
Abstract
We studied use of vitamins, minerals, herbs, and other dietary supplements for cognitive health. We refer to these products as supplements. Data were from the 2007 National Health Interview Survey, which asked about complementary and alternative medicine (n = 22 783). Chi-square and multivariate logistic analyses were weighted for national representativeness, accounting for the survey design. Among supplement users, about 8.8% of those without cognitive problems used them for cognitive health; 15.7% of those with cognitive problems did so. Fish oil, Ginkgo biloba, and vitamins were commonly used for cognitive health. Among supplement users, 38% did not tell health care providers. In adjusted results, adults reporting cognitive problems were more likely than others to use supplements for cognitive health (odds ratio 1.77, confidence interval 1.39-2.25). Adults are more likely to use supplements to treat or cure cognitive problems than to prevent them. Many do not discuss this use with health care providers.
Keywords
Introduction
In 2008, an international estimate was that 34.4 million people had dementia. 1 The number was projected to grow to 63 million by 2030. 2 In the United States, cognitive decline may affect 1 in 4 adults of age 70 and older living in the community. 3 About 5.3 million Americans have Alzheimer’s disease. 4 More than a quarter of adults who live beyond age 85 will develop Alzheimer’s disease or a related disorder. 4 Many older adults have experiences with family or friends who have dementia.
Many adults in the United States are concerned about Alzheimer’s disease, memory loss, or other types of cognitive decline, and want to reduce their risks for these problems. In a poll conducted with respondents as young as 35, nearly 27% reported being concerned about developing Alzheimer’s disease. 5 About 60% of adults responding to a 1999 to 2000 Harris Interactive survey said they were somewhat or very worried about memory loss. 6 One national survey suggested that about half of Americans think there are things we can do to lower our risk of Alzheimer’s disease. 5 In a survey of African Americans, 50% said they had behaviors that they thought would promote “brain health.” 7 In a large qualitative research study conducted at 9 U.S. locations, The Healthy Brain Study, 8 many participants expressed great anxiety and fear about memory loss. 9
People use a variety of alternative therapies hoping they might prevent or treat dementia, primarily vitamins, minerals, herbs, and other dietary supplements. 10 –13 We refer to these products as supplements. There is evidence from observational studies, randomized clinical trials conducted at single sites, and nonrandomized clinical trials that supplements may help to prevent or treat dementia. 10,14 –18 Most systematic reviews of the relevant science have not supported the use of supplements to prevent or treat dementia. 19 –22 The lack of support from systematic reviews may be attributable to the review designs. For example, an influential review sponsored by the National Institutes of Health focused almost exclusively on evidence from randomized clinical trials. 23 Similarly, an influential Cochrane review of Ginkgo biloba use for cognitive impairment and dementia focuses exclusively on randomized double-blind studies. 20 While the rigorous approach of these reviews is useful, the studies ignore evidence from other informative study designs, including even large-scale and well-conducted observational studies that provide much of the available evidence about reducing the risk of dementia in areas other than supplement use, such as physical activity. 24 Moreover, as systematic reviews of randomized trials focused on cognitive health sometimes observe, such trials often have short durations, limited sample sizes, a focus on younger–old populations, inadequate blinding, and other design features that limit their usefulness and applicability to decision making about the safety and efficacy of long-term use at the population level. 25 This is particularly relevant for studying cognitive outcomes such as dementia, which occurs with relatively low incidence except in older populations, and which tends to develop over a period of years. 25
There is evidence that a large percentage of people with dementia may use supplements to treat it, despite potential side effects, and a lack of clear evidence of efficacy. 26 –30 Supplement use for cognitive health is consistent with growing use of complementary and alternative medicine (CAM) generally. 31,32 Many older Americans may believe that supplements can promote cognitive health, including Ginkgo biloba, garlic tablets, ginger root, fish oil, and omega-3 fatty acids, as well as multivitamins and vitamins C, D, and E. 33 –35 The popular media promote these supplements for cognitive health. 36 –38 A concern with use of supplements for cognitive health is that many health care professionals may not ask patients about their use and thus cannot advise patients about potential interactions with conventional medicine. 39 Patients often do not tell their health providers that they use supplements because they do not think it is important 32,40 or are concerned that their provider might disapprove. 41
There is limited research on the use of supplements by people with dementia, 28,29 as distinguished from studies focused on the safety or efficacy of such use. Landin et al 29 found that the most frequently used supplements among persons with dementia were vitamins, followed by garlic, magnesium, ginseng, and omega-3 fatty acids. Jorm et al 28 found that the most frequently used supplements to enhance memory among those with and without memory problems were Ginkgo biloba, vitamins E and B, folic acid, and fish oil. No studies in the United States have examined supplement use for cognitive health using nationally representative data.
We examine supplement use for cognitive health using data from the 2007 National Health Interview Survey (NHIS), a nationally representative survey of adults in the United States, and its CAM supplement. 42 We address 3 research questions. First, what supplements do adults use most often for cognitive health? Second, what percentage of adults who use supplements for cognitive health tell their health care providers? Third, are individuals who use supplements for cognitive health more likely to do so to prevent a cognitive problem such as dementia, or to treat or cure an existing cognitive problem? The limited literature on these issues does not support hypotheses for the first 2 research questions. Our hypothesis regarding the third research question is that people will be more likely to use supplements to treat or cure cognitive problems than to prevent them. This hypothesis is supported by the limited success of conventional medicine in treating cognitive impairment and dementia. Thus, we expect that individuals with cognitive impairment, including those with dementia, may substitute supplements for conventional medicine or use them as a complement.
Methods
Data Source and Study Population
We conducted a cross-sectional analysis of supplement use for cognitive health by Americans aged 18 through 92, using data from the 2007 NHIS and its CAM supplement. The NHIS is a nationally representative household survey conducted annually by the National Center for Health Statistics. 42 The survey collects information about the use of medical services and health status and demographic and economic information. A total of 23 393 adults aged 18 and over responded to the NHIS; 22 783 of them completed the CAM supplement. The study was approved by the Institutional Review Board at the University of North Carolina at Charlotte.
Dependent Variables
Participants had several opportunities to indicate that they used supplements for cognitive health. Participants were asked, “During the past 30 days, did you take any of these herbal supplements?” They were shown a list of 45 herbal supplements and asked to select up to 2 that they had taken. They were also asked, “During the past 30 days, did you take any of these vitamins or minerals?” They were shown a list of 20 vitamin and mineral supplements, including “multivitamins and/or mineral combinations,” and asked to select up to 2 that they had taken. Separately for each herb or vitamin, participants were asked whether they had taken it “to improve mental ability or memory?” Affirmative answers were considered to indicate supplement use for cognitive health.
Respondents were also asked, again separately for each herb or vitamin, whether they had taken it in the past 30 days “to treat or cure a specific disease or health problem,” or “to prevent a specific disease or health problem.” Those responding affirmatively about treatment or cure were shown a list of 81 health conditions and asked whether they used the herb or vitamin “to treat or cure” any of the conditions. Three of the health conditions were cognitive problems, listed as “dementia, including Alzheimer’s Disease,” “memory loss or loss of other cognitive function,” or “senility.” Participants selecting any of these responses were also considered to have used a supplement for cognitive health. Those who said they used the supplement “to prevent” a health problem were separately shown the list of 81 health conditions that included “dementia, including Alzheimer’s Disease,” “memory loss or loss of other cognitive function,” and “senility.” Those selecting any of these as conditions they tried to “prevent” with a supplement were also considered to have used a supplement for cognitive health.
In addition to herbs and vitamins, the NHIS also asked about the use of 15 other types of CAM for cognitive health, although those questions focused only on disease treatment. These were acupuncture; ayurveda; biofeedback; chelation; chiropractic or osteopathic manipulation; special diets; energy healing therapy; hypnosis; homeopathic treatment; massage; movement techniques (eg, Feldenkreis, Alexander Technique, and Pilates); naturopathy; relaxation techniques; traditional healer; or yoga, tai chi, or qi gong. Only 10 participants said they used any of these CAM types specifically for cognitive health. Thus, we focused our analysis on supplement use. The survey also asked about prayer for health, which is often considered to be a form of CAM; those questions did not specifically address cognitive health.
Independent Variable of Primary Interest
The independent variable of primary interest indicated whether the participant reported a cognitive problem. Thus, the estimate associated with this variable indicated the degree to which individuals who used supplements did so to treat or cure cognitive problems. Reports of cognitive problems were responses to the core NHIS survey, rather than to the CAM supplement. Thus, they were made without regard to supplement use and before the respondents were asked to consider supplement use. The variable indicating cognitive problems represented affirmative responses to the question, “During the past 12 months, have you had memory loss or loss of other cognitive functions?” or the question, “Have you ever been told by a doctor or other health professional that you had dementia, including Alzheimer’s Disease?” Another set of variables also identified cognitive problems. Participants were also asked whether they had difficulty with 9 physical activities such as “walking a quarter of a mile, about 3 city blocks,” and 3 social activities such as “go out to things like shopping, movies, or sporting events.” Those who said they had difficulty with any of these activities were then asked, “What condition or health problem causes you to have difficulty with [the activity]?” The individual conducting the survey then selected standardized names for the conditions the participant mentioned, from a list of 35 conditions. One of these was “senility,” which we considered to indicate a cognitive problem.
Control Variables
We used the Andersen model of health services to select control variables and organize their presentation. 43 Since little is known about supplement use for cognitive health, results for the control variables are of interest. Developed to study factors that contribute to the use of acute care health services, the Andersen model has been applied to use of CAM, including supplements. 44 –48 The model suggests that supplement use is determined by 3 sets of factors: predisposing factors, enabling factors, and need factors. 43 Predisposing factors measured in the present analysis were gender, age, marital status, ethnicity, and education. Age was coded to create 2 categories of young adults (19-29 and 30-39), 2 of midlife adults (40-54 and 55-64), and 3 of older adults (65-74, 75-84, and 85+) to represent a life course perspective about cognitive health and to account for a possible nonlinear relationship between age and use of supplements for cognitive health. 49
Five groups represented self-reported ethnicity: African American, Asian, Hispanic, non-Hispanic White (hereafter White), and other. Four categories represented marital status: married, separated, divorced, or widowed; never married; and marital status unknown. Education groups were defined by the highest education level completed: grade 8 or less; grades 9 to 12; high school diploma or general equivalency diploma; associate’s degree; bachelor’s degree; master’s degree, MD, or PhD; or education missing.
The model included 3 enabling factors: income, health insurance, and region of residence. Household income was measured by the income-to-need ratio, a standard measure that adjusts income for household needs based on family size, differing needs for older family members and children, and total household income, using federal guidelines for establishing the threshold that defines poverty. 50 Each individual was represented in 1 of 6 income-to-need groups: <1, 1 to <2, 2 to <3, 3 to <4, 4 to <5, and 5+, with <1 being the poorest and 5+ being the wealthiest. Families with an income-to-need ratio of 1 have exactly the income that defines the federal poverty threshold for someone in similar family circumstances. Those with an income-to-need ratio of 2 have twice that level of income.
Each individual’s health insurance status was represented by 1 of 7 categories: private insurance; Medicare only; Medicare Plus (Medicare with supplementary insurance); Medicaid only; both Medicaid and Medicare (dual eligible); other public health insurance such as military coverage; and uninsured. Each individual’s region of residence was identified as the Northeast, Midwest, West, or South.
The model included 11 measures of health need. Self-reported health was represented as excellent, very good, or good health; and fair or poor health. Health status change compared self-rated health on the day of interview with the same measure a year earlier, measured as better, same, or worse. An additional category identified individuals with missing values for this variable.
Seven dummy variables represented groups of chronic health conditions. We identified the chronic condition groups and the variables that defined them using information in the NHIS; details are available. 47,48 The condition groups were musculoskeletal, endocrine and metabolic, circulatory, depression or depressive symptoms, weight problems, cancer, and nervous and sensory. Two indicators of health risk were current smoker and body mass index (BMI). Four BMI categories were identified using definitions from the Centers for Disease Control and Prevention: underweight, normal weight, overweight, and obese. An additional dummy variable represented individuals with missing BMI information.
Analytical Approach
Analyses included descriptive, bivariate, and multiple logistic regression. All analyses were weighted for national representation and accounted for the survey design. Data were analyzed using SAS 9.1 (Cary, North Carolina). Descriptive results for all variables were calculated for all adults who used supplements specifically for cognitive health. The chi-square statistic compared the values among levels of each variable. We also identified the types of supplements used most commonly for cognitive health.
We assessed variables in the multivariate analysis for multicollinearity using the variance tolerance test. The mean tolerance value was 0.74 (standard deviation 0.17). Two covariates had tolerance values below 0.4: Medicare Plus (0.35), and ages 65 to 74 (0.39). Although all multivariate models involve some degree of multicollinearity, it is not typically considered to be a problem for the analysis when tolerance values are greater than 0.3. 51 Given the much higher average tolerance value in these data, the relatively small standard deviation of such values from their mean, and the small number of variables having even moderately low tolerance levels, we concluded that multicollinearity was not a problem for the analysis.
Results
Sample Characteristics
Table 1 represents 16 784 participants who reported using any CAM, including supplements. They represented about 162 million adults, or about 74% of the adult population of the United States in 2007. Of these, about 15.7% said they had a cognitive problem and used supplements to address it. Another 8.8% of those using any CAM said they did so for cognitive health despite reporting no cognitive problems; they used supplements to prevent such problems.
Number of Respondents and Weighted Number of US Adults Using Dietary Supplements for Cognitive Health, and Their Percentage Among Persons Who Used any Complementary or Alternative Medicine, 2007 a
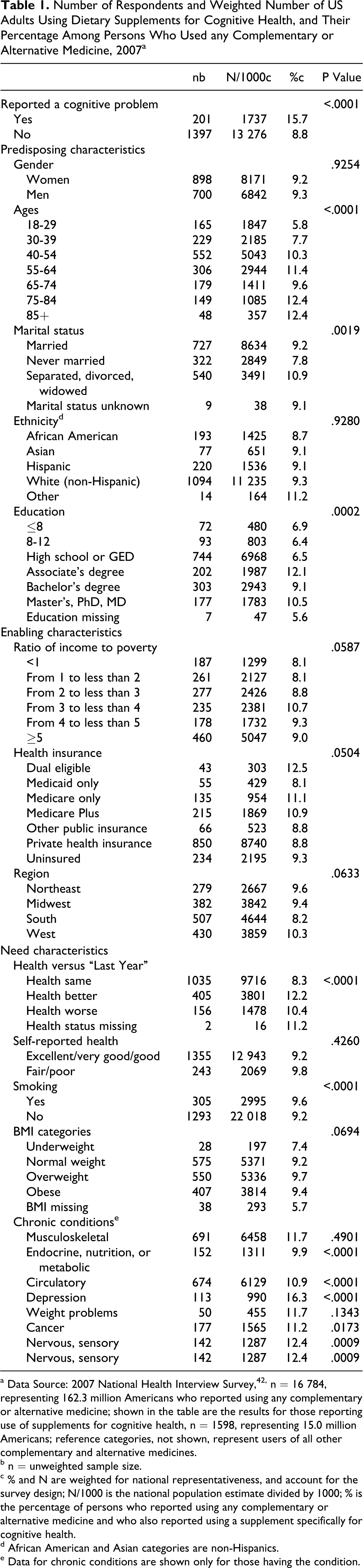
a Data Source: 2007 National Health Interview Survey,42, n = 16 784, representing 162.3 million Americans who reported using any complementary or alternative medicine; shown in the table are the results for those reporting use of supplements for cognitive health, n = 1598, representing 15.0 million Americans; reference categories, not shown, represent users of all other complementary and alternative medicines.
b n = unweighted sample size.
c % and N are weighted for national representativeness, and account for the survey design; N/1000 is the national population estimate divided by 1000; % is the percentage of persons who reported using any complementary or alternative medicine and who also reported using a supplement specifically for cognitive health.
d African American and Asian categories are non-Hispanics.
e Data for chronic conditions are shown only for those having the condition.
There were 149 individuals in this sample who were of age 75 through 84 and used supplements for cognitive health, representing about 1.085 million Americans. (For brevity, and to focus on those using supplements for cognitive health, data representing individuals who used CAM but did not use a supplement for cognitive health are not shown in the table; in the case of age 75 through 84, for example, results for the 1085 individuals at these ages who did not use supplements for cognitive health are not shown, although that group was included in the chi-square analysis represented by the P value.) Weighted for national representativeness, and again using CAM users for the denominator, about 12.4% of individuals in this age group reported using supplements for cognitive health. The P value associated with age, P < .0001, indicates that use of supplements for cognitive health varied significantly by age group in these unadjusted results. This result is consistent with the variation in the observed percentage estimates, where, for example, only 5.8% of those aged 18 through 29 said they used supplements for cognitive health, while 12.4% of the 2 oldest age groups said they did so.
Individuals with associate’s degrees, bachelor’s degrees, and master’s, doctoral, or medical degrees were more likely than others to use supplements for cognitive health, as were residents of the West. Those reporting that their health was currently better than it was a year ago were more likely to use supplements than those who reported their health was now the same or worse. The largest percentage of supplement use for cognitive health was among individuals who reported having depression or depressive symptoms, 16.3%.
Supplements Used Most Often for Cognitive Health
Table 2 shows the 5 herbal and other dietary supplements used most commonly for cognitive health, and the 6 vitamins and minerals used for this purpose. Supplements and vitamins used less commonly for this purpose had small sample sizes and are not reported. Among herbs and other dietary supplements, the most commonly used for cognitive health were fish oil (used by 29% of those using supplements for cognitive health), Ginkgo biloba (23.1%), ginseng (19.1%), pills containing unspecified combinations of supplements (16.1%), and flax oil (12.6%). Of vitamins, multivitamins were the most used (by 58.1% of those using supplements for cognitive health), followed by calcium (16.3%), vitamin C (8.4%), vitamin B (6.3%), vitamin B12 (5.6%), and vitamin E (5.3%). The specific herbs, vitamins, and supplements used for cognitive health were similar for those with and without cognitive problems. In a result not reported in the table, of those who used a dietary supplement specifically for cognitive health, 38% said they did not tell their health care providers.
Vitamins, Minerals, Herbs, or Other Dietary Supplements Used for Cognitive Health, United States, 2007 a
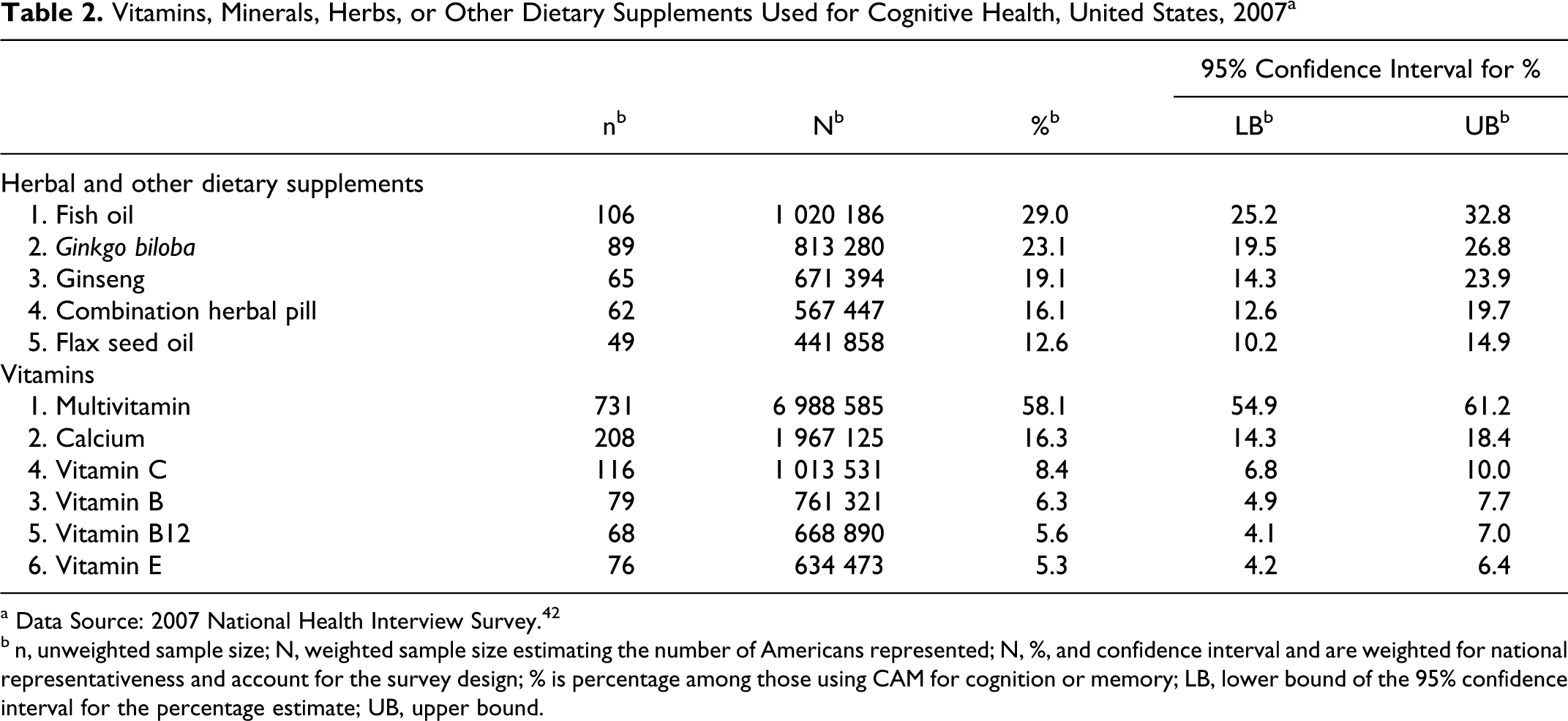
a Data Source: 2007 National Health Interview Survey. 42
b n, unweighted sample size; N, weighted sample size estimating the number of Americans represented; N, %, and confidence interval and are weighted for national representativeness and account for the survey design; % is percentage among those using CAM for cognition or memory; LB, lower bound of the 95% confidence interval for the percentage estimate; UB, upper bound.
Adjusted Results
Table 3 reports results of the multivariate logistic analysis focused on adults who used supplements, predicting that their supplement use was for cognitive health. For each result, the table shows the odds ratio (OR) and the upper and lower bounds of the 95% confidence interval (CI). Adults reporting a cognitive problem were more likely than others to use supplements for cognitive health (OR 1.77, CI 1.39-2.25), indicating that adults are considerably more likely to use supplements to treat or cure cognitive problems than to prevent them.
Among the control variables, several characteristics were associated with lower adjusted odds that supplement use would be for cognitive health. Among the predisposing characteristics, younger individuals and those with less education were substantially less likely to use supplements for cognitive health, compared with their respective reference categories, which were those aged 40 through 54, and those with high school diplomas. An examination of overlapping confidence intervals among the age categories, however, suggests that for the most part only the youngest age category, aged 18 through 29, had significantly lower odds of using supplements for cognitive health than those in age groups other than the reference category. In the enabling characteristics, adults in the lowest 2 income categories were substantially less likely to use supplements for cognitive health than those with income-to-need ratio of 3 to 4. Among the need factors, adults who reported that their health was better currently compared with a year ago were more likely to use supplements than those who reported that their health was the same (OR 1.55, CI 1.34-1.78). Adults who reported depression or depressive symptoms were more likely than those without these conditions to say that they used supplements for cognitive health, as were those with musculoskeletal problems.
Results of Logistic Regression Predicting Use of Dietary Supplements for Cognitive Health, 2007 a
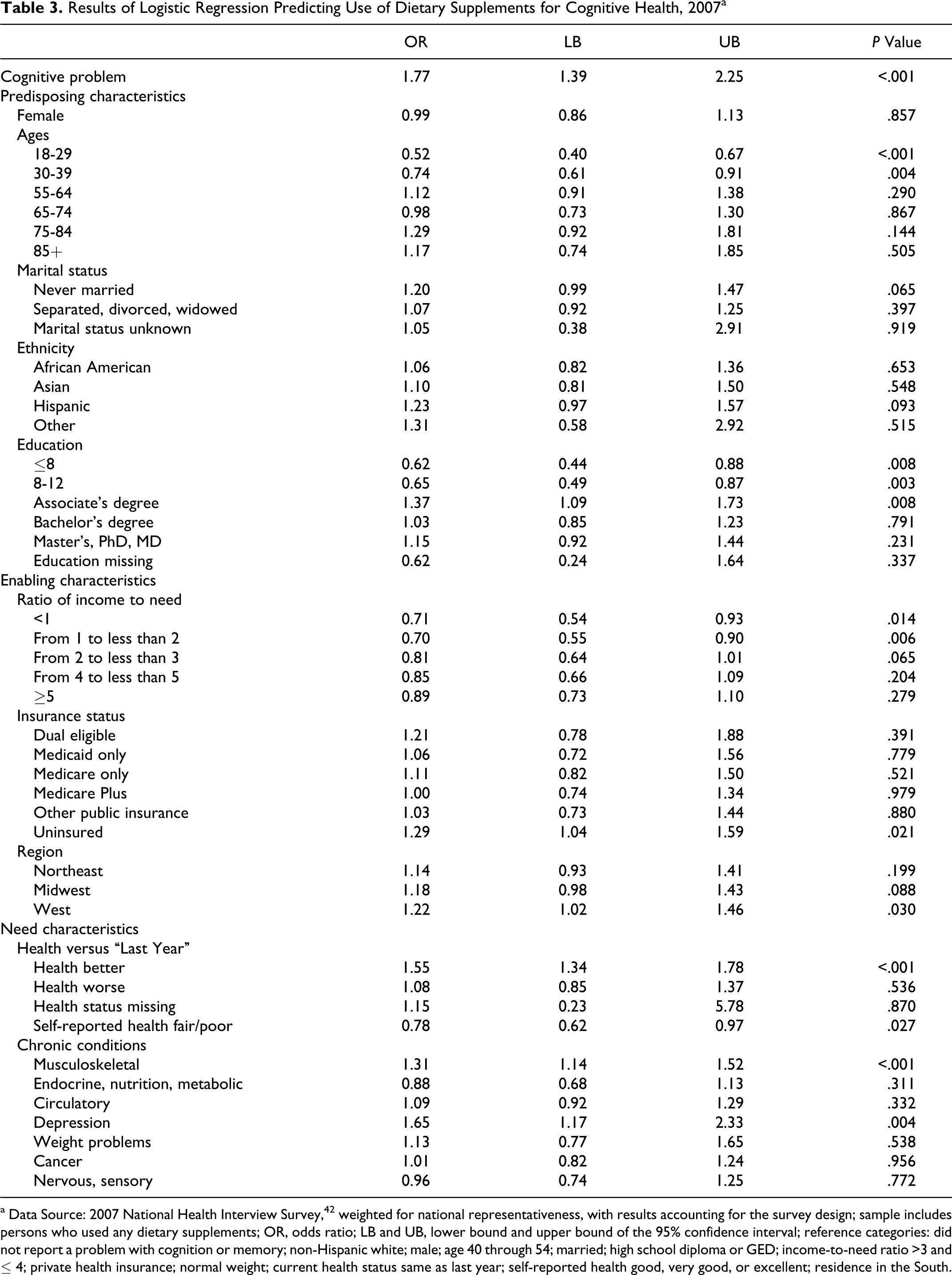
a Data Source: 2007 National Health Interview Survey, 42 weighted for national representativeness, with results accounting for the survey design; sample includes persons who used any dietary supplements; OR, odds ratio; LB and UB, lower bound and upper bound of the 95% confidence interval; reference categories: did not report a problem with cognition or memory; non-Hispanic white; male; age 40 through 54; married; high school diploma or GED; income-to-need ratio >3 and ≤ 4; private health insurance; normal weight; current health status same as last year; self-reported health good, very good, or excellent; residence in the South.
Discussion
We studied use of dietary supplements for cognitive health in a nationally representative sample of individuals who responded to the 2007 NHIS and a supplement to that survey on CAM 42 . A substantial number of adults in the United States use supplements either “to prevent” cognitive problems or “to treat or cure” them. Regarding our first research question, the most frequently used supplements were fish oil, Ginkgo biloba, ginseng, pills that contained a combination of supplements and flax seed oil. The most commonly used vitamins and minerals were multivitamins, calcium, and vitamins B, B12, and E. The findings for the specific types of supplements used for cognitive health in the present study are generally similar to the results of 2 previous studies. 28,29 Some of the vitamins and herbs frequently used for cognitive health in the present study, such as ginkgo and ginseng, may interact with conventional medications often taken by older adults. 27,30
Results suggested that about 15 million Americans used dietary supplements specifically for cognitive health. Regarding our second research question, 38% of them did not discuss that use with their health care providers. It should be noted that providers may not often ask patients about supplement use. Thus, it may be inaccurate to infer that those who did not report supplement use to providers believed that information would be viewed negatively. They may not have discussed this use simply because they were not asked about it. It has been suggested that health care providers should ask patients about their supplement use, so they can advise patients as needed about the potential for adverse interactions with conventional medicines. 29,39 Consistent with our hypothesis for our third research question, adjusted results showed that adults who had cognitive problems were substantially more likely to use supplements for cognitive health than those without cognitive problems. 5,6,9 Thus, adults were more likely to use supplements to treat or cure dementia than to prevent it.
In other findings of interest, in unadjusted results younger adults were less likely to use supplements for cognitive health than adults at middle age or older ages. 49 However, in adjusted results only the youngest age group, aged 18 through 29, showed evidence of less supplement use than most older age groups. Adults with less than a high school education were less likely to use supplements for cognitive health than those with a high school degree. Those with lower income were less likely to use supplements for cognitive health than adults with more income. Adults with depression or depressive symptoms were more likely to use supplements for cognitive health than those without these conditions. Similarly, those with musculoskeletal conditions were more likely than others to use supplements for cognitive health. Collectively, the results for the predisposing, enabling, and need factors were consistent with previous research on the use of CAM, including supplement use. 32,44,48,52
Adults who reported that their health was now better than last year were more likely to have used supplements for cognitive health than those who said their health was the same. While this result may suggest an association between supplement use and improved general health, the study design and the characteristics of our data suggest caution regarding that interpretation. Our data were cross-sectional and self-reported. While these data are appropriate for studying the use of supplements, they have limited usefulness for studying the efficacy of supplements. Moreover, the question about supplement use asked about the use “during the past 30 days,” which may be unrelated to improvements in general health during the past year. Thus, this result provides little information about the potential efficacy of supplements for health.
We acknowledge study limitations. All information was self-reported. Recall error is a possibility. However, limiting the recall period for supplement use for cognitive health to the past 30 days is likely to limit recall error. Information about cognitive health was also limited to self-reports. The NHIS attempted to enhance validity by asking participants whether a physician or other health care provider had told them they have “dementia, including Alzheimer’s disease,” and whether cognitive problems limited activities. Self-reported cognitive problems included self-reports of “memory loss or loss of other cognitive function.” Participants may have reported such loss even if it did not affect them seriously with cognitive impairment or dementia. This concern is not central to our study purpose because even those with mild cognitive problems may seek treatment or cure, as may those who simply believe they have such problems. Thus, we studied individuals’ stated purpose for using supplements, rather than objective measures of use responding to diagnosed need.
Another consideration is that participants could report using up to 2 types of herbs and 2 types of vitamins. As a result, supplement use may be underestimated, as any supplements used beyond the first 2 are unmeasured. The data are cross-sectional. Typically cross-sectional analyses do not provide a basis for inferring causality. In the present analysis, however, respondents identified the reasons that prompted their supplement use. Although inferences about causality depend on participants’ accurate assessments of their own motivations, in general it seems reasonable to judge that most respondents believed they used supplements for the reasons they provided. Finally, although many individual studies offer evidence for benefits of supplements to promote cognitive health, 10,14 –18 the data available in the NHIS did not allow us to examine the safety or efficacy of any supplement for cognitive health.
Baby boomers are aging. It is likely that a growing number of aging adults will become concerned about cognitive health. In the absence of effective conventional medicine to prevent or treat dementia, and with the dramatic increased use of dietary supplements generally, more adults in the United States and elsewhere may turn to supplements for cognitive health. Provisions of the Patient Protection and Affordable Care Act, enacted in 2010, emphasizing the use of interdisciplinary teams of health care providers including licensed practitioners of CAM, may increase access to supplements and to knowledge about their potential value. 53 The present study showed that a substantial number of adults in the United States use supplements for cognitive health. Adults were substantially more likely to use supplements to treat or cure cognitive problems than to prevent them.
Footnotes
Portions of preliminary results of this study were presented as a peer-reviewed poster at the annual meetings of Academy Health, Chicago, IL, June 28-30, 2009, titled, “Use of Complementary or Alternative Medicine (CAM) to Prevent or Treat Cognitive Problems and Communication about CAM Use with Health Care Providers.” Other portions of preliminary results were presented as a peer-reviewed poster at the annual meetings of the Gerontological Society of America, Atlanta, GA, November 18-22, 2009, titled, “Use of Complementary and Alternative Medicine for Cognitive Function: Results of a National Survey.”All analyses, interpretations, and conclusions in this study are the authors’. The National Center for Health Statistics collected the data and made it available. However, the NCHS is not responsible for analyses, interpretations, or conclusions based on those data.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.