
Abstract
The longitudinal influences on physical capacity and habitual aerobic activity level in the early stages of Alzheimer’s disease (AD) are unclear. Therefore, changes in physical capacity and aerobic activity level were evaluated. Twenty-five individuals with AD were assessed annually for 2 years, by 10-m walk test, 6-minute walk test, and timed up-and-go (TUG) single/dual tasks. Habitual aerobic activity was assessed by diary registrations. The AD group showed a lower physical capacity than controls at baseline but comparable levels of aerobic activity. During the follow-up period, physical capacity declined in the AD group, but the aerobic activity levels changed only marginally. Our results show that in the early stages of AD, people are capable of maintaining health-promoting aerobic activity levels, despite a decline in their physical capacity. Additionally, it appears that cognitive dysfunction contributes to an impaired physical capacity. The TUG tasks might, therefore, be useful for detecting early signs of cognitive impairment.
Introduction
In the early stages of Alzheimer’s disease (AD), gait impairment, including a decreased walking speed, and a greater step-to-step variability are present. 1 –3 Recent reports have suggested that the changes in gait pattern and the increased risk of falls among individuals with AD are primarily due to a deficit in executive function, and the ability to divide attention and to interpret and integrate sensory information. 4 –8 The level of physical activity may also play a role in the decline. 9 –11
The World Health Organization discriminates between 2 different aspects of physical activity: capacity and performance. 12 Capacity describes an individual’s ability to execute a task or an action in a standard environment and performance describes what individuals habitually do in their current environment. In the Western world, public health recommendations regarding physical activity for the promotion of health are uniform 13 –15 and state a minimum level of aerobic activity of moderate intensity, for example leisurely walking or cycling, for at least 30 minutes for 5 days each week. Physical activity of this intensity is indicated to have possible positive effects on brain function in the sedentary elderly individuals 16 and on those at risk of developing AD. 17 –19 Moreover, it appears important for individuals in all stages of AD to perform regular physical activity, both for preserving motor function and for benefiting from positive effects on cognitive function, behavioral problems, sleep, and well-being. 20 –23 Nevertheless, physical performance, as indicated by the habitual aerobic activity levels of individuals in the early stages of AD, is unclear. The longitudinal changes in physical capacity and habitual aerobic activity in early-stage AD have, additionally, not been entirely elucidated. 24 The main aim of this study, therefore, was to evaluate changes in physical capacity and performance with an emphasis on habitual aerobic activity, during a period of 2 years in individuals in the early stages of AD.
Methods
Participants
Individuals with AD were recruited from the outpatient department of the Memory Clinic at Uppsala University Hospital, Sweden, for a duration of 20 months. The AD diagnosis fulfilled the current research criteria of Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) 25 and National Institute of Neurological and Communicative Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association. 26 None of the participants had significant cardiovascular disease, or symptoms indicating frontotemporal dementia or Lewy Body dementia. Inclusion criteria for the study were Mini-Mental State Examination (MMSE) score of 20 to 30 points, 27 Functional Assessment Staging (FAST) stage 3 or 4, 28 age 80 years or younger, community-dwelling with a cohabitant, no other illnesses, injuries, or pain substantially affecting mobility, and no other reason for not participating (eg, absence of illness awareness). Of the 48 individuals with AD who fulfilled the inclusion criteria, 19 declined participation. The remaining 29 eligible participants underwent a brief examination, including an interview, after which it was discovered that 3 no longer fulfilled the inclusion criteria and 1 other person withdrew their consent to participate. Thus, in total, 25 individuals with AD were included in the study. A group of 25 age- and gender-matched controls were recruited. Nineteen of them (≥65 years of age) were identified from a register of cognitively healthy people who had previously consented to participate in clinical research, and 6 of them (<65 years of age) were recruited from the staff of a geriatric clinic. The inclusion criteria for the control group were a MMSE score of 27 to 30 points, FAST stage 1 or 2, age 80 years or younger, and no other illnesses, injuries or pain substantially affecting mobility (Table 1). The Regional Ethical Review Board, Uppsala, Sweden approved the study, and all participants gave their informed consent to participate.
Characteristics of Participants With Alzheimer's Disease (AD) and Group-Matched Healthy Controls a
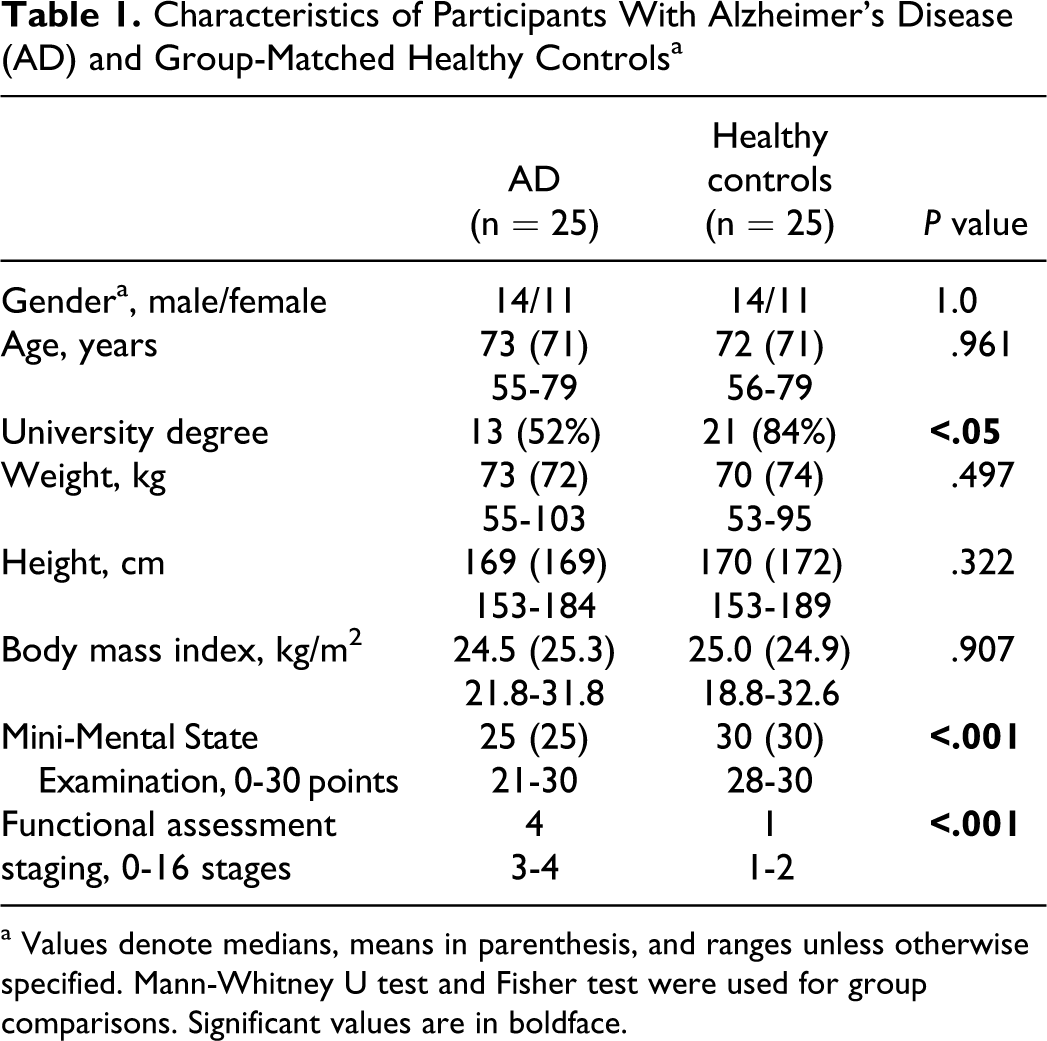
a Values denote medians, means in parenthesis, and ranges unless otherwise specified. Mann-Whitney U test and Fisher test were used for group comparisons. Significant values are in boldface.
Data Collection
The AD group was assessed annually for 2 years by the measurement of physical capacity, physical performance, falls, functional status, and cognitive function. The control group was assessed once, at baseline.
Measurement of physical capacity
The 10-m comfortable walk test (10MWT), starting from a standing position, 29 was chosen to assesses the general physical function, and the 6-minute walk test (6MWT) 30,31 was chosen to assesses endurance and walking capacity. Three different types of timed up-and-go (TUG) tests (1 TUG single and 2 TUG dual tasks) were chosen to assess the basic mobility and divided attention. 32,33 In the 2 TUG dual tasks, the participants simultaneously recited female and male names or animals (names/animals) while walking. Participants were instructed to continue walking, even if they could not come up with any words. In all the 3 types of TUG test, necessary verbal cueing such as “turn around,” “sit down,” or answers to questions such as “and back again?” were given and recorded in the test protocol. The 10MWT, the 6MWT, and the TUG tests are well established and are considered reliable for individuals with AD. 34
Measurement of physical performance
The participants’ habitual aerobic activities of moderate intensity or higher, lasting 10 minutes or more, were recorded in a diary for 2 weeks to gain an overall picture of the aerobic activities performed. 35 In the AD group, registrations were performed or supervised by the participant’s cohabitant. The recorded habitual aerobic activities were classified according to the coding scheme proposed by Ainsworth et al as a basis, 36 related to public health recommendations, 13 –15 and then quantified by calculating minutes/week of aerobic activity of moderate intensity or higher. Additionally, days/week with aerobic activity ≥30 minutes were quantified.
Measurement of falls and functional status
Any falls during the previous year were registered for both the AD and control groups. In the AD group, the cohabitant reported any falls. Functional status, indicating the cognitive state related to activities in daily life, was assessed with FAST, which includes 16 stages (1-7f). 28 Stages 1 and 2 indicate “normal adult” and “normal older adult,” and stages 3 and 4 indicate early dementia and mild dementia, respectively.
Measurement of cognitive function
The AD group completed 4 cognitive tests: the MMSE, 27 the clock drawing test (CD), 37,38 the verbal fluency test (VF), 37 and the trail-making test A (TMT A). 39 The MMSE is a composite screening test of cognitive function; the CD assesses visuospatial function, semantic memory, and planning; the VF assesses semantic memory and language; and the TMT A assesses visual attention and executive function (mental speed and flexibility). The control group only completed the MMSE test.
Statistical Analysis
Descriptive statistics were calculated and nonparametric statistics were applied because of the small sample size. The Mann-Whitney U test was used for continuous variables and Fisher’s test for categorical variables to assess the differences between the AD and the control groups at baseline. The percentage time differences (dual task cost) between TUG single and TUG dual tasks were calculated. For the AD group, longitudinal differences in physical capacity, habitual aerobic activity level, and cognitive function were calculated by Friedman’s test. The Wilcoxon signed-rank test was used for post hoc pairwise analyses of the differences in the follow-up period, and correlations between physical capacity and cognitive function were assessed by Spearman’s rank correlation coefficient. All the tests were 2-tailed. The level of significance was set at P < .05. For post hoc pairwise comparisons, significance was set at P < .025 to adjust for the 2 relevant comparisons. All calculations were performed with SPSS, version 18.
Results
Twenty-two of the 25 participants with AD completed the 2-year study period, reasons for discontinuation were the cohabitant’s occupation (n = 1) or a severe illness other than AD (n = 2). Of the 22 participants completing the study, 21 were still community-dwelling at the end of the study period.
Baseline Comparisons Between the AD and Control Groups
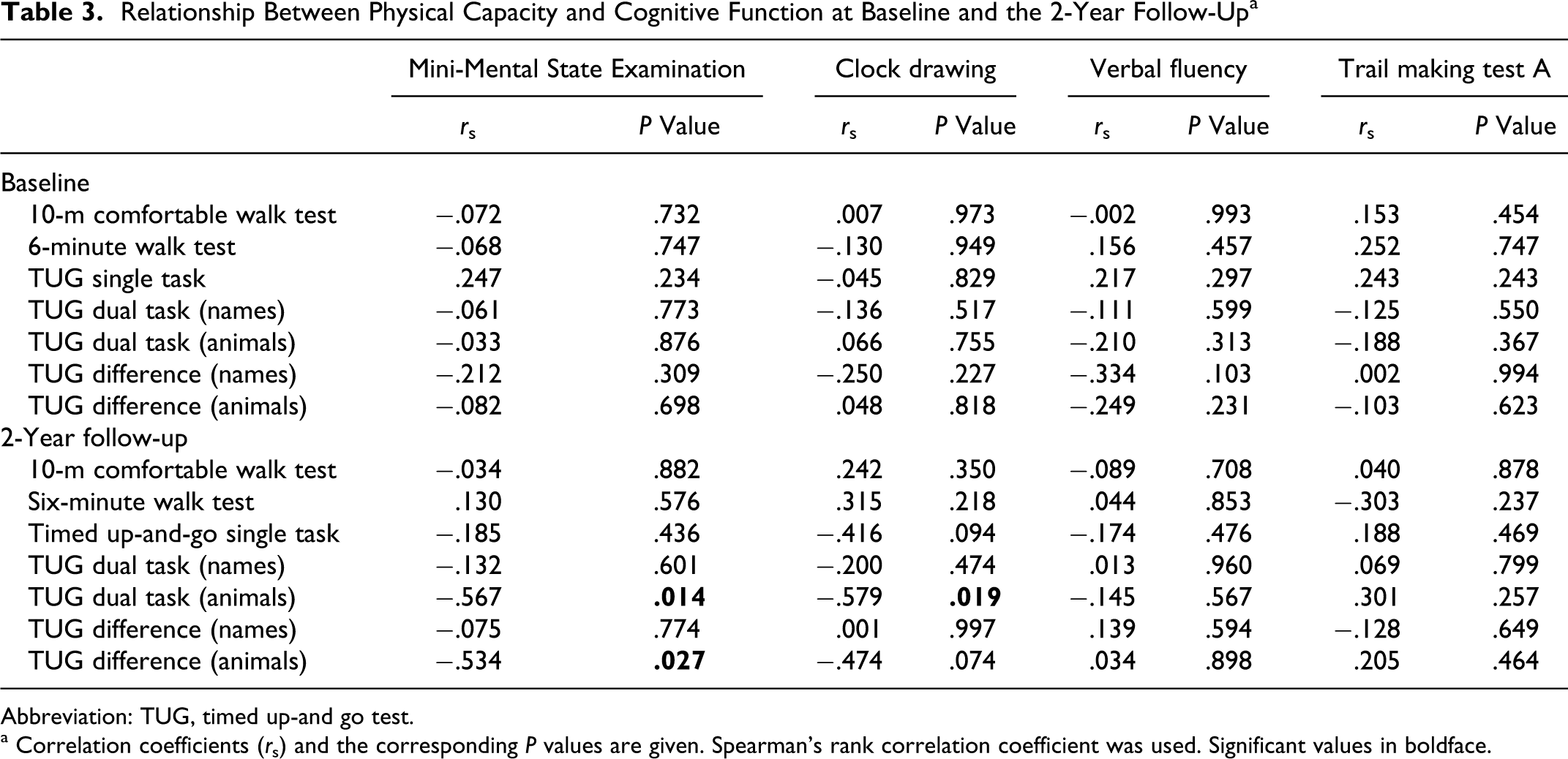
Participants with AD showed results at a significantly lower level than the controls in all included measures of physical capacity (Table 2). The AD group needed a substantially longer time to complete the TUG dual task (names/animals) than the TUG single task, whereas the between-task time differences for the control group were marginal. The dual task cost was 46% (names) and 89% (animals) in the AD group and 7% (names) and 11% (animals) in the control group. During the TUG single task, verbal cueing was needed for 8 participants in the AD group but only 1 in the control group. For both TUG dual tasks, 12 participants in the AD group and none in the control group needed cueing. However, there was no significant correlation between the time differences (TUG dual task minus TUG single task) and the cognitive tests (Table 3).
Baseline results for Physical Capacity and Aerobic Activity Level in Participants with Alzheimer's disease (AD) and Group-Matched Healthy Controls a
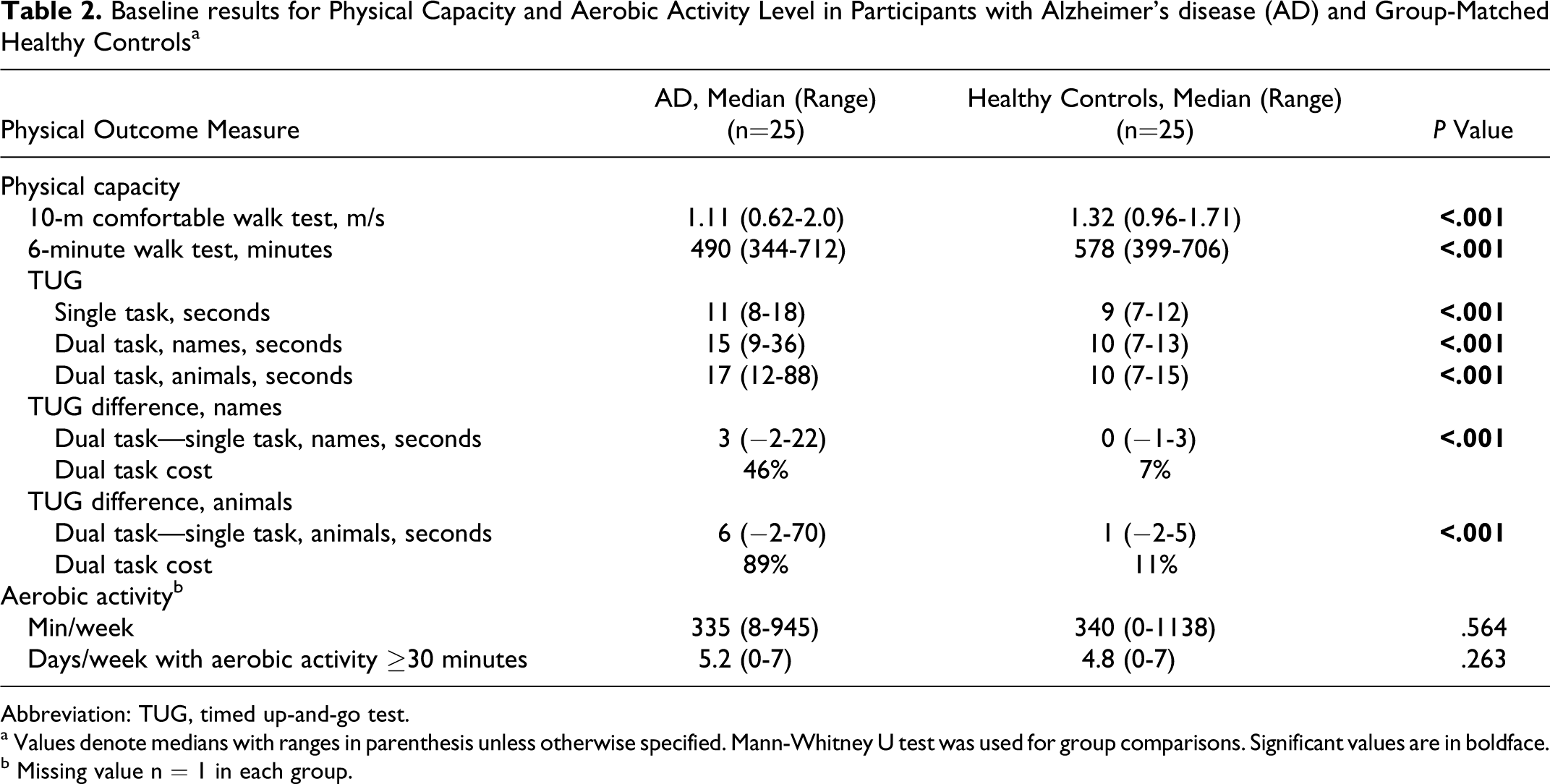
Abbreviation: TUG, timed up-and-go test.
a Values denote medians with ranges in parenthesis unless otherwise specified. Mann-Whitney U test was used for group comparisons. Significant values are in boldface.
b Missing value n = 1 in each group.
There was no difference between the AD and control groups in reported habitual aerobic activity at baseline (Table 2). In both groups, 20 (83%) of the 24 participants reached or exceeded the public health recommendations of 150 minutes of aerobic activity per week. The most common aerobic activities in the AD group were “walking,” “cycling,” and activities categorized as “lawn and gardening.” 36 Similarly, in the control group, the most common aerobic activities were walking and activities categorized as lawn and gardening.
The rate of falls was low in the AD group. At baseline, 3 of 25 participants had experienced 1 fall during the last year. In the control group, 10 participants had sustained 1 or 2 falls during the same period.
Longitudinal Results in the AD Group
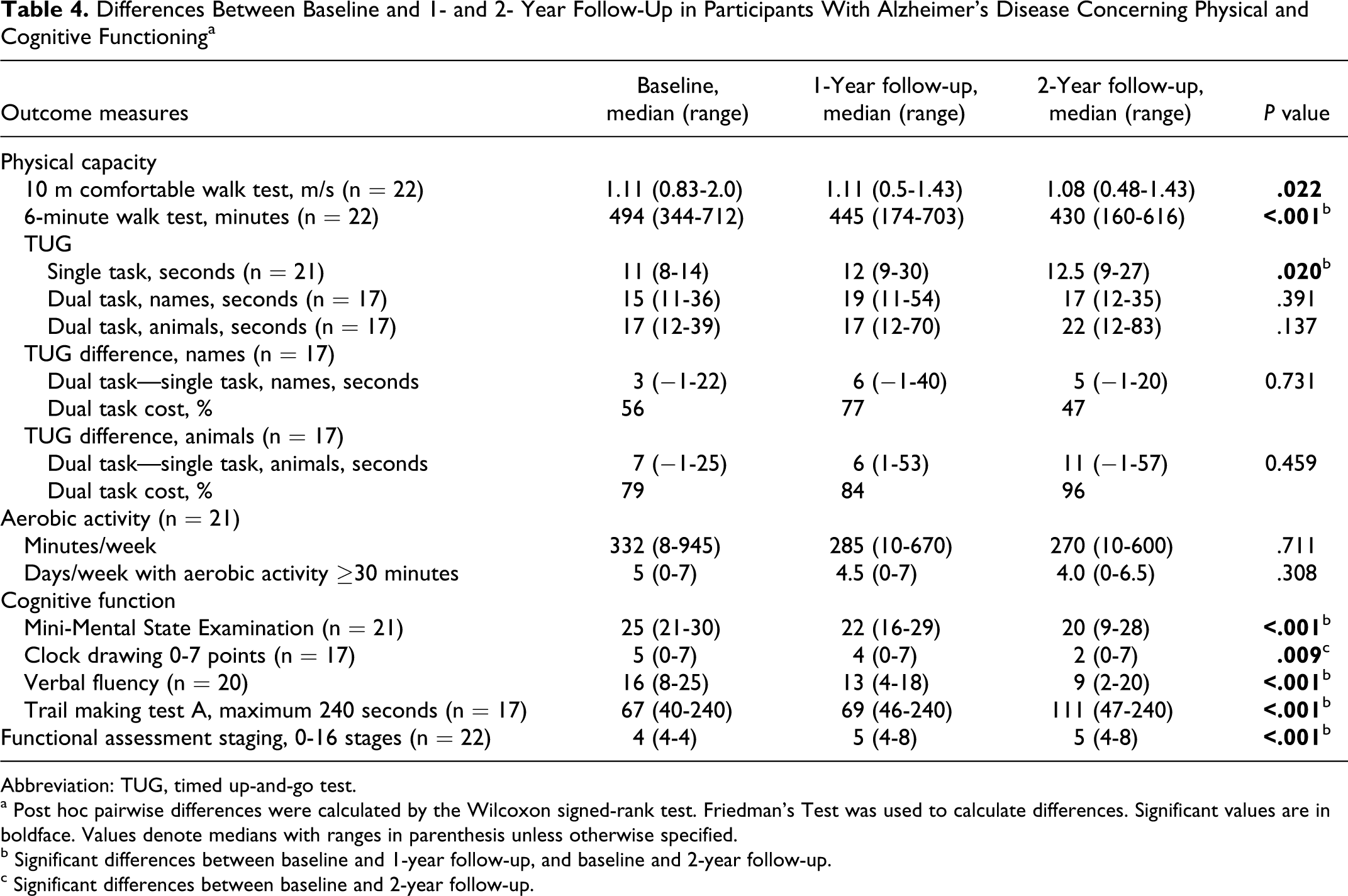
A deterioration of physical capacity was identified in the AD group (Table 4), indicated by decreasing results in the 10MWT, the 6MWT, and the TUG single task. Cognitive function also declined (Table 4), indicated by decreasing results in the MMSE, the CD, the VF, and the TMT A. No significant decline was identified in the TUG dual tasks. However, 5 of the 22 participants were unable to perform the TUG dual task due to impaired cognition. Likewise, the number of participants requiring verbal cueing increased, from 6 to 13 in the TUG single task, from 6 to 12 in the TUG dual task (names), and from 7 to 10 in the TUG dual task (animals). At the 2-year follow-up, moderate, significant correlations were detected between the time difference (TUG dual task [animals] minus TUG single task) and and the MMSE (rs = −.534), and between the TUG dual task (animals) and the MMSE (rs = −.567) plus the CD (rs = −.579) (Table 3).
Relationship Between Physical Capacity and Cognitive Function at Baseline and the 2-Year Follow-Up a
Abbreviation: TUG, timed up-and go test.
a Correlation coefficients (r s) and the corresponding P values are given. Spearman's rank correlation coefficient was used. Significant values in boldface.
Differences Between Baseline and 1- and 2- Year Follow-Up in Participants With Alzheimer's Disease Concerning Physical and Cognitive Functioning a
Abbreviation: TUG, timed up-and-go test.
a Post hoc pairwise differences were calculated by the Wilcoxon signed-rank test. Friedman's Test was used to calculate differences. Significant values are in boldface. Values denote medians with ranges in parenthesis unless otherwise specified.
b Significant differences between baseline and 1-year follow-up, and baseline and 2-year follow-up.
c Significant differences between baseline and 2-year follow-up.
In contrast to declining physical capacity and cognitive function, there was no significant change in reported habitual aerobic activity in the AD group during the 2-year period. However, a slight reduction in aerobic activity was indicated (Table 4). Nevertheless, 17 (81%) of 21 participants in the AD group still reached or exceeded the public health recommendation for aerobic activity. There was no significant change in the rate of falls.
Discussion
The results implied that physical capacity, evaluated by performance-based tests (10MWT, 6MWT, and TUG), was affected in the early stages of AD and continued to deteriorate during the subsequent years of the disease. In contrast, the reported habitual aerobic activity level of the AD group was comparable to that of the healthy controls at baseline and remained relatively stable during the 2-year study period. The baseline impairment of physical capacity supported previous findings from cross-sectional studies, 1,5 however, the continuing decline in physical capacity, but maintained health-promoting aerobic activity levels, has not previously received much attention. The longitudinal findings based on physical capacity, habitual aerobic activity, and cognitive function yielded new perspectives on how the ability to be physically active was influenced during the early years of AD. They indicate that the aerobic activity levels were not associated with the decline in physical capacity and cognitive function. Hence, the promotion of habitual aerobic activity may be considered as a health-promoting intervention in dementia care.
Besides a slowing of walking speed, participants with AD had substantial difficulty in performing the TUG tasks. Even at baseline, almost one third of the AD group required verbal cue support to be able to complete the TUG single task, and nearly half of them required verbal cues to complete the TUG dual tasks: only 1 participant in the control group needed verbal support. At the 2-year follow-up, 5 of the remaining 22 participants in the AD group were unable to accomplish the TUG dual tasks, despite verbal cueing. Systematic reports on the need of participants for verbal cueing have not previously been presented.
In addition, there were distinct time increases between performance of the TUG single and 2 dual tasks: these time increases were larger than the cut-off suggested by Horak et al 40 as a clinically important dual task cost (ie, >10%), and larger than the dual task cost reported among fallers (ie, 25%). 33 The time differences were already present at baseline but did not change significantly during the follow-up period.
The combination of a complex mobility sequence with a simple cognitive task, such as the use of the TUG tests, appeared to be a sensitive measure of divided attention in early-stage AD. In fact, the TUG tests seemed to be more sensitive than solely walking combined with a cognitive task, which has been used in previous studies of individuals with dementia.2,5,8,41 The TUG tests therefore appear viable measurements when screening for the early signs of cognitive impairment, but need to be confirmed in further investigations. The focus of such investigations should be on the dual task costs and the qualitative aspects, such as the need for verbal cueing and changes in gait pattern due to the dual task condition.
Cognitive impairment appeared to interfere with physical capacity, even in the early stages of AD, as seen from the TUG tests results. A possible explanation is that walking under usual circumstances involves both the subcortical brain regions, which are primarily responsible for automatic gait, and the cortical level for the activity of walking, requiring executive function. 4,42,43 As executive function, working memory and the ability to divide attention are commonly impaired in the early stages of AD, 2,5 –8,41,44 a person’s performance of a complex motor test, such as TUG, may be markedly affected if a cognitive task is added, regardless of any instructions to prioritize the motor task. 45 However, there was no significant correlation between the time differences in the TUG and the cognitive tests at baseline. At the 2-year follow-up, there was only a moderately significant correlation between the time differences in the TUG and the MMSE tests. These findings indicate that the cause of the described dual task deficits was complex and involved both impairments in cognitive domains and different individual strategies in a dual task condition.
The fact that more participants in the control than in the AD group had sustained a fall during the last year was unexpected. It might be speculated whether the control group took part in more risky types of activities, although these were not captured by the registrations of aerobic activities. Additionally, the reports of sustained falls in the AD group might not be fully valid, as the participants carried out activities on their own during the day and may have forgotten to tell their cohabitants about any falls that did not result in injury.
Although there was a slow trend toward a lesser amount of habitual aerobic activity throughout the study period, the participants with AD showed a potential to maintain a health-promoting level of aerobic activity. A factor that might have contributed to the relatively stable aerobic activity level was that all the participants except 1 were still cohabiting with a spouse at the 2-year follow-up. This probably increased the possibility of receiving support to maintain a health-promoting level of aerobic activity.
Walking was the most common aerobic activity in our study, which was in agreement with the previous findings, where walking appeared to be prioritized among the people with AD and their caregivers as part of a daily routine for improving well-being and overall health. 46 –48 A high level of aerobic activity is associated with prolonged survival in AD. 49 Moreover, physical activity has possible positive effects on physical capacity, cognitive function, and mood in people with mild cognitive impairment and dementia. 17 –23 Aerobic activity of moderate intensity can have positive structural and functional effects on the brain, particularly on the hippocampus region in the healthy and sedentary elderly individuals. 16,50,51 However, the optimal physical activity for individuals with a differing severity of AD, in terms of type, intensity, duration, and frequency, is unclear. 24,52,53
The results should be interpreted in light of some limitations to the study. One main limitation is the small sample size with a wide age range, which restricts the possibility to generalize the results to a larger population. Furthermore, the high education level among the participants may explain the fact that over 80% in the AD and control groups reached or exceeded the recommended level of aerobic activity, and the AD group’s aerobic activity level remained relatively stable during the follow-up period. Although the need for support to perform habitual aerobic activities was not evaluated, it is possible that the AD group were more active in their everyday lives due to their cohabitants’ support. Despite these limitations, however, deteriorations in physical capacity and cognitive function were demonstrated during the 2-year study period.
Assessing habitual aerobic activity by diary registrations has limitations related to uncertainty of intensity and the risk of overestimation. Combining the diary registrations of habitual aerobic activities with technical equipment such as movement sensors or heart rate monitoring would have enhanced the results. However, the aim of the study, that is to explore the overall picture of habitual aerobic activities performed by people in early stages of AD, could be obtained by the use of diary registrations. The validity of the diary registrations for the aerobic activities of moderate intensity or higher was ensured through careful instructions to the caregivers and participants regarding intensity, clarifications if there was any uncertainty about recorded activities, and classification of activities according to the coding scheme by Ainsworth. 36 The main strength of this study is the longitudinal design focusing on the diverse perspectives of physical activity, namely physical capacity and performance, along with cognitive function in a community-dwelling group of individuals with AD. These findings contribute to current knowledge by providing new perspectives on how the ability to be physically active is influenced during the early years of AD.
These findings raise questions as to whether impaired physical capacity and cognitive function are barriers to maintaining a health-promoting aerobic activity level in the early stages of AD. Hence, it could be speculated whether contextual factors 12 such as lack of support are more important. Therefore, interventions to help support community-dwelling individuals with early AD maintain a health-promoting aerobic activity level should be considered. Additionally, the results highlighted the need of clarifying whether declining physical capacity in early-stage AD primarily reflects declining cognitive function. For this reason, evaluating physical activity interventions by measuring physical capacity should be carried out with cautiousness. However, the interplay between aerobic activity, cognitive function, and physical capacity in early-stage AD needs to be explored further.
Conclusions
Our results show that in the early stages of AD, individuals are capable of maintaining health-promoting aerobic activity levels, despite a decline in their physical capacity. Additionally, it appears that cognitive dysfunction contributes to impaired physical capacity. The TUG tasks might, therefore, be useful for detecting the early signs of cognitive impairment.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Demensfonden Foundation, the Fondkistan Foundation, Novartis, the Swedish Association of Registered Physiotherapists, and Akademiska sjukhuset, Uppsala University Hospital.