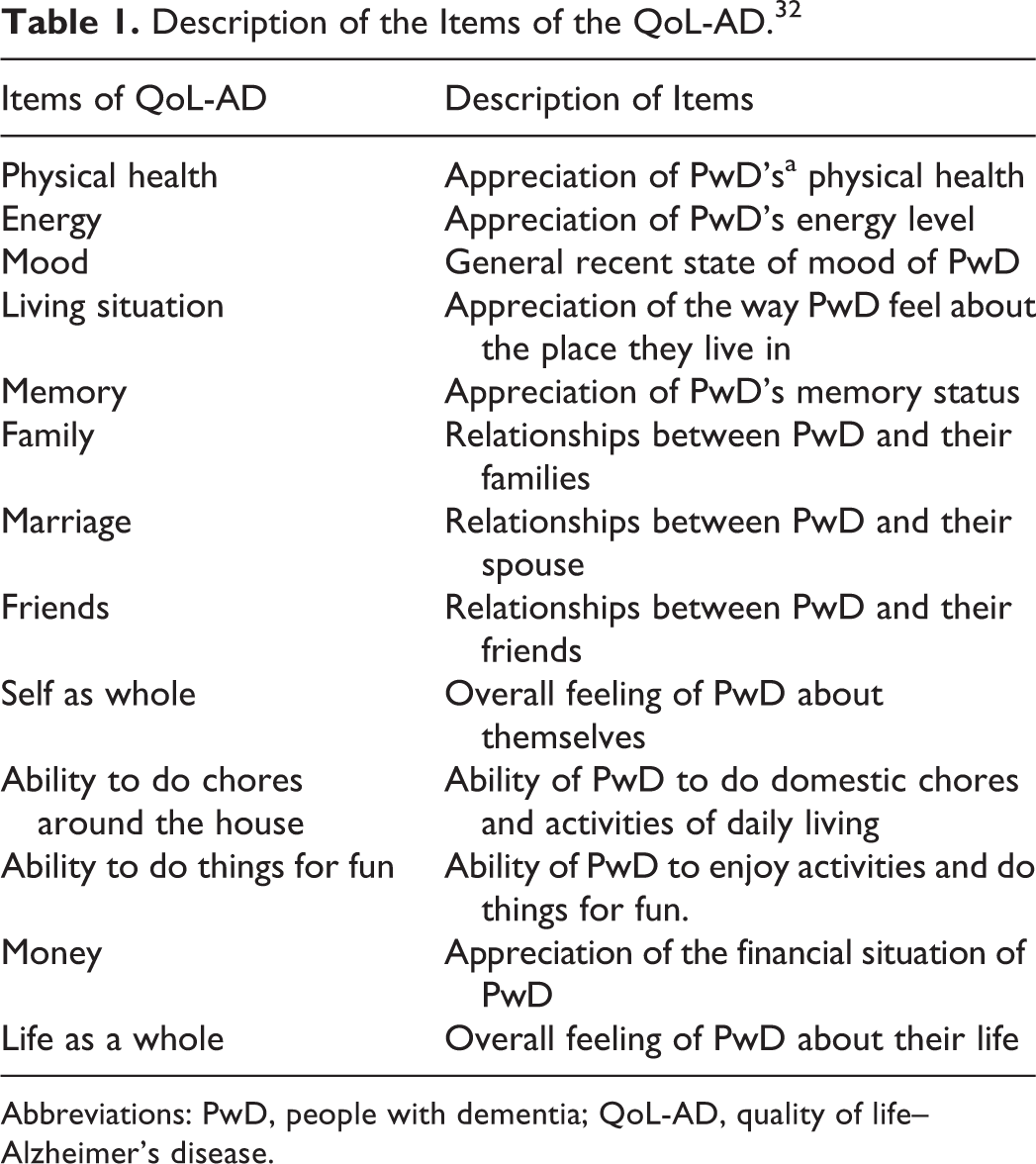
Abbreviations: PwD, people with dementia; QoL-AD, quality of life–Alzheimer’s disease.
In addition to the MMSE score and QoL-AD, observations of the staff in the SCU that chose not to wear uniforms were collected. These observations were collected during the weekly training sessions as well as at a focus group at the end of the study. Reports of training sessions and focus group were written by the trainer and provided qualitative material concerning implemented environmental design changes and implemented practice changes, from the perspective of staff and the trainer. Reports systematically reflected observed changes concerning care, organization, policy, resident, and family issues.
Participants
A total of 35 institutionalized people with dementia of Alzheimer type according to the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition, Text Revision [DSM-IV-TR]) diagnostic criteria were included in this study, of whom 7 died during the study and 1 was transferred to another service. The final experimental group included 13 participants (1 male and 12 females), and the comparison group included 14 participants (all females). The only male participant did not differ from the female participants in terms of age, length of institutionalization, and MMSE; so it was decided not to reject him.
Most participants had language skills that enabled them to communicate with caregivers and express their basic needs and feelings. Admission policies of facilities in which the experiment took place requested assessment of residents for groups to be homogeneous within the SCUs and in order for them to fully benefit from services provided by the SCUs. When assessments of medical staff clearly indicated that residents were not benefiting from the services anymore, it was usually suggested to residents and their families that transfer into another unit would probably better meet their needs.
The mean (M) age was 84.08 years (standard deviation [SD] = 6.55) for the experimental group and M = 80.78 years (SD = 9.86) for the comparison group (t 25 = −1.01; P = .32; not significant [ns]). Mean institutionalization length was M = 2.61 years (SD = 1.84) for the experimental group and M = 1.66 years (SD = 1) for the comparison group (t 25 = −1.68; P = .103; ns). Mean MMSE scores of the participants for whom the administration of the test was possible were M = 7.85 (SD = 5.87) for the experimental group and M = 9.37 (SD = 6.39) for the comparison group (t 13 = 0.47; P = .64; ns), indicating overall severe cognitive impairments.
Groups could thus be considered as comparable in age, gender, length of institutionalization, and cognitive impairment. Adapted written and oral information and consent forms were given to all participants and their families. The study design and data collection received approval from the French national agency on computerized personal data collection (Commission nationalede l’informatiqueetdes libertés).
Data Analysis
To analyze the differences between groups on the QoL-AD for the first set of measures, we calculated the above effect using multiple analysis of variance (MANOVA) using Rao F approximation of Wilks Lambda. A Fischer test (ANOVA) on independent and repeated measures was used for specific comparisons between groups and on both sets of measures. Internal consistency of the QoL-AD (α = .86) indicates that the items of QoL-AD are consistent for measuring QoL but are not redundant and sufficiently different to address the same area of concern. Although the QoL-AD was not designed by its authors for this matter, several studies undertook item-by-item analyses either for correlational analyses purposes 34 or for factorial analyses purposes, 35 suggesting that item-by-item analysis on the QoL-AD can be acceptable for research purposes. Thus, analysis of variations for each item of the QoL-AD was undertaken in order to understand the fields of QoL, which were particularly impacted during the intervention.
Qualitative data were extracted from the trainer reports when it specifically referred to the topic of interest for this study and was analyzed manually and anonymously. The data were then classified into semantic clusters according to observations and debates they referred to and summarized in order to concisely reflect to general ideas that were expressed.
Results
Results on the QoL-AD
Preliminary Comparison Between Groups for the First Set of Measures
The MANOVA on the first set of measures of the QoL-AD shows a significant difference between groups (ΛWilks= .09; F 14,12 = 8.1; P > .0004) M scores and SDs for each group are presented in Table 1. Significant differences concerned the items living situation (F 1,25 = 4.85; P < .04) as well as family (F 1,25 = 9.64; P < .005) in favor of the experimental group, and self as whole (F 1,25 = 6.55; P < .02) as well as life as a whole (F 1,25 = 4.71; P < .04) in favor of the comparison group. The comparison of mean global scores did not show any significant differences between the groups for the first set of measures (F 1,25 < 1, ns).
Comparisons Between the Groups for Both Sets of Measures
The ANOVA between groups for both sets of measures (Table 2) shows a significant difference in the overall score in favor of the experimental group (F 1,25 = 6.89; P < .014). Significant differences, all in favor of the experimental group, were found for the items friends (F 1,25 = 11.04; P < .003), self as whole (F 1,25 = 8.39; P < .008), and ability to do chores around the house (F 1,25 = 5.58; P < .03; Table 2).
Mean Scores (SD) and ANOVA on Both set of Measures of the QoL-AD for the Comparison and the Experimental Group.
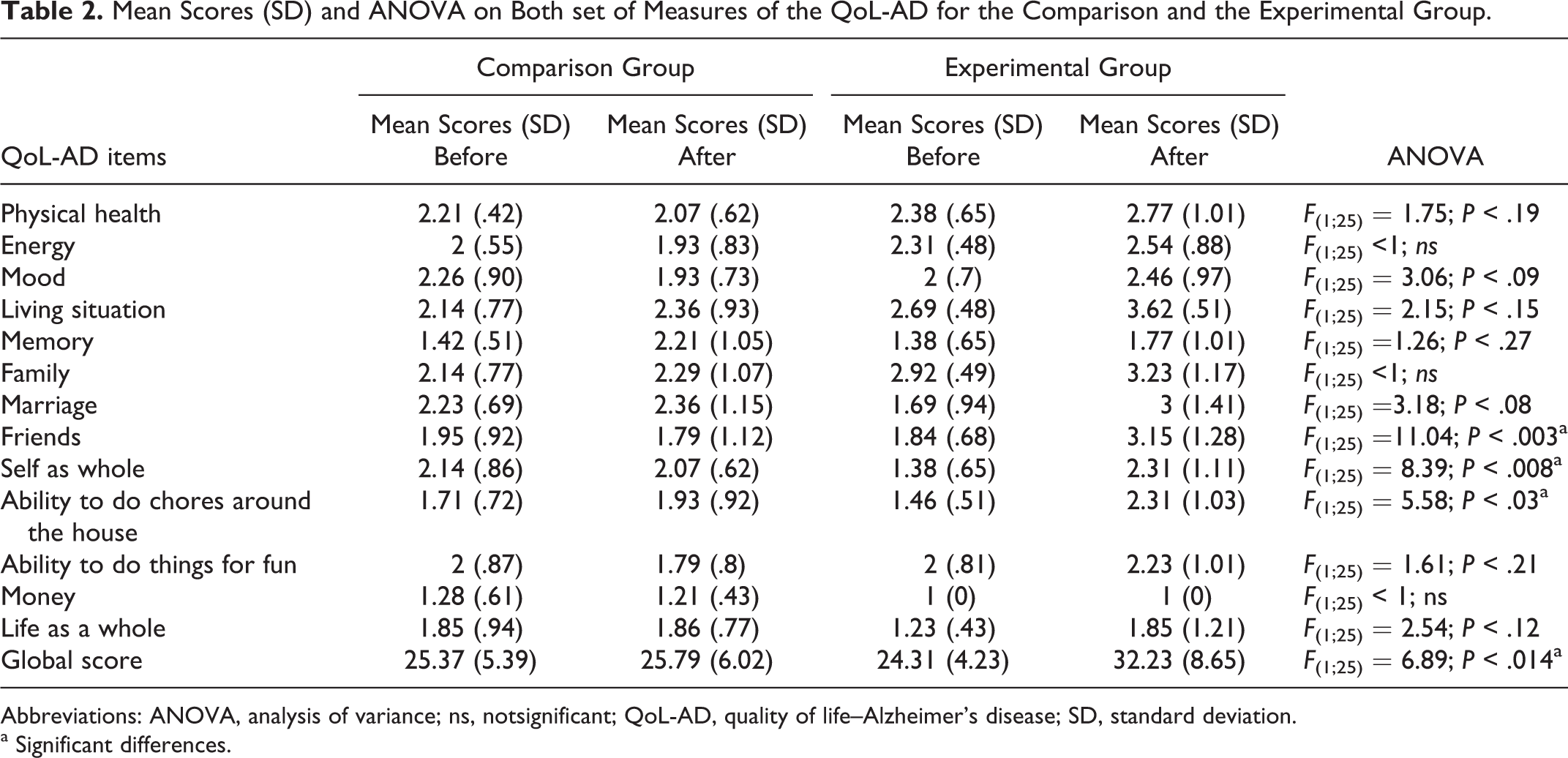
Abbreviations: ANOVA, analysis of variance; ns, notsignificant; QoL-AD, quality of life–Alzheimer’s disease; SD, standard deviation.
a Significant differences.
Qualitative Data
Residents Recognize Caregivers and Compliment Them on Their Attire
Caregivers reported that the residents did not have any problems recognizing them. It was also observed that residents were sensitive to the way the caregivers were dressed and often complimented them on their appearance. This was very much appreciated by the caregivers, because of the effort they had made in choosing their clothes and often resulted in a return of the compliment and conversations about clothing. It was also reported that some of the residents even tried to deduce the mood of the caregivers according to the way they were dressed and the colors they wore.
Residents Adjust Their Behaviors According to the Social Context
It was acknowledged that residents tended to enter into communication with caregivers less to ask for a service than to engage in conversation. In general, when caregivers were in civilian clothes, they seemed to perceive the residents as less demanding and more independent. Caregivers reported that residents engaged more easily in everyday activities such as sweeping the floor, laying or clearing the table, helping with small cooking tasks (eg, making salad dressing, cooking a cake, or preparing starters), folding their clothes, and making their beds. Communication was also reported to be less formal when the caregivers did not wear uniforms than when they wore them. Caregivers stated that residents seemed more easily aware that it was morning when the uniforms were worn.
It Takes Time for Families to Get Used to it
At first, some caregivers reported that certain residents’ family members did not notice them and thought that no caregivers were present in the SCU. Consequently, some of them went to complain directly to the head nurse and/or the director. When the head nurse and/or the director came into the SCU with them to make sure that caregivers were taking care of the residents, they showed the families where the caregivers were. It was thus decided to wear name badges for the benefit of the families. The families, who were initially not enthusiastic about caregivers out of uniform, then expressed their satisfaction with this practice. Caregivers reported having more overall contact with resident families and on more cordial and pleasant terms.
Caregivers Feel More Comfortable and Engage More With Residents
Caregivers reported that it felt more pleasant and comfortable to interact with residents when they wore street clothes and they felt closer to the residents and their needs—more at ease engaging in conversation on intimate subjects. They also reported being more at ease encouraging residents to take part in leisure and/or everyday activities. Caregivers wearing street clothes indicated that some of their coworkers in other services reacted negatively to them for not wearing uniforms, some assuming that they were not really working and others believing that the management staff showed preference for these caregivers. Caregivers of the SCUs in street clothes usually interpreted these attitudes as jealousy.
More Hygienic
Most of the caregivers agreed that wearing the same uniforms for hands-on body care and at meal times was not hygienic. Most caregivers reported that they themselves would not appreciate being taken care of this way nor would they like it for their relatives. Putting on scrubs temporarily if hands-on body care was required during the rest of the day was not reported as annoying or time consuming for any of the caregivers.
Discussion
Results of both quantitative and qualitative data are discussed and compared when they appear to be complementary.
The differences between data sets that appear in the preliminary analysis for the first set of measures of the QoL-AD did not appear to affect further data processing. Only the mean score for the item self as a whole changed significantly in favor of the experimental group in the second set of measures, whereas it was initially significantly higher for the comparison group. The other items did not differ significantly for the ANOVA including the second set of measures.
Judging a Book by its Cover
In our study, not wearing uniforms while taking care of PwD seems to impact QoL positively as measured by the QoL-AD. The QoL-AD score showed significant improvement in PwD when the feeling of self as a whole is compared to the comparison group. This finding can be partly interpreted to be the result of a decrease in a group-based judgment bias similar to the one Bronfenbrenner 36 describes in the mirror-image perception phenomenon in a latent group opposition context. Mirror-image perception is a phenomenon that can be defined as reciprocal views of members of the different groups, usually opposed by some more or less visible and perceptible differences, with each group perceiving itself more positively than the opposing group. According to Pronin 37 (p38) “even when differences between groups are minimal and trivial, people tend to favor ingroups over outgroups.” Social processing requires complex cognitive abilities and skills, thus it is possible that PwD may be more susceptible to forming judgment biases.
As stressed in the introduction of this article, uniforms can be perceived as symbols of an authority or as relating to service, thus emphasizing membership of another group and resulting in an unbalanced relationship. When 2 groups are differentiated by intrapersonal means, such as attire and task, phenomena similar to mirror-image perceptions can be activated. Alternatively, when intrapersonal characteristics of one of the groups are attenuated and similarities of attitudes and interests are found, it is possible that the groups perceive themselves as more alike in terms of personal characteristics and values. Sandman, Norberg, and Adolfsson 38 observe similar changes in behavior and verbal communication of patients with dementia during meal times according to whether nurses wore uniforms or street clothes.
The positive QoL-AD results concerning self as a whole, when staff do not wear uniforms in the SCUs may well reflect a sense of self of PwD that is more consistent with the perception of the social environment in which they live. The fact that caregivers report that not wearing uniforms facilitates communication and participation in everyday activities could be a positive consequence of the decrease in mirror-image perception, further supported by the significant difference between the mean scores of the experimental group and the comparison group for the item ability to do chores around the house of the QoL-AD. This result is concordant with the findings of Logsdon et al 32 on a negative correlation observed between impairments in instrumental activities of daily living and QoL. It can therefore be explained by the fact that residents do not perceive the caregivers as people who owe them a service when in street clothes but more as people who might assist them when needed and enabling them more control over their own environment.
Caregivers’ report that residents are sensitive to the way caregivers dress and compliment them on their attire confirms that a social process of this kind takes place. Compliments were usually returned to the residents by the caregivers, and therefore dressing and appearance took more importance in everyday life.
Our results also suggest that PwD describe their current relationships with friends as better when caregivers do not wear uniforms than when caregivers wear uniforms. These results lead to several interpretations, of which the first 2 support the postulate of a mirror-image perception judgment bias: (1) PwD recognize caregivers as people with whom they could potentially become friends and not simply as staff; (2) the fact that the social environment is less institutional and more home like could facilitate engagement in conversation with other residents; (3) having a less institutional social environment might also be perceived as more inviting for actual friends of institutionalized PwD to come and visit them.
All these results are concordant with Rodin’s 39 observations concerning institutionalization and sense of control. According to Rodin, institutionalization can be iatrogenic in that being in an institution increases dependency, depression, and social withdrawal. On the contrary, environments that give a greater sense of control give rise to better behavioral adjustment. 40 Therefore, we could hypothesize that wearing street clothes contributes to fade away institutional characteristics.
In summary, as Woods 41 suggests, these outcomes emphasize the need for congruency of social care attitudes with care activities in SCUs for PwD. As mentioned earlier in the methodology description, caregivers only wore their uniforms during morning hands-on body care and put their street clothes back on after it was finished. They adjusted their attire according to the context of care they were engaged in and the relationships that caring required. It is possible that residents might have felt less uncomfortable to have intimate care done by depersonalized caregivers wearing uniforms. Inversely, our outcomes also seem to indicate that they felt more comfortable doing daily activities with caregivers wearing street clothing.
The Caregiver’s Point of View
Caregiving in community services may well be considered what Hugues 42 calls dirty work, low-skilled tasks indicating a low status in the professional and social hierarchy. Caregivers undoubtedly draw dignity and rewards from direct caring situations. 43 Despite this, social comparison with higher status coworkers carrying out different tasks and with higher hierarchal positions, likely threatens their confidence, leading to poor self-esteem and jeopardizing their professional identity.
Wearing uniforms only in the mornings and then street clothes in the afternoon might well have given caregivers the opportunity to see themselves in context and reconsider their profession. According to their reports, these caregivers feel more at ease in their relationships with residents as well as with their families. Residents and families also report seeing these caregivers differently when they interact with them. Thus, as Coombes and Heilman 44 suggest, the abandoning of uniforms could remove a barrier to communication enabling beneficial relationships to develop.
The pleasantness that caregivers perceive when not wearing uniforms could also be interpreted as a decrease in burnout. Burnout involves deindividuation and depersonalization processes linked to identity that could well be attenuated by wearing street clothes. 45 Wearing street clothes may, therefore, have restituted an identity mirrored back by residents and their families, which in turn enabled caregivers to communicate more with residents and deal more empathetically with them. Once the caregivers implemented not wearing uniforms, hygiene matters were not seen as a barrier, reinforcing the idea of reduced burnout and increased individuation toward residents. Moreover, jealousy expressed by uniformed coworkers toward those without uniforms and their perception that the managerial team preferred these colleagues emphasize the positive self-perception wearing street clothing triggers in such a context.
Ethical Considerations Toward Wearing Uniforms in SCUs of PwD
According to Carl Rogers, who inspired Tom Kitwood’s theory of personhood, 23 client- or person-centeredness implies valuing attitudes over techniques 46 and emphasizes the centrality of congruency and authenticity. According to Rogers, 46 professionals must be genuine and establish a person-to-person relationship; a direct relationship without trying to hide behind a facade (eg, their profession). They must be open to the feelings and attitudes that flow toward them. 46 Given these attitudes, wearing uniforms in SCUs appear to be contradictory with a person-centered approach. Person-centeredness implies (1) services provided in a normalized and intimate environment; (2) commitment from staff members; and (3) emphasis on a social rather than medical model of care. 47
The ethics of wearing uniforms can also be seen from an empirical point of view and interpreted in 2 different ways. First, one could interpret the reluctance of some staff members to not wear uniforms as a result of a false belief about aging and dementia and regarding how nurses can make an important difference in dementia care. Like AIDS in the 1980s, the reluctance of staff members to not wear uniforms could be analyzed as psychological resistance linked to the stigma surrounding dementia, the false belief that dementia (and maybe also aging altogether) is an infectious-like, dirty disease.
According to the outcomes of this study, however, this reluctance can also be seen as revealing caregivers normative attitudes regarding the relationship they should have with the PwD they care for. Their desire to wear uniforms reflects the kind of relationships caregivers prefer and value as well as the kind of relationships they consider ethical. Wearing uniforms may help staff members fit their self-perception to their professional identity. Some staff members may prefer to act as professionals, not “persons,” in order to have ethical relationships with PwD. Some caregivers may find it contradictory being professional and not wearing a uniform. Uniforms might be seen as a way of reintroducing professionalism, where care relationships are sometimes overlooked as involving too much affect and personal interaction.
It is not necessary to decide who is right and who is wrong in this debate. Person-centeredness and professionalism are not mutually exclusive. Which is more respectful to the personhood of PwD is also not always evident. What is being emphasized here is the difference between psychological resistance based on false beliefs and a normative attitude regarding the kind of relationships that are ethical and that this distinction is important when managing staff in dementia care.
Limits of the Study
Because only one man was represented in the study, we cannot make generalizations regarding gender. Although it did not seem to affect the data analysis, the fact that both the groups were not completely homogeneous at baseline for the QoL-AD could represent a limitation of the study. The higher mean scores of the QoL-AD in the control group at baseline might mean that they were less sensitive to change. Although the QoL-AD proxy responses are considered as acceptable, 32 some research has shown that proxy responses were not always fully concordant with PwD responses and views of QoL. 48,49 Therefore, although qualitative and quantitative analyses seem to be concordant in our study, cautions should be taken when interpreting these results.
Conclusion
In this study, we investigated the impact of wearing uniforms or wearing street clothes in care environments for PwD. Quantitative results of the study show overall improved QoL scores for the group of institutionalized PwD that experienced daily living with caregivers who did not wear uniforms after morning body care. Qualitative study outcomes suggest that not wearing uniforms also impacts communication skills and relationships between PwD and caregivers. Caregivers wearing street clothes after hands-on body care also seem more satisfied with their professional status.
Results also indicate the importance for care managers in nursing homes to carefully analyze the meaning of staff members’ reluctance not to wear uniforms. Although wearing uniforms can be a matter of pride regarding one’s professional status, when the reluctance to dress in street clothes during care is the result of false stigmatized beliefs, this might be the need to modify the representations staff members have of dementia and PwD. When the reluctance is the result of a normative attitude, it might be important to discuss with staff members their representations of what a person-centered approach of care is or should be. In summary, not wearing uniforms during care is not just a matter of “judging a book by its cover” but should be seen as a general attitude toward institutionalized PwD. Attire and behavioral adjustments of caregivers according to the caring context in which they engage also emphasize the semantic difference between “caring for” as a humanistic attitude and “taking care of” as a technical skill.
Footnotes
Acknowledgments
The authors wish to thank the Social Welfare Department of the Agirc-Arrco Aging Pension for supporting this study as well as Caroline Charras, PhD, Michèle Fremontier, PhD, and Teresa Heady, MA, for rereading the article and suggesting changes. The authors also wish to thank the Interdem members that have commented on this study while it was presented during the Interdem Symposia that took place in merge of the 27th International Conference of ADI.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.