
Abstract
Aim:
Efficacy and safety of Cistanche tubulosa glycoside capsules (CTG capsule, Memoregain®) for treating Alzheimer’s disease (AD) were studied.
Methods:
A total of 18 patients with AD administered with Memoregain® for 48 weeks were assessed for drug efficacy by Alzheimer’s Disease Assessment Scale–cognitive subscale (ADAS-cog), Mini-Mental State Examination (MMSE), Activities of Daily Living (ADLs), Blessed Behavioral Scale, and Clinical Global Impression (CGI) scales.
Results:
The MMSE score was 14.78 ± 2.51 at baseline and 14.06 ± 4.26 at study completion. While changes in ADAS-cog score before and after 48 weeks of treatment were statistically insignificant, the score improved, deteriorated, and remained unchanged in 10, 7, and 1 patients, respectively. The ADL and CGI scores showed no significant difference from baseline. All adverse reactions were mild.
Conclusion:
After Memoregain® treatment, patients with AD showed no obvious aggravation of cognitive function, independent living ability, and overall conditions but were stable throughout the study. Comparison with other long-term medications with acetylcholinesterase inhibitors suggests that Memoregain® has a potential to be a possible treatment option for mild to moderate AD. Large trials with bigger population are required to confirm.
Introduction
Alzheimer’s disease (AD), also known as senile dementia or dementia of the Alzheimer’s type, is the most common type of degenerative disease of the nervous system. 1 Owing to apoptosis of a large number of nerve cells, AD often clinically manifests as a global and progressive deterioration of higher nerve functions, including personality changes, affective disturbances, and decline in memory, mathematical abilities, power of judgment, and learning abilities. This results in the global deterioration of daily living abilities and social intelligence competencies. The incidence of AD increases exponentially in an age-dependent manner. 1 In China, the morbidity rate linked to dementia is 4.3% to 7.3% for residents above 65 years of age, among which AD accounts for 47% to 77% of the cases. With an increase in the aging population, AD is increasingly becoming an important disease of social concern. 2
CTG capsule, referred to as Cistanche tubulosa glycosides hereafter, is a botanical prescription drug for dementia in mainland China, containing active ingredient extracted from the desert plant Cistanche tubulosa (Schenk) R. Wight and a group of phenylethanoid glycosides containing mainly echinacoside and acteoside. Each CTG capsule contains 300 mg of Cistanche tubulosa glycosides. Cistanche tubulosa is a traditional Chinese medicine, it has been considered as a superior tonic and earned the honor of “ginseng of the deserts.” The scientific values of Cistanche tubulosa lie in the treatment of kidney deficiency, impotence, female infertility, morbid leucorrhea, profuse metrorrhagia, and senile constipation. 3 Modern pharmacological studies have shown that Cistanche tubulosa glycosides have activities such as antioxidation, neuroprotection, antiinflammatory, improving body immunity, advancing the ability to learn and memorize, treating AD, antiaging, and antifatigue. 4 –8 . Cistanche tubulosa glycosides can increase the learning and memory activity in AD mice induced by quinolinic acid, 9 β-amyloid (Aβ) peptide, 10 and aluminum trichloride. 11 Cistanche tubulosa glycosides can enhance learning and memory by inducing nerve growth factor. 12 Echinacoside has antiapoptotic effects on SH-SY5Y neuronal cells following tumor necrosis factor-α-induced apoptosis and rescues behavioral function in a mouse model of Parkinson’s disease. 13 –15 A study has shown that verbascoside/acteoside, one of the other major active ingredients of Cistanche tubulosa glycosides, can antagonize the apoptosis of nerve cells caused by the excessive synthesis of nitrogen oxide via inhibition of the inducible nitric oxide synthase gene expression. 16 Studies have also shown that verbascoside exerts neuroprotective effects against 1-methyl-4-phenylpyridium and glutamate-induced neurotoxicity in PC12 cells 17 and significantly improves scopolamine-induced memory deficits in vivo. 18 In preclinical studies, Cistanche tubulosa glycosides inhibit Aβ peptide accumulation and aggregation in cellular assay and improve cognitive performance in Aβ-induced cognitive dysfunction in rats. Recent research has shown prospects of the broad application of phenylethanoid glycosides in the treatment of neurodegenerative diseases. 13 The AD remains incurable even today.
Acetylcholinesterase inhibitors (AChEIs) such as donepezil and rivastigmine can alleviate symptoms by increasing intracerebral acetylcholine concentrations. Memantine, an N-methyl-
This open-label, nonplacebo-controlled clinical trial aims to study the clinical effectiveness and safety of Cistanche tubulosa glycosides in the treatment of AD using a small sample size, prior to conducting a large randomized, double-blind, placebo-controlled, and multicenter clinical trial.
Materials and Methods
Study Population
Individuals meeting the National Institute of Neurological and Communicative Disorders-Alzheimer’s Disease and Related Disorders Association criteria for the clinical diagnosis of AD 19 were considered for this study. Individuals aged 50 to 80 years of either gender, with a Mini-Mental State Examination (MMSE) 20 score of 10 to 18 points, a Hachinski ischemic score (HIS) of <7 points, without a history of stroke and a cranial magnetic resonance imaging with no manifestations like subcortical diffuse leukoencephalopathy or multiple lacunar infarcts were included in the study. The study particulars were explained to the patients and their guardians, and written informed consent was obtained prior to their participation in this clinical trial.
The following patients were excluded from the study: (1) individuals with obvious cardiac, hepatic, or renal insufficiency; hematological diseases; severe infection; mental illness; cancer; alcohol abuse or drug abuse; and so on; (2) patients classified as New York Heart Association grade III or IV; those with serum creatinine (SCr), blood urea nitrogen (BUN), total bilirubin (T-Bil), aspartate aminotransferase (AST), and alanine aminotransferase (ALT) levels 1.5 times higher than normal; (3) patients with other brain diseases or systemic diseases accompanied by dementia, such as brain trauma, tumors, infections, hypothyroidism, or vitamin B12 deficiency; (4) individuals with completed tests on vitamin B12 level, thyroid function (free triiodothyronine, free thyroxine, and thyroid-stimulating hormone), and syphilis (Treponema pallidum particle agglutination, rapid plasma reagin) at the beginning of the study; (5) patients with depressive disorders and a score of >17 points on the Hamilton Depression Inventory 17-item scale; (6) individuals with primary or lower level of education and unable to understand or cooperate in study conduct; (7) patients participating in other clinical trials within the previous 4 weeks. But patients in trials treated with donepezil, rivastigmine, memantine, selagine, or cetams could be included if they would take 1 month of wash-off; (8) patients with known allergies to Cistanche tubulosa glycoside compositions; and (9) pregnant or lactating women.
Study Design and Dosing Method
This trial was an open-label, nonplacebo-controlled clinical study on Cistanche tubulosa glycosides for the treatment of moderate AD. Each patient was designed to be administered two 300 mg Cistanche tubulosa glycosides capsules 3 times per day for 48 weeks. Such dosage regimen was selected because it had been approved by State Food and Drug Administration in China for treating vascular dementia. Patients underwent the Alzheimer’s Disease Assessment Scale–cognitive subscale (ADAS-cog; referred to as ADAS hereafter) and MMSE assessment at baseline, weeks 12, 24, 36, and 48. Activities of Daily Living (ADLs), Blessed Behavioral Scale (BBS; family members were inquired), clinical efficacy, and drug safety were evaluated once in every 4 weeks. Enrolled patients received Cistanche tubulosa glycoside capsules (Memoregain®, 2 capsules, thrice a day; Sinphar Tian-Li Pharmaceutical Co, Ltd, Hangzhou Sinphar Group, China) for a total of 48 weeks. The capsules were taken infused in warm boiled water after meals. In the study, the first patient was enrolled in June 2008, and the last patient completed treatment in June 2010.
Efficacy Evaluation
The primary efficacy outcome was the ADAS scores. 21,22 The secondary efficacy variables included the intelligence change, MMSE; the independent living ability, ADLs scale 23 (based on a total score of 74 items, including eating, walking, toileting, bathing, maintaining personal hygiene, telephoning, appearance, maintaining dressing, TV watching, chatting, cleaning plates, looking for articles, homemaking, drinks, cooking, emptying trash, getting around, shopping, dating, staying alone, talking, reading, writing, entertaining, etc); the BBS 24 ; and the Clinical Global Impression scale.
Safety Evaluation
Safety was evaluated based on vital signs (including blood pressure, heart rate, and body weight); laboratory tests including routine blood tests (white blood cell total count and differential count, hemoglobin, red blood cell count, and platelet count) and biochemical tests (blood glucose, BUN, SCr, potassium, sodium, chloride, calcium, T-Bil, total protein, serum albumin, ALT, and AST); electrocardiography (ECG); and any adverse events occurring during the course of the study, which were recorded in the case report form.
Statistical Analysis
Statistical analysis was carried out using the statistical package for the Social Sciences software (SPSS 11.5) for Windows. Demographic and baseline characteristics of patients were analyzed using descriptive statistics. Paired t test was used to compare the differences in scores/levels between pretreatment and different periods of treatment as this study was designed as a single-arm treatment, in which the significance level was set as .05. Descriptive statistics were also employed for safety data analysis.
Results
Patient Demographics
A total of 18 patients aged 55 to 80 years (mean ± standard deviation age, 73.06 ± 6.21 years; 6 males and 12 females) completed the 48-week observation period. The majority of patients had received over 5 years of education; the mean period of education was 10.75 ± 2.69 years. The mean MMSE score was 14.78 ± 2.51 points (range, 10-18 points), the mean HIS was 2.61 ± 1.03 points (range, 1-4 points), and the mean Hamilton depression rating scale score was 3.50 ± 2.48 points (range, 0-10 points).
Changes in the Cognitive Function
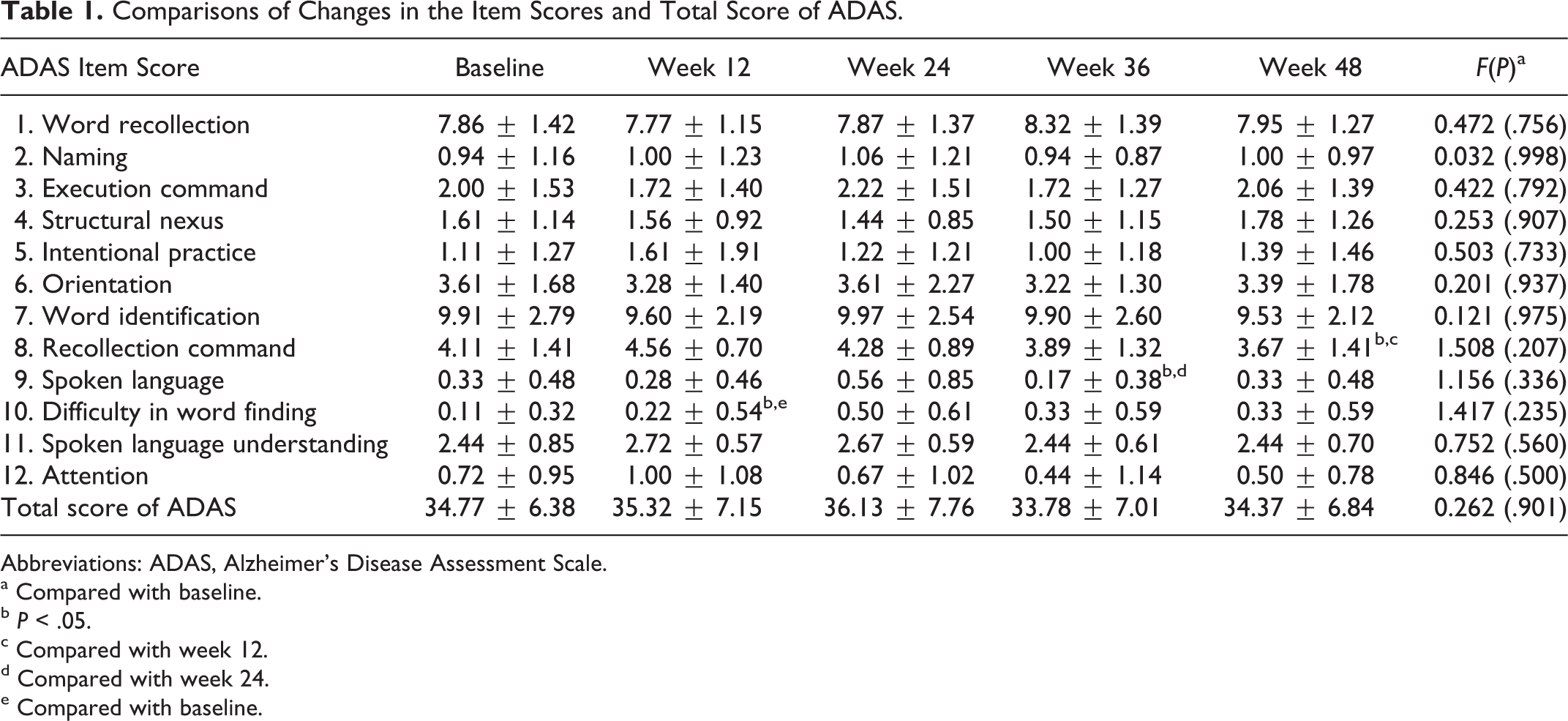
Changes in the total ADAS score, which was the primary measure of outcome, showed no significant differences after week 48 when compared to the total score before week 48 (Table 1). Pairwise comparisons of the 12-item scores of ADAS revealed significant differences only in recollection command (compared between weeks 12 and 48), spoken language (compared between weeks 24 and 36), and difficulty in word finding (compared between baseline and week 24; P < .05; Table 1). Compared to the baseline levels, the total ADAS score improved by 0.4 points without any statistical significance, at the end of week 48; the score improved in 10 patients, deteriorated in 7 patients, and remained unchanged in 1 patient; thus, 11 patients showed no deterioration, and the nondeterioration rate was 61.1% (95% confidence interval [CI], 35.8%-82.7%). The total MMSE score showed no significant difference after week 48 as compared to the total score before week 48 (Table 2). Further analysis by pairwise comparisons of the MMSE item scores also showed no significant differences (Table 2). The MMSE score decreased by 0.72 points on an average after week 48 as compared to the score before week 48, but they are not statistically different. Among the 18 patients, the score improved in 8 patients and deteriorated in 10 patients; thus, 8 patients showed no deterioration, and the nondeterioration rate was 44.4% (95% CI, 21.5%-69.2%).
Comparisons of Changes in the Item Scores and Total Score of ADAS.
Abbreviations: ADAS, Alzheimer’s Disease Assessment Scale.
a Compared with baseline.
b P < .05.
c Compared with week 12.
d Compared with week 24.
e Compared with baseline.
Comparisons of Changes in the Item Scores and Total Score of MMSE.
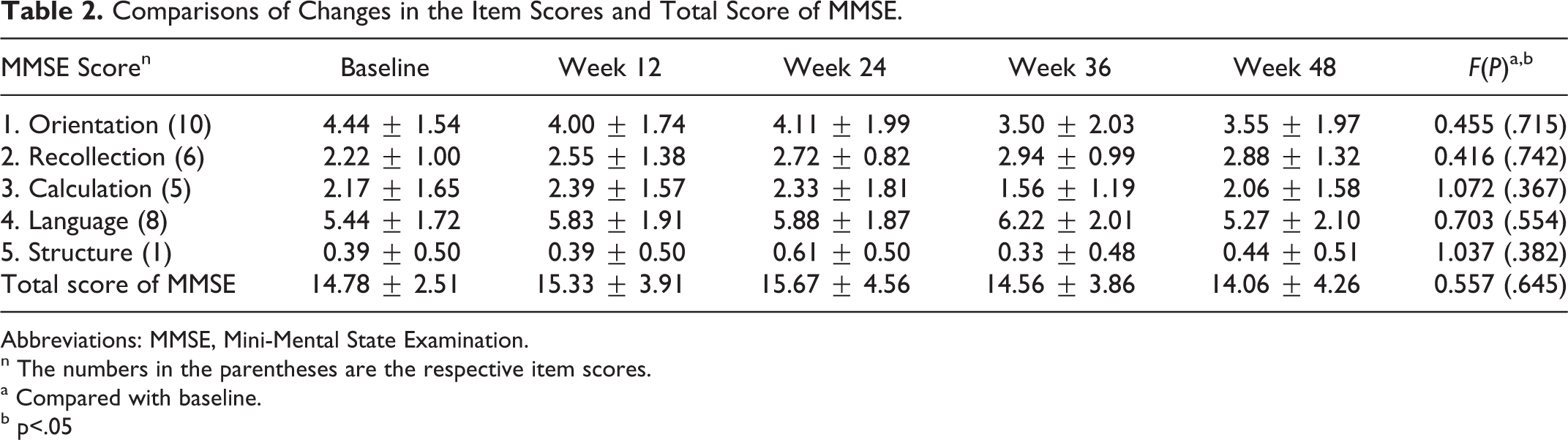
Abbreviations: MMSE, Mini-Mental State Examination.
n The numbers in the parentheses are the respective item scores.
a Compared with baseline.
b p<.05
Independent Living Ability and Capability of Action and Activities
Comparisons of the independent living ability and the capability of action and activities, before and after 48 weeks of treatment are shown in Table 3. Among personality changes, the assessment score was lowest at week 20, for the assessment at the end of weeks 36, 48 patients were significantly better than those at baseline (P < .05). Pairwise comparisons of ADL assessment (13 items) showed no significant differences from baseline.
Changes in BBS and ADCS-ADLs.
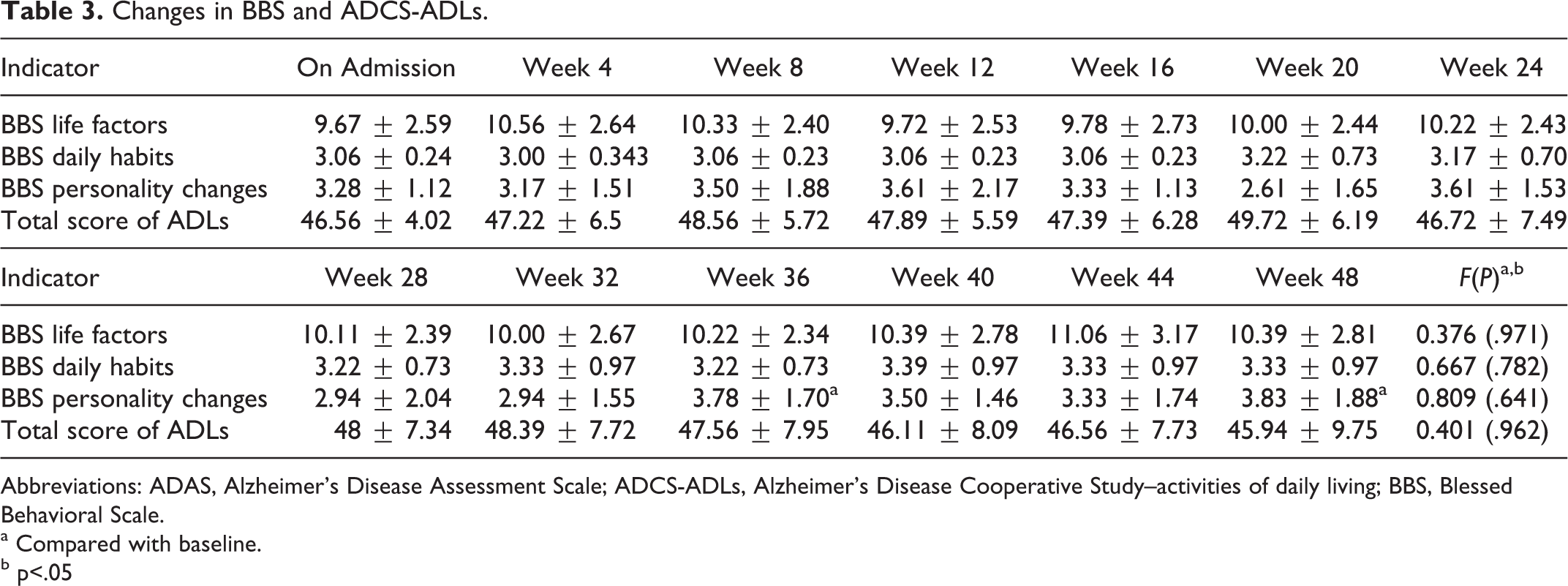
Abbreviations: ADAS, Alzheimer’s Disease Assessment Scale; ADCS-ADLs, Alzheimer's Disease Cooperative Study–activities of daily living; BBS, Blessed Behavioral Scale.
a Compared with baseline.
b p<.05
Changes in the Overall Severity and Efficacy
Comparisons of the changes in the overall severity and efficacy are shown in Table 4. The severity levels, rated as 0 = no symptom, 1 = basically no symptom, 2 = pretty mild, 3 = mild, 4 = moderate, 5 = tended to be severe, 6 = severe, and 7 = very severe, for the assessment at the end of weeks 36, 40, and 44, were significantly different from those at baseline, but this was not the case at the final (week 48) assessment. Changes in the overall efficacy, measured as 0 = not available, 1 = significantly improved, 2 = improved, 3 = improved a bit, 4 = no change, 5 = worsened a bit, 6 = worsened, and 7 = severely worsened, showed no statistical significant difference. These results show that the cognitive function, independent living ability, and overall changes in patients with AD showed mild deterioration or remained stable. Analysis of various tests and item scores of the scale showed that there were no selective changes in scores either during the course of treatment or after 48 weeks of treatment.
Comparisons of Changes in the Overall Severity and Efficacy.
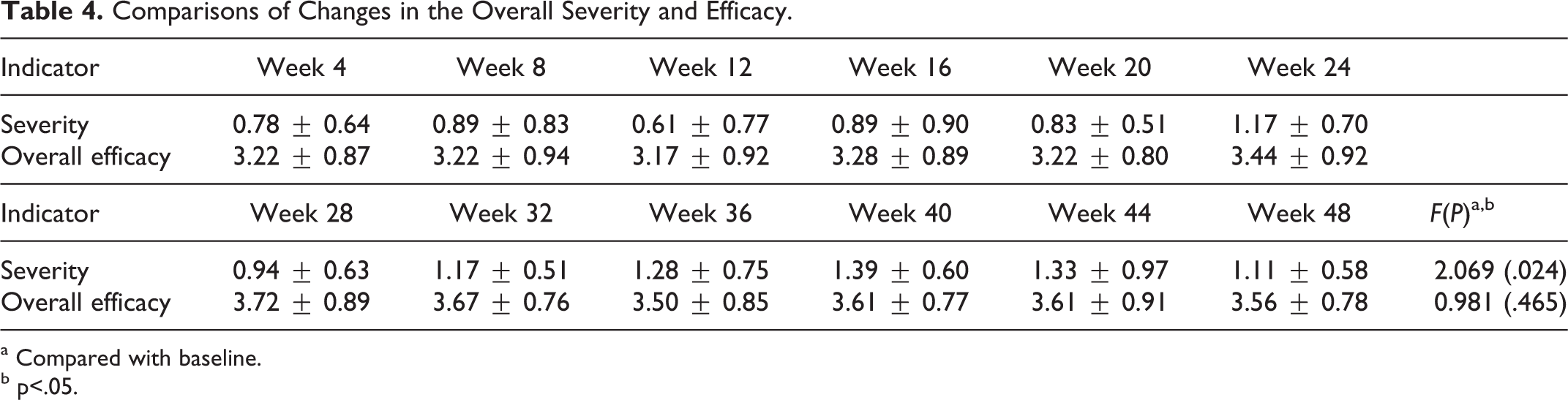
a Compared with baseline.
b p<.05.
Adverse Reactions
There was clinically no significant change in mean systolic blood pressure, which was 133.39 ± 14.18 mm Hg at the beginning of the study and 139.89 ± 23.52 mm Hg at the end of the study (Table 5). However, diastolic blood pressure at weeks 24, 36, and 48 lowered significantly 6 to 7 mm Hg from week 0. There were no significant changes in body weight, heart rate, and ECG pattern between baseline and the end of the study. Statistically significant deterioration was not seen in any safety measurement assessed in this study, In 1 patient, nausea developed after 8 weeks of medication and disappeared after 3 days. Routine urinalysis in 1 patient was positive for red blood cells (+++) after 24 weeks of medication, and the B-ultrasound at another hospital showed bladder stones; a repeat urinalysis showed normal results. One patient had hallucinations at the beginning of the study and was administered 2.5 mg/d olanzapine; the hallucinations recurred 12 weeks after medication initiation but were alleviated after symptomatic treatment with 5 mg/d olanzapine. One patient showed an increase in blood glutamate pyruvate transaminase level at week 24 of evaluation and 3 patients at week 48; these improved after symptomatic treatment. Since all these adverse reactions were relatively mild, patients did not stop taking Cistanche tubulosa glycosides.
Safety Data Analysis.
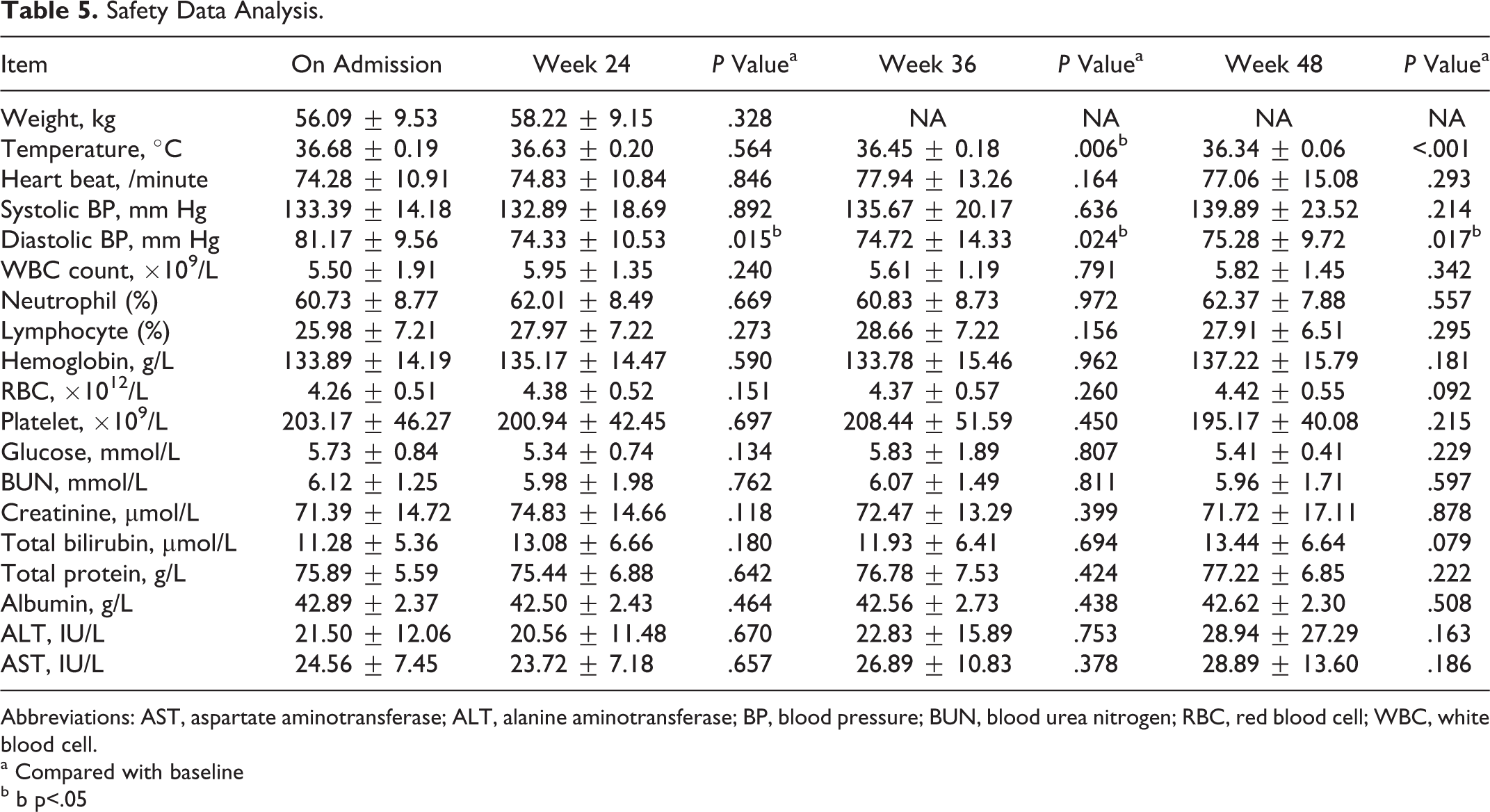
Abbreviations: AST, aspartate aminotransferase; ALT, alanine aminotransferase; BP, blood pressure; BUN, blood urea nitrogen; RBC, red blood cell; WBC, white blood cell.
a Compared with baseline
b b p<.05
Discussion
The ADAS and MMSE are the most commonly used indicators of cognitive function in AD. 25 Clinical trials on the use of AChEIs (donepezil [Aricept], galantamine [Reminyl], and rivastigmine [Exelon]) in the treatment of AD are frequently carried out all over the world. Majority of these trials last for 3 to 6 months and seldom for more than 1 year. Winblad et al, Wilcock et al, and Raskind et al showed that after about 1 year of treatment with AChEIs, the cognitive function of patients decreased slightly when compared to that at baseline. 26 –28 This is similar to the results of cognitive function of patients in this trial that showed no significant changes after 1 year of treatment of AD with Cistanche tubulosa glycoside. The ADAS score improved in 55% (10 of 18) patients. However, Cistanche tubulosa glycosides cannot be assumed to be superior to any AChEI medication for the treatment of AD, particularly since this trial is an open-label observational study with a small sample size.
There were differences between Cistanche tubulosa glycosides therapy and AChEI therapy for the treatment of cognitive function in AD. There were consistent results in cognitive function during the whole process of treatment with Cistanche tubulosa glycosides; however, in a study with AChEIs, an obvious improvement was noted around the third month and a limited change in the later phase. Additionally, Cistanche tubulosa glycosides were not selective in treating the cognitive function domain of AD. However, in a study of AChEI treatment, changes in the ADAS-cog score were limited to significant improvements in word recollection and word identification. 29 On the other hand, the major side effect after AchEI treatment is gastrointestinal reactions that were relatively rare with Cistanche tubulosa glycosides.
There were no significant differences between the assessment results for independent living ability and the capability of action and activities before and after 48 weeks of treatment with Cistanche tubulosa glycosides. There were also no significant differences in the results for pairwise comparisons of ADL assessment. The above results show that the independent living ability of patients with AD remained stable, which was in line with the changes in cognitive function. Green et al reported a 2.06-point decrease in the instrumental ADL score on an average annually for untreated moderate AD, 30 indicating that the stable state of independent living ability after treatment with Cistanche tubulosa glycosides is an indication of the efficacy of treatment.
Our results show that the Cistanche tubulosa glycoside capsules are effective and safe for the treatment of moderate AD, which is in accordance with the ability of Cistanche tubulosa glycosides to inhibit excessive apoptosis of nerve cells.
There have been many fundamental and clinical research studies on the treatment of AD with traditional Chinese medicine. In the preparation of clinical drugs, ginkgo biloba 31 and huperzine A 32 have been used in clinical practice in some Chinese hospitals. There have been several clinical trials on compound preparations of Shenghuangyizhi granule 33 and on kidney-toning and blood-activating therapy 34 in the treatment of AD. All these studies used donepezil as the control and obtained results showing no significant difference between the investigational agent and the onepezil treatment during the observation period (Table 6). In these clinical trials, the sample size was generally small, the observation time was short (2-6 months), and the MMSE and ADAS scores were used to evaluate efficacy, as commonly adopted worldwide. Changes in the ADAS score in the course of treatment with these drugs were similar to the therapeutic effects of donepezil (Shenghuangyizhi granule vs donepezil: 25.04 ± 6.65 vs 25.86 ± 7.08 before treatment and 19.76 ± 5.17 vs 18.87 ± 5.95 after 90 days of treatment) but were different from those observed in this study (35.32 ± 7.15). Thus, the mechanism underlying the treatment of AD with Cistanche tubulosa glycosides is not only different from that of AChEIs but also different from that of other types of traditional Chinese medicines. Antagonism of nerve cell apoptosis is a specific neuroprotective effect of Cistanche tubulosa glycosides. In future, a big population, randomized, double-blind, controlled, and multicenter clinical trial should be designed, with a longer observation time and with AChEI- and placebo-controlled groups for further investigation of the efficacy and mechanism of action of Cistanche tubulosa glycosides in the treatment of AD.
One-Year Follow-Up After Treatment of AD.
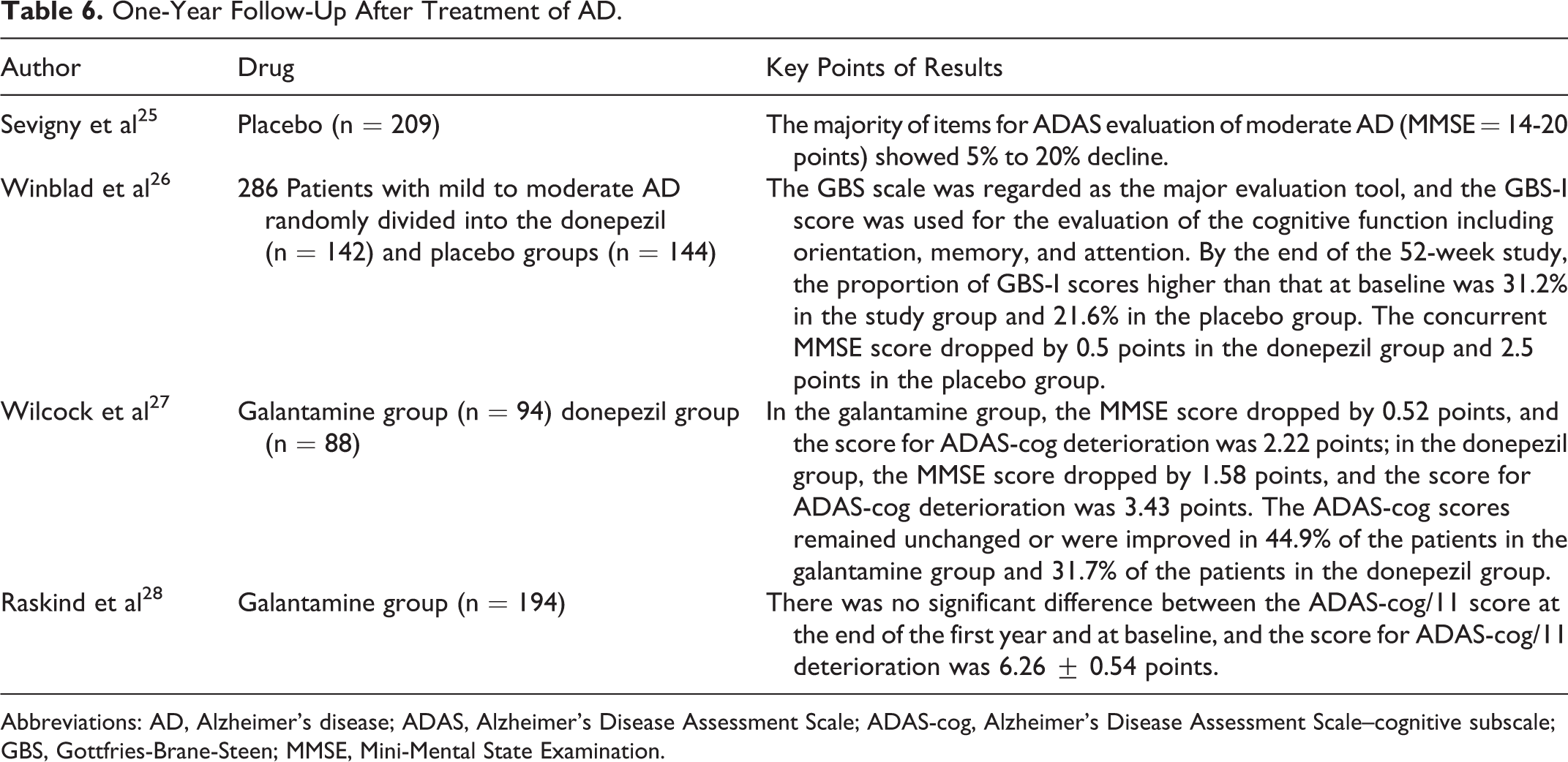
Abbreviations: AD, Alzheimer’s disease; ADAS, Alzheimer’s Disease Assessment Scale; ADAS-cog, Alzheimer’s Disease Assessment Scale–cognitive subscale; GBS, Gottfries-Brane-Steen; MMSE, Mini-Mental State Examination.
Footnotes
Acknowledgments
We would like to thank our distinguished and honored chairman Dr Chuan-Zhen Lu and Prof Zhi-Ying Wu for their direction to clinical trial team of Department and Institute of Neurology Huashan Hospital, Fudan University. Without their assistance, this study would not have been completed.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sinphar Pharmaceutical Co., Ltd. is the sponsor of this study. The authors from Department and Insititute of Neurology at Fudan University Huashan Affilitated Hospital declare no conflicts of interest. The sponsor was responsible for providing the investigational product. The authors took responsibility for arranging the subject schedule, gathering the data from the investigational site to create and interpretation the clinical database.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.