
Abstract
Background/rationale:
The identification of Alzheimer’s Disease (AD), the emotional reactions, and the perceived threat to AD were compared across 3 Greek samples: 147 primary care health professionals (PCHPs), 74 health and social service graduate students, and 99 laypersons. Within the group of PCHPs, physicians, nurses, and social workers were compared. The factors associated with emotional reactions were examined. Finally, the Emotional Reactions Scale’s (ERS) latent structure was validated.
Methods:
The participants were asked to identify the disease of a vignette, respond to the ERS and in 3 indices of perceived threat.
Results:
The PCHPs identified AD equally accurate to laypersons. Students and laypersons reported the most intense emotions. Social workers perceived higher consequences than physicians and nurses. Age, personal experience, education, and perceived concern predicted emotional reactions.
Conclusions:
Findings underscore the importance of implementing education and training actions to increase AD identification, reduce negative emotions, and further advance care for patients.
Keywords
Introduction
The study compares the identification of Alzheimer’s disease (AD), the emotional reactions to AD, and the perceived threat of developing AD within 3 groups: (i) primary care health professionals (PCHPs), namely, those working in a primary care setting as part of a multidisciplinary team (eg, physicians, nurses, and social workers), (ii) health and social service students (ie, nursing and social work students), and (iii) laypersons from the community. It must be stressed that we refer to identification in terms of the designation of a disease to a vignette rather than a formal diagnosis carried out only by the professionals. Secondary aims were the examination of the predictors of the emotional reactions and the validation of the factor structure of the ERS.
Findings suggest that the majority of the laypersons believed that they were not very knowledgeable about AD, 1 whereas family physicians were found to lack diagnostic accuracy particularly about mild dementia. 2 Other studies have shown that the majority of the laypersons 3 and family physicians 4 correctly recognized nearly all AD symptoms to be warning signs of the disease. Professionals working with the patients with dementia were the most knowledgeable about AD, caregivers and older adults followed, and undergraduate students were the least knowledgeable. 5 In line with this result, caregivers (eg, professional or family) have been found to be more knowledgeable about AD than noncaregivers, probably because of their experience with the disease. 6,7 Using the vignette methodology, the majority of the 70 Greek laypersons from the community identified dementia in general and nearly half of the participants identified AD in specific. 8 In another Greek study, physicians have reported that AD is underdiagnosed or misdiagnosed and general public have admitted difficulties in recognizing the early signs of AD. 9 Mental health professionals are more knowledgeable about age-related cognitive changes than psychology students. 10 The PCHPs are those who essentially care within primary settings for elderly people suffering from a developing dementia. Notwithstanding the importance, little is known about whether PCHPs and students aspiring to work in primary sector accurately identify AD. Both PCHPs and specialists (ie, neurologists/psychiatrists) have reported to be qualified to diagnose dementia, with specialists reporting being more competent. 11,12 Studies have shown that medical students 13 and health and social graduate students from disciplines of social work, nursing, occupational therapy, and medicine 14 had fair knowledge about dementia. To the authors’ knowledge, no study has examined AD identification across multiple samples such as PCHPs, health and social service students, and laypersons. However, early detection of the AD symptoms may result in adequate help-seeking behaviors by laypersons, timely diagnosis by professionals, and may optimize the quality of care for the patients. 15,16
Information about the reactions to people with AD can help implement interventions that focus on reducing the stigmatization associated with the disease. Several studies have documented laypersons’ emotional reactions toward individuals diagnosed with AD across different cultures. Responding to the Emotional Reactions Scale (ERS), Jewish Israeli, 17 Israeli Arabs, 18 and Greek laypersons 8 have been found to express highly positive emotions and low negative emotions toward an individual with AD. Israeli family physicians have reported significantly higher levels of positive emotions than negative toward the patients with AD. 19 Similar results have been reported in Israeli psychiatrists. 20 Interestingly, PCHPs’ emotional reactions toward AD have received far less attention. The students’ emotional reactions have also received scant attention. Beck 21 examined the emotions of nursing students while caring for cognitively impaired elders. They reported to experience a variety of negative feelings and also empathy toward the patients with dementia. Other findings have shown undergraduate students expressing more compassionate emotions toward a patient with AD. 22 Another aim of the present study was to validate the factor structure of the ERS. Contrary to studies that have shown either 4 factors accounting for the 16 items of the ERS 17 or 3 factors accounting for 9 items of the ERS, 19,20 a Greek study 8 has revealed 5 factors. It was deemed imperative to validate a measure in Greek for assessing emotional reactions toward a patient with AD, as no such measure currently exists. 23
A concept that is closely related to emotional reactions is personal experience with AD. Studies have shown that contact positively affects laypersons’ perceptions of the elderly people. 24,25 It has been shown that psychiatrists’ familiarity with a person with AD is associated with decreased negative feelings. 20 Another study has shown that undergraduate psychology students’ close contact with a person with AD results in intense empathy feelings. 26
Of great interest is the possible influence of cognitive factors in one’s emotional reactions. Perceptions about the susceptibility of developing AD, attribution of dangerousness, 18,27 and responsibility of the person with AD 4,19 all have been associated with higher levels of negative emotions toward the person with AD. There is evidence of a significant positive association between perceived threat and laypersons’ emotional reactions. 17 In a Greek study, perceived threats were found to affect layperson’s emotional reactions toward the individual diagnosed with AD. 8 The participants with continuous concerns about the likelihood of developing AD expressed more rejection feelings. Those with greater anxiety toward the threat of AD expressed more social feelings and those with greater perceived susceptibility expressed more aggressive feelings toward the individual diagnosed with AD. Our study will examine rates of perceived threat and also correlates with emotional reactions to all 3 sampling groups. Results from a review 1 indicated that the percentage of laypersons’ concern about developing AD ranges from 26% to 49%. The majority of Greek laypersons (72%-77%) reported that they had never felt any threats about developing AD. 8 To the authors’ knowledge, no study has reported rates of perceived threat in other groups, such as PCHPs or students.
Only 1 Greek study of the identification of AD, emotional reactions, and perceived threat toward individuals diagnosed with AD has been conducted. 8 The findings, though not yet published, have been reported in this review. However, this study was conducted solely with laypersons. The present study will carry these explorations a stage further by examining the disease identification, emotional reactions, and cognitive perceptions of AD across a range of samples, especially those who come into contact with elderly people and/or with individuals with AD, such as PCHPs. For the sake of primary prevention, health and social service graduate students were included and compared with PCHPs and laypersons. Academic education emphasizing dementia to students in these disciplines who are likely to work with elderly people is a priority for primary prevention in order to create a competent workforce in dementia care services. The study was repeated within a subsample of physicians, nurses, and social workers.
In line with previous findings, 8,17 it was hypothesized that overall the samples (a) would accurately identify AD, (b) would report more positive and less negative emotions toward an individual diagnosed with AD, and (c) would perceive low threats about developing AD. As a result of both formal training and frequent professional interaction with patients with AD, 5 it was further anticipated that the PCHPs would be the most accurate in identifying AD and express the most positive and the least negative emotions; the students would follow and the layperson would come last. Within the group of PCHPs, compared to nurses and physicians, social workers were expected to be less accurate in identifying AD, expressing more positive emotions toward an individual with AD and perceiving lower threats about developing AD, as a result of their academic training oriented to social care. Social workers have a psychosocial perspective, with a broadened view of health and a focus on the social determinants of health, whereas physicians and nurses are medically trained and their approach is a narrow biomedical one to physical illness. 16 , 28
A secondary aim was to examine the correlation of the emotional reactions with cognitive determinants (disease identification and perceptions of threat of AD), personal experience with AD, and sociodemographic characteristics. Positive emotions to a high extent and negative emotions to a low extent were anticipated by those who would be more accurate in identifying AD compared to those who would be less accurate in identifying AD. Those with personal experience with an AD person, 20,23,27 those reporting lower threats about developing AD, 8,17 the women, 8,17 the more educated, 18 and the older participants 8,17,29 were also expected to express more positive emotions compared to those without personal experience with a patient with AD, those reporting perceptions of higher threat, the men, the less educated, and the younger participants, respectively. Finally, based on inconclusive findings 8,17,19,20 of the latent structure of the ERS, a final aim of the study was to test its factorial validity in the Greek sample. The findings of this study hopefully will help the identification of areas for potential intervention, such as the development of strategies for those at risk for advancing AD identification, minimizing negative reactions, and perceptions about AD, which will further result in improved care for the patients and their families.
Methods
Sample
Three convenience samples, all residents of the island of Crete, Greece were recruited: 147 PCHPs (32.0% men and 68.0% women), 74 graduate students (14.9% men and 85.1% women) enrolled in the Health and Social Welfare School of the Technological Education Institute of Crete, and 99 laypersons from the community (49.5% men and 50.5% women). The PCHPs were recruited from 17 primary care centers located in the 4 regions of Crete. They were physicians (40.8%), nurses (23.8%), midwives (9.5%), and social workers (8.8%). The majority of the PCHPs (63.3%) reported to provide services to elderly people and patients with dementia, with no relevant education (78.2%), though. The students were recruited to be all seniors, so as to compare in academic training with the PCHPs. Of the students, 47.3% had personal experience with a patient with AD, who was a relative (62.9%) or an acquaintance (37.1%). The laypersons were employees in private sector (33.3%) or had other nonscientific position (57.6%). Laypersons had personal experience with a person with AD (47.5%), who was an acquaintance, a relative (43.9% each), or a friend (12.9%). In general, significantly more women (74.4%) than men (25.6%) had experience with a person with AD (χ 2 (1) = 5.66, P = .013). Participants’ sociodemographic and health characteristics are presented in Table 1.
Participants’ Characteristics
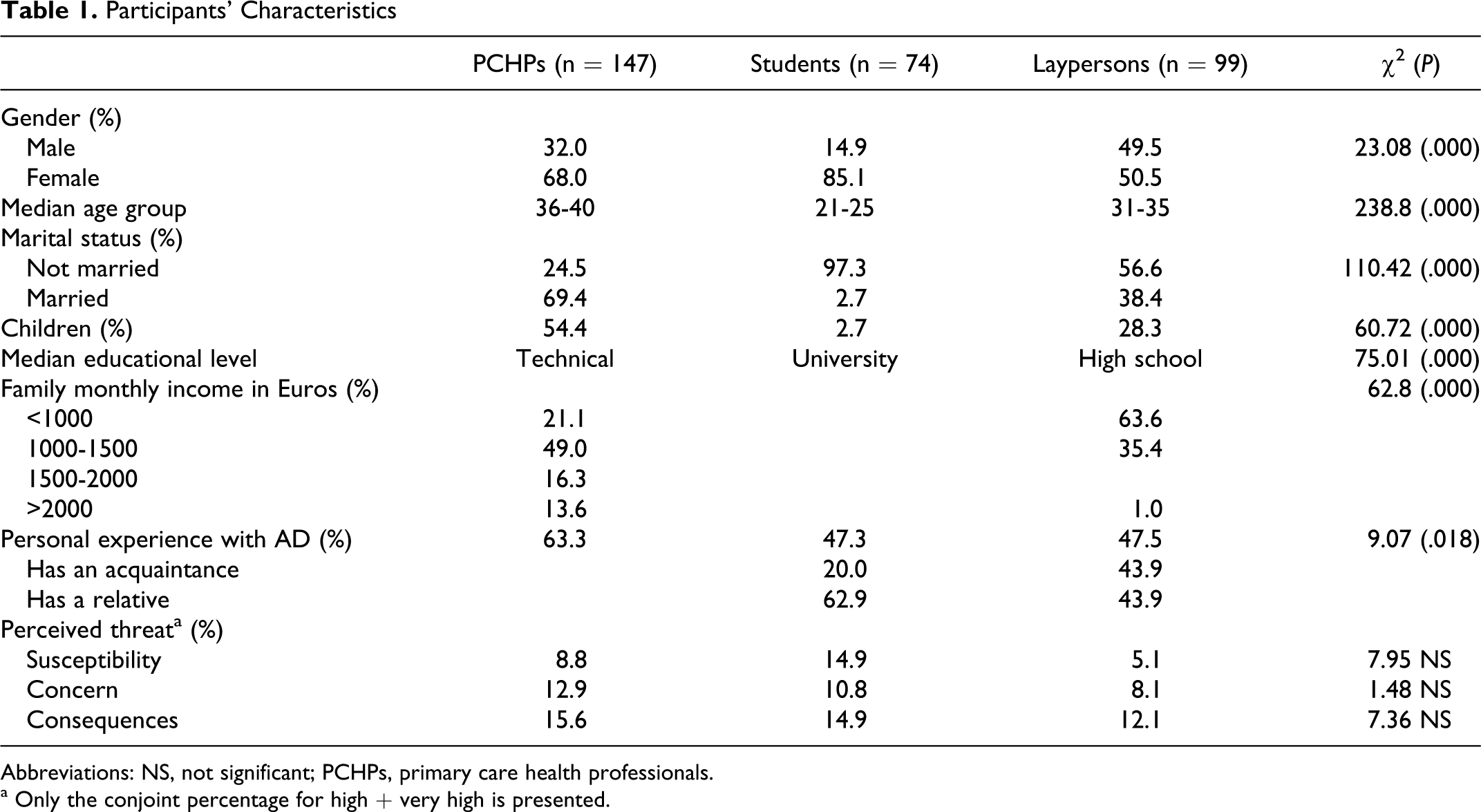
Abbreviations: NS, not significant; PCHPs, primary care health professionals.
a Only the conjoint percentage for high + very high is presented.
Measures and Procedures
Disease identification
Participants were presented with a vignette, slightly modified from that created by previous studies, 8,17 describing a person with a moderate level of AD impairment according to the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) criteria (see Appendix A). Using an open question, participants were asked to identify the disease from which they believed that the person was suffering.
Emotional reactions
Participants were asked to indicate their emotional reactions to the person described in the vignette using the ERS. 17 The ERS consists of 16 items allocated in 4 subscales. 17 A typical item of each subscale is Rejection: disgust; Anxiety: uneasiness; Prosocial: sympathy; Aggressive: anger. Each item was rated on a 5-point Likert-type scale, ranging from 0 (not at all) to 4 (extremely). Higher scores represented higher engagement with each emotion. The maximum score for the entire questionnaire is 64. Acceptable alpha reliability coefficients have been reported 27 : Rejection .61; Anxiety .77; Prosocial .72; Aggressive .71. The ERS was translated to Greek by an English-speaking health professional and it was back-translated by an independent translator. Two bilingual experts compared both the English and the Greek versions and finally a Greek translation was agreed upon. The validity of the vignette was examined by giving it to 5 experts in the field of dementia and asking them to give a blind diagnosis. The AD diagnosis was given by all experts.
Perceived threat about developing AD
Participants were asked to report their perceptions regarding the likelihood of developing AD using 3 items (i) how likely they felt they would develop AD at some point in their lifetime (perceived likelihood/susceptibility); (ii) how concerned they were about developing AD at some point in their lifetime (perceived concern); and (iii) how emotionally stressful they believed AD would be should they develop it (perceived consequences). Each item was rated on a 5-point Likert-type scale, ranging from 1 (not at all) to 5 (very much). Higher scores indicated perceptions of greater threat.
Other measures
Participants’ background characteristics included (a) sociodemographic characteristics (eg, gender and age) and (b) personal experience with AD (whether they know someone who had been diagnosed with AD).
Data Analysis
All statistical analyses, but confirmatory factor analysis (CFA), were conducted with the SPSS 17.0. A CFA was conducted, using Analysis of Moment Structures 6 (AMOS 6), to confirm the underlying structure of the ERS and Cronbach’s α coefficients were produced to test the subscales’ reliability.
Results
Identification of AD
The majority (62.2%) of the participants in all groups identified AD accurately. Significantly more laypersons (71.7%) than PCHPs (61.2%) and students (51.4%) identified AD (χ 2 = 7.58, P = .023). To rule out potential confounders, a logistic regression analysis was conducted on identification as outcome, with gender, age group, educational level, personal experience, and perceived threats entered as predictors. A test of the full model predicted identification (Omnibus chi-square=24.05, df = 11, P = .013). The model accounted for between 7.3% and 10% of the variance. Overall 65.7% of the predictions were accurate. Group was the only significant predictor of identification (P = .001). Students were 3.39 more likely to identify a disease other than AD (95% confidence interval 1.55 and 7.38; Wald test =.869, df = 1, P = .002) compared to PCHPs.
Emotional Reactions
Factor structure of the ERS
Previous studies, all using an exploratory factor analysis (EFA), have proposed either a 4-factor structure for the English ERS 17 or a 5-factor structure for its Greek translation. 8 A CFA was conducted to determine which of the 2 alternative models fit the data. The following goodness-of-fit measures were used: the χ 2 /degrees of freedom ratio (CMIN/DF) below 3, the standardized root mean square residual between 0.5 and 0.10, the goodness-of-fit index and the comparative fit index above 0.90, and the root mean square error of approximation between 0.05 and 0.08. The Consistent Akaike’s Information Criterion and the Expected Cross-Validation Index were used in the comparison of the models; the smaller the values the better fit.
From Table 2 it can be seen that, although the indices for the estimation of the 5-factor model were not very good, they yielded a better fit than the 4-factor model. The examination of the Modification Indices for both models revealed that there were misspecified error covariances between items, which were consecutively added to the respecification of the subsequent models (see Table 2). The Model II.2 was considered to represent the best fitting to represent the data. The 5 factors are social (concern, compassion, desire to help, and sympathy), aggression (irritation, ridicule, disgust, anger, and rejection), anxiety (fear, uneasiness, and insecurity), acceptance (consternation and embarrassment), and rejection (impatient and discouragement). The maximum score for each subscale is social: 16; aggression: 20; anxiety: 12; acceptance: 8; and rejection: 8.
Summary Goodness-of-Fit Statistics in Determination of the Models
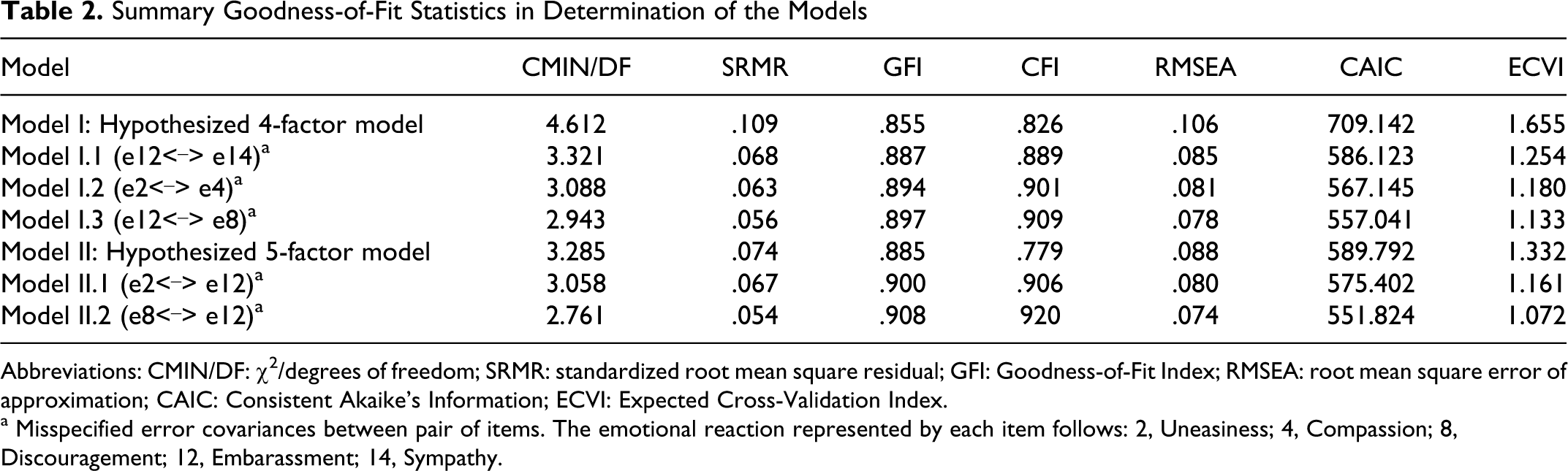
Abbreviations: CMIN/DF: χ 2 /degrees of freedom; SRMR: standardized root mean square residual; GFI: Goodness-of-Fit Index; RMSEA: root mean square error of approximation; CAIC: Consistent Akaike’s Information; ECVI: Expected Cross-Validation Index.
a Misspecified error covariances between pair of items. The emotional reaction represented by each item follows: 2, Uneasiness; 4, Compassion; 8, Discouragement; 12, Embarassment; 14, Sympathy.
Reliability coefficients of the ERS
The reliability of the overall scale was acceptable for the PCHPs (.68), the students (.79), and the laypersons (.65). Considering the overall sample, the alpha coefficients were good for the subscales social (.78) and aggression (.85), acceptable for the anxiety subscale (.67), and low for the acceptance (.46) and rejection subscales (.47). There were considerable subscale variations between the samples, with the alphas ranging from .42 to .79 for the laypersons in the rejection and social subscales, respectively.
Emotional reactions to an individual diagnosed with AD
The participants’ reactions to the person described in the vignette in each of the 16 emotions are presented in Table 3. As can be seen, the participants reported positive emotions to a high extent and negative emotions to a low extent. The differences between the samples were significant. Although the students reported significantly more negative emotions (total scale score: 19.9) than laypersons (9.4) and PCHPs (7.7; F 2 = 148.09, P = .000), they also expressed significantly more positive emotions (total scale score: 13.6) compared to laypersons (9.9) and PCHPs (9.7) (F 2 = 54.16, P = .000). No pairwise differences between laypersons and PCHPs were observed. An item-by-item comparison indicated that there were significant differences across the samples in all feelings but disgust. Uneasiness, insecurity, embarrassment, and discouragement were the most highly reported emotions for both students and PCHPs; students also expressed impatience. The most highly reported emotions for laypersons were uneasiness and embarrassment.
Emotional Reactions to a Person Suffering From AD Across the 3 Samples
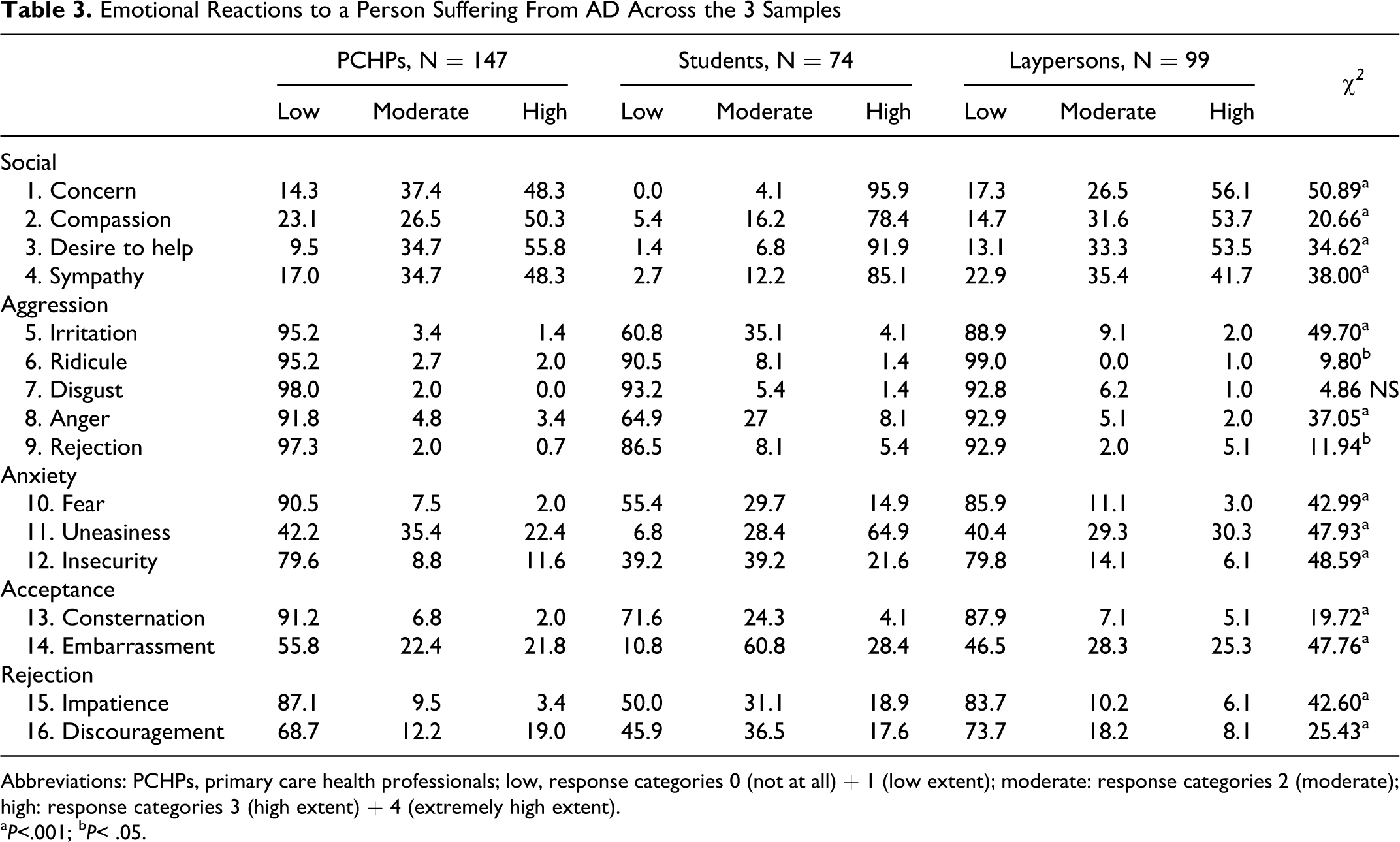
Abbreviations: PCHPs, primary care health professionals; low, response categories 0 (not at all) + 1 (low extent); moderate: response categories 2 (moderate);
high: response categories 3 (high extent) + 4 (extremely high extent). a P<.001; b P< .05.
Group differences as a function of covariates
We further examined whether emotional reactions (ie, prosocial, aggression, anxiety, acceptance, and rejection) differed by group, while controlling for covariates (gender, age group, educational level, disease identification, personal experience, and perceived threat). The MANCOVA revealed a significant multivariate main effect (Wilks’s λ = 0.328, F 10,600 = 44.780, P = .000, partial η 2 = .427, power = 1.000). Significant univariate effects were found for all emotions, with PCHPs expressing the lowest mean scores compared to the students and laypersons (Table 4). No pairwise differences between students and laypersons were found.
Subscales’ Mean Scores Across the 3 Samples
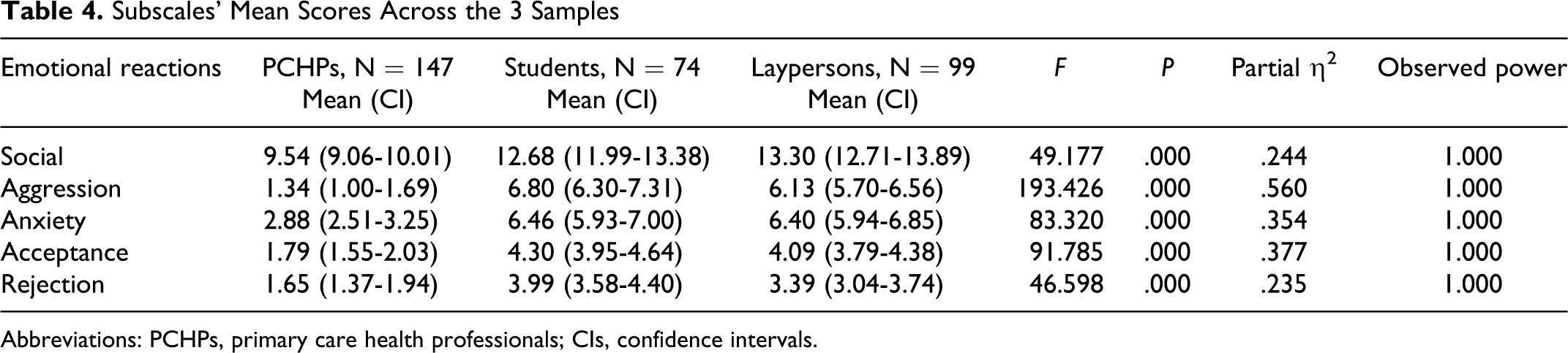
Abbreviations: PCHPs, primary care health professionals; CIs, confidence intervals.
Variables associated with emotional reactions
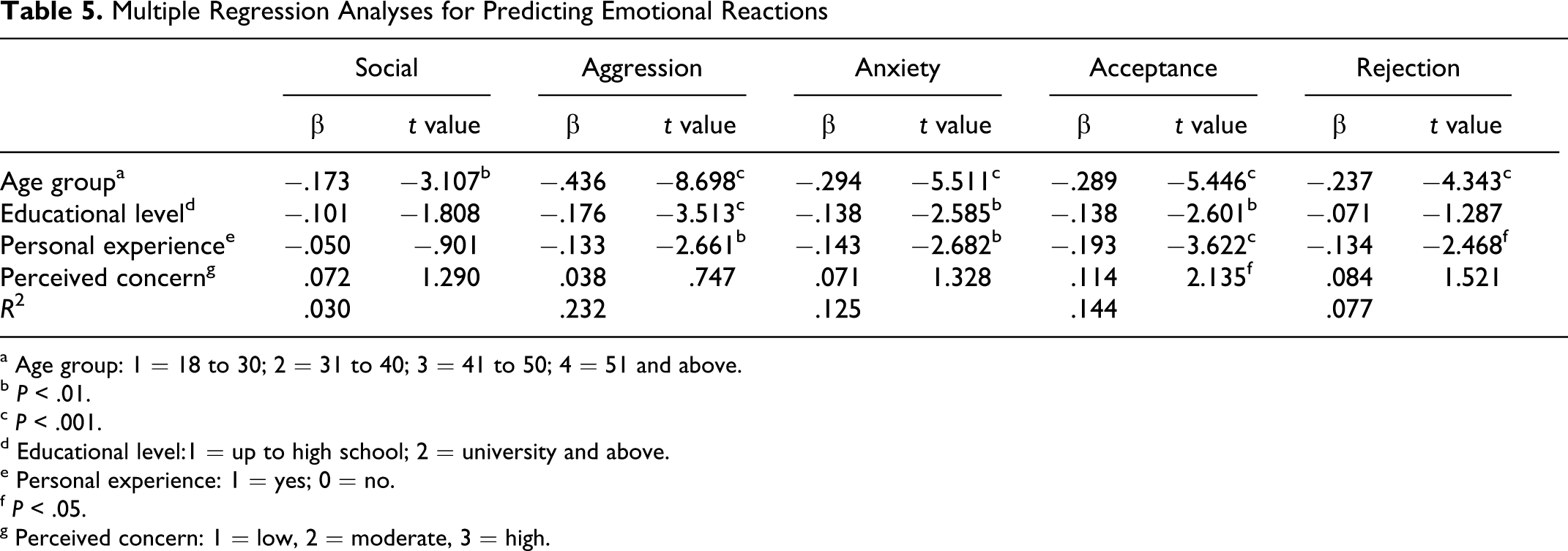
Separate multiple regressions, using the stepwise method, were conducted for each ERS subscale. Initially, the independent variables were sampling group, gender, age group, educational level, personal experience with AD, disease identification, and the 3 indices of the perceived threat. The most significant predictor in all equations was group, with the PCHPs expressing less intense emotions than the students and laypersons. The models explained 20.5% to 54.3% of the emotional reactions. Because this finding was anticipated given the MANCOVA results, the analyses were repeated with group subsequently being excluded from the predictors. In Table 5 the standardized β coefficients and t scores of the variables that were statistically significant in at least one of the equations are presented. Age was associated with all emotions in a low degree. Personal experience was associated with all emotions in a low degree, except social feelings. Educational level was associated with lower aggression, anxiety, and acceptance, and perceived concern was associated only with higher acceptance. The models explained 3% to 23.3% of the emotional reactions. Gender, disease identification, perceived likelihood, and perceived consequences were not significantly associated with the emotional reactions.
Multiple Regression Analyses for Predicting Emotional Reactions
a Age group: 1 = 18 to 30; 2 = 31 to 40; 3 = 41 to 50; 4 = 51 and above.
b P < .01.
c P < .001.
d Educational level:1 = up to high school; 2 = university and above.
e Personal experience: 1 = yes; 0 = no.
f P < .05.
g Perceived concern: 1 = low, 2 = moderate, 3 = high.
Perceived Threat
The majority of the participants reported not at all or very low susceptibility, concern and anxiety toward the individual with AD (69.9%, 69.1%, and 62.2%, respectively). The students had higher susceptibility scores (1.54) compared to the PCHPs (1.40) and laypersons (1.27; F 2 = 3.888, P = .021). After controlling for covariates (gender, age group, educational level, disease identification, and personal experience), MANCOVA failed to show significant group differences (Wilks’s λ = 0.960, F 6,608 = 2.076, P = .054, partial η 2 = .020, power = .752).
Differences Within the Subgroup of Physicians, Nurses, and Social Workers
A binary logistic regression analysis was conducted, using enter method, with diagnosis as the dependent variable and subgroup, gender, age group, educational level, personal experience, and perceived threat as covariates. A test of the full model was statistically nonsignificant, indicating that none of the predictors could reliably predict diagnosis (Omnibus chi-square=16.26, df = 11, P = .132).
Taking into account the variability of covariates (gender, age group, educational level, disease identification, personal experience, and perceived threat), MANCOVA revealed a significant multivariate main effect between the subgroup of physicians (N = 64), nurses (N = 35), and social workers (N = 13) across prosocial, aggression, anxiety, acceptance, and rejection emotional reactions (Wilks’s λ = 0.769, F 10,188 = 2.639, P = .005, partial η 2 = .123, power = .957). A univariate test showed differences on anxiety (F 2 = 4.254, P = .017, partial η 2 = .080, power = .732), with social workers demonstrating a lower percentage than the others, though the test exceeded P < .01.
The MANCOVA revealed a significant multivariate main effect between the subgroups across perceived threat (Wilks’s λ = 0.865, F 6,198 = 2.484, P = .024, partial η 2 = .070, power = .827), after removing the effect of covariates (gender, age group, educational level, disease identification, personal experience). Social workers expressed lower perceived consequences (0.89) compared to the physicians (1.56) and nurses (1.51; F 2 = 4.299, P = .016, partial η 2 = .078, power = .737).
Discussion
Despite the proliferation of studies on laypersons’ attitudes and knowledge about mental disorders in recent years 3,17 , there is a shortage of research to date on how the public and specialists (PCHPs, social work, and nursing students) perceive neurodegenerative diseases such as AD. This is crucial, though, because as the population grows old, higher proportions of people will increasingly come into contact with persons diagnosed with AD. This study sought to address a gap in the understanding of Greek laypersons and specialists’ identification of AD, emotional reactions, and perceived threat about developing AD.
Both PCHPs and students were expected to perform better than laypersons in identifying AD, endorsing more positive emotions and perceiving lower threats about developing AD. A study 30 has found practitioners and graduate students, both from the field of social work, to be equally accurate in recognizing pathological memory aging deficits. But this was not the case in the present study. After removing the effects of covariates, PCHPs did not significantly differ from laypersons in AD identification. In line with a recent review, 2 in which dementia diagnosis was given in less than two-thirds of patients with moderate to severe dementia, in our study 61.2% of the PCHPs identified AD. Given that the PCHPs would have been originally “laypersons,” it is highly unlikely that health training did not improve AD awareness. There may be several reasons for this finding. One interpretation is that PCHPs are fully aware of the multiple causes for mental impairment, so an initial diagnosis such as depression or dementia might be quite appropriate before further information is gathered. It can also be assumed that PCHPs accurately recognize the symptoms of the vignette as warnings signs of a degenerative disease, but they lack specialist support (eg, psychologists and social workers) 15 or specific differential skills and tools to diagnose AD. 31 Studies have shown that experts/specialists are more knowledgeable about dementia than generalists. 11,32 Other findings have shown that younger general practitioners (GPs) are less confident in diagnosing dementia 33 and females tend to diagnose significantly fewer cases annually. 34 Our sample mainly included female (68%) and young PCHPs (median age group: 36-40). In Greece, the individuals with early signs of AD are initially admitted in a primary care, and consecutively, they are referred to those eligible to diagnose neurodegenerative diseases (ie, neurologists). 35 Thus, the PCHPs may be reluctant to identify AD, diffident, or even fearful of stigmatizing the sufferer. 2 The identification of AD can be quite a challenge in the primary care setting, where a relatively short health care–patient interaction occurs and patients often demonstrate a mixture of multiple symptoms and health problems. 2 A moderate level of impairment, such as the one exhibited by the vignette, might have been difficult to be identified 2 by PCHPs. In our study, a high percentage of the PCHPs (78.2%) admitted no specific AD education. Abundant evidence has demonstrated that, as a result of low levels of overall knowledge 33,25 and lack of specific training about dementia, 34 GPs in primary care experience difficulty, miss or delay diagnosis of dementia. 2,9,12,15,35,36
Unexpectedly, laypersons were found equally accurate to the PCHPs in identifying AD. Although one study has shown that laypersons were equally knowledgeable to service providers about pathological memory aging issues,
30
in Greece
9
AD remains undiagnosed by both physicians and laypersons. Additionally, many studies
3,37
have demonstrated that the majority of laypersons correctly recognized nearly all symptoms they were presented with to be warning signs of AD (eg, disorientation) but Greek laypersons have been shown to be incapable in identifying the early symptoms of the disease.
It was also expected that academic training would have played a role, with students, if not equal to the PCHPs, being more competent in identifying AD than the laypersons. But this again was not the case. The students were the least competent in identifying AD among the 3 groups. Differences in the knowledge about pathological memory aging issues, with students being the least knowledgeable compared to laypersons and service providers, has been found. 30 This is an important result with noteworthy implications, considering that the students would be likely to encounter people with dementia in the near future. Notwithstanding the recent advancement in the Greek academic training to include aging and gerontological issues, it may not fully address these issues. It has been found that only about 3% of nearly 10 000 pages of social work textbooks included aging content. 38 In fact, curriculum in Health and Social Welfare School is limited in one course on aging issues. Further improvements in both undergraduate and postgraduate health care training may needed to fully cover the issues of dementia and AD specifically. Another explanation may be that students lack the clinical experience with the people with dementia. So their judgment is based exclusively on the misconceptions they may hold about aging (similarly to laypersons).
In line with previous results, 17 overall the participants endorsed more positive than negative emotions. However, after removing the effect of covariates (gender, age group, educational level, disease identification, personal experience, and perceived threat), MANCOVA showed that PCHPs were shown to express the least intense emotions (both positive and negative), with students and laypersons being more or less comparable. It has been shown that those with greater knowledge of aging may hold less ageist attitudes. 39 It is not clear, though, why PCHPs were found to express the least positive emotions. An explanation may be the PCHPs’ belief that not much could be done to improve the patients’ quality of life because of lack of resources available to support patients’ care in the community. 3 Thus, the accumulated experience about the problems of providing care for patients with AD may foster feelings of frustration and resignation. It can also be assumed that these feelings stem from their potential belief of lack of knowledge or their uncertainty in identifying AD. It has been found that the greater the intergroup anxiety (ie, anxiety when anticipating contact with the elderly people) the more negative attitudes and behaviors toward the elderly people 24,40 ; it could also be associated with negative emotions.
Students were shown to express high positive emotions (eg, prosocial). This may indicate their willingness to help, especially because of the near prospect of them working in the health and social welfare. Unexpectedly, they reported negative emotions in a comparable degree to that of the laypersons and in a much higher degree than the PCHPs. It is possible that academic training is limited in offering only the theoretical knowledge and not the experience to intervene in practice with geriatric patients and furthermore, the skills to cope with emotional reactions AD may elicit them. Indeed, the Health and Social Welfare School’s curriculum offered in Technological Educational Institute of Crete allows the students to have a relative short period of practicum in units with geriatric patients. On the other hand, it could be argued that PCHPs hold less negative emotions as a result of interacting in practice with individuals diagnosed with AD. In our study, personal experience was actually found to be a significant predictor of participants’ lower aggression, anxiety, acceptance, and rejection. It may be that negative emotional reactions could be bend over with interacting in practice with individuals diagnosed with AD, just as contact has been found to affect perceptions of the elderly people 25,41 and empathy feelings toward them. 26
Not surprisingly, the younger participants were found to report more intense emotions, both positive 42 and negative. 17 Consistent with other results, lower education 18,42 and higher perceived concern 8,17 were associated with higher acceptance to the person with AD. Personal experience was associated with less intense emotional reactions. 24,25,41 It has been shown that the more contact with elderly persons in the workplace the less anxiety. 43 Because of small sample sizes, it was not possible to examine predictors of the emotions separately in the groups of PCHPs, students, and laypersons. Future studies need to address this issue.
Surprisingly, within the group of PCHPs, identification of AD and emotional reactions did not differ between the social workers, nurses and physicians. This could be a consequence of the small sample sizes in these categories, particularly social workers, for a test to be significant. Future studies in multiple samples of considerable size may be needed.
The majority of the participants in all groups expressed low perceptions of threat about developing AD at some point in their lifetime. This is in line with previous studies 8,18 in respect to laypersons. No group differences were observed, despite the expectation. It is likely that perceived threat is associated with personal experience in the way that those who have personal experience with AD perceive lower threats. All participants were familiar with AD, either in a personal or professional level. Subgroup differences were found, with social workers expressing lower perceived consequences, compared to physicians and nurses. It is not clear why social workers believe that AD would be less stressful should they develop it than the others. A possible explanation is that social workers are more prepared to cope with the impairment the AD may elicit, due to their knowledge of the available community resources for the individuals diagnosed with AD. This merits further research.
With respect to the ERS, contrary to previous findings, 17 the 5-factor model 8 best fitted the data. Werner and her colleagues have repeatedly confirmed 4 factors underlying the ERS 17,18 with good reliabilities (ranging from .61 to .77). They have, however, consistently used EFA. In general, EFA may be appropriate for scale development, while CFA would be preferred when the researcher has a theory for the latent variable structure. 44 It is considered necessary, though, to be reported that the misspecified error covariances pertained those items, for which 2 alternative (ie, similar) Greek translations were sited in the questionnaire. A possible explanation is that those items represent systematic, rather than random, measurement error, which may derive from the translation of the items. No improvements were made as the internal consistency of the scale was satisfactory in each sample. Also the reliabilities of 3 subscales were adequate, whereas the low reliabilities of the acceptance and rejection subscales could be a result of the small number of items (2 items each). In summary, the 5-factor model of the ERS represented an accurate specification of its factorial structure for the Greek sample data. We have not examined the ERS’ structure in the 3 groups separately, because of small sample sizes. Further research would be desirable to provide firmer conclusions on the structure of the scale and to examine whether the latent factor structure of the ERS is the same and the factor loadings equivalent across samples.
The study has several limitations. First, all 3 samples were convenience and not probability ones. However, the results are in line with other European studies and may be considered to provide an accurate account of the current situation in Greece. The use of vignette methodology, though widely used, 27 limits our conclusions in response to the case presented. Some of the ERS subscales had relatively weak internal reliability (<.70) and results should be cautiously interpreted for these subscales. Finally, this study included PCHPs with various specialities and students of both social work and nursing schools. Additional studies to more homogenous subsamples are required.
In conclusion, students were shown to diagnose AD in a lower percentage than the other groups and hold more negative emotions toward an individual diagnosed with AD than the PCHPs. Laypersons adequately identified AD but their emotional reactions were comparable to those of the students. Although PCHPs identified AD in a higher percentage than the other groups, the percentage was lower than expected. They expressed the least negative emotional reactions to the individual with AD but still the least positive ones. Perceived threat was in general low within the groups of PCHPs, students, and laypersons but social workers reported higher perceived consequences compared to physicians and nurses. Significant predictors of intense emotional reactions were younger age, no personal experience with AD, lower education, and higher perceived concerns about developing AD.
These findings have important implications. Notwithstanding the rapid developments taking place in the area of dissemination of AD information, the findings of the present study indicate that there is still long way to go. The study suggests that the identification of AD could be further advanced and the negative emotions could be further reduced. This could be succeeded with the implementation of actions tailored to address the needs of each group. This may require the targeted training of the prospective PCHPs and the ongoing training of the current ones in gerontology issues and in appropriate diagnostic tools to optimize identification. Aging education also needs to directly address negative emotions toward individuals diagnosed with AD. Studies based on attribution theory 27 have demonstrated that emotional reactions could impact directly on discriminatory behaviors. Other findings have shown that negative attitudes toward the AD are associated with an increased level of burden by the caregivers. 45,46 Thus, sufficient academic preparation could serve to decrease negative stereotypes and discriminatory behaviors against AD. Although laypersons were found not to be at high risk, increasing government and advocacy initiatives and enforcing antidiscrimination policies and campaigns could advance AD identification and empathetic feelings toward individuals with AD. Actions to address the younger, the less educated, those with personal experience with AD, and those with higher concerns about developing AD should be implemented. In conjunction these actions targeting all risk groups could probably result in better care for individuals diagnosed with AD.
Footnotes
Appendix A
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.