
Abstract
Frontotemporal dementia (FTD) is the second most common type of presenile dementia and is the most common form of dementia with the onset before 60 years of age. Its typical symptoms include behavioral disorders, affective symptoms, and language disorders. The FTD is a genetically and pathologically heterogeneous degenerative disorder. Animal models have provided more insights into the pathogenic mechanisms. There are currently no medications that are specifically approved for the treatment of FTD by the Food and Drug Administration. In this article, we review the recent advances in the molecular pathogenesis, pathology, animal models, and therapy for FTD. Better understanding of the pathogenesis and the use of animal models will help develop novel therapeutic strategies and provide new targets for FTD treatment.
Introduction
Frontotemporal dementia (FTD) is an insidious, progressive neurodegenerative disease. It is the second most common dementia with presenile onset, after Alzheimer’s disease (AD), and accounts for 5% to 15% of all types of dementia. 1,2 It is a costly disease, both in terms of personal suffering and economic loss. The 3 typical clinical syndromes of FTD include behavioral, emotional, and language disorders. 3 Patients with FTD typically present with symptoms including personality changes, impulsivity, psychiatric disorders, hyperthymia or apathy, and overactivity. It encompasses a range of clinical syndromes such as behavioral variant frontotemporal dementia (bvFTD), semantic dementia (SD), corticobasal syndrome (CBS), progressive nonfluent aphasia (PNFA), and a range of different pathologies. 4 Each subtype of FTD includes some significant syndromes. Specifically, some patients of bvFTD become apathetic and social withdrawn, or oppositely others can become disinhibited and perform some inappropriate acts such as sexual or criminal behaviors. Patients of SD have trouble in naming and semantic understanding, but are intact with word pronunciation and speech fluency. In contrast, patients of PNFA have inability to articulation but without trouble in word comprehension. Patients of CBS have difficulties in movement, but differentiate diagnosis with Parkinson disease and progressive supranuclear palsy (PSP) is needed. The clinical presentations of FTD differ from those of AD. In the early stages of FTD, patients typically present with personality and behavioral changes, including impulsivity, disinhibition, executive dysfunction, and language abnormalities. In contrast to patients of AD, patients of FTD usually perform relatively well in visuospatial ability and memory tasks. 5 As the clinical manifestations overlap with other psychiatric disorders such as personality disorders, affective disorders, and AD, FTD is often misdiagnosed.
In this article, we use FTD as general term for the clinical syndromes and frontotemporal lobe degeneration (FTLD) for the associated pathologies. Here, we review the recent research progress in the molecular genetics, pathology, animal models, and therapy of FTD.
Molecular Genetics
Frontotemporal dementia is a genetically and pathologically heterogeneous degenerative disorder. 6,7 Approximately one-third to one-half of the FTD cases are caused by gene mutations, 8 but the majority are sporadic without a definite known cause. There are many pathogenic genes related to FTD. Mutations in the genes of microtubule-associated protein tau (MAPT), progranulin (PGRN or GRN), and C9ORF72 have been shown as the major causes of FTD. Minority of cases are caused by mutations in 4 other genes: valosin-containing protein (VCP), TAR DNA-binding protein 43 (TARDBP), chromatin-modifying protein 2B (CHMP2B), and fused in sarcoma (FUS). In addition, an involvement of apolipoprotein E (apoE) gene locus in the genetics of FTD has been reported. 9
Microtubule-Associated Protein Tau
The MAPT gene lies on chromosome 17q21.1. The major function of tau is to stimulate the microtubule assembly and to maintain the microtubule structure, which is crucial to maintaining the integrity of nerves and axoplasmic transport. The MAPT gene has been shown to contain 2 extended haplotypes, termed as H1 and H2. The H2 haplotype is associated with the appearance of clinical symptoms in carriers at a relatively earlier age and with a dramatic decline in glucose utilization in the frontal brain areas. 10 Altered metabolism of tau protein affects its interactions with tubulin, leading to destabilization of the microtubule structure and initiating the generation of toxic tau aggregates and may be a cause of FTD. 11
It has been shown that cerebral spinal fluid (CSF) levels of tau are abnormal and amyloid-β peptide (1-42) levels are decreased in patients of FTD. 12 Distinguishing features of patients with tau-positive FTD include visual perceptual–spatial difficulties and extrapyramidal disorders, and these are observed more frequently than in other patients of FTD. These patients have relatively significant cortical atrophy in the frontal and parietal regions as shown by magnetic resonance imaging (MRI), and the pathology in these regions is obvious. Patients with tau-negative FTD are also distinguished by their greater difficulties on social intercourse, language, and executive functions. This is accompanied by significant cortical atrophy in the frontal and temporal regions and significant frontal and temporal pathology. 13
Progranulin
Progranulin is encoded by a single gene on chromosome 17q21. Loss-of-function mutations in the PGRN gene have been identified as a monogenic cause of FTLD. 14 –16 In patients of FTLD with ubiquitinated inclusions (FTLD-U), there are mutations in the gene coding for PGRN. 14-15 Davion et al suggest that PGRN mutations may also occur in apparently sporadic FTD-U cases. 17 Chiang et al reported that PGRN mutations may be one of the causes of FTD in the Karolinska family. 18 It has been reported that haplo insufficiency of PGRN resulting from PGRN gene mutations is one of the predominant mechanisms leading to FTD. 19,20 And recently suberoylanilide hydroxamic acid, a Food and Drug Administration (FDA)-approved histone deacetylase inhibitor, has been identified as an enhancer of PGRN expression. 21 It has demonstrated therapeutic potential in other neurodegenerative diseases and thus holds promise as a first-generation drug for the prevention and treatment of FTD.
Recently, there is evidence provided by Bossu et al that circulating interleukin (IL)-6 is increased in the PGRN-mutated patients of FTD when compared to both patients of PGRN nonmutated FTD and controls. 22 They concluded that the profile of circulating proinflammatory cytokines is altered in PGRN-related symptomatic FTD. Thus, IL-6 is as a possible specific mediator and a potential therapeutic target in this monogenic disease.
In addition, patients with FTD with PGRN mutations have a faster rate of whole brain atrophy than patients of FTD with MAPT mutations, but similar rates of hippocampal atrophy. 23 Neuroimaging studies show that PGRN and MAPT mutations have distinct patterns of atrophy—asymmetric fronto-temporo-parietal atrophy with PGRN versus relatively symmetric medial temporal and orbitofrontal lobe atrophy with MAPT mutations. 24
C9ORF72 Gene
DeJesus-Hernandez et al 25 reported an expansion of a noncoding GGGGCC hexanucleotide repeat in the gene C9ORF72 that is strongly associated with the disease in a large FTD/amyotrophic lateral sclerosis (ALS) kindred, previously reported to be conclusively linked to chromosome 9p. Their findings indicate that repeat expansion in C9ORF72 might be a major cause of both FTD and ALS. This view was supported by Renton et al. 26 They found that a large proportion of apparently unrelated familial ALS and FTD cases carried the same hexanucleotide repeat expansion within C9ORF72. This repeat expansion segregates perfectly with the disease in the Finnish population, underlying 46.0% of familial ALS and 21.1% of sporadic ALS in that population. Taken together with the D90A superoxide dismutase 1 (SOD1) mutation, 87% of familial ALS in Finland is now explained by the simple monogenic cause. The repeat expansion is also present in one-third of familial ALS cases of outbred European descent, making it the most common genetic cause of these fatal neurodegenerative diseases identified to date. These studies demonstrate that a massive hexanucleotide repeat expansion within C9ORF72 is the cause of chromosome 9p21-linked ALS, FTD, and ALS-FTD. Recently, it was reported that the C9ORF72 gene mutation was associated with patterns of atrophy, predominantly frontal lobe atrophy, with involvement of the anterior temporal, parietal lobes, and cerebellum. 27 This specific pattern differed from that observed in MAPT and GRN mutations and sporadic behavioral variant of FTD.
Valosin-Containing Protein
The VCP is a member of the AAA-ATPase gene superfamily and functions as a molecular chaperone in a plethora of distinct cellular activities, including ubiquitin-dependent, endoplasmic-reticulum-associated protein degradation, stress responses, programmed cell death, membrane fusion, nuclear envelope reconstruction, and postmitotic Golgi reassembly. Many of these activities are directly or indirectly regulated by the ubiquitin proteasome system (UPS). 28,29 The VCP gene mutations can cause inclusion body myopathy, Paget’s disease of the bone, and FTD. 30 However, the mechanisms by which VCP mutations cause neurodegeneration and TAR DNA-binding protein 43 (TDP-43) accumulation are unclear.
TAR DNA-Binding Protein 43
The TDP-43, which is encoded by the TARDBP gene located on chromosome 1, is the major pathological protein in FTLD-U. 31 –34 The TDP-43 continuously shuttles between the nucleus and the cytoplasm. This process is partially regulated by nuclear localization signals and nuclear export signals. 35,36 The TDP-43 manages the regulation of transcription and splicing and is a neuronal activity-responsive factor functioning in the regulation of neuronal plasticity. 37 In addition, it is involved in other cellular processes such as apoptosis, cell division, micro RNA biogenesis, and messenger RNA stabilization. 38,39 The loss of normal TDP-43 function may contribute to the pathogenesis of FTLD. 39
The FUS Gene
The FUS gene, on chromosome 16, was originally identified as a component of fusion oncogenes in a variety of human cancers. 40 It encodes FUS protein, which is a ubiquitously expressed, 41 multifunctional, DNA/RNA-binding protein that shares striking functional homology with TDP-43. 42,43 The FUS is a highly conserved ribonucleoprotein that mainly resides in the nucleus while shuttling between the cytoplasm and the nucleus, 44,45 but in neurons and glia, it has a predominant nuclear localization. 41 The normal physiological role of FUS in the brain is not completely understood, but it may be involved in neuronal plasticity and the maintenance of dendritic integrity. 46,47 The FUS has recently been linked to both ALS and FTLD. 42,48 The FUS inclusions are seen in the brains of many FTD cases (FTLD-FUS). 4,49
Chromatin-Modifying Protein 2B
The first CHMP2B mutation was identified in a large Danish FTLD family 50 and the second mutation was subsequently identified in a Belgian patient with familial FTLD. 51 These mutations lead to C-terminal truncation of the CHMP2B protein. Animal models of the CHMP2B gene mutations have been generated and will be discussed below.
Pathology
The neuropathology of FTLD syndromes is heterogeneous. The 2 major pathologies are FTLD-tau and FTLD-TDP, which are characterized by tau or TDP-43 positive inclusions, respectively. 4,52 The FUS-positive inclusions have recently been described in a subset of FTLD cases 53,54 and 2 rare neuropathological subtypes remain, those with ubiquitin-positive inclusions that are negative for tau, TDP-43, and FUS, termed FTLD-UPS 49 (primarily CHMP2B mutation cases) and those with no discernable inclusions, termed FTLD-ni. 49 The nomenclature for FTLD has been updated (Table 1). 49
Nomenclature for Frontotemporal Lobar Degeneration (Mackenzie et al 49 ).
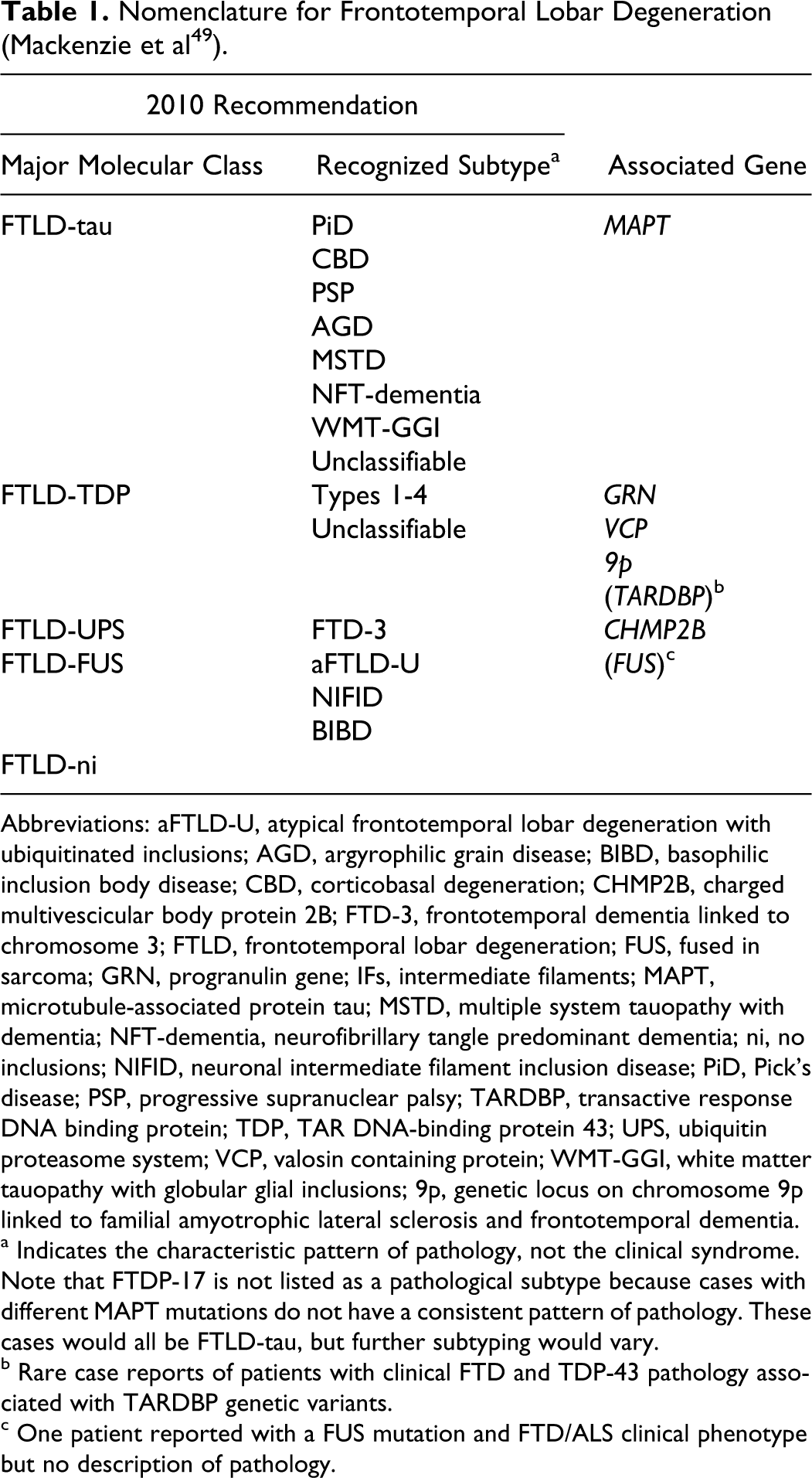
Abbreviations: aFTLD-U, atypical frontotemporal lobar degeneration with ubiquitinated inclusions; AGD, argyrophilic grain disease; BIBD, basophilic inclusion body disease; CBD, corticobasal degeneration; CHMP2B, charged multivescicular body protein 2B; FTD-3, frontotemporal dementia linked to chromosome 3; FTLD, frontotemporal lobar degeneration; FUS, fused in sarcoma; GRN, progranulin gene; IFs, intermediate filaments; MAPT, microtubule-associated protein tau; MSTD, multiple system tauopathy with dementia; NFT-dementia, neurofibrillary tangle predominant dementia; ni, no inclusions; NIFID, neuronal intermediate filament inclusion disease; PiD, Pick’s disease; PSP, progressive supranuclear palsy; TARDBP, transactive response DNA binding protein; TDP, TAR DNA-binding protein 43; UPS, ubiquitin proteasome system; VCP, valosin containing protein; WMT-GGI, white matter tauopathy with globular glial inclusions; 9p, genetic locus on chromosome 9p linked to familial amyotrophic lateral sclerosis and frontotemporal dementia.
a Indicates the characteristic pattern of pathology, not the clinical syndrome. Note that FTDP-17 is not listed as a pathological subtype because cases with different MAPT mutations do not have a consistent pattern of pathology. These cases would all be FTLD-tau, but further subtyping would vary.
b Rare case reports of patients with clinical FTD and TDP-43 pathology associated with TARDBP genetic variants.
c One patient reported with a FUS mutation and FTD/ALS clinical phenotype but no description of pathology.
Josephs et al have observed severe caudate atrophy at autopsy in FTLD-FUS, and they hold the view that one of the most characteristic features of FTLD-FUS is severe caudate atrophy, identified on gross and microscopic examination. 55,56 Caudate atrophy on MRI appears to be significantly greater in FTLD-FUS compared to FTLD-TDP and FTLD-TAU, suggesting that severe caudate atrophy may be a useful clinical feature to predict FTLD-FUS pathology. 57
A significant decrease in sAβPPβ, Aβ38, and Aβ40 levels in CSF is found in FTD. 58 Significant changes in amyloid biomarkers, particularly for Aβ38, are therefore seen in FTD and that can be considered as a potential biomarker to differentiate FTD. Thus, this could be quite useful for diagnostic purposes and might provide additional evidence on the interrelationship between Tau and AβPP biology.
Animal Models
Animal models are useful in dissecting the pathogenic mechanisms and offer a valuable technique for further investigations into FTD. Here, we summarize several types of animal models reported in recent years.
The FUS Transgenic Rats
Mutant FUS transgenic rats have been recently generated. 59 These rats developed progressive paralysis secondary to degeneration of motor axons and displayed a substantial loss of neurons in the cortex and the hippocampus. This neuronal loss is accompanied by ubiquitin aggregation and glial reactivation in the brain. Although transgenic rats that overexpressed the wild-type human FUS were asymptomatic at young ages, they show a deficit in spatial learning and memory and a significant loss of cortical and hippocampal neurons at advanced ages. These results suggest that mutant FUS is more toxic to neurons than normal FUS and that increased expression of normal FUS is sufficient to induce neuronal death. The FUS transgenic rats reproduced some phenotypes of ALS and FTLD and will provide a useful model for mechanistic studies of FUS-related diseases.
The CHMP2B Transgenic Mice and CHMP2B Knockout Mice
Ghazi-Noori et al 60 generated the first mouse model of CHMP2B-induced neurodegeneration and showed that expression of mutant CHMP2Bintron5 leads to striking neurodegenerative changes that were not observed in CHMP2Bwild-type transgenics or CHMP2B knockout mice. Their studies have provided evidence in favor of a gain-of-function mechanism for CHMP2B-induced FTLD by showing neuropathology mimicking human patients only in the CHMP2Bintron 5 mice and not in the CHMP2Bwild-type mice or Chmp2b knockout mice. They also identify axonal changes as an early degenerative feature in the CHMP2Bintron 5 mice, suggesting a potential role for altered axonal function in the disease process. The generation of this CHMP2Bintron5 mouse model has provided new insight into the mechanisms by which mutant CHMP2B leads to neuronal dysfunction in vivo.
Mouse Models of PGRN-Deficient FTLD
It has been reported that certain aspects of PGRN-deficient FTLD can be modeled in the mouse (Grn−/−). 61 Large number of activated microglia and astrocytes are accumulated in the brains of aged Grn−/− mice. 8,62 Abnormal microgliosis and astrogliosis can be detected as early as 7 months of age, the same age at which social behavior abnormalities are first observable. Also by this time, abnormal intracellular accumulations of ubiquitinated autofluorescent lipid–protein aggregates called lipofuscin, which are by-products of failed proteolysis, begin to be seen in the Grn−/− neurons. 63 However, the Grn−/− mice do not develop significant cytoplasmic accumulations of TDP-43. This model will provide an important platform for understanding the pathophysiology of FTLD and the basic biology of PGRN in the brain.
Loss-of-function mutations in the PGRN gene were recently identified as the cause of tau-negative, ubiquitin-positive FTD. 14-15 Subsequently, PGRN-deficient mice were used to investigate the role of PGRN in FTD. In this model, the mice display behavioral deficits in social recognition and depression- and anxiety-like behaviors. Moreover, these mice develop cognitive deficits that progress with aging. These deficits are associated with neuropathological changes, such as accumulation of ubiquitin and cytosolic phosphorylated TDP-43 in the hippocampus. 62
P301L Tau Mice
The expression of human FTD mutant P301L tau has been reported to reproduce tau aggregation and neurofibrillary tangle formation in mice. 64,65 These tau transgenic models of FTD have shown that FTDP-17 mutations accelerate tau aggregation and cause neuronal dysfunction and loss in vivo. Furthermore, the tau transgenic mice model has important aspects of FTD, such as PSP and corticobasal degeneration, through the exhibition of glial pathology that affects neuronal function and thus the manifestation of these behavioral symptoms. 66
A novel research approach has incorporated a single mutation, which is homologous to the common FTDP-17T P301L mutation, directly into the endogenous mouse gene. The “P301L” tau knockin mouse model mimics the human disease.67.In contrast to existing transgenic mouse models that overexpress human P301L mutant tau, no overt tau pathology develops during the normal life span of the knockin mice. This model may therefore represent the earliest pathological alterations caused by tau dysfunction.
The models described above have provided powerful tools for our further understanding of relevant human diseases. However, they may not accurately reproduce the anatomical distribution of the lesions in the human brain. The mouse models are thought to be superior to the invertebrates in studying memory and motor functions in consideration of neuroanatomy and the endocrine system. However, recent work in invertebrate species highlights the advantages in dissecting signaling pathways, performing modifier screenings and analyzing families of mutations in parallel.
K3 Mice Model for Human FTD With the K369I Mutation
The K3 mice, a transgenic mouse strain which is reported to express human tau carrying the FTD mutation K369I, not only model histopathological characteristics of FTD with the K369I tau mutation but also models memory impairment, amyotrophy, and Parkinsonism. The K3 mice provide a unique model for aspects of Pick’s disease, but are mainly used to explore FTD-associated Parkinsonism and memory impairment. 68
Therapy
There has been considerably less research focusing on the treatment of FTD than that of AD. There are currently no FDA-approved medications specifically indicated for the treatment of FTD. 69 At present, several pharmacological approaches, such as antidepressants, antipsychotics, anticholinesterase agents, and memantine, have been widely used clinically in order to control the specific symptoms of FTD. López-Pousa et al 70 performed a cross-sectional design using 1092 cases with AD and 64 cases with FTLD registered by the Registry of Dementias of Girona. They found that 43.8% of the patients of FTLD took antidementia drug, 31.3% of the patients of FTLD used antipsychotics, 1.6% of the patients of FTLD used anti-Parkinson drug, and 53.1% of the patients took antidepressants. However, they concluded a discrepancy regarding clinical practice and the recommendations based upon clinical evidence. On the whole, it does not mean that there is little effect on drug treatment. Specifically, antidepressants and antipsychotics mainly appear to improve behavioral symptoms of FTD including irritability, agitation, depressive symptoms, and eating disorders. 71 –75 Anticholinesterases and memantine have been widely used in the treatment of AD. Acetylcholinesterase inhibitors (AChEIs) can improve the cognitive performance, activities of daily living, behavioral symptoms, and executive function as well as visual attention. 76 –78 They can also reduce the worsening of clinical AD symptoms. 79 However, AChE inhibitors were not found effective or even can worsen the disinhibition and compulsions rather than exert a beneficial effect in patients with FTD. 80 –82 Memantine, a more recent AD drug, shows significant benefits on cognitive abilities and global functioning. 83 Some studies have also shown that it can improve the language function 84 and may help alleviate the behavioral symptoms. 85 As to FTD, the efficacy of memantine is relatively positive.
Antidepressant and Antipsychotics
Studies of antidepressant medications for FTD have mainly been focused on serotonin selective reuptake inhibitors (SSRIs), trazodone, and atypical antipsychotic drugs.
The SSRIs
The recovery of the serotoninergic system may play an important role in the effective treatment of FTD. 86 The SSRIs (including fluoxetine, sertraline, and paroxetine) appear to improve the behavioral symptoms 71-72 and decrease the disinhibition impulsivity, repetitive behaviors, and eating disorders in FTD. 73 However, little evidence for a curative effect on the cognitive symptoms has been found. 71 Ishikawa et al described 2 patients with FTD with compulsive complaints of pain. 87 Fluvoxamine markedly improved their complaints of pain as well as other typical symptoms. Fluvoxamine may be effective in addressing behavioral disturbances due to an improvement in serotoninergic dysfunction in the frontal medial and cingulate cortices. It may also be effective in managing compulsive complaints of pain as a result of improvement in compulsive symptoms and exaggerated reactions to pain in FTD or, alternatively, of the analgesic effect of the SSRI. Moretti et al conducted an open-label, randomized, uncontrolled study. 88 Patients aged 64 to 68 years with a diagnosis of FTD were randomized to receive paroxetine up to 20 mg/d (n = 8) or piracetam up to 1200 mg/d (n = 8). At 14 months, the patients treated with paroxetine showed significant improvements in behavioral symptoms and the side effects were easily tolerable and there were no dropouts. However, Deakin et al reported conflicting findings based on a double-blind, placebo-controlled crossover trial in 10 patients with FTD. 89 Doses of paroxetine were progressively increased to 40 mg daily and the same regimen was used for placebo capsules. All participants were assessed using a battery of cognitive tests in the sixth week following the onset of treatment. At each assessment, caregivers were interviewed using the Neuropsychiatric Inventory (NPI) to assess delusions, hallucinations, agitation, depression, anxiety, euphoria, apathy, disinhibition, irritability, and aberrant motor behavior. The Cambridge Behavioral Inventory (CBI) was also used to assess the changes in behavior, personality, mood, memory, orientation, and activities of daily living. The results showed that there were no significant differences in either the NPI or the CBI scores between the 2 groups. However, paroxetine caused a decrease in accuracy in paired associates learning, reversal learning, and delayed pattern recognition. Thus, in opposition to the view of Moretti et al, the researchers reported that a chronic course of paroxetine may selectively impair the aspects of cognitive function. The discrepancy in the results of the above 2 studies may be due to the differences in the participants studied. For example, some patients with advanced FTD may have severe depletion of the 5-hydroxytryptamine (5-HT) receptor-containing neurons and declining paroxetine’s effects. The discrepancy could also be due to procedural and methodological differences including drug selection and dose differences.
Trazodone
At present, most studies on trazodone have confirmed that trazodone has a positive effect in patients with FTD. It appears to be an effective treatment for the behavioral symptoms including irritability, agitation, depressive symptoms, and eating disorders. In addition, it can moderately control the clinical severity, 73,90 although results from the Mini-Mental State Examination have not shown significant improvement between pre- and posttreatment. There are 2 major shortcomings in these studies, namely small sample sizes and inconsistent evidence for improvement. Further investigation with a larger cohort is needed to reveal the efficacy. Whether trazodone may act by modulating the function of 5-HT system and the corresponding receptors also warrants future studies.
Antipsychotics
Antipsychotics, such as aripiprazole and olanzapine, can improve the clinical symptoms of FTD such as behavioral disturbances and irritability. 73 –75 Unfortunately, they may also cause side effects, such as somnolence, weight gain, Parkinson’s symptoms, and increase susceptibility to extrapyramidal side effects, 91 which limit their therapeutic use.
Anticholinesterases and Memantine
Due to the efficacy of cholinesterase inhibitors and memantine for AD, their use for treating bvFTD is common, despite the lack of strong evidence to support such treatment. 92 Because no drugs specific for treating FTD are currently available, AD drugs are commonly used for improving the clinical outcome of patients with FTD.
Cholinesterase inhibitors
The pathophysiology of FTD and AD is somewhat different. It has been confirmed that the acetylcholine system appears to be relatively intact in patients with FTD. 71,93,94 Di Lazzaro et al used short latency afferent inhibition of the motor cortex to examine the function of central cholinergic circuits. Dysfunction of the central cholinergic circuits was observed in AD but not in FTD. 95 The issue of whether cholinesterase inhibitors may be effective in the treatment of FTD has caused concern among researchers. Rivastigmine, an inhibitor of acetylcholinesterase and butyrylcholinesterase, was reported to improve the behavioral impairment and reduce the caregiver burden of patients with FTD. 96 However, donepezil, another AChE inhibitor, was found to worsen disinhibition and compulsions rather than exert a beneficial effect. 80 It has been confirmed that galantamine, also an AChE inhibitor, is not effective in bvFTD, although a trend for efficacy was found in primary progressive aphasia. 55 A recent study reported that significant brain cholinergic deficits are not seen in FTD by [ 11 C] N-methylpiperidin-4-yl acetate positron emission tomography. 97 This finding may explain the unresponsiveness of patients with FTD to cholinergic modulation therapy.
Memantine
As has been discovered from recent AD drug studies, memantine may function not only as an antagonist of N-methyl-
Conclusions and Future Directions
Although approximately one-third to one-half of the FTD cases are caused by gene mutations, the exact pathogenesis of the majority FTLD is still unclear. There is currently no evidence-based effective treatment for FTD. The few clinical trials conducted so far had relatively small sample sizes and were rarely controlled studies. Furthermore, the conclusions of drug efficacy drawn from these studies are conflicting. Fortunately, evidence relating to neural and biochemical changes lends support to the investigations of antidepressants and the explorations of other new drugs. Molecular and genetic studies, especially studies targeting tau protein, TDP-43 and FUS, may provide feasible avenues in developing effective treatments or even cure for FTLD. Exploring novel animal models may offer valuable methodologies for further investigations into FTD and challenge current hypotheses. Meanwhile, more large-scale, placebo-controlled trials are needed to explore the efficacy of currently available symptomatic treatments for FTD. If successful, such studies will have the benefit of providing evidence-based clinical treatment recommendations for currently available drugs.
Despite the recent advancements, there are multiple questions that remain unanswered. Is there a common pathophysiologial mechanism that underlies the different forms of hereditary FTLD-U and FTLD-tau? Does the aggregation of 1 protein trigger other disease processes (such as Alzheimer’s disease and Lewy body disorder) with the corresponding protein deposition? Can the development of novel biomarker assays help diagnosis and differential diagnosis of FTD? As our knowledge of FTD develops, clinicians should be aware of the large variation in onset age and the wide clinical spectrum of symptoms. At the same time, a revised clinical criterion based on an international large-scale study is needed. It will be much beneficial if the new clinical criterion can incorporate the pathophysiology and the clinical features of FTD.
Future scientific efforts should emphasize on the 3 key directions. First, explore biomarkers that can be examined in clinical laboratories to support the diagnosis and differential diagnosis of FTD. Second, renew attempts should be made to develop animal models that imitate the progression of FTD, different stages of the disease, and the various spectrums. Finally, based on these efforts in elucidating the pathophysiology, an emphasis must focus on the development of effective therapeutic interventions for FTD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Key Project of the Department of Science and Technology of Zhejiang Province (No. 2007C13053), from the Key Program of Natural Science Foundation of Zhejiang Province (No. Z2100133), and from the Supported by Program for Changjiang Scholars and Innovative Research Team in University (No. IRT1038) to Dr. W.Chen, and the Science and Technology Programme of Hangzhou Municipality (No. 20100633B08) to Dr Y. Shen.