
Abstract
Alzheimer's disease (AD) affects the entire family system, including young children. Yet there are few resources to help children understand AD. Storybooks are used to educate children about other diseases and may be useful in AD as well. In this study, we examined the depiction of AD in 33 English-language children’s storybooks written specifically about AD. As a group, storybooks present AD as a brain disease, but provide little information about the diagnostic process or treatments. Clinical presentations are diverse among characters with AD, and no single book presents a comprehensive depiction of the cognitive, behavioral, affective, and functional symptoms of the disease. In fact, the prevalence of some symptoms in this “population” of storybook characters diverges substantially from epidemiological reports. Books designed to familiarize children about AD should be comprehensive and accurate. Current resources, while useful, could be improved to ensure health literacy about AD in young children.
Introduction
With the prevalence of Alzheimer's disease (AD) expected to increase significantly over the next few decades, 1 more young children (ie, age 4-12) are likely to encounter AD in grandparents or great grandparents with the disease or in parents with early-onset AD. 2 -4 Alzheimer's disease can affect young children in several ways. When encountering an individual with AD, children may be confused by behavior that seems odd and inexplicable. When people with AD repeat stories, express paranoid or suspicious beliefs, wander or become agitated, or fail to recognize family members, these symptoms can be upsetting and difficult for children to understand. 5 As a result, children choose to spend less time with older relatives who have AD, 6 experience less emotional intimacy with individuals with AD, 7 and feel embarrassed when explaining a relative’s AD to friends. 8 Alzheimer's disease may also change relationships that children have with other family members, as parents take on more caregiving responsibilities and have less time for their children. 2,9 Indeed, in some families young children may be enlisted to help with caregiving or assume household responsibilities. 10
Fortunately, children’s attitudes toward people with AD can be improved by certain forms of contact with individuals who have dementia. For instance, in several studies, children who attended intergenerational programs with nonrelative individuals with dementia had higher levels of acceptance, more empathy, and more positive attitudes toward individuals with AD. 11 Exposing young children to people with AD can have a positive impact on attitudes and beliefs, yet young children have few opportunities to receive information about AD. A number of respected organizations recommend that parents have candid conversations about AD with their children, discussing its effects on people with the disease and family members as well as the emotions children may experience (eg, Alzheimer’s Association, Alzheimer’s Disease Education and Referral Center). 12,13 However, these organizations provide few specific suggestions about how to talk about AD with young children. Moreover, parents may not initiate conversations about AD because of limited time, low confidence in their own AD knowledge, or because they try to shield young children from information about health and disease. 14 Among the many methods for relaying information to children about AD, storybooks may be an effective way to help parents provide information and initiate conversations about AD.
Bibliotherapy resources for children have addressed many health domains including asthma, 15 physical injury, 16 developmental disability, 17 anesthesia, 18 and death. 19,20 These books provide facts and information about health topics in a relatively nonthreatening format, enabling children to explore the sensitive and emotional topics. 21 In addition, storybooks can help children recognize that they are not alone in their experience and can provide models of behavior that children can apply in their own lives. 22,23 Another benefit is that storybooks can be read at a child’s pace, allowing children and parents to reread and discuss the material as they are ready. Further, they can be reread, thereby reinforcing knowledge over time. Finally, storybooks help parents by providing a structure that can guide difficult conversations with their children.
Despite these potential benefits, for storybooks to be helpful, they need to be comprehensive and accurate in their depiction of AD. The purpose of this study was to undertake a systematic analysis of children’s storybooks about AD, to determine how people with AD are presented and how the disease is depicted, with a particular emphasis on symptom portrayal.
Methods
Materials
Thirty-three children’s storybooks with content related to AD were examined (see Appendix A for a bibliography). Titles were identified by searching key words “Alzheimer's disease,” “dementia,” and “children’s books” in the WorldCat database and the Web sites of 2 major book distributors (Amazon and Barnes & Noble). In addition, books recommended by AD organizations (ie, Alzheimer’s Association, Alzheimer’s Disease Education and Referral Center) were considered. For this analysis, books were included if they were (1) written specifically about AD, as indicated by the book title or a publisher’s book summary that said a character had AD, (2) written in English, (3) available for purchase in the United States, (4) written for a prekindergarten to sixth grade reading level according to the published age range, and (5) illustrated, so as to limit this sample to storybooks and exclude chapter books.
The books in this analysis were published from 1988 to 2009. The reading level ranged from 4 to 12 years and from prekindergarten to sixth grade. Books ranged in length from 11 to 63 pages. Information about the authors was identified from book jackets and a Google search. Authors were diverse in age (range = 9-71) and occupation (48% authors, 27% teachers; other occupations included psychologist, registered nurse, journalist, librarian, marketing executive, stage manager, and translator). While details were rarely available about authors’ experiences with AD, 58% (n = 19) were described as knowing someone with AD.
Coding Procedure
A coding scheme for book content was developed based on a preliminary examination of 5 storybooks and previous research that focused on the depiction of illness, injury, death, and health in children’s books. 16,24 In this article, we focus on the depiction of AD and its symptoms. The list of cognitive symptoms coded in this study was developed based on the criteria for Dementia of the Alzheimer’s Type in the Diagnostic and Statistical Manual of Mental Disorders. 25 The emotional, behavioral, and functional symptoms that were coded were described by the Alzheimer’s Association’s pamphlet, The 10 Warning Signs of Alzheimer’s. 26 In all, 5 coders (4 research assistants and the author E.Y.S.) independently coded all 33 books. One book was used for training purposes. The research assistants and the author (E.Y.S.) compared the results and resolved specific coding discrepancies, which resulted in the consensus data used in this report.
Review of AD Symptom Epidemiology
In order to compare the prevalence of AD symptoms across the storybooks to the prevalence reported in epidemiological studies, we conducted a literature review to establish symptom rates. We searched the PubMed, PsycInfo, and Google Scholar databases for articles published between 1994 and 2012. Key words included “Alzheimer's disease,” “symptom prevalence,” “psychiatric symptoms,” “aphasia,” “apraxia,” “agnosia,” “anger,” “anxiety,” “depression,” “delusions,” “hallucinations,” “sleep disturbances,” “wandering,” “functional impairment,” and “activities of daily living.” Studies were included if the sample consisted of people with Alzheimer’s disease (ie, not other forms of dementia or mild cognitive impairment). Several symptoms described in the epidemiologic literature were not part of the coding scheme and were excluded from this analysis (extrapyramidal symptoms, gait disturbances, myoclonic jerks, personality changes, hyperphagia, and family or marital problems).
Data Analysis
Descriptive statistics were calculated to summarize how AD was portrayed. We considered the characters in the storybooks to represent a “population” of individuals with AD, and we calculated the prevalence of each symptom within that population for comparison with published epidemiological prevalence data. Verbatim quotes were extracted as examples of disease and symptom characterization.
Results
Broad Characterization of the Disease
These storybooks generally portrayed the disorder, which was most often labeled Alzheimer’s disease, as a progressive disorder, caused by changes in the brain, characterized by slow deterioration in several domains of functioning, though with limited mention of treatments or their efficacy. The majority of books (76%) made a point of labeling the main character’s disorder, while the remaining 24% did not. Of the books providing a label for the symptoms, 88% described the main character as having “Alzheimer's disease.” Other less frequent labels included “brain disease,” “memory loss” and being “sick.” A quarter of the books mentioned the diagnostic process in some way, describing that it involved a physician (eg, “Mom said that Grandpa went to the doctor because he kept forgetting things”)27(p10) and several tests (eg, “[The doctors] took blood from Grandma’s arm, took her in for x-rays, and did many other tests”).28(p15) However, detailed information about the diagnostic process was missing from most books. Only a few books (12%) clarified who could get AD (eg, “Kids never get Alzheimer's Disease but many older people do”)29(p3) or addressed communicability (eg, You can’t catch AD like you can catch a cold).30(p25)
An explicit distinction between AD and normal aging was made in only 18% of the books. One maternal character highlighted the difference saying, “Some memory loss is quite normal for older people . . . the doctor decided to give Grandpa lots of tests to find out if his problem was something different.”31(p11-12) When books described what is happening to the person with dementia (PWD), they often relied on simple explanations of changes occurring in the brain. ‘Grandma’s brain is like this,’ she said. ‘Some pieces are lost and will never be found. Other pieces are there, but she can’t fit them into pictures without first finding the missing pieces. Each day, more pieces disappear.’32(p18)
[B]rain cells are tangled up and dying.33(p15)
Alzheimer's disease . . . when the body stays but the mind leaves.34(p23)
It’s like having my mind filled with cobwebs.
29
(p9
)
Some books explained what was going on by highlighting neurological changes and focusing on structures (eg, the brain), whereas others extrapolated those changes to focus on higher order aspects of cognition and thought (eg, the mind). Six books (18%) mentioned treatments but made only oblique reference to their effectiveness (eg, “She was told there were many different medicines and treatments that might help Grandma”28(p17); “Grandpa Dan takes special medicine, and it helps him, but the Alzheimer's still makes him forgetful and confused”).35(p6) A third of the books addressed prognosis in some way, generally portraying AD as a slow deterioration, with a progressive worsening of cognitive and functional symptoms. Grandpa will become more and more forgetful and confused, until one day he won’t remember anything, not even us.
33
(p8
)
Mommy and Daddy said that someday Nana might forget how to do everyday stuff.36(p16)
The doctors tell me that things will get worse over the next few years. Some days will be good, and some days not so good.33(p17)
When her brain no longer sends messages to the rest of her body—like to her heart and her lungs—she will die. Or, she may develop another illness that she can’t handle because her brain isn’t telling her body what to do.
32
(p16
)
In only 3 books was there a clear statement that there was no cure for AD (eg, ‘“Grandma won’t get better,’ Mom warns. ‘Doctors and scientists are trying awfully hard but don’t yet have a cure for Alzheimer's Disease’”).29(p5) Furthermore, only 2 books (6%) provided an estimated life expectancy, and even these were vague. In one book the child was told that the PWD would live “a long time”36(p12) and in another the child’s mother explained that, “Because Grandpa has Alzheimer's disease, [death] may happen sooner than we would expect for a man Grandpa’s age.”33(p30)
Depiction of AD Symptoms
There was wide variability across storybooks in the symptoms presented, ranging from 6 books presenting only 1 to 2 symptoms, to 1 book presenting a character with AD having 15 symptoms. Across all books, the mean number of symptoms was 4.5 (SD = 2.7). As a set, the storybooks described a range of symptoms associated with AD (see Figure 1). Cognitive symptoms appeared most often, with memory deficits depicted in every book. Agnosia, executive dysfunction, and disorientation were the next most common symptoms, though they appeared in only 45% to 58% of books. The most commonly presented behavioral symptoms were wandering, agitation, and sleep disturbance, though again they appeared in few of the books (15% to 18%). Anger/irritability was the most commonly presented affective symptom, appearing in 36% of books; depression and anxiety appeared very infrequently and euphoria not at all. The most commonly presented functional impairments were driving limitations, difficulty toileting, and problems with eating, appearing in 9% to 12% of the books.
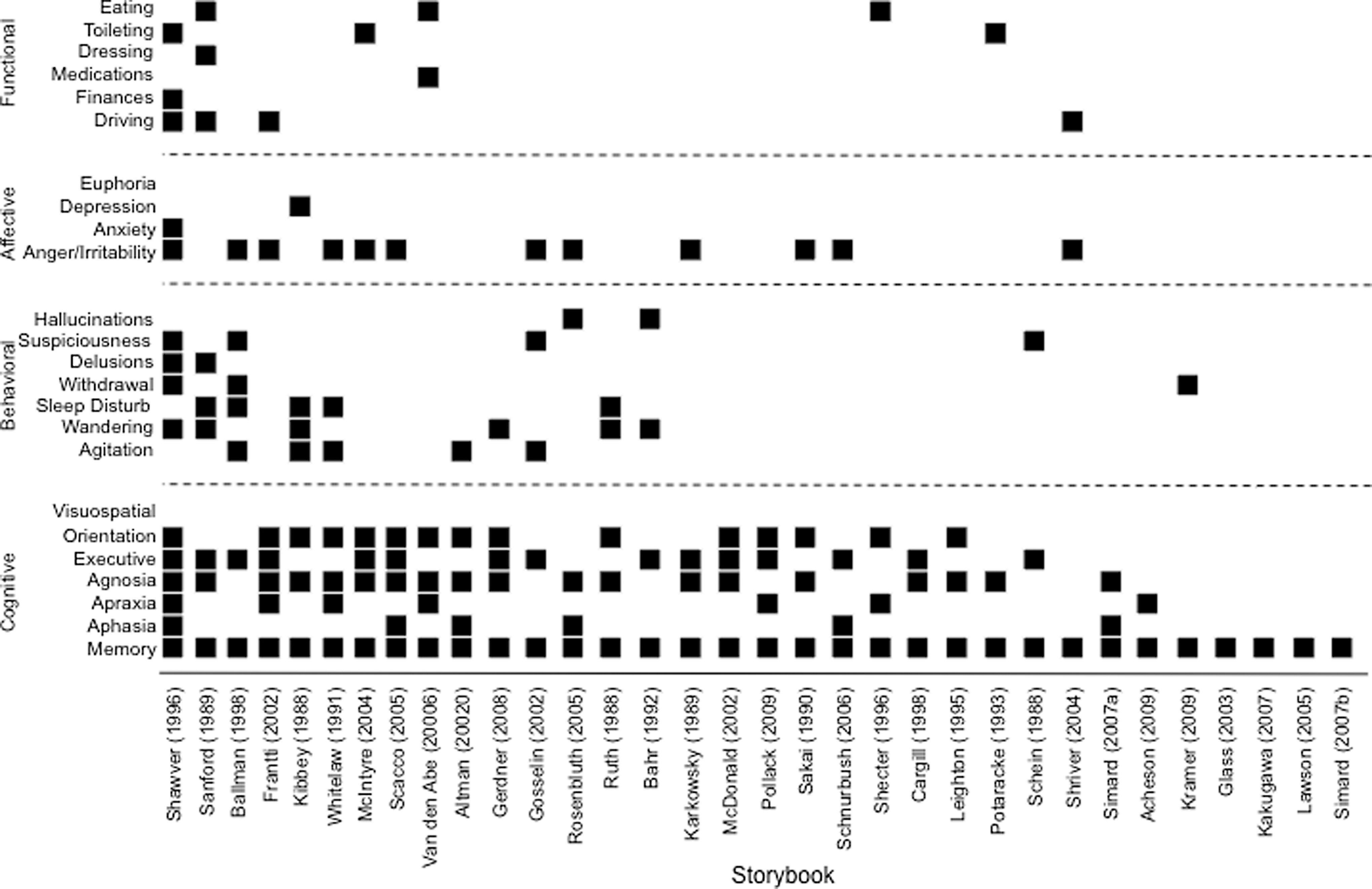
Symptoms appearing in each storybook.
Table 1 includes the prevalence of cognitive, behavioral, emotional, and functional symptoms across this “population” of characters with AD, along with a comparison to the prevalence documented in scientific sources. Across all the storybooks, the prevalence of symptoms was lower than the prevalence suggested by epidemiological studies. Cognitive symptoms were most prevalent in the storybooks, and memory impairment was universal. In contrast, compared with the epidemiologic data, agnosia and executive dysfunction were overrepresented in the storybooks, whereas aphasia and apraxia were underrepresented. We were not able to find comparative information regarding the prevalence of memory impairment (perhaps because of its ubiquity), disorientation, or visuospatial impairment.
Prevalence of AD Symptoms in the “Population” of Storybook Characters Compared to the Prevalence in Published Reports.
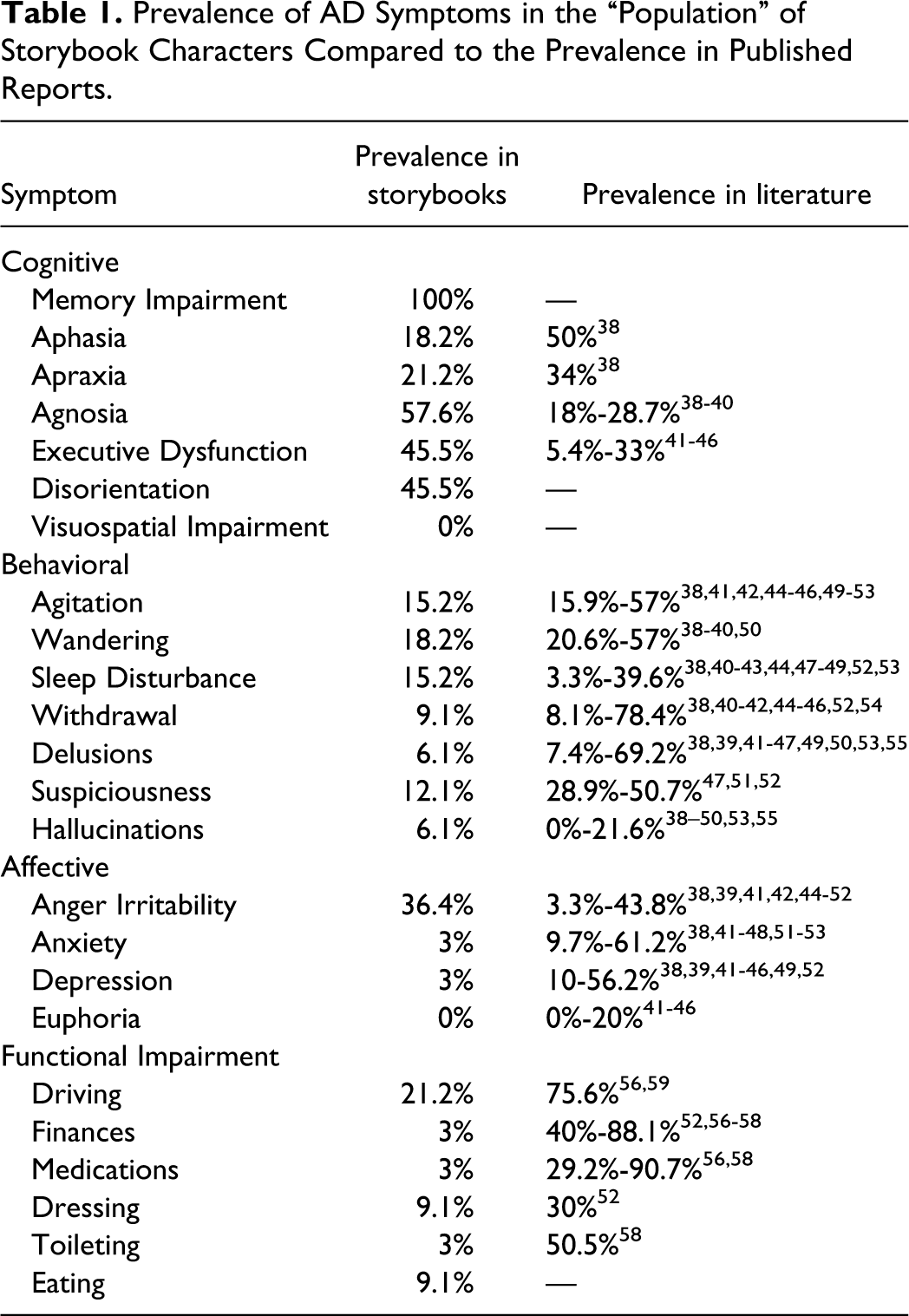
The prevalence of behavioral symptoms in the storybooks was on the low end of the range reported in epidemiological reports. As for affective symptoms, anger/irritability appeared more often in the storybooks than the rates suggested by epidemiological data, and anxiety, depression, and euphoria appeared less often in the storybooks than in actual people with AD. The largest discrepancy was in the area of functional impairment, with impairments less common in the storybooks relative to their actual prevalence. While 24% of the storybooks had characters in residential facilities, these characters were relatively healthy, mobile, verbal, and independent in their activities of daily living. It is worth noting that when diagnostic criteria for AD 37 are applied to storybook characters, 21% of those characters would not qualify for a diagnosis of AD.
Discussion
In this study, we reviewed 33 storybooks designed to familiarize young children with AD. Storybooks that are accurate and comprehensive may be a useful source of information about AD. Our results suggest that, as a group, these books offer a useful introduction to AD, though there is notable variation across books, with some books providing very limited information and others addressing important issues such as etiology, course, and treatment. Most of these books are direct about labeling the disease so that children will become familiar with the term Alzheimer’s disease; this frankness is welcome. However, the books are less clear about differentiating AD from normal aging, a misconception common even among adults. 60 Storybooks that attempt to characterize what is happening in the brain tend to rely on simplified descriptions (eg, “mind filled with cobwebs”), and it is unclear whether this strategy is helpful for children or if it leaves them with misconceptions about the disease. 29 Alzheimer’s disease is, of course, a complicated neurological condition consisting of pathophysiological features well beyond the understanding of most children, and some degree of simplification is necessary. The books also vary in the degree to which they cover the process of diagnosis, available treatments, and other features of the disease that are likely to be on the minds of children (eg, several child characters expressed concerns about whether AD is contagious or heritable).
It would seem useful for storybooks to address the natural history of AD, given its lengthy and progressive course, yet only a few discuss its longitudinal course. Children are likely to observe grandparents with AD change slowly over several years, and storybooks might help them prepare for the progressive nature of the disease and its symptoms, even though young children’s conception of the passage of time may differ from adults’. If the average number of years between diagnosis and death in AD is anywhere from 3 to 10 years, 61,62 young children could spend a substantial portion of their early life witnessing how AD unfolds over time.
Across the books, cognitive symptoms are commonly presented, whereas behavioral and affective symptoms and functional impairments are depicted less often. This seems consistent with the general public’s perception that the cardinal symptoms of AD are confusion, poor memory, wandering, and difficulty with activities of daily living. 63 Further, the universal inclusion of memory impairment in these storybooks reflects the diagnostic criteria at the time. However, this leaves readers of these storybooks relatively uninformed about other common symptoms, particularly neuropsychiatric disruption and functional impairment. There are several reasons why storybook authors might not address these complex symptoms. First, the authors themselves have a range of experience with AD, and they may construct characters based on limited personal experience rather than a broad, professional understanding of symptoms. Second, certain symptoms may be easier to depict in a storybook. For example, word-finding difficulties can be portrayed by showing a person with dementia struggling to name an object or recall a person’s name, whereas anxiety, withdrawal, and incontinence may be more challenging to depict. Third, authors may try not to frighten children by avoiding more severe symptoms such as aggressiveness, hallucinations, suspiciousness, or extreme dependency. Indeed, the few characters portrayed in a residential care facility were relatively healthy and end-stage dementia was missing entirely. While these storybooks protect children from the more grim images of advanced disease, the consequence is that children may not learn about what truly happens in AD until they witness it in their own family.
In this sample of storybooks, the prototypical person with AD has a memory impairment accompanied by agnosia and executive dysfunction, is disoriented to person and place, is prone to wander from home, experiences some mild agitation and disrupted sleep, and has angry outbursts from time to time. However, most of the books (1) lack a full range of symptoms that (2) exert an influence over many domains of life, and that (3) evolve and progress with time. Of course, any actual person with dementia will not experience every potential symptom, so a storybook character who has every symptom would be just as unrealistic as a character with 1 to 2 symptoms. Nonetheless, depending on the book, children may receive a limited presentation of what happens to a person when she has AD and how that person may change over time. In addition, overlooking the difference between normal aging and dementia-related disease could reinforce inappropriate stereotypes of all older adults. Authors no doubt balance realism with a consideration for what is developmentally appropriate material for young readers. If this delicate balance is achieved, storybooks may introduce children to important concepts about AD, prepare them for changes they may observe in real people with AD, and facilitate children’s adjustment to these changes.
To our knowledge this is only the second study to examine a collection of contemporary storybooks about AD. 4 Despite the breadth of this review, several limitations should be noted. First, we did not include the examination of storybook illustrations in this analysis as the illustrations generally did not depict AD symptoms. Second, storybooks that focus on a disease have several goals they must balance: providing information about the condition, responding to the likely concerns of their young readers, and developing a narrative that is appealing and engaging. All of these goals must be accomplished within the format of a relatively short book that must capture and hold a young child’s attention. Therefore, it may be unrealistic to expect storybooks to be the one and only source of complete information about AD. In our critique, we were examining the accuracy and comprehensiveness of the books, with less regard for the other demands of the genre. In addition, in our comparison of symptom “prevalence” in the books with actual epidemiological data, parallels between symptoms were not always direct. For instance, “confusion” appears as a symptom in many epidemiological studies but without clear definition, so comparison with confusion in the storybook characters may be flawed. And again, it may not be reasonable to hold storybooks to the same educational standards as other sources of information, such as brochures or Web sites.
Despite these limitations, our analysis has provided a summary of contemporary storybooks and highlighted several weaknesses in their content. Storybooks have the potential to be an important educational resource. They can help parents find a way to introduce the topic of dementia to their children, and they can provide children with an introduction to the disease. Moreover, storybooks can provide information well beyond symptoms, by addressing the emotional and social challenges children may face when a family member has AD. Future research could take a two-pronged approach. First, research could systematically examine what content is essential for a comprehensive storybook about AD by asking children about their preconceptions of the disease. Second, research could examine what children learn from these storybooks and how they might be used by parents most effectively to help children understand AD. The development of AD resources for children of all ages may be particularly beneficial as more young children experience AD in their own lives.
Footnotes
Appendix A
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.