
Abstract
The purpose of this study was to evaluate the deficits of metaphor and sarcasm comprehension in Alzheimer’s disease (AD), as pragmatic interpretation such as metaphor and sarcasm comprehension is required in social communication. A total of 31 young normal controls, 104 aged normal controls (ANC), 42 patients with amnesic mild cognitive impairment (aMCI), and 30 patients with mild AD were evaluated by Metaphoric and Sarcastic Scenario Test, which consists of 5 metaphoric and 5 sarcastic questions with 5 answer choices. Scores were analyzed using the repeated measures analysis of variance (metaphor/sarcasm vs 4 participant groups). Sarcasm comprehension, which requires second-order Theory of Mind (ToM), started to deteriorate in ANC, and metaphor comprehension, which requires first-order ToM, started to deteriorate in aMCI, and both deteriorated as disease progressed. Literal interpretation of pragmatic language is characteristic in patients with mild AD. Such misinterpretation would result in social miscommunication, even if they still retained semantic-lexical competence.
Introduction
Communicative competence occupies a central place in participation in social activities and it can be impaired in patients with Alzheimer’s disease (AD). In AD, lexical-semantic competence is deteriorated as a result of cognitive decline. 1 However, patients could also have communicative difficulties even from the stage where lexical-semantic competence is still preserved. In social communication, literal lexical-semantic comprehension is not sufficient. 2 Comprehension of nonliteral implication is often required to infer a speaker’s intended meaning (Theory of Mind [ToM]), 3 which is not always expressed explicitly.
Theory of Mind is considered to consist of 2 stages, first-order ToM is the ability to grasp the intentions of the speaker and second-order ToM is the ability to infer the speakers’ evaluation for an attributed thought. 4 –7 Metaphor and sarcasm comprehension are considered to be appropriate materials of ToM. 8 First-order ToM is sufficient for metaphor comprehension. 9 Metaphor suggests meanings through mental linkage and comparison of similarities between different expressions normally not related to each other. 10,11 Second-order ToM is required for sarcasm comprehension. 5 Sarcasm expresses something other than explicitly stated and especially the opposite of the literal meaning of the utterance. 12 Thus comprehension of sarcasm requires the ability to reflect on the speakers’ evaluation about the attributed thought, adding to utterance intention. 4
Metaphoric and sarcastic competence has been mainly studied to evaluate the social communicative competence in the phases of development and its disorders, 13 as interaction with other people is critical for normal neurocognitive development. 14 In the phase of aging and degeneration, it is also meaningful to evaluate the decline of social communicative competence. However, a recent review on nonliteral language in AD noted a severe lack of evidence. 15 Furthermore, previous reports on metaphor and sarcasm comprehension are inconsistent; for example, deficits in metaphor comprehension were reported from early stages of AD, 16 –18 whereas concerning irony and sarcasm, previous studies did not find a significant impairment relative to an aged control group, 19,20 which is surprising because irony involves more cognitive processes than metaphor. 21
The controversy could be partly due to the material in the test; it is a prerequisite that difficulty level of lexical-semantic aspects is even among sentences used in the tests. Thus, we conducted the present study to evaluate the deficits of metaphor and sarcasm in AD using a questionnaire that consists of the same type of sentences with similar difficulty levels and whose efficacy was validated for differential diagnosis of developmental disorders in children. 22 For a better understanding of characteristics of AD, error patterns were analyzed. We hypothesized that comprehension might be deteriorated at the early stages of disease and sarcasm comprehension might be deteriorated earlier than metaphor comprehension.
Methods
Participant
The participants were 31 young normal controls (YNC), 104 aged normal controls (ANC), 42 patients with amnesic mild cognitive impairment (aMCI), and 30 patients with mild AD in Clinical Dementia Rating scale (CDR) 1. The YNC were university students and ANC were recruited from community dwellers, who underwent clinical interviews by a clinician who specialized in evaluation of dementia. Patients were recruited from the outpatient clinics. The exclusion criteria were psychiatric diseases and delirium. Verbal incomprehension was also an exclusion criterion. The participants were required to read out the questions and those who lacked fluency were excluded. Concerning language ability, the participants received the Mini-Mental State Examination (MMSE) and were confirmed to have the capacity to name simple objects, repeat phrases, follow written commands, and write a sentence with a noun and a verb. The participants were diagnosed based on the criteria for AD by National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer’s Disease and Related Disorders Association 23 and on the criteria for aMCI by the report of the International Working Group on Mild Cognitive Impairment. 24 Patients with aMCI were limited to those free from objective symptoms of other types of dementia such as dementia with Lewy bodies or frontotemporal dementia. The Ethics Board of the Gunma University School of Health Sciences approved all procedures (No. 21-26), and written informed consent was obtained from all the participants.
Task
Metaphor and sarcasm comprehension was evaluated by the Metaphoric and Sarcastic Scenario Test (MSST), which was developed for discrimination of high functioning pervasive developmental disorders from attention deficit/hyperactivity disorders in young children. 22 This test consists of 5 metaphoric and 5 sarcastic sentences; metaphoric sentences are odd numbered and sarcastic sentences even. The words and sentences in MSST were selected from standard textbooks of Japanese language (Mitsumura Press) for 1st, 2nd, and 3rd grades in elementary school. Therefore, the lexical-semantic components were not above the levels for those who completed 6 years of elementary school education. The test employed a multiple-choice style, that is, 1 choice was correct and 4 were incorrect. The wrong choices included a literal interpretation, an answer associated with part of the sentence, misunderstanding of the sentence, and not knowing. The number of correct answers represented the metaphor score and sarcasm score, respectively. Each pattern of incorrect answers was totaled. Cognitive performance was assessed using MMSE.
Analysis
Group comparison of scores and the 4 error scores were conducted using the repeated measures analysis of variance (metaphor/sarcasm vs 4 participant groups).
Among aged groups, we conducted the repeated measures analysis of covariance (metaphor/sarcasm vs 3 participant groups) with covariates of age, sex, education, and MMSE scores. A post hoc test was conducted with multiple comparisons with Bonferroni correction. All analyses were conducted using the Japanese version of SPSS for Windows version 19.0 (IBM Corporation, New York). Significance was set as P < .05.
Results
Demographic scores are shown in Table 1. The results of the MSST are shown in Table 2 and Figure 1. The main effect indicated that sarcasm was more difficult to comprehend than metaphor (F 1,203 = 54.634, P < .001), and interaction with participant groups was also significant (F 3,203 = 3.354, P = .020). According to within-subject post hoc analysis, no significant difference was observed between metaphor and sarcasm scores in YNC (P = .442), whereas in ANC, aMCI, and mild AD, scores of sarcasm was significantly lower than that of metaphor (P < .001 in all the groups). According to between-subject post hoc analysis, metaphor scores were not different between YNC and ANC, whereas metaphor scores were significantly better in ANC than in aMCI (P = .011) and in aMCI than mild AD (P < .001). Sarcasm scores were significantly better in YNC than in ANC (P = .040), in ANC than in aMCI (P = .005), and in aMCI than in mild AD (P = .002).
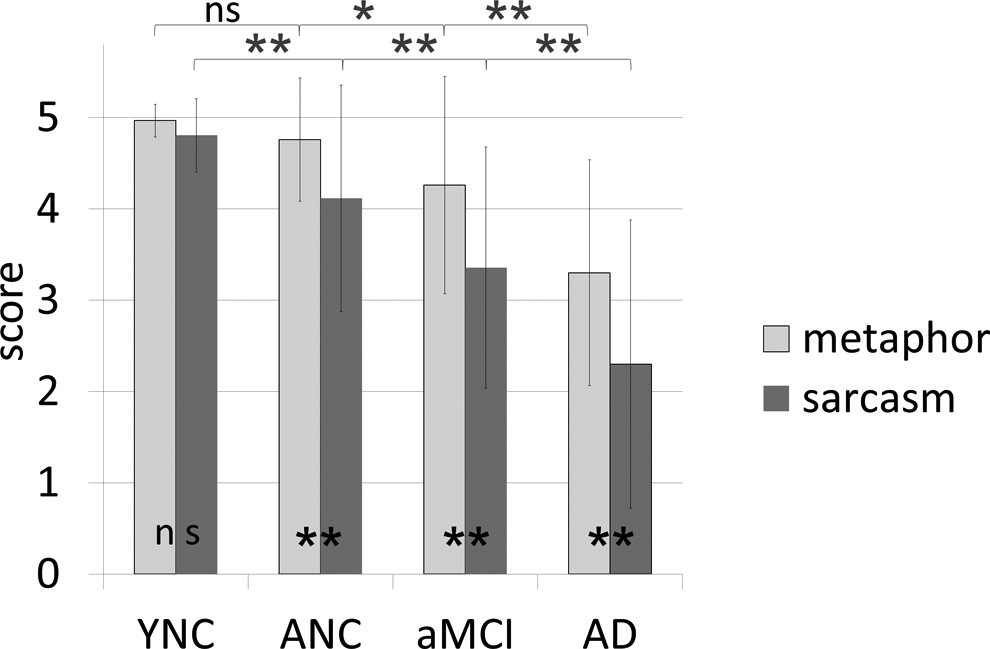
Scores of correct answers. Sarcasm scores were significantly lower in ANC than YNC, whereas metaphor scores were not different between the 2 groups. Metaphor scores were deteriorated from MCI. Post hoc analysis of 2 × 4 analysis of variance (metaphor and sarcasm; 4 groups) was conducted; * in upper row indicates statistical significance of between subject analysis of metaphor, * in middle row indicates that of sarcasm, and * in the bottom row indicates statistical significance calculated by intrasubject analysis. *P < .05, P < .001. YNC indicates young normal controls; ANC, aged normal controls; aMCI, amnestic mild cognitive impairment; AD, patients with mild Alzheimer’s disease in clinical dementia rating 1.
Demographic Data. a
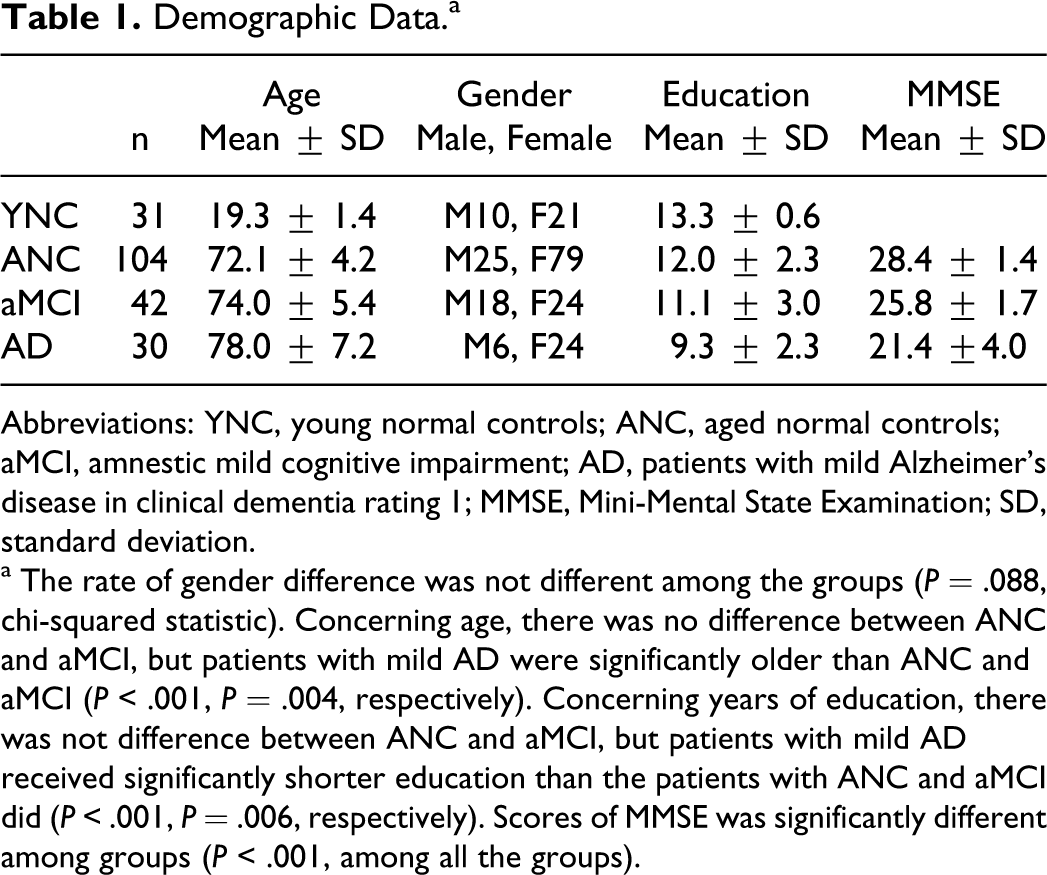
Abbreviations: YNC, young normal controls; ANC, aged normal controls; aMCI, amnestic mild cognitive impairment; AD, patients with mild Alzheimer’s disease in clinical dementia rating 1; MMSE, Mini-Mental State Examination; SD, standard deviation.
a The rate of gender difference was not different among the groups (P = .088, chi-squared statistic). Concerning age, there was no difference between ANC and aMCI, but patients with mild AD were significantly older than ANC and aMCI (P < .001, P = .004, respectively). Concerning years of education, there was not difference between ANC and aMCI, but patients with mild AD received significantly shorter education than the patients with ANC and aMCI did (P < .001, P = .006, respectively). Scores of MMSE was significantly different among groups (P < .001, among all the groups).
Correct Answers.
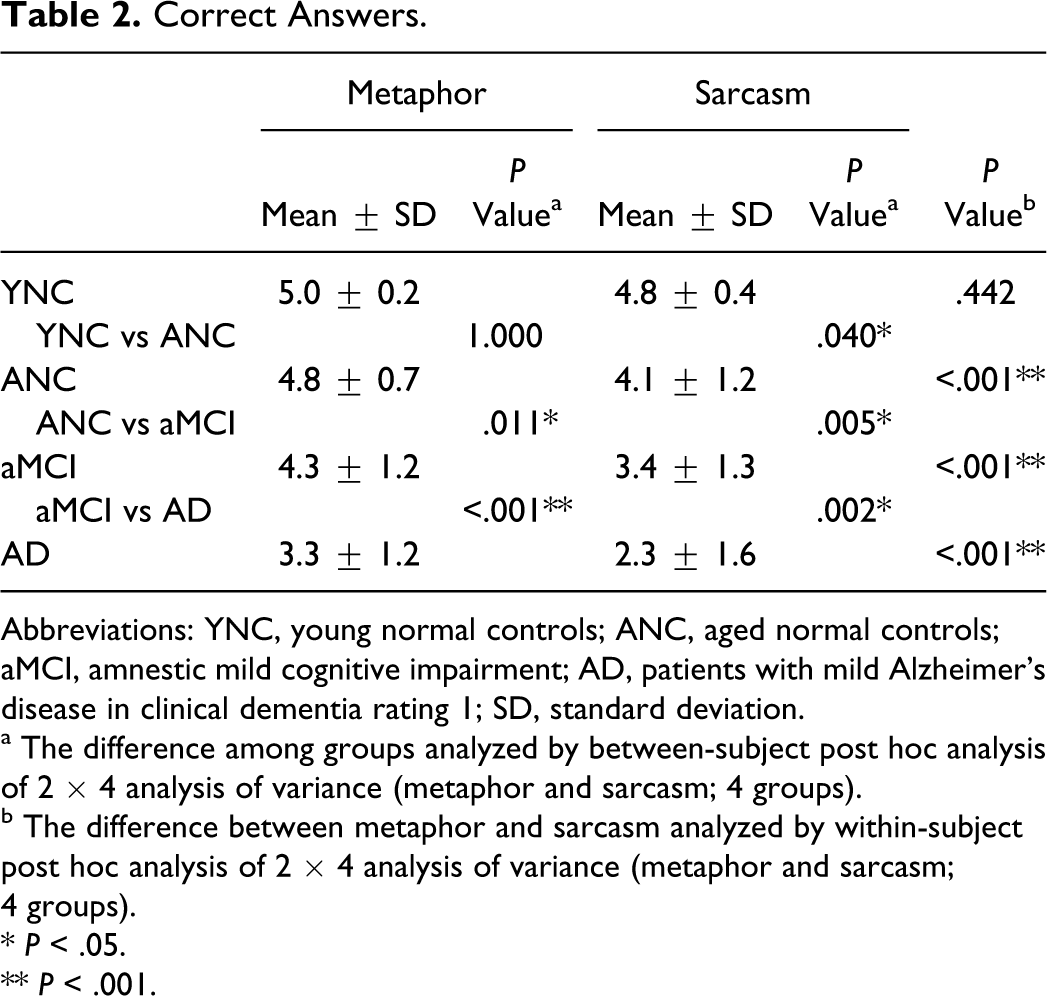
Abbreviations: YNC, young normal controls; ANC, aged normal controls; aMCI, amnestic mild cognitive impairment; AD, patients with mild Alzheimer’s disease in clinical dementia rating 1; SD, standard deviation.
a The difference among groups analyzed by between-subject post hoc analysis of 2 × 4 analysis of variance (metaphor and sarcasm; 4 groups).
b The difference between metaphor and sarcasm analyzed by within-subject post hoc analysis of 2 × 4 analysis of variance (metaphor and sarcasm; 4 groups).
* P < .05.
** P < .001.
Concerning the error patterns, group differences were observed only in literal interpretation and there were no group differences in the other 3 error patterns (an answer associated with a part of the sentence, misunderstanding of the sentence, and not knowing; Table 3, Figure 2). The main effect was significant (F 1,203 = 34.283, P < .001) and interaction was also significant (F 3,203 = 6.887, P < .001). According to the between-subject post hoc analysis, frequency of the errors of literal interpretation of metaphor and sarcasm comprehension were not different between YNC and ANC (P = 1.000 in both), and ANC and aMCI (P = .115, P = .349, respectively), whereas a significant difference was observed between aMCI and mild AD (P < .001 in both). According to within-subject post hoc analysis, the errors of literal interpretation were more in sarcasm than in metaphor in aMCI (P = .038) and in mild AD (P < .001), whereas there was no significant difference in YNC (P = .187) and in ANC (P = .072).
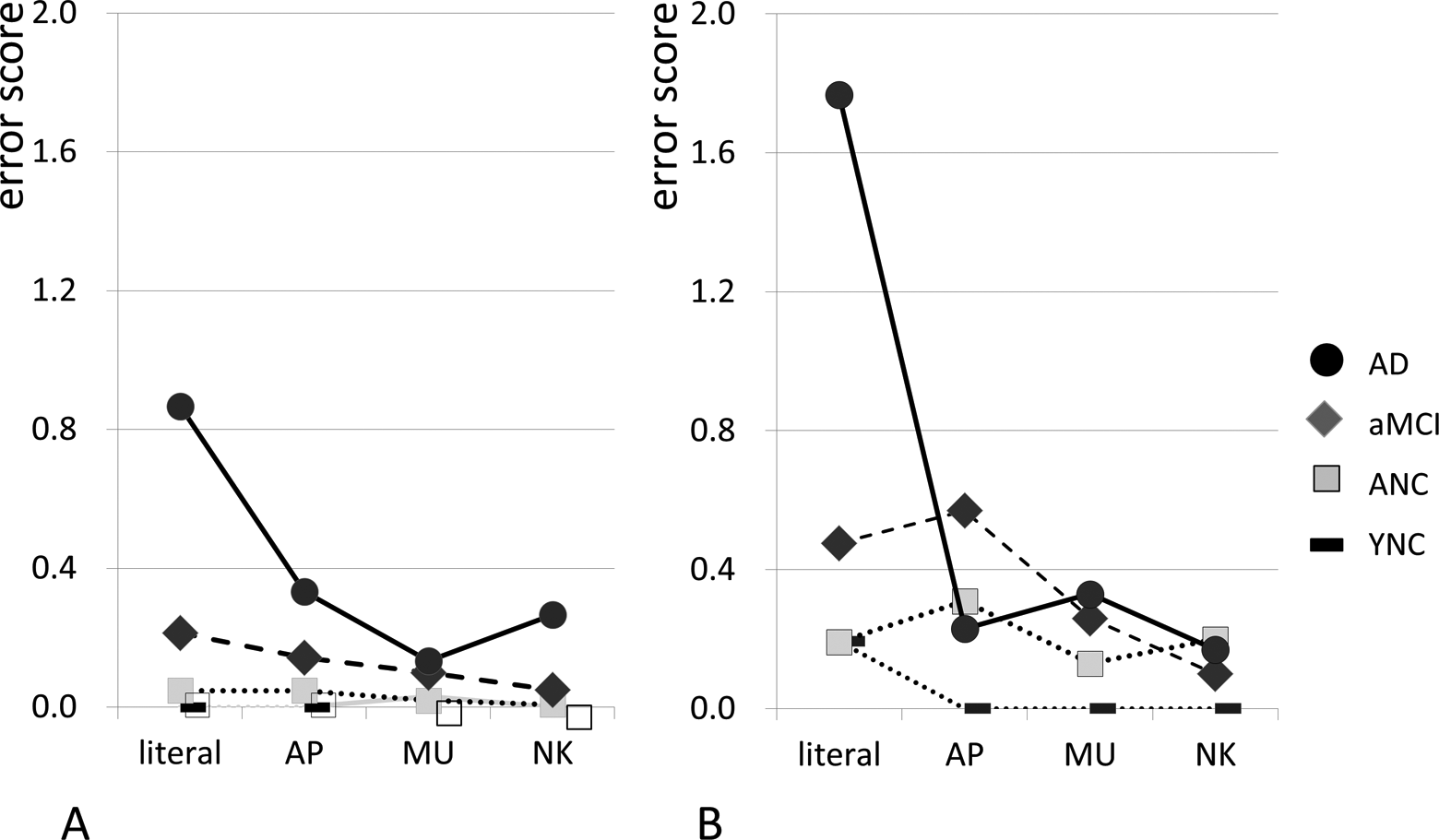
Error patterns. Error patterns of metaphor (A) and sarcasm (B). Significant differences among groups were observed in literal errors in both metaphor and sarcasm and the other 4 patterns of error were not significantly different among groups. AD indicates patients with mild Alzheimer’s disease in clinical dementia rating 1; aMCI, amnestic mild cognitive impairment; ANC, aged normal controls; YNC, young normal controls; literal, literal interpretation; AP, answers associated with part of the sentence; MU, misunderstanding of the sentence; NK, not knowing.
Errors of Literal Answers.
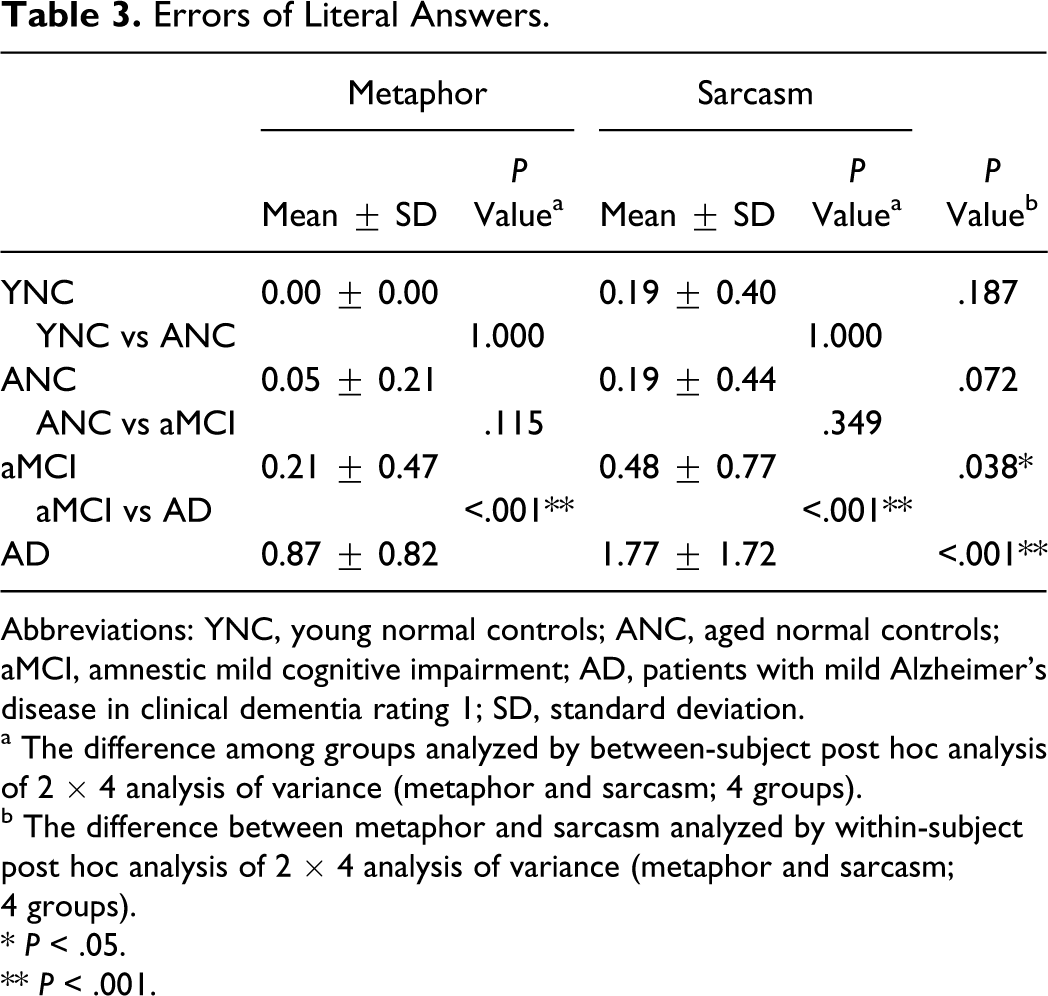
Abbreviations: YNC, young normal controls; ANC, aged normal controls; aMCI, amnestic mild cognitive impairment; AD, patients with mild Alzheimer’s disease in clinical dementia rating 1; SD, standard deviation.
a The difference among groups analyzed by between-subject post hoc analysis of 2 × 4 analysis of variance (metaphor and sarcasm; 4 groups).
b The difference between metaphor and sarcasm analyzed by within-subject post hoc analysis of 2 × 4 analysis of variance (metaphor and sarcasm; 4 groups).
* P < .05.
** P < .001.
There was weak correlation between MMSE scores and metaphor (r = .362 P < .001) and sarcasm scores (r = .337, P < .001).
The difference among the aged groups of ANC, aMCI, and mild AD remained by the repeated measures analysis of covariance with covariates of age, sex, education, and MMSE scores. According to within-subject post hoc analysis, in ANC, aMCI, and mild AD, scores of sarcasm was significantly lower than that of metaphor (P < .001, P < .001, P = .004, respectively). According to between-subject post hoc analysis, metaphor scores were significantly better in ANC than in aMCI (P = .040) and in aMCI than mild AD (P = .002). Sarcasm comprehension was significantly better in ANC than in aMCI (P = .021) and in aMCI than in mild AD (P = .023).
Discussion
Scores for both metaphor and sarcasm were not significantly different from each other in YNC, which confirmed that the difficulty level of metaphor and sarcasm comprehension tested by MSST was not different, at least among young participants.
The result suggested that deterioration of sarcasm comprehension was an age-related change. Sarcasm scores were significantly lower in ANC than in YNC, whereas no difference was observed in metaphor comprehension. Empirical developmental studies of normal children have found that metaphors are comprehended at an earlier age than ironies. 4 One factor critical for understanding verbal irony (sarcasm) is an individual’s ability to attribute appropriate second-order ToM. 4 The success of the second-order ToM task emerges at around age 5 or 6 25 and it has been revealed that age-related decline occurred directly in the second-order ToM and indirectly in the first-order ToM. 26 The influence of difference in difficulty level could not be ruled out. Colston and Gibbs have shown that it takes healthy adults longer to read ironic than metaphoric statements, which suggests that irony (sarcasm) processing requires more cognitive load than metaphor processing. 5
Age-related decline in metaphor comprehension was not shown in the present study. The deterioration was reported in the early stage of AD by a study that did not include the participants with MCI, 16 –18 and the present study showed that comprehension begins to decline even during aMCI, the prodromal stage of AD.
Another issue was with the comprehension of conventional metaphor. In the present study, conventional metaphor comprehension was deteriorated as well as nonconventional novel expressions, as shown in previous studies. 16,17 However, Amanzio et al reported the deficits in nonconventional novel metaphors, while no impairment was observed in conventional metaphors. 18 The study assumed that conventional metaphors might be interpreted automatically through frequent usage, whereas novel metaphors recruited ToM processes. However, the patients might tend to avoid complicated pragmatic wording and without usage in everyday speech, conventional metaphors could recruit ToM processes as novel metaphors.
Deficits of AD were characterized by literal interpretation; concerning error patterns, group differences were observed only in the pattern of literal interpretation. Decline of inhibition could be related to choosing literal interpretation. Metaphor and sarcasm comprehension requires contextual coherence judgment, as literal interpretation can be taken out of context. It has been proposed that both the literal and the nonliteral meaning are activated concurrently and the inappropriate meaning is inhibited by the context. 27 –31 However, patients with AD had difficulty suppressing inappropriate literal interpretation, which is concurrently activated. 32,33 Literal interpretation of metaphor causes misunderstanding and that of sarcasm could be more problematic. In sarcastic expression, the speakers say the opposite of what they mean 15 and thus the patients with AD may interpret the utterance as admiration, which would be opposite to the speakers’ intention. Such misinterpretation would result in social miscommunication.
Miscommunication between patients and caregivers could lead to behavioral and psychological symptoms of dementia (BPSD) in patients and distress in caregivers. 34 –37 Therefore, caregivers’ understanding of decreased communication abilities in patients may reduce BPSD and caregiver distress. 38,39
As a limitation, the groups of the present study were not matched for age and education. Based on the results of the present study, further study is required with a larger group of participants for consideration of clinical relevance.
Footnotes
Acknowledgments
The authors thank all the study participants, Dr Masamitsu Takatama, Geriatrics Research Institute and Hospital, Maebashi, and Rumi Shinohara and Yuko Tsunoda, at the Gunma University, Maebashi, for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Dr Yamaguchi is supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Science, Sports, Culture and Technology, Japan (23300197 and 22650123) and a Grant-in-Aid for Scientific Research (H22-Ninchisho-Ippan-004) from the Ministry of Health, Labor and Welfare, Japan.