
Abstract
To investigate the association of the hypotensive syndromes orthostatic hypotension (OH), postprandial hypotension (PPH), and carotid sinus hypersensitivity (CSH) with cognitive impairment (mild cognitive impairment/dementia). Continuous measurements of blood pressure (Finapres) were performed during active standing, meal test, and carotid sinus massage, among 184 elderly patients presenting with falls. Mild cognitive impairment (MCI) and dementia were diagnosed following a multidisciplinary assessment. The study design was a retrospective cohort study. The OH, PPH, and CSH were observed in 104 (58%), 108 (64%), and 78 (51%) patients, respectively. A total of 79 (43%) patients were cognitively impaired (MCI impairment n = 44; dementia n = 35). The prevalence of cognitive impairment varied little across the hypotensive syndromes (32%-43%) and was similar in patients with and without hypotensive syndromes (P = .59). In this geriatric population with a high prevalence of both hypotensive syndromes and cognitive impairment, patients with one or more hypotensive syndromes were not likely to have cognitive impairment.
Keywords
Introduction
The relationship between blood pressure (BP) and dementia in elderly patients remains poorly understood. Epidemiological studies link high BP during mid-life and late life to increased dementia risk. 1,2 However, other studies failed to replicate this association or found contrary results that suggest better cognitive performance with high BP in those over 75 years. 3,4 An important limitation of these studies is that the associations were based on single or very few BP measurements. This is valid only if one assumes that BP is a static variable that can be extrapolated over time. However, with aging, impairments in cardiovascular responses and hemodynamic compensatory mechanisms frequently result in hypotensive syndromes, including orthostatic hypotension (OH, prevalence 5%-50%), 5 –7 postprandial hypotension (PPH, 38%-69%), 8 and carotid sinus hypersensitivity (CSH, 30%-40%). 9,10 Thus, a proportion of the elderly population has recurrent episodes of hypotension that may induce cerebral hypoperfusion and ischemic brain injury, resulting in cognitive decline. 11 –13 These hypotensive syndromes could confound the relationship between BP (based on extrapolation of single static measurements) and dementia. A positive correlation has been found between the fall in systolic BP and structural brain damage (deep white matter changes) in the patients with dementia. 14,15
This study tested the hypothesis that elderly patients with hypotensive syndromes are at increased risk of cognitive impairment (mild cognitive impairment [MCI] or dementia).
Methods
Patients and Assessments
This retrospective study used a clinical database with comprehensive information on 202 consecutive patients aged 65 years and over, referred between 2007 and 2009 to the Falls and Syncope Clinic of the Department of Geriatric Medicine. The majority (75%) of the patients were referred because of falling; other reasons were dizziness and/or syncope. An important aspect of this database is that all patients underwent a comprehensive evaluation of OH, PPH, and CSH (details below) regardless of whether a hypotensive syndrome was suspected.
Baseline characteristics and prescribed medication were recorded 1 week prior to the testing of hypotensive syndromes. Baseline BP was measured using a mercury sphygmomanometer and was referred to as clinic BP. Functional performance was evaluated with the Groningen Activity Restriction scale (GARS; range 0-53, with higher scores indicating more impairment). 16 Cognitive status was evaluated with the Mini-Mental State Examination (MMSE; range 0-30, with higher scores indicating better cognitive status) 17 and the cognitive and self-contained part of the Cambridge Examination for Mental Disorders of the Elderly (CAMCOG; range 0-104, with higher scores indicating better cognitive status). 18 Dementia was diagnosed by following the guidelines for Alzheimer’s disease (National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer’s Disease and Related Disorders Association criteria), 19 Lewy body dementia (criteria of the dementia with Lewy bodies [DLB] consortium), 20 frontotemporal dementia, 21 and vascular dementia (NINDS-AIREN criteria). 22 The MCI was diagnosed according to the criteria described by Petersen. 23 Severity of cognitive impairment was measured with the Clinical Dementia Rating scale (CDR). 24 Diagnoses were determined in a weekly multidisciplinary meeting, including the patient’s result of brain imaging.
To investigate the presence of hypotensive syndromes, 3 diagnostic tests were performed: the active standing test (S) to evaluate OH, the meal test (M) to evaluate PPH, and a carotid sinus massage (C) to assess carotid sinus hypersensitivity. These 3 tests will be referred to collectively as the SMC test.
After an overnight fast, medications were temporarily stopped until completion of the SMC test. Assessments were performed in a quiet and climate-controlled room. Beat-to-beat BP and heart rate were continuously measured from the finger using the photoplethysmographic method (Finapres). The Finapres method is a noninvasive technique that assesses variations in BP and heart rate. 25 Patients were excluded from the SMC test in case medications could not be temporarily interrupted or if they were unable to follow the instructions because of delirium, psychosis, or severe dementia (CDR 3).
Standing-Meal-Carotid Sinus Massage Test Procedure
Orthostatic test
After a 10-minute resting period in the supine position, the patients were asked to stand up and remain standing for 10 minutes. The baseline values of BP and heart rate were defined as the average during the 60 seconds before standing. During standing, the average of 20 beats (10 beats before and 10 beats after each interval of 60 seconds after standing) was used as the average value for each minute. The OH was defined as a decrease of at least 20 mm Hg in systolic BP and was recorded at any of the 10-minute averages after the first 60 seconds after rising. 26 In addition, analyses were repeated using the more stringent criterion of a reduction of 30 mm Hg. Diastolic OH, which can be defined as a decrease of at least 10 mm Hg in diastolic BP, was not included in this study because such small declines are irrelevant with regard to cerebral hypoperfusion. 27
An index of baroreflex function was calculated by dividing the maximal change in heart rate by the maximal change in systolic BP while standing up (measured within the first 30 seconds after standing up).
Meal test
After a 10-minute rest, the patients had 10 minutes to consume a standardized fluid meal. The meal consisted of 100 mL glucose syrup (Nutrical) and 100 mL lactose-free full milk (Soy milk calcium Alpro) with a total energy of 292 calories, 2 g of fat, and 4 g of proteins. Heart rate and BP were continuously measured from 10 minutes before the start of the meal to 75 minutes after the meal. Again, the baseline values of BP and heart rate were defined as the average of the 60 seconds before starting the meal. The mean values of BP and heart rate were calculated from the average of 20 beats taken at 5-minute intervals (10 beats before and 10 beats after each 5-minute interval after ending the meal). The PPH was defined as at least a 20 mm Hg decrease in systolic BP during any of these intervals. 6 Analyses were also repeated using the more stringent criterion of a reduction of 30 mm Hg.
Carotid Massage
Because it was part of the standard diagnostic procedure, to avoid adverse events carotid massage was not performed in patients with carotid bruits or significant carotid stenosis, history of ventricular arrhythmia, or recent history (within last three months) of myocardial infarction (MI) or cerebral ischemia. 28 Patients lie on a tilt table, and after 5 minutes of rest, the right carotid artery sinus is massaged for 5 seconds. One minute after the BP returns to normal or after symptoms or clinical signs cease, the left carotid artery sinus is massaged. In case of a negative result, the test is repeated with the patient in a 70-degree tilt. The heart rate response to carotid massage is the longest R wave to R wave (R-R) interval during or promptly after the massage. The BP response is the average of the 3 lowest, consecutive systolic BP values following massage; the 10-beat average directly before massage is the baseline value. The CSH is defined as an R-R interval of at least 3 seconds (cardioinhibitory type), a 50 mm Hg or greater decrease in systolic BP (vasodepressor type), or a combination of both (mixed type). 29
Statistical Analyses
The SPSS (version 16 for Windows) was used to analyze the data. The significance level was set at .05. Independent t tests and chi-square tests were used for continuous and categorical variables, respectively. Age, body mass index (BMI), GARS, baseline systolic and diastolic BP, heart rate, and the baroreflex index were used as independent variables in 1-way analysis of variance (ANOVA) of cognitive impairment (dependent variable). The 1-way ANOVA was also used to compare the score of MMSE and CAMCOG, in the presence of 1, 2, or 3 hypotensive syndromes (independent variable). We performed an additional analysis with a cutoff value of 30 mm Hg instead of 20 mm Hg for OH and PPH.
Results
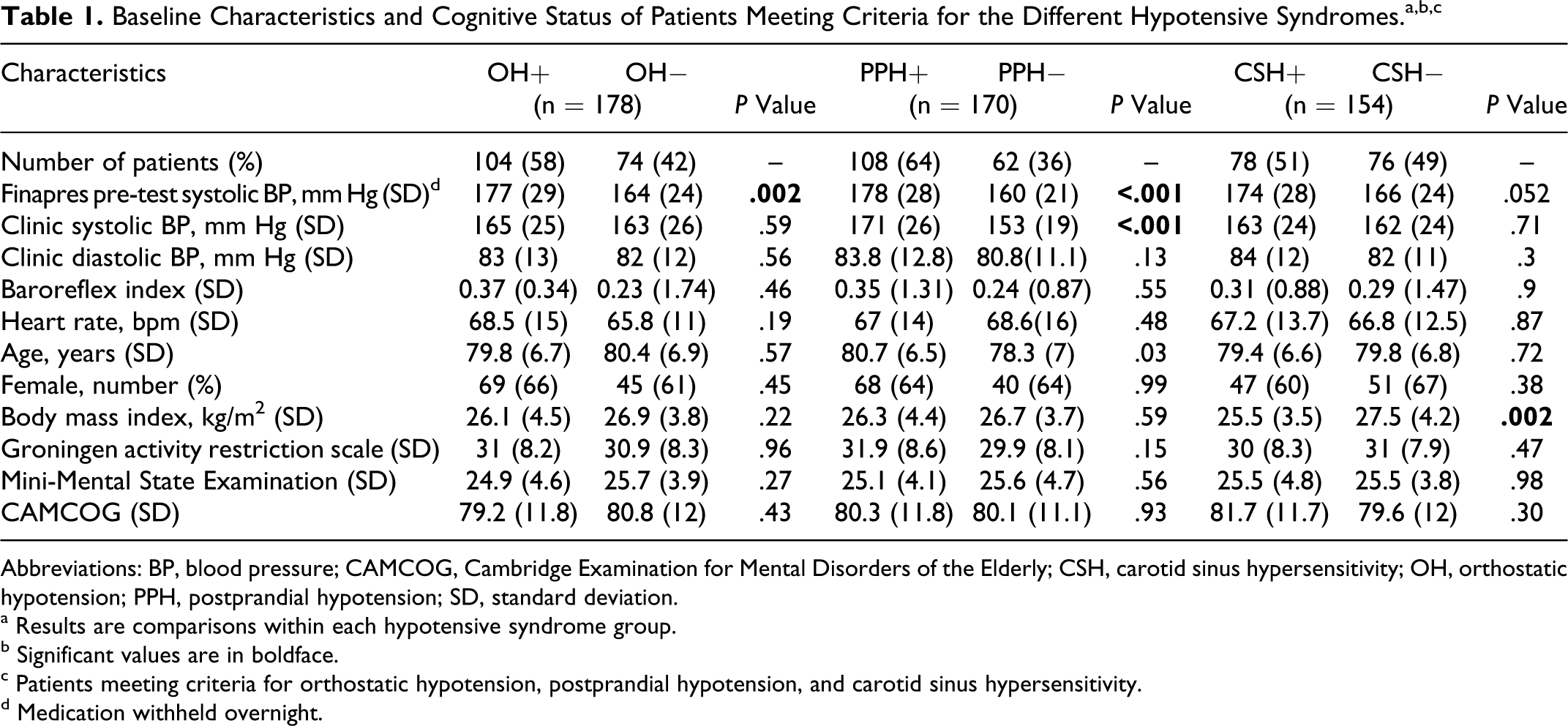
Baseline characteristics are reported in Tables 1 and 2. From the original sample of consecutively referred patients (n = 202), 18 were excluded prior to the SMC test because of very severe dementia (CDR = 3; n = 9), acute illness requiring hospitalization (n = 8), or death (n = 1). The remaining 184 patients were all included, but 6 patients opted out of testing for OH, 14 opted out of testing for PPH, and 30 were excluded from the CSH testing because of the aforementioned contraindications. No complications or adverse events occurred during or after the SMC testing.
Abbreviations: BP, blood pressure; CAMCOG, Cambridge Examination for Mental Disorders of the Elderly; CSH, carotid sinus hypersensitivity; OH, orthostatic hypotension; PPH, postprandial hypotension; SD, standard deviation.
a Results are comparisons within each hypotensive syndrome group.
b Significant values are in boldface.
c Patients meeting criteria for orthostatic hypotension, postprandial hypotension, and carotid sinus hypersensitivity.
d Medication withheld overnight.
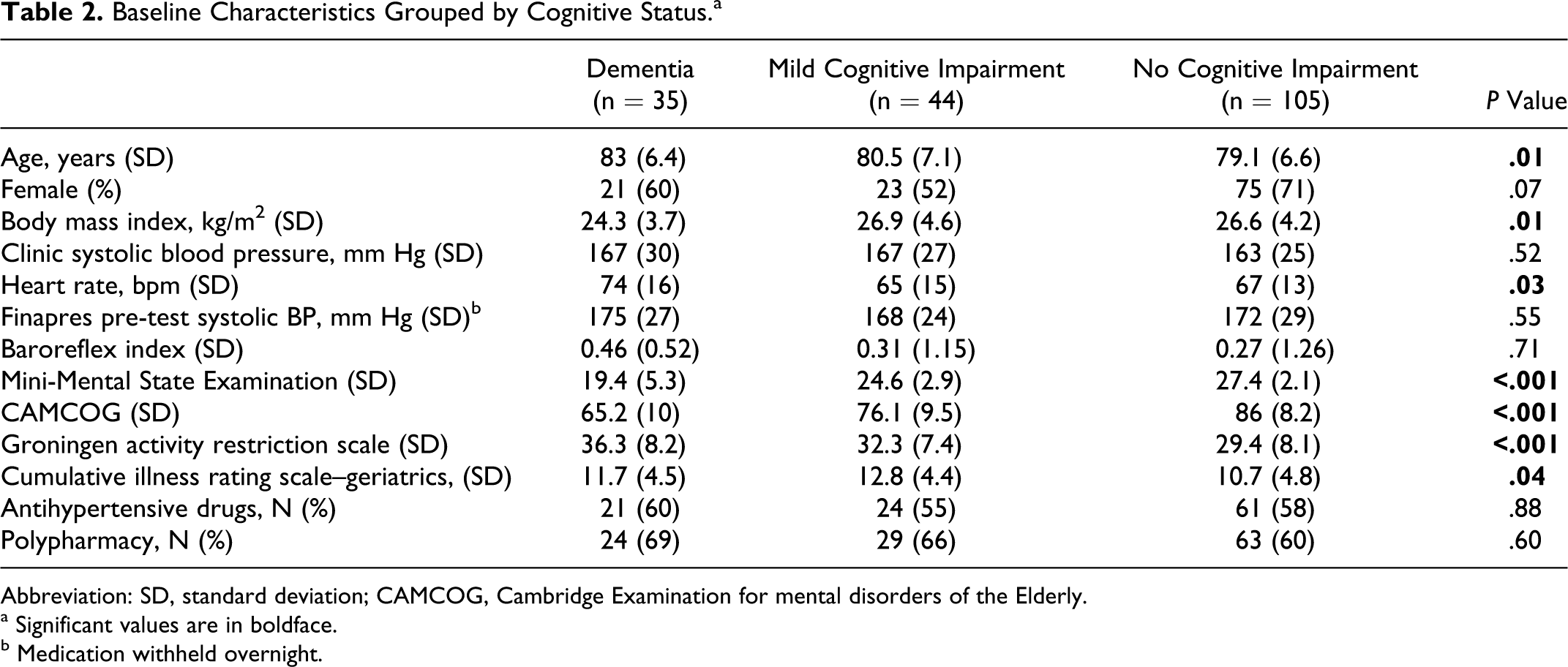
Baseline Characteristics Grouped by Cognitive Status. a
Abbreviation: SD, standard deviation; CAMCOG, Cambridge Examination for mental disorders of the Elderly.
a Significant values are in boldface.
b Medication withheld overnight.
Mean age was 80.2 ± 6.8 years; 65% were female. More than half of patients met the criteria for at least 1 of the 3 hypotensive syndromes; the highest prevalence was for PPH (n = 108; 64%), followed by OH (n = 104; 58%) and CSH (n = 78; 51%; n = 4 cardioinhibitory, n = 46 vasodepressor, n = 28 mixed).
Patients with PPH were older than those without (P = .03); patients with CSH weighed less than those without (P = .002).
Patients with OH and PPH had higher pretest Finapres systolic BP (ie, the measurements taken after overnight withholding of drugs), which was not the case for patients with CSH (Table 1). Patients with PPH also had substantially higher clinic systolic BP, that is, while taking usual medication (171 ± 26 mm Hg vs 153 ± 19 mm Hg, P ≤ .001). Antihypertensive drug use was similar across all the groups and unrelated to the presence of hypotensive syndromes. The use of psychopharmacological medication was also similar across the groups (P = .69; data not shown). There were no differences in the baroreflex index among the groups.
Table 2 shows the comparison of patient characteristics according to the cognitive status. Mild to moderate dementia (CDR 1-2) was diagnosed in 35 (19%) patients with the following diagnoses: probable Alzheimer’s dementia (n = 16), Alzheimer’s disease mixed with vascular pathology (n = 8), probable vascular dementia (n = 5), DLB (n = 3), and frontotemporal dementia (n = 3). The MCI (CDR = 0.5) was diagnosed in 44 (24%) patients. The patients with dementia were older (P = .01), weighed less (P = .01), and had a higher baseline heart rate (P = .03) compared to patients with MCI and patients without cognitive impairment.
Hypotensive Syndromes and Cognitive Status
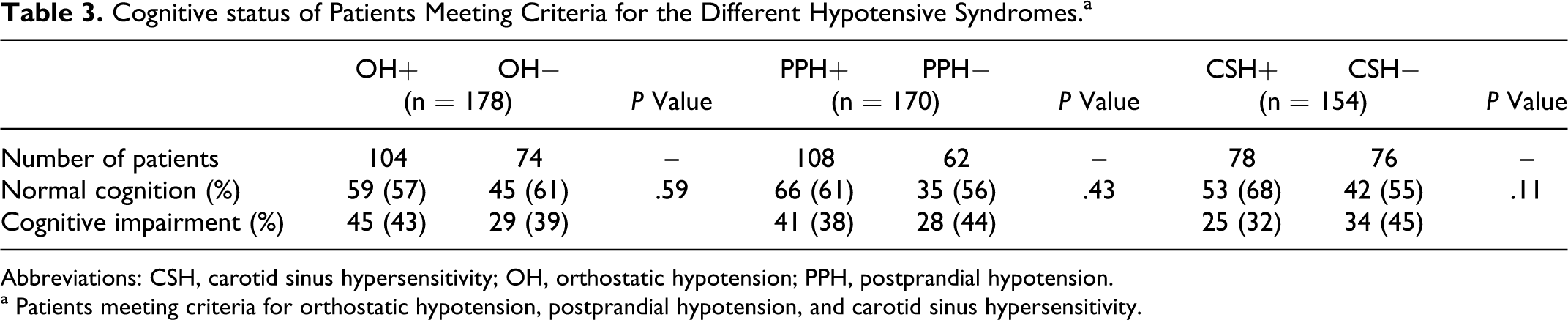
Table 1 shows that patients with hypotensive syndromes did not perform worse on cognitive tests (MMSE and CAMCOG). Table 3 indicates that a clinical diagnosis of cognitive impairment (either dementia or MCI) was not more prevalent in patients with hypotensive syndromes.
Cognitive status of Patients Meeting Criteria for the Different Hypotensive Syndromes. a
Abbreviations: CSH, carotid sinus hypersensitivity; OH, orthostatic hypotension; PPH, postprandial hypotension.
a Patients meeting criteria for orthostatic hypotension, postprandial hypotension, and carotid sinus hypersensitivity.
Figure 1 illustrates the prevalence of hypotensive syndromes in groups categorized by the cognitive status. The prevalence of the 3 hypotensive syndromes was not higher in patients with dementia or MCI. Regression analysis of the relationship between hypotensive syndromes and cognitive diagnosis, correcting for possible confounders such as age, BMI, MMSE, CAMCOG, and GARS scores, did not alter the results.
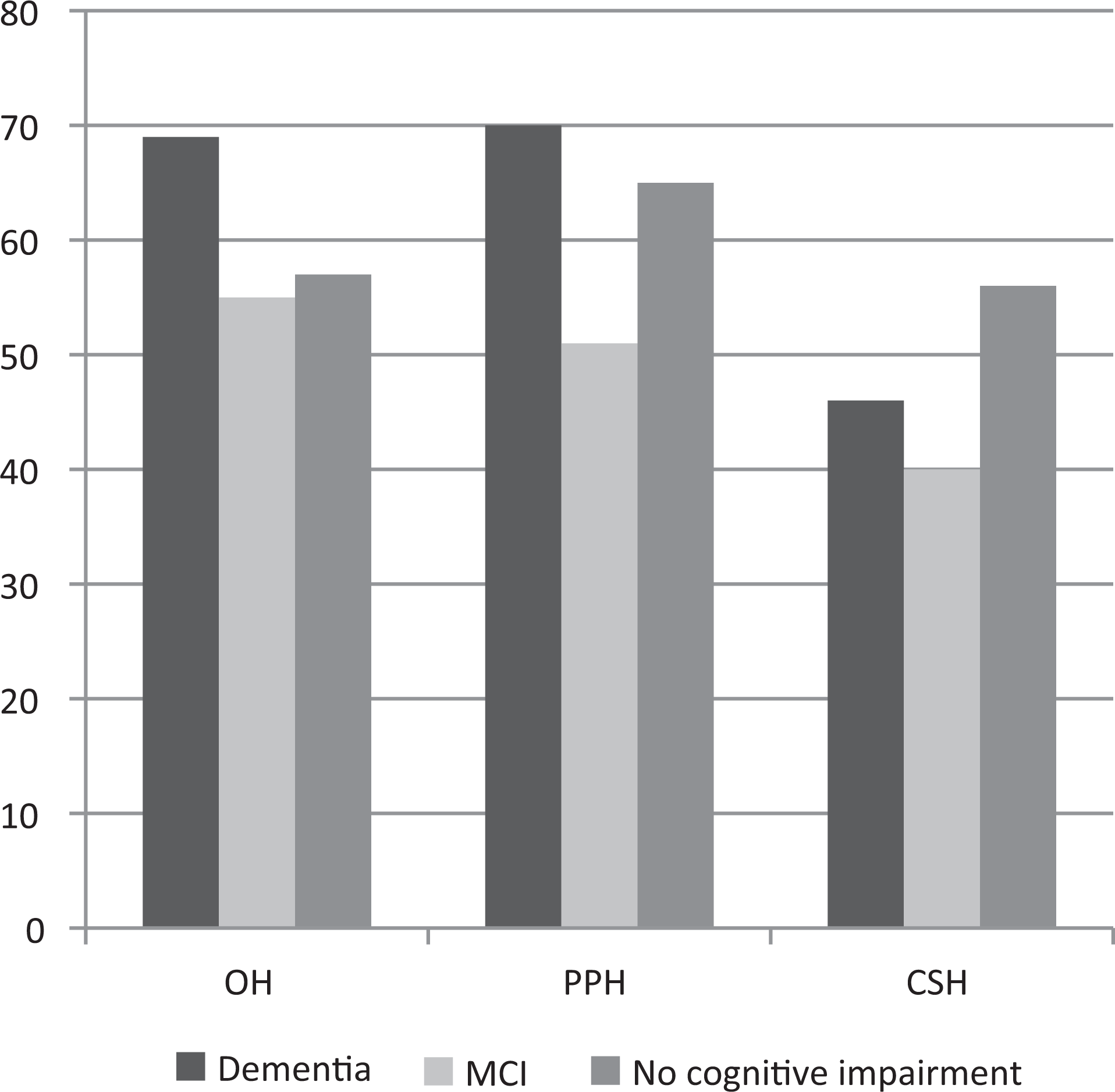
Prevalence of hypotensive syndromes* in relation to cognitive status. Orthostatic hypotension, n = 178; postprandial hypotension, n = 170; carotid sinus hypersensitivity, n = 154. * indicates patients meeting criteria for orthostatic hypotension, postprandial hypotension, and carotid sinus hypersensitivity and MCI indicates mild cognitive impairment. P values are not significant.
The data were re-analyzed using the clinically more relevant cutoff of 30 mm Hg instead of 20 mm Hg decrease in BP for OH and PPH. This reduced the number of patients with OH from 104 to 76 and the number of patients with PPH from 108 to 72; the prevalence was 42% for each syndrome. In these patients with more severe OH and PPH, the prevalence of cognitive impairment was identical to patients without these hypotensive syndromes. Patients with more severe OH and PPH were older (OH 81.5 ± 6 years; PPH 81.8 ± 6.3 years) than patients without OH or PPH (78.9 ± 7.1 and 78.4 ± 6.8 years, P = .001). They had higher pretest Finapres systolic BP (P < .001), and patients with PPH again had substantially higher clinic systolic BP (175 ± 25 mm Hg vs 156 ± 22 mm Hg, P < .001) and worse functional performance (GARS 32.8 ± 9 versus 30 ± 7.8, P = .04).
Of all 184 patients, 73 patients had 2 hypotensive syndromes (OH and PPH in 34, OH and CSH in 23, and PPH and CSH in 16), and 27 patients had all 3. The prevalence of cognitive impairment did not differ among patients with none, 1, 2, or 3 hypotensive syndromes.
During testing, hypotensive symptoms were reported by 40% of the patients with OH, 62% of patients with PPH, and 14% of patients with CSH. Cognitive impairment/dementia did not influence the report of hypotensive symptoms.
Discussion
The main finding of this study is that patients with recurrent episodes of low BP (hypotensive syndromes) were not likely to have cognitive impairment. More than half of this geriatric population, referred to a Falls and Syncope clinic, met the criteria for OH, PPH, or CSH. Forty-two percent of the patients had cognitive impairment, and half of those patients had dementia. However, the prevalence of cognitive impairment was unrelated to whether patients had 1, more than 1, or no hypotensive syndrome.
The study population was a selected group of patients. As was illustrated by the comorbidity and functional performance scores and polypharmacy, patients were frail. A high prevalence of hypotensive syndromes is correlated with comorbidity. 6,7 The prevalence rate of 58% for OH was slightly higher in a comparable population, 6 whereas the prevalence for PPH and CSH was in line with the other studies. 9 –11 In contrast to the limited measurements of cuff BP in most OH prevalence studies, this study used continuous measurements of beat-to-beat BP and heart rate. Thus, our study had increased sensitivity to detect hypotensive syndromes. Nevertheless, even with a less sensitive but more specific threshold for the diagnosis of OH and PPH (a reduction of 30 mm Hg instead of 20 mm Hg), the prevalence of both syndromes remained high.
The BP measurements were performed in all patients, even if there was no clinical suspicion for a hypotensive syndrome (less than 25% of the patients were referred for syncope, eg, patients with a clear alternative explanation for a fall). In line with the previous work, the high prevalence rate of hypotensive syndromes in this study is probably an accurate reflection of a high prevalence of BP instability in elderly patients. This study adds to previous reports because it combined assessments of the 3 most common hypotensive syndromes in conjunction with a highly sensitive method of continuous BP registration.
The selection of this study population led to an enriched sample with regard to the prevalence of hypotensive syndromes and cognitive impairment, increasing the power to detect an association between the 2. However, no such association was found. We will discuss the possible explanations for our findings.
A cutoff value of 20 mm Hg for OH and PPH may lead to the inclusion of the patients with insignificant reductions in brain perfusion pressure. In this population with an average systolic pressure between 160 and 170 mm Hg, a 20 mm Hg reduction in BP may not lead to a critical reduction in brain perfusion that could lead to cognitive impairment. 27,30 However, using a cutoff of 30 mm Hg, which creates a subgroup of patients with more severe hypotensive episodes, did not change the results.
The impact of a hypotensive episode on the brain depends on its magnitude and duration. The 3 syndromes cover a spectrum from short (CSH, 3-10 seconds) to long duration (PPH, several minutes). Also the frequency of the episodes may determine the effect on the brain. The OH may occur several times a day, each time a patient stands up; PPH frequency depends on the number and type of meals per day. The CSH-induced hypotension may be related to head rotation, but the frequency of these episodes can only be speculated. 31 Despite their potential differences in the impact on the brain, there was no difference in the prevalence of cognitive impairment among the syndromes, nor was there evidence for a dose–effect relationship, that is, having more than 1 syndrome had no effect on the cognitive status.
Given the gradual onset of most cases of dementia, the noticeable effects of episodic hypotension on the brain may be delayed. The cross-sectional design of the study is limited because the duration of the hypotensive syndromes is unknown. Referral to a Falls and Syncope clinic could suggest a recent onset of the syndromes. However, the high prevalence of these syndromes with aging, even in random samples of asymptomatic elderly individuals, suggests otherwise. 7,10 In addition, in a large proportion of patients in this study, dizziness or syncope was not the reason for referral, and the hypotensive syndromes were considered a chance finding in many patients with clear alternative explanations for their fall. Therefore, we argue that the hypotensive syndromes will have been present for months or years.
Cognitive impairment, especially if mild, may have been missed. However, all patients underwent a standardized comprehensive diagnostic evaluation of the cognitive function; it is improbable that cognitive impairment was selectively missed in patients with hypotensive syndromes. On the other hand, patients with more severe cognitive impairment may not have been referred for fall or syncope analysis, thereby limiting this study to patients with MCI and mild to moderate dementia.
Our findings confirm an earlier observation that orthostatic hypotension was unrelated to cognitive function in home dwelling and institutionalized elderly individuals (>70 years). 32 Using the MMSE, these authors found that orthostatic hypotension (systolic or diastolic) did not predict cognitive decline. 32 The present study adds a more rigorous assessment of both BP and cognitive function. In patients with Parkinson’s disease, who due to autonomic failure may have frequent exposure to hypotensive episodes, there was no association between OH or PPH and cognitive impairment. 33
The apparent absence of a relationship between hypotensive syndromes and cognitive impairment could indicate, even in frail elderly individuals, that the brain is able to sustain periods of low BP. The mechanism that stabilizes brain perfusion following a change in BP is known as cerebral autoregulation. 27 Despite the commonly held opposite view, 4 a recent review found no evidence that cerebral autoregulation is impaired in the elderly patients over 75 years old, 27 and autoregulation was also not impaired in older patients with dementia. 30
A potential limitation of this study is that advanced neuroimaging, such as volumetric analyses of white matter lesions or diffusion tensor imaging using magnetic resonance imaging (MRI), were not used as indicators of cerebrovascular damage from hypotensive episodes or balance deficits. However, our outcome measure of a clinical diagnosis of dementia or MCI can be regarded as more clinically relevant. Subanalysis was not possible because of the low number of diagnosed vascular dementia.
Many of our patients had hypertension, and we found that patients with hypotensive syndromes had higher BP. This supports the evidence that hypertension predisposes patients to hypotensive syndromes. 34,35 We temporarily stopped all overnight medication prior to the BP tests to disentangle drug-related hypotensive effects from hypotensive syndromes and inherent BP regulation disorders.
Use of antihypertensive medication may affect dementia risk 36 and could have affected results; however, excluding patients on antihypertensive drugs did not affect the outcome of our study.
In conclusion, this study adds for the first time a report of 3 common hypotensive syndromes together, in conjunction with a highly sensitive method of continuous BP registration. We found no evidence that episodic hypotension increases cognitive impairment in a group of frail elderly individuals. Our data do not support the suggestion that geriatric patients may be more harmed by episodic hypotension than by high BP. The high prevalence of hypotensive syndromes further indicates that blood pressure should not be considered to be a static phenomenon in this population. Episodic hypotension from hypotensive syndromes and visit-to-visit variability 37 in BP should be taken into account when trying to elucidate the effects of BP on the brain.
Footnotes
Acknowledgments
We would thank Anja Bos, PA, for performing and analyzing the SMC tests in all patients.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.