
Abstract
Aim: To evaluate the safety of pacemaker implantation in patients with Alzheimer’s disease (AD). Methods: We reviewed all cases admitted to our institution between January 2008 and June 2009, with symptomatic bradyarrhythmia for whom a permanent pacemaker was implanted. Beginning in June 2009, we prospectively collected data from all patients with the same diagnosis and procedure. Patients with a diagnosis of AD were included in the study. The risks and frequency of complications due to the pacemaker implantation were evaluated. Because of the older age of patients, they were divided into 2 groups to define the effect of age on complication rate. Group 1 consisted of patients aged <75 years, and group 2 consisted of those who are ≥75 years. Results: Among the 574 patients with permanent pacemaker, 20 patients (3.4%) had a diagnosis of AD. Three patients with an AD experienced a complication and all were in group 2. However, the rate of complication was not significant within groups (P = 1.000). Reoperation was needed for all of them, and it was significantly higher in patients with AD than in patients without a concomitant disease (P = .006). Patients in group 2 had 3 times higher rate of complication (21.4%) than those without an AD and aged ≥75 years (7.1%; P = .125). Conclusion: Pacemaker implantation may be of risk in patients with AD, especially in those aged ≥75 years.
Introduction
Alzheimer’s disease (AD) is a common worldwide public health problem. Patients with AD are generally elderly and have multiple comorbidities. 1 –4 Also, immobility is not a rare issue in these patients. So the management of atrioventricular (AV) block is challenging. Indications for permanent pacemaker and the risks of the procedure are not clear. Therefore, we aimed to evaluate the safety of pacemaker implantation in the elderly individuals with this disease.
Methods
We reviewed all cases admitted to our institution between January 2008 and June 2009, with a diagnosis of symptomatic second-degree or third-degree AV block, 2:1 AV block, atrial fibrillation with bradycardia (average heart rate ≤40 bpm on 24-hour Holter monitoring) for whom a permanent pacemaker was implanted. Beginning in June 2009, we prospectively collected data from all patients with the same diagnosis and procedure. Bradyarrhythmia was defined by the surface electrocardiography. Patients with the diagnosis of AD were included in this study. The diagnosis of AD was established by the neurologist according to the criteria of Diagnostic and Statistical Manual of Mental Disorders. 5 Patients with gradual onset of memory loss and continuing cognitive decline without any underlying causes such as infections, nutritional deficiencies, traumatic brain injury, endocrine conditions, cerebrovascular diseases, seizure disorders, brain tumors, and substance abuse were defined to have AD. 5
Because of the older age of patients, they were divided into 2 groups to define the effect of age on the rate of complication. Group 1 consisted of patients aged <75 years, and group 2 consisted of those who are ≥75 years. Pacemaker types were chosen according to the type of bradyarrhythmia, patient’s age, physical status, and mobility state. Pocket hematoma requiring a drainage, local pacemaker area infection, lead infection, lead dislodgement, and pneumothorax occurred after the implantation of the pacemaker was defined as a complication. A complication rate was compared among patients with AD and those without a disease based on the same age group. Also the rate of reoperation due to the complication was compared, irrespective of age, in patients with AD to those without a disease. Collection and analyses of data were authorized, and the study was approved by the ethical commitee of our hospital.
Statistical Analysis
Quantitative variables were expressed as mean ± standard deviation, and the qualitative variables were expressed as percentage (%). Categorical data were compared using the chi-square test or Fisher exact test. Logistic analysis was applied for multivariate analysis. P < .05 was considered statistically significant. All statistical studies were carried out using NCSS (Number Cruncher Statistical System) 2007 and PASS 2008 Statistical Software Program (Utah).
Results
Among 574 patients (290 women, mean 67.7 ± 15.73 years) with permanent pacemaker, 20 patients (3.4%) have had a diagnosis of AD (12 women, mean 83.6 ± 6.96 years). The most frequent electrocardiogram findings were complete AV block (40%) and 2/1 AV block (35%). Patients’ age was between 12 and 97 years (73-97 years in AD). Three patients were in group 1 and 17 in group 2. One patient in group 1 and 3 patients in group 2 were implanted a dual chamber (DDD) pacemaker (20%), and others were implanted a single-chamber (VVI) pacemaker (80%). Three patients experienced a complication; 2 developed pocket hematoma and 1 developed lead dislodgement. All the 3 patients belonged to group 2 and everybody had a VVI pacemaker. However, complication rates were not different between groups 1 and 2 (P = 1.000; Table 1). All of them underwent a reoperation; 2 underwent hematoma drainages and 1 underwent lead reposition. Both patients with hematoma had a history of cerebrovascular accident and were on warfarin therapy. These 2 patients were diagnosed to have an AD before the cerebrovascular accident. Warfarin was stopped before the procedure and restarted the day after the procedure. Procedure was performed if the international normalized ratio is ≤1.5. Bridging to the heparin was not applied. Because there was no complication in group 1, a group 2 patient was compared with pacemaker implanted patients ≥75 years old without an AD; the rate of complication was 21.4% and 7.1%, respectively. However, this was not statistically significant (P = .125; Table 2). Of the 574 patients with a pacemaker, 60 patients without an AD experienced a complication. Of these, only 9 (15%) patients underwent a reoperation, and this was significantly lower than that in patients with AD (100%; P = .006; Table 3).
Complication Rates of Pacemaker Implantation According to the Age of Patients With Alzheimer’s Disease a
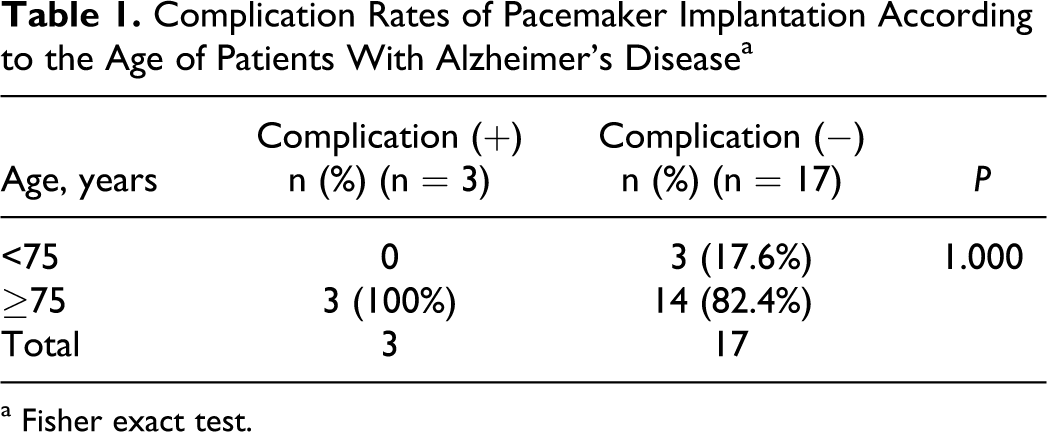
a Fisher exact test.
Complication Rates of Pacemaker Implantation in the Very Elderly Individuals With and Without Alzheimer’s Disease a
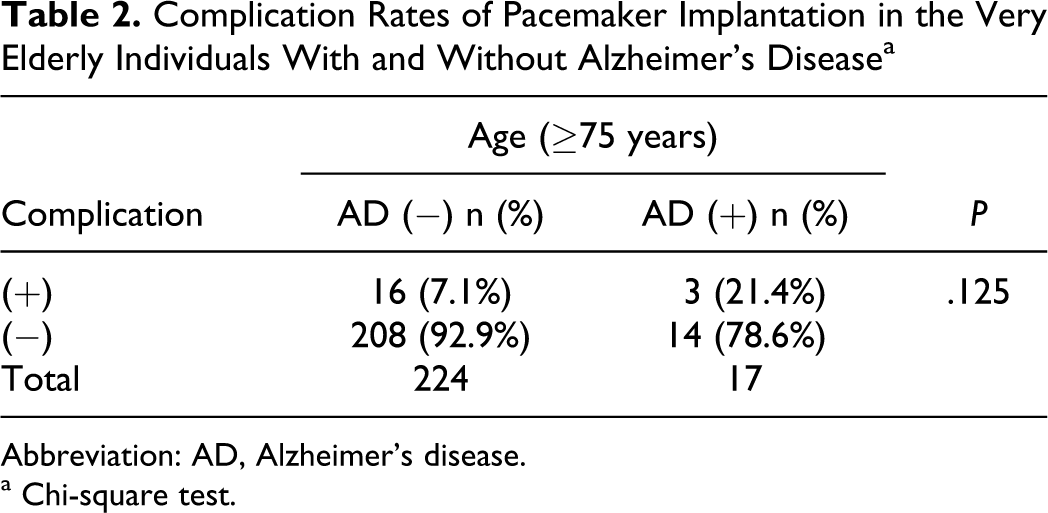
Abbreviation: AD, Alzheimer’s disease.
a Chi-square test.
The Rate of Reoperation in Pacemaker-Related Complications of All Pacemaker-Received Patients Based on the Existence of Alzheimer’s Disease a
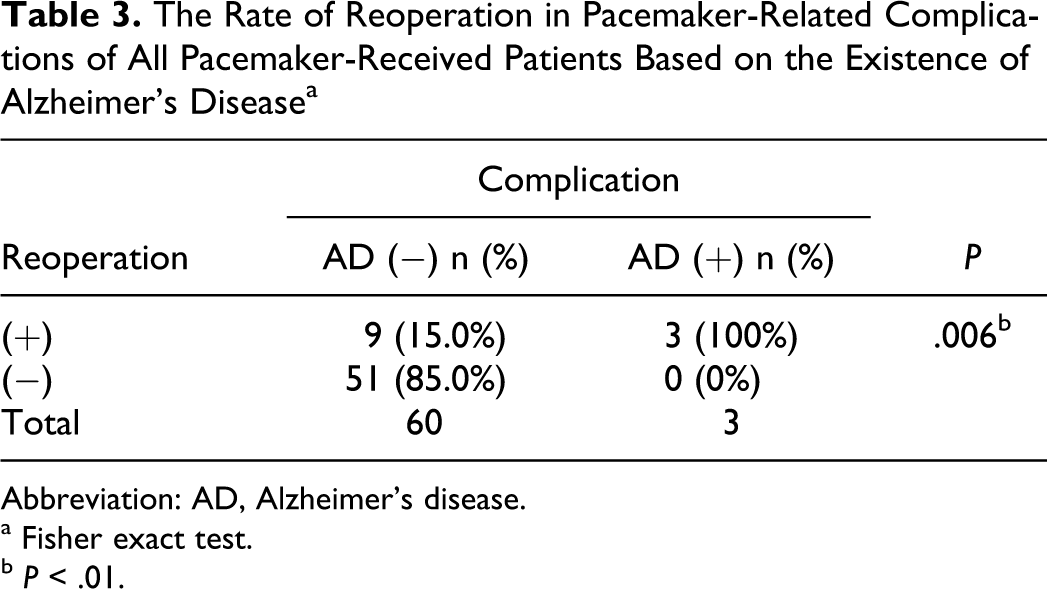
Abbreviation: AD, Alzheimer’s disease.
a Fisher exact test.
b P < .01.
Discussion
Alzheimer’s disease is a common worldwide public health problem. The disease most often presents with subtle onset of memory loss followed by a slowly progressive dementia that has a course of several years. Patients with this disease are generally >70 years. Elderly patients may be at increased risk of implant complications and are increasingly being referred for pacemaker implantation. Pacemaker use is high in older people, with an estimated 70% to 80% of all permanent pacemakers implanted in individuals aged ≥65 years. In a large multicenter trial, the complications from pacemaker implantation in the elderly patients aged ≥65 years were seen in 6.1% of patients, and 4.4% of patients required a repeat surgical procedure. 6 In our study, the overall rate of complication was 11% (63 of 574 pacemaker patients). To the best of our knowledge, there is no report of pacemaker-related complication rate in patients with AD. In our cohort, 15% of patients with AD experienced a complication. Bailey and Wilkoff declared that a pacemaker or defibrillator implantation in the elderly patients was not associated with significant increase in the complication rates. 7 In our findings, the rate of complication in the elderly population aged ≥75 years was 7.7% (19 of 244 patients). We also defined that 21.4% of AD patients aged ≥75 years who received the pacemaker experienced a complication, and this was 3 times higher than that in controls. Although this was not statistically significant, we suppose that an operator might be better needing to weigh the risks and benefits for each patient. Additionally, unlike in other studies, this study demonstrated that elderly patients with AD, in case of complication, always need a reoperation. This may be because of the high incidence of comorbidities, usage of antiplatelets/anticoagulants, and poor communication with the patients. After the implantation of devices, the patient would have either moved around earlier than a desired time or lied on his or her side, which would have led to lead dislodgement. The prevalence of cerebrovascular accident is increasing with age and it is high in patients with AD. So antiplatelet/anticoagulant usage is also high, which in turn increases the risk of pocket hematoma. Pocket hematomas are generally small in size and rarely need drainage, less than 0.5% of cases. Both our patients with pocket hematoma were on warfarin therapy. Discontinuation of warfarin without a bridging therapy did not prevent a hematoma and the drainage was needed. Recent studies demonstrated that interruption of warfarin with bridging to heparin or continuation of warfarin therapy during the procedure did not increase the risk of pocket hematoma. 8,9 Our patients were very elderly and older age might increase, by itself, the risk of reoperation. The low body mass index and week muscular structure might be inadequate, with low local pressure, to stop the leakage of blood.
Lead complications are the main reason for reoperation after implantation of pacemakers. Mainly procedure-related factors were identified as independent risk factors for lead complications. 10 Rarely, in the elderly individuals, it may be related to the patients unconsciousness. 11 Dislodgement of the lead, especially in pacemaker-dependent patients, is a dreadful complication. It must be repositioned without delay or will result in death. Our patient was not dependent on pacemaker. In our patient lead dislodgement occurred after the discharge from hospital and it was not related to the operation but could have been due to poor cooperation from the patient, may be the patient moved his arms over the shoulders shortly after the discharge.
The hemodynamic changes of aging include a reduction of ventricular compliance and increased contribution of atrial contraction to ventricular filling. Pacemakers that maintain synchrony between atria and ventricles may, therefore, be particularly advantageous in older adults. 6,7,12 A DDD pacemakers were not associated with increased risk of complications. 6 In our study, any patient with DDD pacemaker experienced a complication. We suppose that every patient, including elderly patients with AD, with indications to a DDD pacemaker might be encouraged to be implanted an appropriate pacemaker. Alzheimer’s disease, by itself, might not preclude this indication. Because dual-chamber synchronous pacing is the best way of avoiding a pacemaker syndrome which frequently occurred in the case of a VVI pacemaker.
In conclusion, patients with AD are generally elderly and are increasingly being referred for pacemaker implantation. Pacemaker implantation may be of risk in patients with AD, especially in those aged
Footnotes
This article is accepted as a poster presentation in 27th National Congress of Cardiology in Istanbul, and the abstract was published in the archives of the Turkish Society of Cardiology.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.