
Abstract
Reserve and resilience are recognized as essential for effective intervention and prevention of dementia. However, it is not known if these factors also protect against risk for dementia in the Greater Bay Area (GBA) of Mainland China. Studies of risk factors across regions of China provide an evidence base for future research in the GBA. However, population-based studies are rare and do not account for the cultural differences in levels of education, income, literacy and modifiable lifestyle factors. Critically, extant studies do not allow for differences in languages spoken across the region, which will bias results and potentially minimize true prevalence. Based on the conclusions reported in this Special Collection, research in the GBA should focus on resilience and reserve using preserved native language communication skills.
Introduction
The Special Collection of the American Journal of Alzheimer’s Disease and Other Dementias Intervention and Prevention of Neurodegeneration see https://ipndgba.edu.hku.hk/home has a recurring theme of building resilience in different cultures. The conference was designed to examine these issues in the Greater Bay Area (GBA) of China including Hong Kong, Macau, Shenzhen and Guangdong. International researchers have an interest in the GBA because of the fastgrowing population and the accompanying burden of age-related illness as well as the potential benefits of early intervention to prevent dementia. In the same year, the Association for Pacific Rim Universities (APRU) hosted the Population Aging Conference with a focus on East Asia but also including Australasia, Pacific Nations, South-East Asia and Americas https://apru.org/event/apru-population-aging-conference-2021/. The objective of the meetings was to promote healthy aging and thus Quality of Life (QoL), culminating in the emergent theme of this Collection - specifically, the identification of cultural differences in research on Alzheimer’s disease and dementia. The goal here is to highlight these findings for the GBA.
To achieve this goal, the present paper considers the expertise of invited international authors from countries around the Pacific Rim (Australia, China, Canada, Peru) as well as the EU and UK. The common findings is that cultural factors can be used to strengthen resilience. For example, exploiting familiar knowledge such as previously learned oral and written language skills in the native and also the non-native language. These factors contribute to a cognitive reserve that is acquired before disease onset by millions of patients all over the world. Other cultural skills include art, education, exercise, games, music, singing, theater and modifiable behaviors such as food preference, smoking, and substance use. Some of the papers report original research on how such cultural factors contribute to the prevention and intervention of Alzheimer’s disease and dementia, whereas others systematically review extant evidence. All papers converge on the same view: culture specific awareness is vital.1–9
The Special Collection begins with a review of the work of Brayne and Wu 2 who conclude that awareness of cultural contexts in which assessment and treatment occur is often absent or at least not reported, in large population based studies of aging and dementia. They describe the variation they observe within a country (UK) among aging populations by comparing the changes in health conditions across time and place using examples from population-based studies in England and Wales. They recommend public health researchers adopt a lifecourse approach to the assessment and care of patients that is guided by the cultural context in order to integrate variability in life experiences and social circumstances with changes to cognition, functioning, physical health and wellbeing. This allows population-based studies to translate more readily to international initiatives for dementia and to Sustainable Development Goals.
Berkes and Bialystok 3 consider cultural differences in language usage and argue that this is a generalisable proxy measure of cognitive reserve. They also argue that speaking more than one language can impact the trajectory of disease onset in patients who have higher cognitive reserve (bilinguals). They review their own findings showing that bilingual patients present with symptoms of Alzheimer’s disease at a later stage of the illness, but decline more rapidly than monolingual peers. This is, first, evidence of a dissociation between cognitive and neural reserve and, second, highlights the value of cultural awareness to cognitive reserve. They also discuss limitations of the reserve hypothesis for patient treatment, as the disease progresses.
Carthery-Goulart and colleagues 4 continue this theme by reporting a systematic review and exploratory meta-regression of extant research testing the hypothesis that a bilingual benefit is modulated by the linguistic distance between a pair of languages spoken by bilingual seniors. They report that bilingual seniors speaking distant language pairs showed better performance on cognitive tasks overall. However, modulatory influences of language distance on dementia diagnosis were not yet clear due to the small number of studies meeting the inclusion criteria. They recommend more detailed reporting of individual differences in languages spoken than hitherto to assess the impact of language distance and other variables on disease progression.
Custudio and colleagues 5 focus on a specific cultural difference (literacy) within a country - Peru. Not all Peruvians learn reading and writing skills as in any country around the world. This limits the type of testing that can be administered to diagnose dementia reliably as well as introducing negative bias for these patients thus reducing QoL. They presented an adapted version of the Alzheimer’s Disease Cooperative Study-Activities of Daily Living to patients, and found that the ADCS-ADL is a reliable tool for use with patients who have relatively low levels of education. They also discovered that performance on the Peruvian-Spanish version is correlated negatively with AD severity, suggesting this is a valid tool for use across Peru.
Montesinos and colleagues 6 further highlight additional cultural issues in South American countries for the intervention and prevention of neurodegenerative disease. They examine the impact on brief cognitive screening and primary care on individuals who are not literate. They validated a test comparing free recall and total recall performance of 63 patients with early Alzheimer’s disease with 60 amnestic mild cognitive impairment (aMCI) and 64 cognitively healthy individuals. Recall did not depend on literacy. Performance also distinguished MCI patients from controls, thus producing a reliable tool for assessing cognitive decline in South Americans who speak hundreds of different languages, but many of whom are not yet literate.
Nielsen 7 extends work on cultural differences to a review of research comparing cognitive assessments performed in the EU, which like South America as a whole, is characterised by cultural, linguistic, socio-economic and political diversity including refugees who are often not yet literate. Most studies have a focus on cultural differences such as language barriers, differences in level of education and literacy, and acculturation in refugees. Nielsen concludes that the European Cross-Cultural Neuropsychological Test Battery (CNTB) and the Rowland Universal Dementia Assessment Scale (RUDAS) are both reliable and valid tools for testing patients in the EU as they are culturally sensitive and minimize bias in language background.
Dementia is not only caused by Alzheimer’s disease. Ruggero and colleagues 8 return to QoL by reporting their research on patients who have Primary Progressive Aphasia (PPA), a dementia that begins with loss of language and progresses to cognitive impairments. They look at dementia from a Whole of Life perspective taking into account communication skills within the carer network, another cultural difference across the world of research in dementia. They observed differences in QoL between patients and their communication partners who are often confederates in assessment and treatment of neurodegenerative disease. Their results suggest that communication is optimal when partners share a common set of cultural values.
Population based studies in Greater China report the region is at risk of increased morbidity due to Alzheimer’s Disease and other dementias. 9 However, prior to 2020, risks were not reported in the international literature and, furthermore, few studies considered the GBA as a region with a distinct cultural and linguistic profile such as rapid growth in education, GDP, multilingual speakers and developments in technology. The pandemic delayed the incredible pace of sustained growth in the GBA, but of course not aging per se. Given approximately 100 million residents, the GBA is on a trajectory toward increasing demands for intervention and prevention of dementia. Papers in this Special Collection highlight a need for resources that target modifiable risk factors so that cognitive reserve can be used to build resilience.
Burden of Alzheimer’s Disease in Mainland China and the GBA
Covid-19 took a particularly large toll on the elderly in the GBA. One insight to emerge from the pandemic, and also recognised by the National Institute of Aging (NIA), 10 is the value of resilience and reserve for the prevention and recovery from disease which is defined as a “dynamic property enabling cells, organs, organisms or individuals to ….. recover.” This includes cognitive reserve. Neurodegeneration is a natural consequence of aging and yet some patients sustain QoL with little sign of functional decline. Others experience morbidity, mental and physical decline that diminishes QoL. The NIA definition recognises cognitive reserve depends on retention of cultural resources that were acquired premorbidly. In theory, cultural resources can be learned at any age to promote healthy aging. However, the question if cultural resources can be exploited in neurodegenerative disease is open. Little evidence of positive effects of new learning in patients who have dementia living in the GBA is available.
Prevalence, Mortality, and DALY Estimates for Alzheimer’s Disease and Dementias in 2016 Compared to 1990 and Percentage Change of Age-Standardized Rates by Location.

Population based studies of prevalence in Mainland China show significant differences across regions between gender and level of education (literate vs non-literate) but less between urban and rural dwellers.9,19 Inspection of Table 1 shows that Hong Kong has the highest prevalence of Alzheimer’s of all regions in China. This is possibly due to historically better health care; greater number of research studies meeting international standards; as well as the availability of reliable and valid cognitive tests and neuroradiology tools.20,21 However, availability is increasing - specifically with reference to the regions in the GBA.22–24
Demographic and Matching Statistics for Alzheimer patients and Control Groups.

Univariate Analysis of Clinical, Cognitive and Language Group Differences.
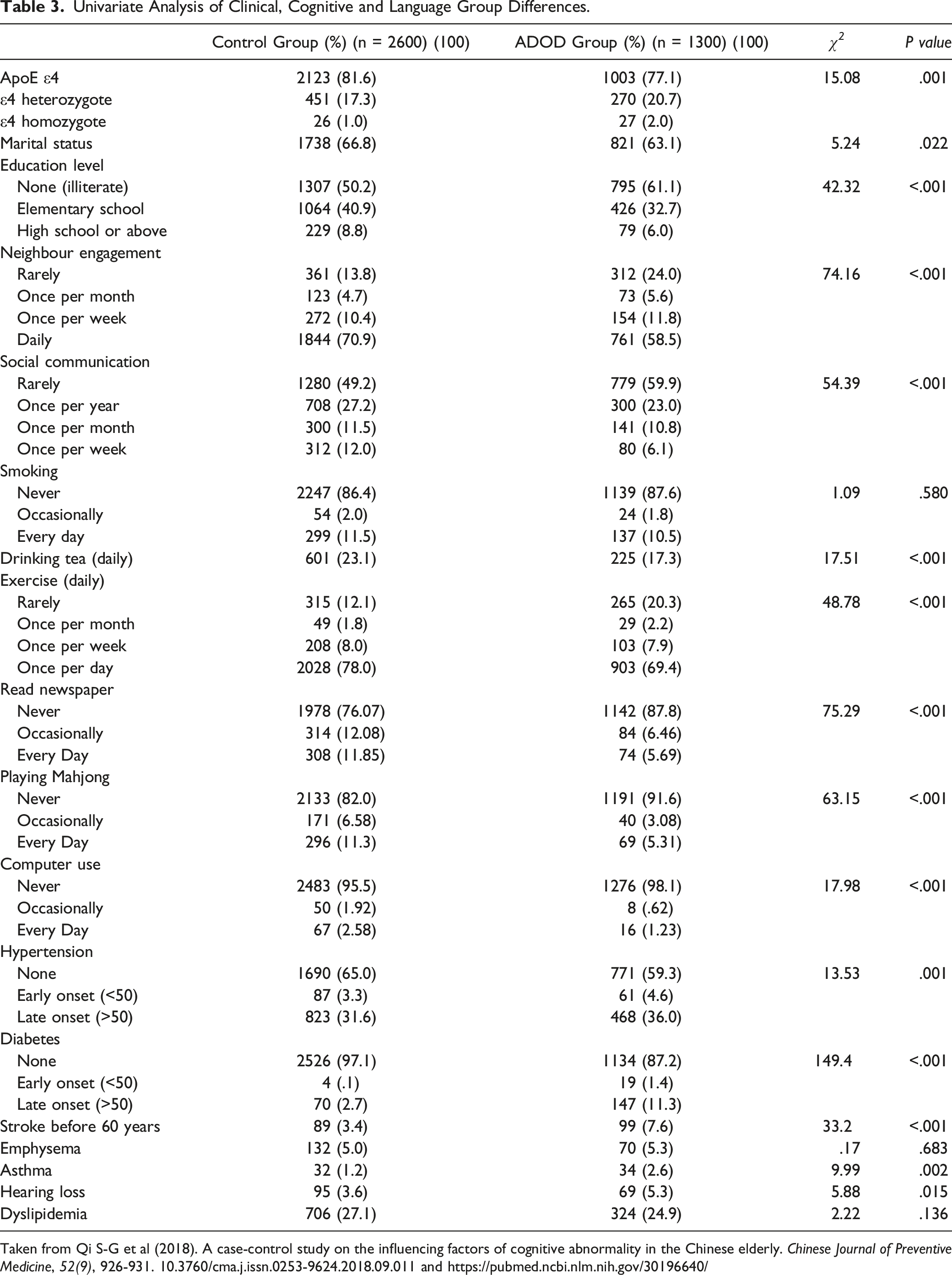
Taken from Qi S-G et al (2018). A case-control study on the influencing factors of cognitive abnormality in the Chinese elderly. Chinese Journal of Preventive Medicine, 52(9), 926-931. 10.3760/cma.j.issn.0253-9624.2018.09.011 and https://pubmed.ncbi.nlm.nih.gov/30196640/
1300 cases were identified in the probable Alzheimer’s group, including 420 males and 880 females aged 72.86 ± 7.48 years old. The control group had 2600 individuals including 840 males and 1760 females aged 72.79 ± 7.43 years old. There were no significant differences in the distribution of age, sex, or residential location between groups. Cases were matched to two participants without cognitive impairment yielding 2600 case controls. All participants were administered physical measurements, laboratory tests and a face-to-face interviews in Putonghua on data about age, gender, education level, marital status, social interaction, diet, exercise, behavioral habits (eg, drinking and smoking), chronic disease and treatment (asthma, diabetes, emphysema, hearing loss, hypertension and strokes), activities of daily living; cognitive habits (computer usage, playing games, reading). Physical measurements including height, weight, waist circumference, BMI, blood pressure and heart rate were also recorded. Laboratory tests included blood glucose, lipid, and ApoE genotype testing. ApoE genotype testing was performed using genomic DNA extraction.
Statistical analyses were performed using χ2 test to compare proportion of responses derived from cases and controls, followed by univariate analyses of the risk factors that discriminated cases from controls. The significant factors from the univariate analyses were used for multivariate conditional logistic regression analysis fitting Cox’s model with OR (95% CI) level P < .05 statistically significant. Single-factor analyses revealed probable AD cases had significantly greater ApoE genotypes; asthma, diabetes, hearing loss, hypertension and stroke before the age of 60; and more likely to live alone (single, divorced, widowed). Cases had lower levels of education and literacy; fewer neighborhood interactions and social activities; less daily tea drinking; less exercise; reading; playing games; and computer use with no other significant differences.
Summary
The risk factors in Mainland China resonate with findings of the Lancet Commission Report. Population based studies in the GBA report variability in demographic characteristics, health outcomes and risk factors. For example, life expectancy is longer in Hong Kong and Macao than in Guangdong. Education and income are also lower in Guangdong. There are cultural similarities however. Cantonese is a native language in the GBA. Tri-lingualism (Cantonese, English and Putonghua) are officially recognized in Hong Kong and Portuguese is officially recognized in Macao but this policy is not recognised in Mainland China. Other languages in the GBA include Hakka, Hindi, Hokkien, Talagog, Nepali, Teochew, Urdu, and Yue dialects making it a truly multilingual linguistic environment. Bi-literacy using the English alphabet and Chinese characters is officially recognised in Hong Kong but not in several other parts of the GBA. Given that modification of risk factors requires communication (literacy, speech), multilingualism should be embedded in health policy in the GBA. Indeed, research in Hong Kong suggests that speaking more than one language may have beneficial effects on brain regions that are vulnerable to Alzheimer’s Disease.27-29 Average levels of educational attainment in Hong Kong and Macao are among the highest in the world on international tests such as PISA and TIMMS. Low levels of educational attainment and literacy are a risk factor according to the Lancet Commission. Therefore education, specifically with regard to literacy within the GBA, should be a target. Given levels of education and literacy are variable across the GBA, another recommendation is that bi-literacy should be encouraged.1,29 Some of the factors in Table 3 could be interpreted as showing benefits from cognitive reserve such as computer use, reading, games and communication (conversation, social engagement). 30 This is consistent with the recommendations from the NIA Reserve and Resilience Collaboratory https://reserveandresilience.com. 10
Implications
Seniors who are diagnosed with Alzheimer’s can preserve cognitive and neural reserve with a focus on communication during exercise, neighborhood conversation, and in social activities. However, more research is needed to test hypotheses about possible benefits of multilingual communication on cognitive reserve, neural maintenance, and modifiable risk factors in the GBA. This requires the combination of large population cohorts and experimental methods. Both methods require culturally sensitive measures that consider native language use. 1
The ecological validity of tests for Alzheimer’s in the GBA is unknown. Although reliable and valid tests for the diagnosis of cognitive and communication difficulties are available for Cantonese speakers eg AD8, Mattis, MOCA, MMSE, these instruments would benefit from estimates of language proficiency and domain of language usage. It is recommended that future studies use the criteria and definitions proposed by The Executive Committee of the NIA Collaboratory to test cognitive reserve and brain maintenance. According to their criteria “Cognitive reserve is a property of the brain that allows sustained cognitive performance in the face of age-related changes and brain insult or disease wherein property of the brain refers to mechanisms including molecular, cellular and other levels.” Using these criteria, brain maintenance and cognitive reserve are both relevant to building resilience across the GBA.
Conclusions
This Special Collection highlights several research findings that can be used to guide policy and research in the GBA. Barriers to health include Communication disorders eg, hearing, literacy and speech impairments in indigenous and minority language speakers. Many seniors in the GBA are also not literate, have low levels of education and income and have limited access to further education. Moreover, if patients are screened for cognitive impairments in non-native languages (English or Putonghua), then the reliability of diagnoses is doubtful.
One immediate goal is the early detection of cognitive, communication, hearing, language, speech (aphasia) impairments to minimize barriers to health care. Furthermore, screening tests that are designed for patients with lower levels of literacy and administered in a native dialect are needed to restore ecological validity. Healthy aging frameworks should emphasize maintaining QoL and wellbeing. 2 This approach would include cultural awareness to build resilience in the GBA as the papers in this Special Collection have confirmed.3-8
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by HSS Prestigious Fellowship in the Humanities and Social Sciences awarded by the Research Grants Council of Hong Kong Grant Number 37000419 to Brendan Stuart Weekes (PI).