
Abstract
Introduction
One of the most prevalent neurological disorders is dementia. The number of demented patients all over the world is expected to grow from 24.3 million in 2001 to 81.1 million in 2040 as a result of increased life expectancy. 1 In Western countries, Alzheimer’s disease (AD) and vascular dementia (VaD) are the most common forms of dementia, with respective frequencies of 70% and 15% among all patients with dementia. 2 Atrial fibrillation (AF) is a well-known risk factor for stroke in the elderly individuals. 3,4 In individuals between 80 and 89 years of age, AF is responsible for approximately one third of all stroke cases. 5 Also, clinically silent cerebral infarctions were diagnosed in 13% to 26% of patients with AF. 6
Data from observational studies show that AF plays a role in the pathogenesis of cognitive dysfunction. In the Rotterdam study, a positive association was found between AF and impaired cognitive functions (odds ratio [OR] = 1.7, 95% confidence interval [CI] 1.2-2.5) or dementia (OR = 2.3, 95% CI 1.4-3.7). 7 In cross-sectional studies, AF was associated with cognitive dysfunction, independent of cardiovascular risk factors or stroke. 8, 9 In longitudinal studies assessing the link between AF and dementia, a high Kaplan-Meier cumulative rate of dementia of 22.5 per 1000 person-years was found, 10 whereas in the general population, the incidence of dementia was 6.8 per 1000 person-years. 11 There is a controversiality regarding the role of AF as a risk factor for development of dementia. Several studies have shown that AF predicts the onset of dementia after stroke, 12,13 whereas others did not found such an association. 14,15 There are many possible mechanisms that might explain the association between risk of dementia and AF. Cerebral hypo perfusion due to fluctuations in the cardiac output and thromboembolic damage are involved.16 Cerebrovascular disease often coexists and overlaps with AD and silent micro infarcts may contribute to AD development. 17
The present study aimed to evaluate whether, and to what extent, AF is interrelated to the overall cognitive status in a large group of patients with ischemic stroke, controlling for the presence of some prevalent comorbidities characteristic of such patients. We hypothesized that ischemic stroke patients with AF might show lower Mini-Mental State Examination (MMSE) scores, compared with patients without AF. Such data would assist in identifying factors associated with cognitive decline and may also assist in evaluating rehabilitation potential and disability risk.
Methods
Hypothesis
A diagnosis of AF at admission to a rehabilitation ward would assist in predicting cognitive ability among patients with ischemic stroke.
Design and Setting
The Geriatric Rehabilitation ward at the Sheba Medical Center is a 36-bed unit. This ward utilizes an interdisciplinary team approach, where representative from geriatrics, physiotherapy, nursing, rehabilitation therapies (physical, occupational, and speech), social services, and psychology meet twice a week to evaluate the status of each patient. During these meetings, a treatment plan is established and monitored with the purpose of coordinating and integrating staff activities and promoting effective rehabilitation. The patients undergo a typical physical and occupational therapy (6 hours for 6 days per week).
Study Population
This retrospective study included 919 patients with ischemic stroke. Two hundred and twelve patients were excluded due to severe aphasia or cognitive and behavioral impairments that did not allow for a cognitive assessment using the MMSE tool.
Patients were consecutively admitted to our ward during a 7-year period, after a short stay in the departments of internal medicine or neurology. Stroke was diagnosed on the basis of clinical presentation of acute onset of focal neurological signs. Computed tomography or magnetic resonance imaging scans were performed in all cases to confirm the presence of ischemic stroke.
Primary inclusion criteria, other than ischemic nature of stroke, included stable medical status (enabling active rehabilitation treatment) and a length of stay and nature of ischemic stroke in the rehabilitation ward of more than 7 days (assuming that a shorter extent of rehabilitation is meaningless). The study sample did not include patients with residual brain damage due to infection, trauma, or surgery and patients with space occupying lesions or hemorrhagic stroke.
The presence of arterial hypertension, ischemic heart disease (manifested as stable or unstable anginal syndrome), AF, previous stroke, diabetes mellitus, and hyperlipidemia were established by medical history, obtained by interview and a complete physical examination. The variable "dementia" was a prestroke diagnosis obtained from the patients’ medical files upon admission to the ward.
Cognitive Assessment
Patients’ cognitive status was assessed by the 18 MMSE within 1 week after admission to the rehabilitation ward. The MMSE scores lower than 24 points were considered suggestive of cognitive impairment. 19 Patients were not excluded on the basis of lower limits on the MMSE scores.
Atrial Fibrillation Assessment
The presence or absence of AF was established upon registry data positive of AF (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code 427.31). We included patients with a diagnosis of AF (whether chronic or paroxysmal AF) on index day.
Statistical Analysis
Depending on the presence/absence of AF, patients were divided to 2 groups. Comparisons between the groups of patients, as defined above, regarding demographical and clinical characteristics, were performed using t tests and chi-square tests. The association of sociodemographic characteristics, AF, and medical conditions to the cognitive status was performed in 2 models: (a) when the full MMSE scale was used as an outcome, a linear regression analysis was performed; (b) when MMSE score was dichotomized at the 24 points cutoff, a logistic regression was applied. The statistical significance level was set to .05. The SPSS for Windows software, version 11.0, was used for these analyses.
Results
The data of 707 patients with consecutive ischemic stroke (age range 48-96) admitted during a 7-year period were available. The clinicodemographic characteristics of these patients are shown in Table 1. Mean age was 74.11 ± 9.29 years, mostly men (57.1%), whereas mean MMSE scores were 22.45 ± 5.42 (Table 1). One hundred and twenty-six patients (17.8%) were diagnosed to have AF. There were no statistically significant differences between these patients and the remaining nonatrial fibrillation patients (n = 581) by means length of stay, hypertension, ischemic heart disease, dementia, or previous stroke. Age, gender, Parkinson disease, and MMSE scores emerged as the only statistically significant parameters differing between those with and without AF (Table 1). Since an MMSE score ≥24 defines group of patients without cognitive impairment, we performed a linear regression analysis to test for predictors of MMSE scores. This showed (Table 2 ) that AF (P = .003), older age (P < .001), female sex (P = .001), diabetes (P = .003), and dementia (P < .001) were independently associated with lower MMSE scores. None of the other variables that we tested, including arterial hypertension, ischemic heart disease, and Parkinson’s disease, were predictive of MMSE scores. In addition, logistic regression analysis predicting for cognitive impairment (MMSE < 24), while controlling for confounding variables, showed that AF (OR 1.6; CI 1.03-2.47, P = .03) and female sex (OR 1.57; CI 1.11-2.2, P = .009) were associated with increased risk of cognitive impairment (Table 3 ).
Clinicodemographic Characteristics of Patients by Atrial Fibrillation a
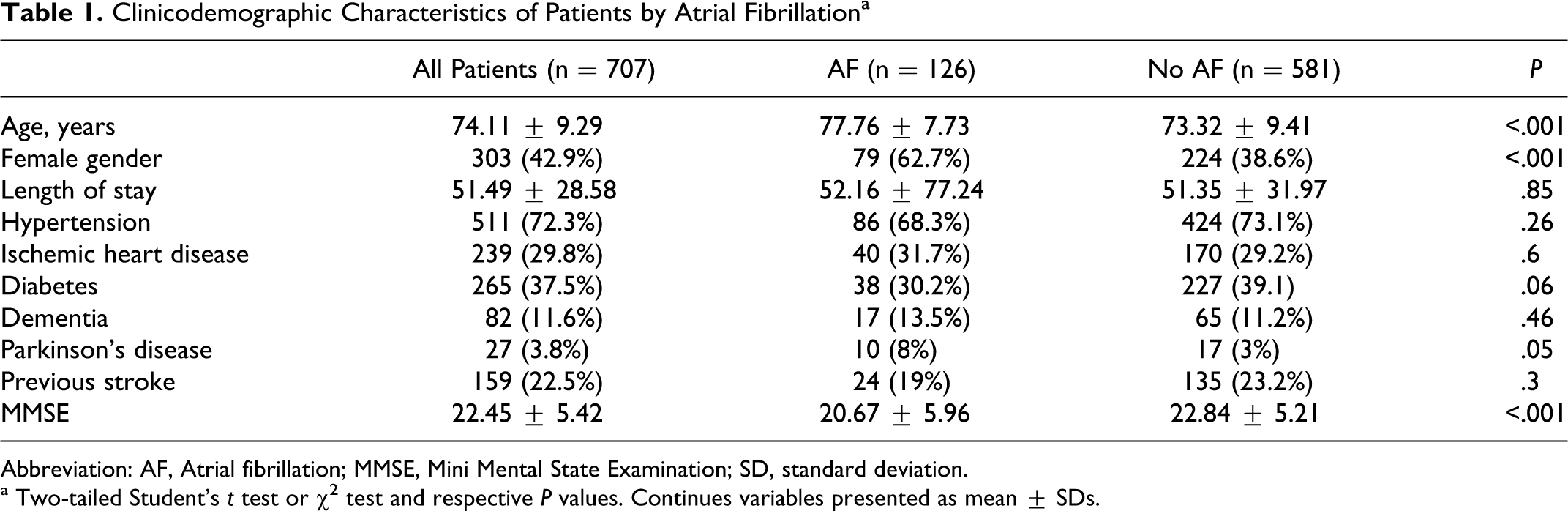
Abbreviation: AF, Atrial fibrillation; MMSE, Mini Mental State Examination; SD, standard deviation.
a Two-tailed Student’s t test or χ 2 test and respective P values. Continues variables presented as mean ± SDs.
Regression Coefficients of Clinical Variables and MMSE Scores
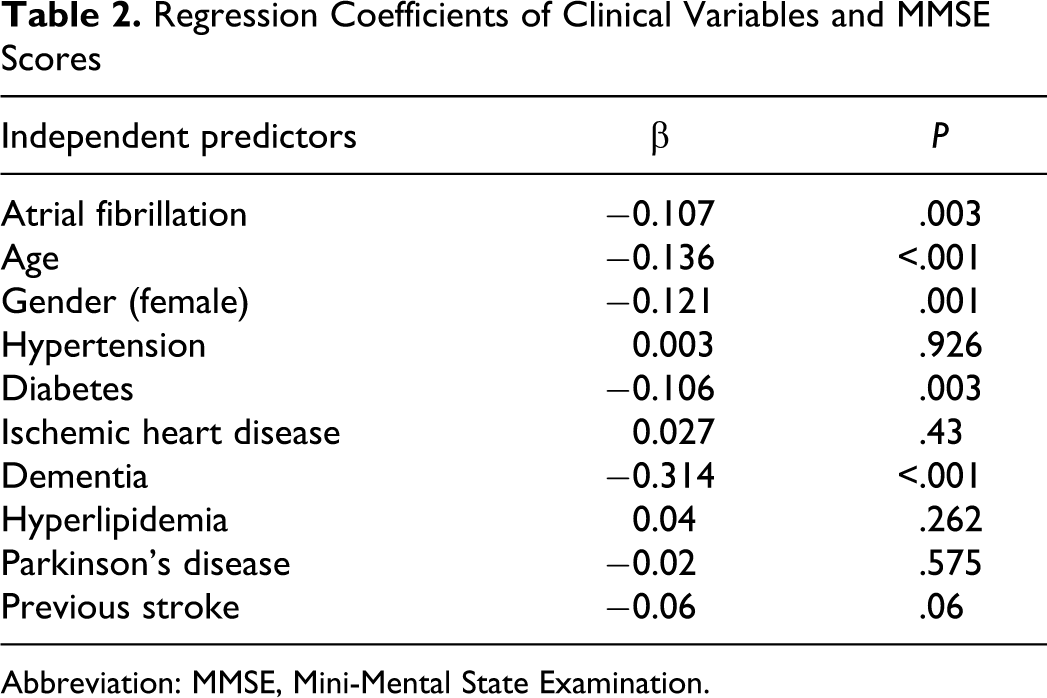
Abbreviation: MMSE, Mini-Mental State Examination.
Coefficients of Studied Variables and Cognitive Impairment (MMSE < 24) a
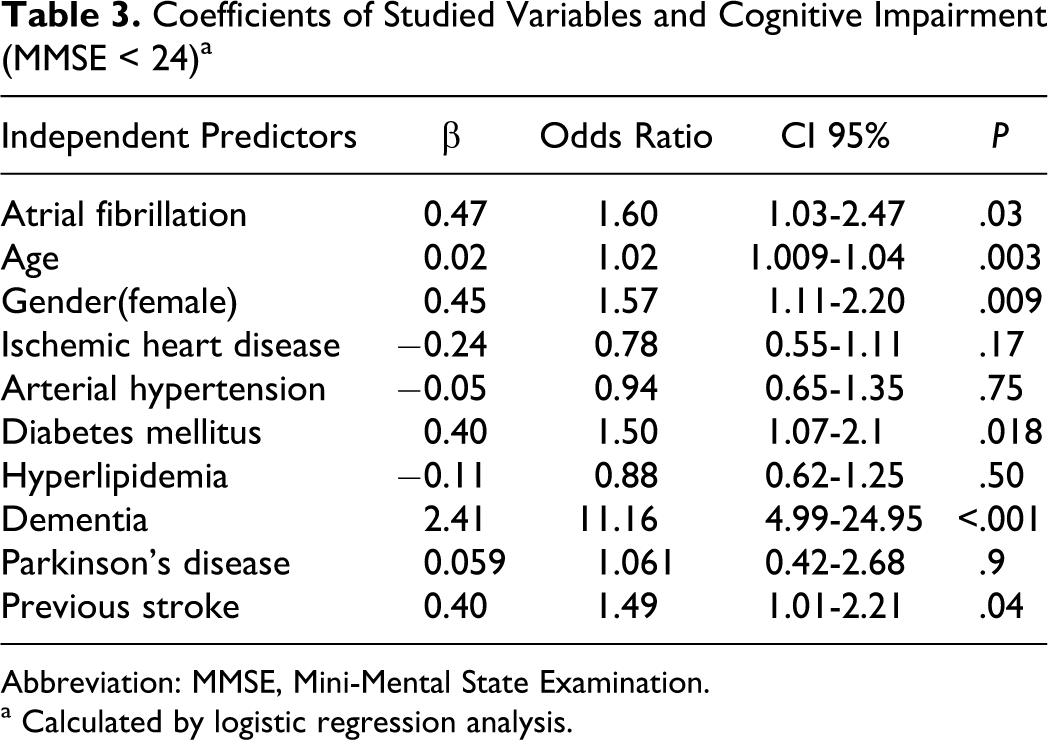
Abbreviation: MMSE, Mini-Mental State Examination.
a Calculated by logistic regression analysis.
Discussion
The area of AF and cognitive impairment is fairly new with research developments currently being made. 20–22 The present study focused on the possible interrelation of AF and cognitive impairment, in a group of patients with a recent onset ischemic stroke. Our data show that a diagnosis of AF upon admission is associated with lower MMSE scores, thus, indicating cognitive impairment. After multivariate adjustment (for age, gender, arterial hypertension, diabetes mellitus, ischemic heart disease, dementia, Parkinson’s disease, previous stroke), the association between AF and cognitive decline remained evident. These data are consistent with previous studies, showing similar findings in nonstroke affected patients and are not surprising considering that patients with nonrheumatic AF do suffer more severe, disabling and fatal strokes. 5,23 It was found that among patients without previous stroke, AF was associated with significantly lower MMSE score compared with patients with sinus rhythm 24 and hippocampal atrophy. 25 In a cross-sectional study, men with AF had lower mean cognitive scores than men without AF and the exclusion of patients with stroke did not alter this relationship. 24 In a prospective 9-year follow-up study, AF was a significant risk factor for stroke but not for dementia in patients aged 85 years or older. 25
Several important limitations of the present study are worthy of mention, resulting from its retrospective nature and the fact that this is a single-site study. First, it is unclear how representative patients at a rehabilitation ward are of the overall poststroke population. Also, despite adjustment made for important confounders, still other could have been considered, in particular those relating to other illnesses. A validation study of registry data, including accuracy of source documents and the level of skill and care applied in abstracting data, was not performed. This article may also be criticized for not using a neurological severity score considering that stroke patients with AF may suffer greater neurological disability. 26,27
Finally, longitudinal follow-up data would contribute to a better understanding of the interrelations between AF, stroke, and cognition, in later stages.
Despite these limitations, the present study is advantageous in the sense that it comprised a relatively large sample of patients, focusing on the possible role of AF on cognitive level among ischemic stroke patients, thus, is more likely to represent day-to-day clinical practice, rather than just a trial population.
We conclude that patients with AF who suffer ischemic strokes have lower MMSE scores and may therefore be at increased risk of adverse rehabilitation outcomes. These findings should be considered when selecting and developing resources for patients with stroke with AF.
Footnotes
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.