
Abstract
Background: Restless legs syndrome (RLS) is a neurological disorder characterized by the urge to move the legs associated with peculiar unpleasant sensations during periods of rest and inactivity that are relieved by movement. A few studies analyzed RLS in neurodegenerative diseases such as Alzheimer's Disease (AD). The aim of our study was to assess the prevalence and the clinical characteristics of RLS in a cohort of AD patients. Methods: Three hundred and thirty-nine subjects with a diagnosis of AD were recruited. Cognitive, functional, and neuropsychiatric measures were collected at baseline and six-monthly for a 2-years follow-up Results: Fourteen subjects met the RLS criteria. RLS subjects were more frequently male (p:0,006) and younger than AD subject without RLS (p:0,029). MMSE, ADL and IADL were not significantly different. NPI total scores did not differ significantly, however, AD patients with RLS were found to be more apathetic (p:0,001) than AD subjects without RLS. Conclusion: RLS prevalence in our AD cohort was estimated to be about 4%. RLS appeared to be associated with neuropsychiatric symptoms such as apathy. RLS and apathy might share a common pathophysiological basis represented by a dysfunction of the central dopaminergic system
Keywords
Introduction
Restless legs syndrome (RLS) is a neurological sensory-motor disorder characterized by a compelling urge to move the legs. It is usually accompanied by unpleasant sensations involving legs during periods of rest and inactivity (eg, night time) that are typically relieved by movement. Its prevalence, increasing with age, is influenced by sex (being higher in women) and race (being lower in Asian populations) and it is estimated to be about 8% in the elderly population. 1 The diagnosis of RLS is essentially clinical and based primarily on the patient’s history and on a detailed physical and neurological examination. The clinical assessment is usually normal with the exception of secondary forms of RLS sustained by clinically detectable conditions such as renal failure, iron deficiency, neuropathies, and pregnancy. The RLS diagnostic criteria were introduced in 1995 and revised in 2003 by the International Restless Legs Syndrome Study Group. 2 A definitive diagnosis is made when 4 essential criteria are simultaneously present. Three additional supportive criteria may be helpful for the differential diagnosis in uncertain clinical cases (Table 1).
Criteria for Restless Legs Syndrome.a
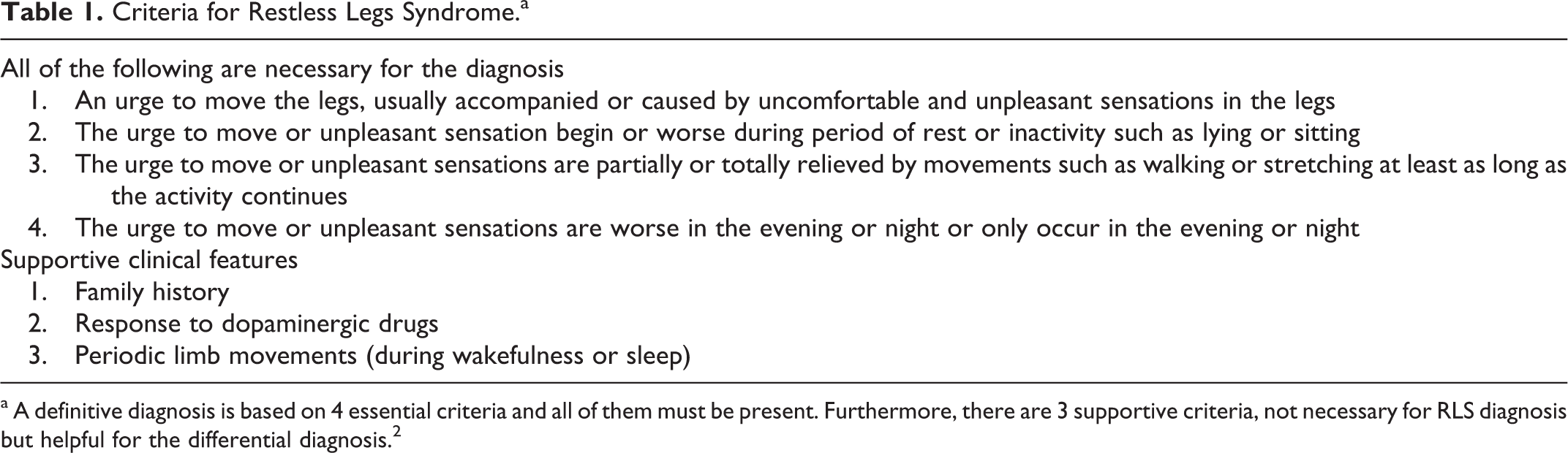
a A definitive diagnosis is based on 4 essential criteria and all of them must be present. Furthermore, there are 3 supportive criteria, not necessary for RLS diagnosis but helpful for the differential diagnosis. 2
Although the etiology of RLS is still unknown, its clinical manifestations are actually attributed to a central dopaminergic dysfunction. In fact, brain imaging studies performed in patients with RLS have shown abnormal dopamine (DA) D2 receptor binding or dopaminergic hypoactivity in striatal and extrastriatal brain regions. 3 Moreover, pharmacological studies have demonstrated an improvement in RLS symptoms with the administration of levodopa or dopaminergic agonists; conversely, they are worsened by tricyclic antidepressants, antihistamines, and others agents negatively affecting the dopaminergic transmission (eg, antinausea medication 4 ). Consistently with this hypothesis, the circadian pattern of RLS symptoms appears to be strongly related to DA plasma levels, being lower during the night time when RLS symptoms are more frequent. Furthermore, iron deficiency seems to sustain secondary forms of RLS by interfering with the synthesis of DA and the regulation of DA receptors in the brain.5,6
Basing on these premises, RLS should be expected to be frequently associated with neurodegenerative disorders such as Parkinson’s disease, Lewy body dementia, and Alzheimer’s disease (AD). In fact, these conditions are characterized by a progressive neuronal loss in the central nervous system and, consequently, by biochemical changes involving several neurotransmitter systems including the dopaminergic transmission. Nevertheless, to date, RLS has been scarcely investigated in the context of these neurodegenerative diseases, especially in AD. Available evidences based on a limited number of observations do not suggest an increased risk of developing neurodegenerative diseases in patients with RLS or, on the contrary, an increased prevalence of RLS in patients with neurodegenerative diseases.7–9
Detecting RLS in elderly patients and, particularly in patients with dementia, might have important clinical implications. In fact, one of the most important disturbances in these populations is the sleep fragmentation that is frequently poorly investigated and generically treated with sedative agents that may also negatively affect the cognitive functioning. On the contrary, the identification of specific causes underlying sleep disorders may allow to adopt appropriate treatments such as low dose of dopaminergic agents in RLS cases.
In April 2010, we performed a cross-sectional study aimed at evaluating the prevalence and the clinical characteristics of RLS in a group of patients with AD recruited from March 2006 to March 2010. Secondarily, over the next 2 years, we investigated the presence of clinical manifestations differently characterizing the course of AD among patients exhibiting or not exhibiting RLS symptoms.
Materials and Methods
The study was conducted at the “Memory Clinic”, Department of Neurology and Psychiatry, of the University “Sapienza” of Rome. Patients affected by AD diagnosed according to the National Institute of Neurological and Communicative Disorders and Stroke–Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) 10 criteria were recruited from March 2006 to March 2010. In April 2010, patients were divided into “patients with AD with RLS” group and “patients with AD without RLS” group, if they, respectively, complained or not RLS symptoms and satisfied or not the diagnostic criteria of RLS (Table 1). The RLS was investigated by adopting a simple questionnaire, developed on the basis of diagnostic criteria, administered to patients and bed partners (Table 2). Only patients who answered “yes” to all questions were considered to be affected by a possible RLS. The same questions were also submitted to carers living with the patients. Diagnosis of RLS was ultimately established if the bed partners could also confirm that the participant complained about a restless, pins-and-needles, or creepy-crawly sensation in the legs. The flowchart of the study is shown in Figure 1.
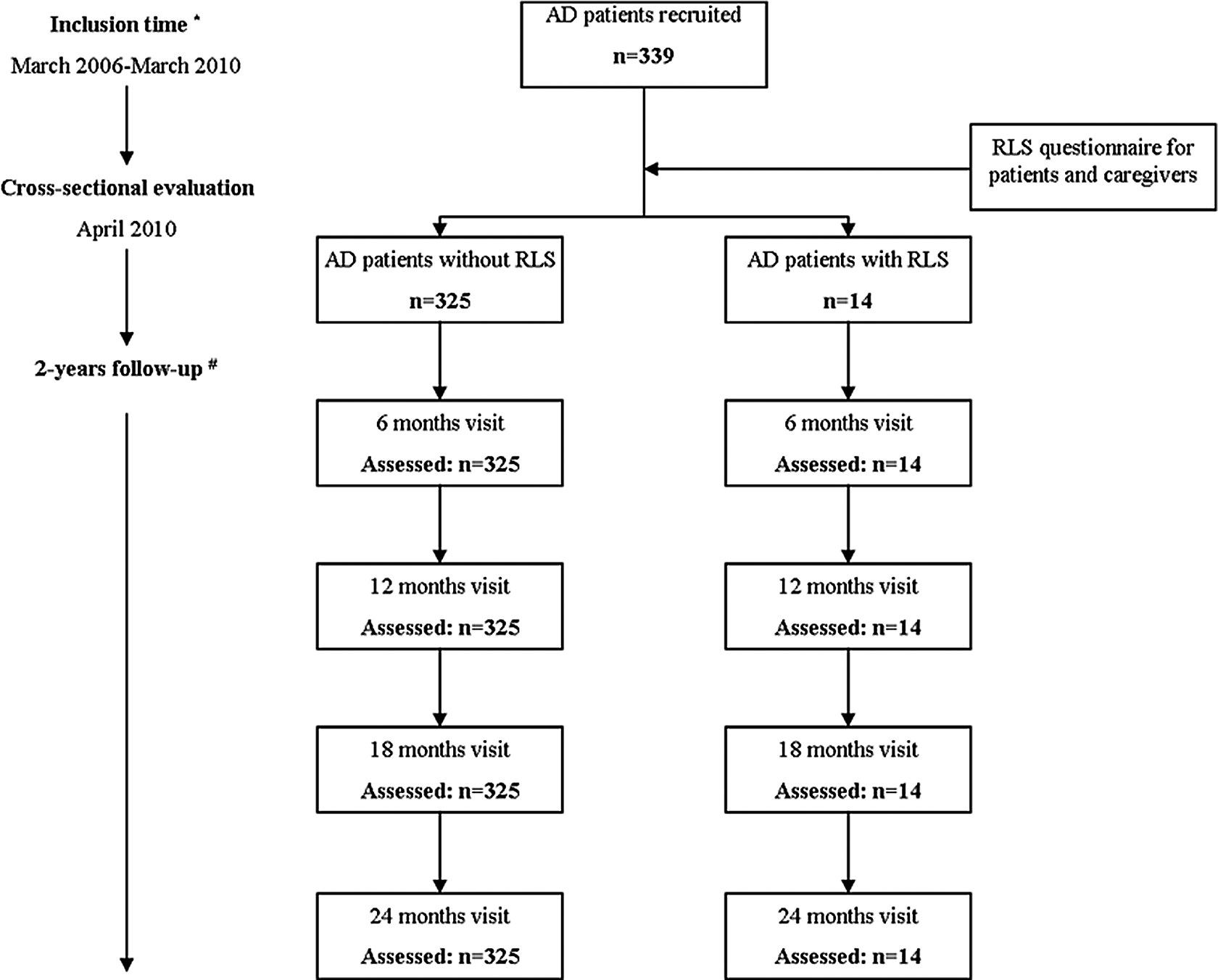
Flowchart of the study. *Physical and neurological examinations, neuropsychological assessment, morphological and functional neuroimaging, Mini-Mental State Examination (MMSE), activities of daily living (ADL), instrumental activities of daily living (IADL), and Neuropsychiatric Inventory (NPI). #MMSE, ADL, IADL, and NPI.
Questions Based on Essential Criteria.a

a This questionnaire was administered to patient and bed partners to detect RLS symptoms. Only patients answering “yes” to all questions were considered as having RLS.
The detailed clinical history (with special focus to comorbidities and concomitant pharmacological treatments) was recorded from the patients and/or first-degree relatives. Patients were subjected to a standardized neuropsychological evaluation, and a morphological (magnetic resonance imaging or computerized tomography) and/or functional (99mTc-HMPAO single photon emission computerized tomography [SPECT] or 18FFDG positron emission tomography [PET]) brain imaging. Moreover, laboratory tests aiming at excluding secondary forms of RLS were performed in the patients with AD with RLS group.
Neuropsychological assessment was performed at first visit in 12 patients with RLS and 285 patients without RLS by means of Rey 15 word list (verbal memory and learning), Rey Complex Figure (constructional ability and visual memory), Trail Making Test A and B (conceptual tracking and shifting abilities), Stroop Colorword test (selective attention), Coloured Progressive Matrices (abstract thinking), Frontal Assessment Battery (frontal functions), FAS and Animal Naming (phonemic and semantic fluency), and Aachener Naming subtest (naming). All raw scores were adjusted for demographic variables and compared to the cutoff scores according to normative data for the Italian population.11,12
In April 2010 and 6-monthly for a 2-year follow-up, all the participants were subjected to a general physical and neurological examination and to the assessment of the following clinical variables: (1) global cognitive functioning, assessed by the Mini-Mental State Examination (MMSE); (2) functional independence, measured by the activities of daily living (ADL) and instrumental activities of daily living (IADL) scales; and (3) neuropsychiatric symptoms, evaluated through the Neuropsychiatric Inventory (NPI).
Statistical analysis was performed using the Statistical Package for Social Science (SPSS) version 16 (SPSS Inc., Chicago, IL, USA). Parametric statistics (t of student for independent samples) were run for discrete and continuous variables such as age at AD diagnosis, years of school, and so on. Nonparametric tests (crosstabs, chi-square, and Mann-Whitney U tests) were used for categorical variables and frequencies such as sex, frontal onset, MMSE, IADL, ADL, NPI, neuropsychological tests, and number of patients taking acetyl-cholinesterase inhibitors (AChE-Is) or antidepressants. Statistic level of significance was set at .05. A logistic-regression model was run to evaluate the relation between the RLS and the variables identified as significant or at borderline level in the univariate analysis at inclusion time in the study. We assumed that the clinical features valued at time of inclusion (April 2010) have not changed from the time of onset of RLS. Odds ratios with relative 95% confidence intervals were estimated.
Results
A total of 339 patients with AD were finally recruited. All enrolled patients were Caucasians; the demographic and clinical characteristics of the study sample are shown in Table 3. The RLS was detected in 14 (4.1%) participants. These participants were more frequently male (71.4%; P = .006) and younger (69.00 ± 6.11 vs 73.83 ± 8.11; P = .029) than the patients with AD without RLS. Median time of RLS appearance was 4 years after the occurrence of the first cognitive symptoms of AD. Of the 14 participants, 9 belonging to the patients with AD with RLS group had an amnestic onset, while 5 patients (35.7%; P = .011) exhibited a “frontal” presentation consisting of social disinhibition, apathy and inertia, inappropriate jocularity, verbal, and motor perseverations. The frontal presentation was clinically assessed during the first visit at our center. No significant differences were found at the time of inclusion (April 2010) concerning neurological and physical examinations, concomitant pharmacological treatments (ie, AChE-I and antidepressants), and neuroradiological findings.
Demographic and Clinical Characteristics of the Sample.a
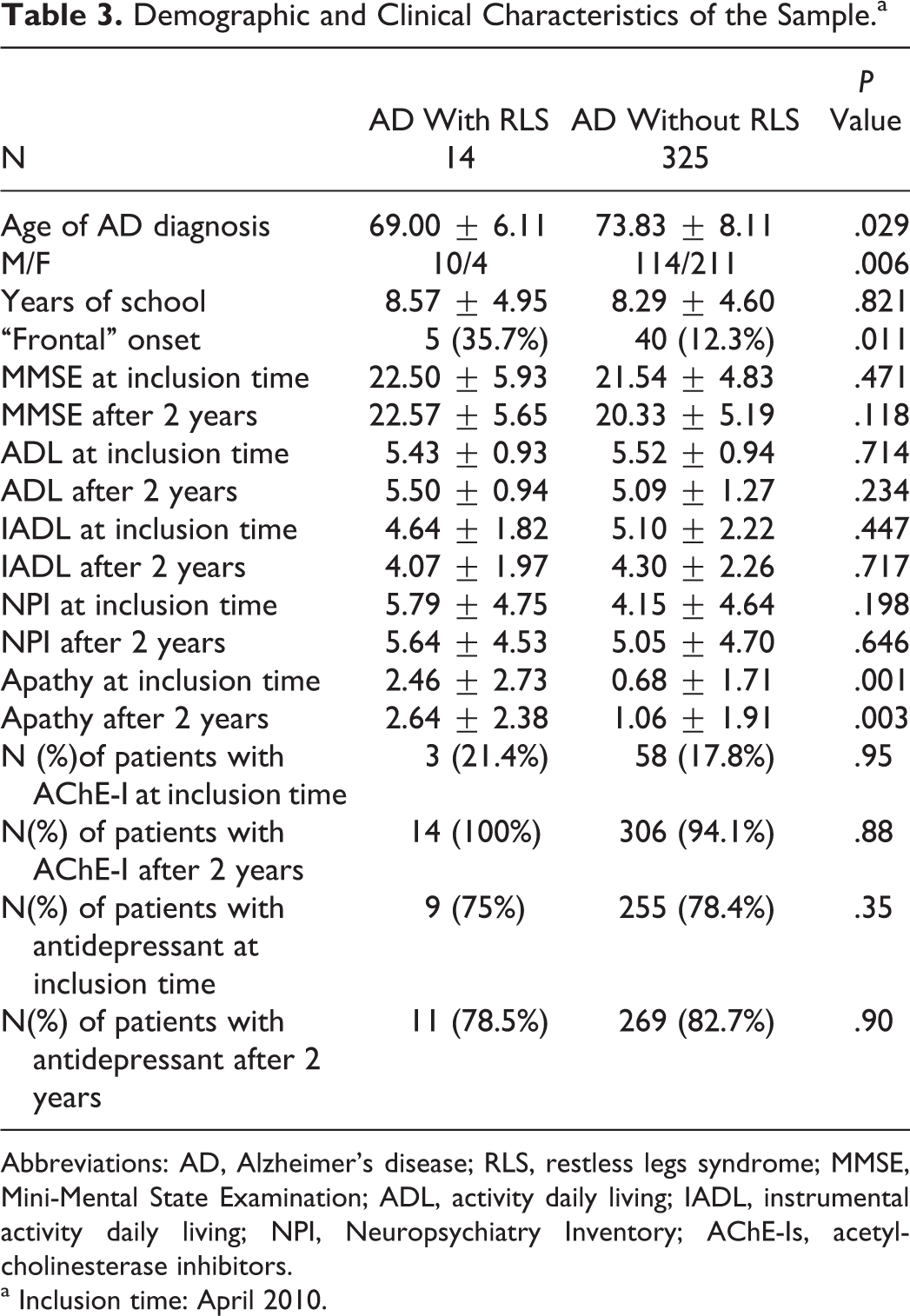
Abbreviations: AD, Alzheimer’s disease; RLS, restless legs syndrome; MMSE, Mini-Mental State Examination; ADL, activity daily living; IADL, instrumental activity daily living; NPI, Neuropsychiatry Inventory; AChE-Is, acetyl-cholinesterase inhibitors.
a Inclusion time: April 2010.
With regard to neuroimaging evaluations, we have performed a SPECT in 57 patients (6 in RLS group and 51 in without RLS group), a PET in 14 patients (1 in RLS group and 13 in without RLS group), and RM and/or TC in all patients.
The 2 groups had a similar cognitive profile in neuropsychological assessment except for visual memory that resulted to be more frequently impaired in patients with AD without RLS (Table 4). However, the small number of participants on AD group with RLS did not lead to definitive conclusions and so we have decided to not include the cognitive data in the logistic regression model. The 2 groups were comparable with regard to MMSE, ADL, IADL, and total NPI scores, both at the time of inclusion and after 2 years of follow-up. Interestingly, patients with AD with RLS exhibited significantly higher scores in the “apathy” NPI item when compared to patients with AD without RLS. This finding was observed at the time of inclusion (P = .001) as well as the end of follow-up (P = .003).
Neuropsychological Assessment at the First Visit.
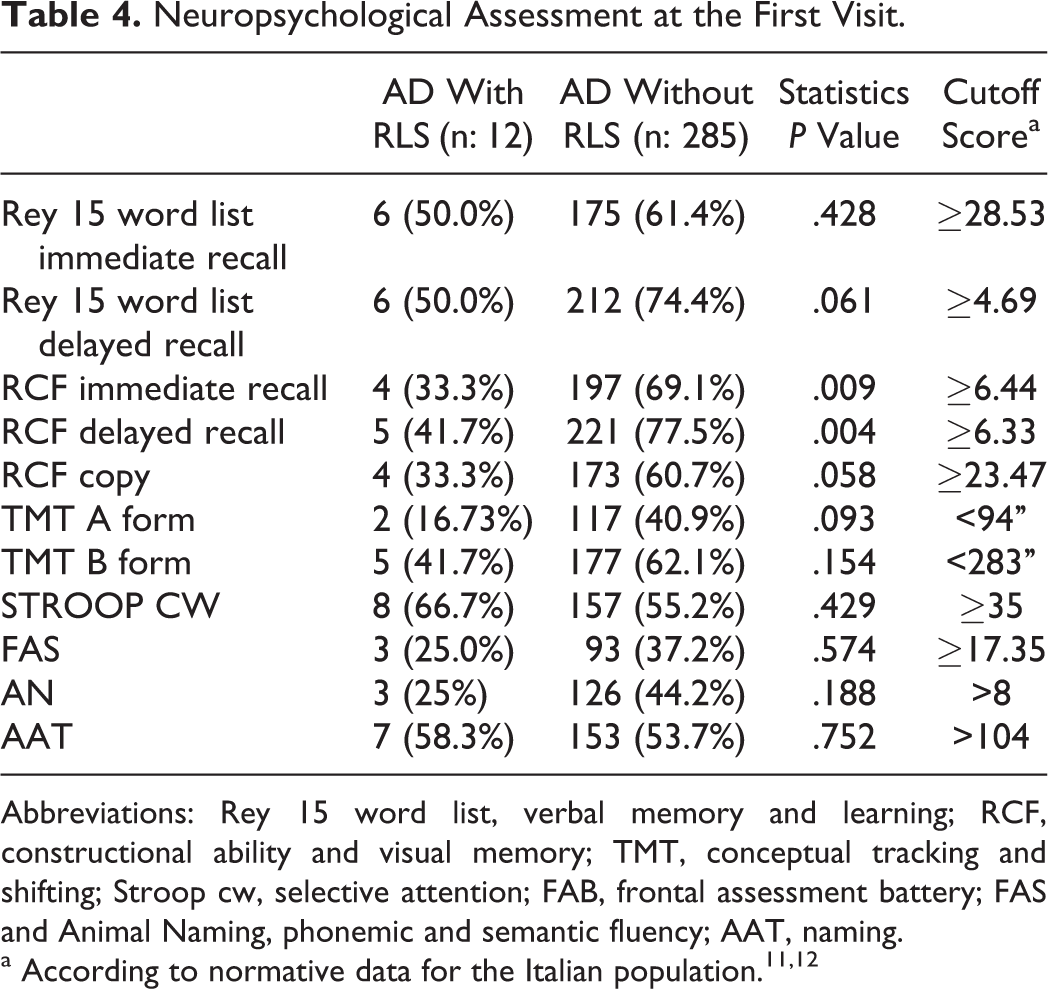
Abbreviations: Rey 15 word list, verbal memory and learning; RCF, constructional ability and visual memory; TMT, conceptual tracking and shifting; Stroop cw, selective attention; FAB, frontal assessment battery; FAS and Animal Naming, phonemic and semantic fluency; AAT, naming.
The logistic regression model (Table 5) showed how the male sex and the presence of apathy at inclusion time (April 2010) were statistically significant predicting factors for the occurrence of RLS, while an early age at AD diagnosis and a frontal onset were at borderline significance.
Logistic Regression Model on Factors Predicting the Probability of Having RLS
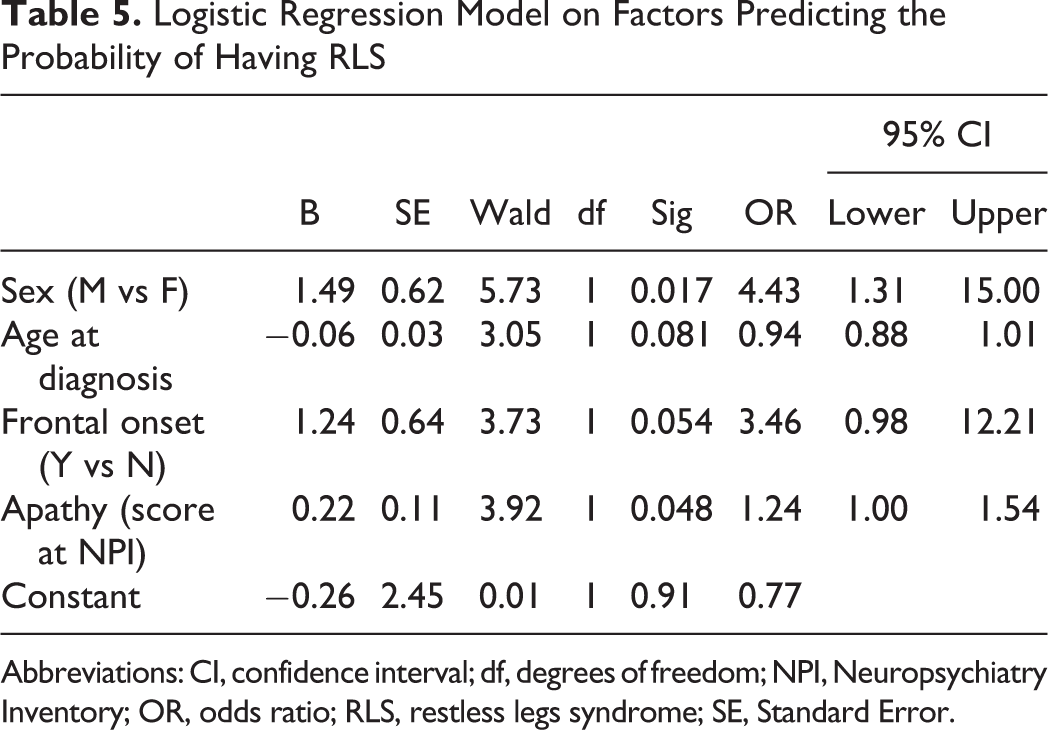
Abbreviations: CI, confidence interval; df, degrees of freedom; NPI, Neuropsychiatry Inventory; OR, odds ratio; RLS, restless legs syndrome; SE, Standard Error.
Discussion
To our knowledge, this study represents the first attempt aiming at specifically investigating prevalence and clinical features of RLS among patients affected by AD. To date, available reports have mainly explored sleep disorders among cognitively impaired participants in a generic manner, without focusing on the specific clinical conditions. Moreover, these studies have mostly involved patients affected by moderate to severe cognitive impairment and thus often institutionalized.13–15 On the contrary, we enrolled only participants affected by mild AD in an outpatient setting.
In our study, RLS prevalence was estimated to be about 4%, and thus lower than expected considering the available data regarding the general elderly population. In fact, disregarding age and gender differences, the prevalence of RLS among Caucasians is reported to be approximately 8% to 12%. It increases with age and it is higher in women. These data might indicate that, in our AD population, RLS could have been underdiagnosed. One possible explanation could be related to the method used for detecting RLS in our group of patients with AD. In fact, considering that patients with AD may have difficulties to describe their sensations, we decided to diagnose a patient as having RLS only if the compelling urge to move legs during rest, especially at night, was simultaneously reported by the patient and confirmed by the carer. Unfortunately, some practical issues (ie, patients were frequently accompanied to visit by familiars not living with them) may have limited the application of this method.
One other possible interpretation of the low RLS prevalence detected may be referred to the observational nature of the study. In fact, some patients might have developed RLS manifestations after the 2 years of follow-up.
About 36% of the patients with AD with RLS referred an onset characterized by social disinhibition, apathy, verbal, and motor perseveration. On the contrary, a “frontal” onset was found only in 12.3% of the patients with AD without RLS. Moreover, patients with AD with RLS were more apathetic than the patients without RLS. This association with apathy appears to be of interest because, so far, the chronic sleep loss (in the RLS secondary to sleep fragmentation) among patients with dementia was found to be associated with depression and aggressiveness. 16 In this context, we hypothesize that RLS and apathy might share a common pathophysiological basis consisting in a dysfunction of the central dopaminergic system. Nowadays, it is thought that RLS results from a central dopaminergic dysfunction in striatal and extrastriatal brain regions. 3 At the same time, according to Levy and Dubois definition 17 of apathy as “a quantitative reduction of self-generated voluntary and purposeful behaviours” and according to the relationship between DA and reward-seeking, or wanting behavior,18,19 a hypothesis for dopaminergic basis of apathy in AD has been proposed.
Some studies have suggested that dysfunction in the dopaminergic system (in particular in brain reward system) may account for apathy in patients with AD.20–22 In this regard, a SPECT study recently performed in patients with AD with apathy have shown a significantly decreased blood perfusion of the anterior cingulate and orbitofrontal cortex regions. 23 These areas appear to be crucial for dopaminergic-mediated reward and pleasure behavior in healthy individuals. 24 Moreover, postmortem studies of patients with AD have demonstrated changes in DA receptor density and distribution. In particular, D2-like receptors density was found to be significantly reduced in the striatum of patients with AD compared to age-matched healthy controls. 25 Finally, PET studies with radiolabeled D2-specific antagonists have confirmed the significant decrease in D2 receptors levels in the striatum of patients with AD.26,27
In our study, the neuroimaging data were not significantly different between 2 groups of patients. Nevertheless, in a number of patients with AD with RLS (n = 6; 42.8%) the SPECT studies demonstrated a decreased blood perfusion in orbitofrontal regions in addition to the typical brain areas involved in AD pathology. However, this observation cannot be generalized because only 57 patients (6 with and 51 without RLS) have performed this examination.
All these data, on the whole, seem to support our hypothesis of a relationship between RLS and apathy in patients with AD.
Some issues could potentially influence the interpretation of our findings. First, the limited number of patients with AD with RLS, and particularly of the subgroup exhibiting a “frontal presentation,” may not lead to definitive conclusions, and consequently larger studies are needed. Second, in assessing RLS, we adopted a questionnaire that has not been previously validated in populations of patients with dementia. This may have affected our results considering the difficulties of participants with cognitive impairment in recording and describing somatic sensations. Moreover, we could not exclude patients with RLS occurring before AD.
Besides these limitations, our study still has several strengths. First, the study design with semiannual clinical assessments provided a detailed monitoring of cognitive and noncognitive symptoms. Moreover, the constant involvement of familiars and caregivers in diagnosing RLS allowed us to limit the biases potentially arising from the reduced reliability of patients with AD in completing the screening questionnaire. Third, we have outlined the possible factors associated with RLS such as the male sex, an early age at AD diagnosis, a frontal onset, and the presence of apathy.
In conclusion, this is the first study specifically evaluating the RLS features and prevalence in an outpatient AD population. The development of appropriate RLS screening tools that take into account the peculiar features of patients with dementia is required. At last, a cohort study on patients with AD enrolled at the time of diagnosis should be performed to estimate the incidence of RLS and to assess the possible relationship between AD and RLS.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.