
Abstract
Although the term wandering is routinely used by clinicians, researchers, and informal caregivers (ICs), the meaning of this term varies depending on the source of the definition and the context in which it is used. The purpose of this study was to examine the terms ICs used to describe different scenarios that have been identified in literature as “wandering,” determine their perception of risk, and compare their definitions of wandering with the perspectives of researchers. Structured interviews were conducted with 128 ICs of older adults with dementia. Informal Caregivers rarely used the term wandering to label different scenarios that had been previously identified in the literature as wandering. Responses to a survey of 17 wandering experts did not reflect agreement on a definition for wandering. These findings suggest that a broad set of terms should be used to describe this potentially dangerous behavior when health care providers communicate with ICs.
Introduction
The term wandering is routinely used by clinicians, researchers, and informal caregivers (ICs) to describe a behavior associated with dementia that has been noted to be linked with earlier institutionalization, 1 anxiety, physical injuries, and death. 2 However, the meaning of this term varies depending on the source of the definition and the context in which it is used. In response to the array of published definitions, descriptors, and impressions of wandering, Algase and colleagues proposed a provisional definition for dementia-related wandering, delineating it as “a syndrome of dementia-related locomotion behavior having a frequent, repetitive, temporally-disordered and/or spatially-disoriented nature that is manifested in lapping, random and/or pacing patterns, some of which are associated with eloping, eloping attempts, or getting lost unless accompanied.” 3
However, the term wandering continues to be used differently from the proposed definition with its meaning influenced by the source, sample, and environment. For example, researchers have used wandering as a blanket term that includes several behaviors such as nighttime walking, aimless walking, excessive activity, and shadowing the caregiver. 4 Others have narrowed the scope of the definition and defined wandering based on a particular environment. In nursing homes, wandering has been defined as aimless and disoriented ambulation, which may include pacing, lapping, or random ambulation. 5 Community-dwelling older adults with dementia have been identified as “… a wanderer if aberrant motor behavior (like pacing up and down or spinning around) was present, if the subject was known to wander aimlessly, and if the caregiver confirmed that this behavior was frequent (at least several times a week).” 6 Nurses have labeled a behavior as wandering if it exposes the person with dementia to harm or does not fit with the established boundaries, limits, or obstacles. 7
Some researchers have debated whether one of the descriptors included in Algase’s definition, “getting lost unless accompanied,” is a separate behavioral outcome and distinct from wandering. Researchers have identified that the antecedents to “getting lost unless accompanied” as routine independent walks in the community that may lead to becoming lost, an inability to return home independently, or getting separated from a caregiver while out in the community. 8 Furthermore, these lost instances were not preceded by abnormal locomotion patterns typical of wandering. 9 Notably, these findings do not appear to fit with the aforementioned provisional definition of wandering.
While the definition of wandering is still under debate by researchers and professionals, one of its limitations is that it does not take into account how ICs for people with dementia define wandering. To date, research has not examined ICs’ perception and understanding of the term wandering. What the literature does show is that some ICs are concerned about the potential for their care recipients (CRs) to wander or become lost. In a study examining ICs’ perception of risk, about a quarter of the study participants were worried about potential wandering or becoming lost events. Notably, almost 40% of this sample reported a wandering or a lost event during the past year. 10 These findings suggest that there is a gap in how ICs and health professionals perceive the term wandering. Knowledge of ICs’ perceptions may have important implications for managing this specific behavior in a CR.
The current study had multiple goals. The primary goal of the study was to identify and explore inconsistencies between ICs’ and wandering experts’ use of the term wandering. A secondary goal was to understand how IC’s perceived instances in which they did not know the whereabouts of their CR. Instances where the CR was lost will be referred to as a “missing incident” throughout the remainder of this article. 11 The final goal was to compare ICs’ understanding of the word wandering with that of researchers with an expertise in wandering behaviors and missing incidents. Improved clarity of the term wandering has the potential to prevent miscommunication in research and clinical settings and to enhance the safety and well-being of older adults with dementia and their ICs. This is particularly important because the antecedents and interventions for wandering behaviors and missing incidents are different.
Methods
Early Trajectory of Wandering in Veterans With Mild Dementia
The current study was conducted as an adjunct to an ongoing study, Early Trajectory of Wandering in Veterans With Mild Dementia (ETW). ETW was a 2-year longitudinal study that recruited older adults with a diagnosis of mild dementia who were living in the community and their ICs; both participants provided informed consent. During the informed consent process, the term wandering was not expressly defined but was used interchangeably with the phrase “getting lost or separated from their families.”
At the baseline of the ETW study, participants had a Mini-Mental State Examination 12 score of 18 or above and a Clinical Dementia Rating scale 13 score of 0.5 or 1.0, both suggesting the presence of mild dementia. The study procedures included 4 study visits over a 2-year period that involved neuropsychological testing and ambulation monitoring. Bimonthly phone calls were conducted between the study visits. A total of 138 dyads (ie, veterans with dementia and their ICs) were enrolled in the ETW.
Current Study
In year 2 of the ETW study, during one of the bimonthly telephone calls, ICs were asked to participate in a brief interview for this study. Ten dyads dropped out of the ETW study at the start of the current study for reasons that included death (n = 7), relocation (n = 1), and worsening of illnesses (n = 2). All the remaining caregivers (n = 128) agreed to participate in a telephone interview for the current study.
IC’s assessment of wandering
Utilizing a cross-sectional design, structured interviews were conducted with ICs of older adults with dementia. The interviews, conducted by the first author, on average lasted approximately 10 minutes. Each IC was asked 9 open-ended and yes/no questions about the terms they would use to describe wandering and missing incidents using 4 different scenarios (unknown location, driving to a location and not returning when expected, walking to a location and not returning when expected, and becoming lost; see Appendix A). Scenarios were selected because they had been identified as wandering incidents in the literature. If an IC endorsed that they had personally experienced a scenario (ie, driving to a location and not returning when expected), they were asked, “What terms did you use to describe this occurrence?” ICs that had not experienced a specific scenario were asked to consider the scenario hypothetically and report their concerns. For the final question of the interview, ICs were asked to provide their own definition of the term wandering.
After the interviews were completed, the quantitative data were analyzed using SPSS. Qualitative responses were reviewed and evaluated for common themes by the 3 authors and 4 gerontologists with expertise in dementia care. Each reviewer independently examined the ICs’ responses. Following the initial review and a formal group review process, similar themes were identified and aggregated. For example, aimless walking and walking without a purpose were combined into one theme. A subsequent review of all interview data resulted in complete agreement among the reviewers on the final 12 themes.
Wandering expert assessment of wandering
Members of the International Consortium on Wandering and Missing Incidents were invited to participate in this study. This 24-member committee meets semiannually to discuss and conduct research on wandering. Most committee members are full-time researchers in academic and clinical settings. Members were contacted by e-mail and invited to participate in the Internet-based survey. The survey presented the 12 themes that were derived from data collected from IC interviews (see Table 3 for a list of items). The wandering experts were asked to select all themes that were consistent with their definition of wandering. Additionally, they were asked to describe how they would explain wandering to an IC (see Appendix B). The average survey took less than 5 minutes to complete. Responses were tabulated on the Internet-based survey Web site. Statistical analysis of responses consisted of frequency distributions and means ± standard deviations (SD).
Results
Caregiver Component
Demographic characteristics of the ICs were collected during the baseline interview of the ETW (see Table 1 ). Typical of the Veterans Health Administration population, most of the ICs were wives (79.0%, n = 101) of male veterans (90.0%, n = 115) and were older (n = 70, ±10.9) than the national average age (51 years) for ICs of persons with dementia. 14
Care Recipient and Caregiver Demographics at Baseline Assessment of ETW a
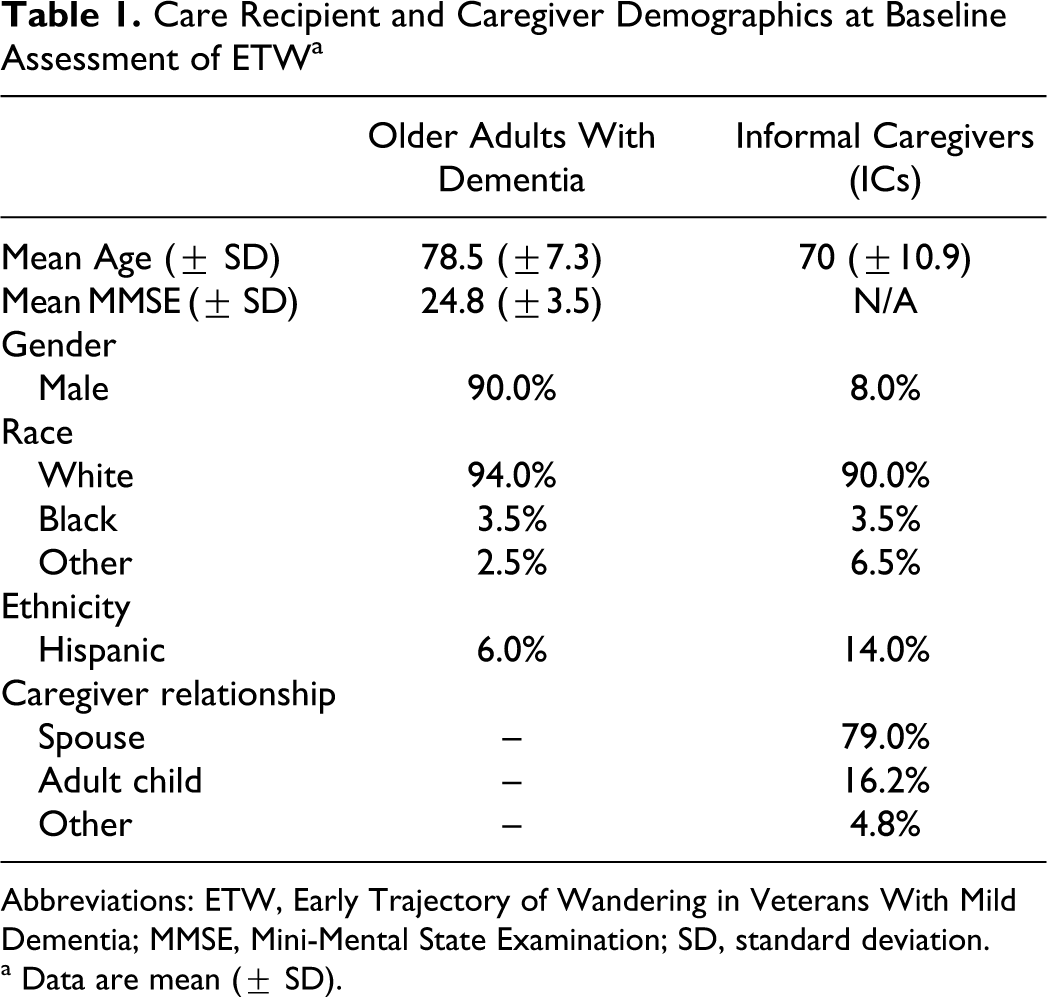
Abbreviations: ETW, Early Trajectory of Wandering in Veterans With Mild Dementia; MMSE, Mini-Mental State Examination; SD, standard deviation.
a Data are mean (± SD).
Percentage of events in past year
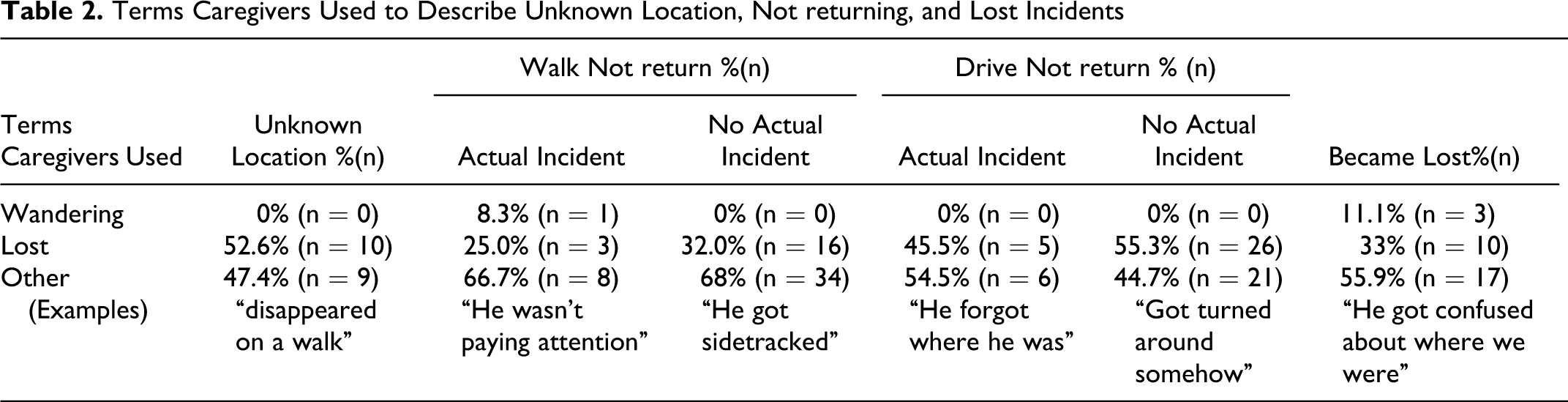
When ICs were asked, “During the past year, was there ever a time you did not know where your CR was?” 15% (n = 19) of ICs indicated yes (these are referred to in Table 2 as actual incident). However, later in the interview, 23% (n = 27) of the ICs indicated that their CR had become lost at least once in the past year. At the conclusion of the interview when each IC was asked whether the CR was a wanderer, only 5% (n = 6) of ICs endorsed this item (see Table 2).
Terms Caregivers Used to Describe Unknown Location, Not returning, and Lost Incidents
Terms ICs used to describe scenarios
When ICs were asked, “During the past year, was there ever a time you did not know where your CR was?” About 15% (n = 19) of ICs indicated they had experienced not knowing the CR’s location. None of these ICs described this missing incident as wandering. The most common term ICs used was “lost” (53%, n = 10).
When asked, “Has your CR ever gone out on a walk and not returned home at the time you expected?” about 10% (n = 12) of ICs indicated that this had happened. One of the 12 ICs described this situation as wandering and 3 described it as lost. Informal caregivers of CR who had not taken a walk without returning were asked to imagine that their CR had taken a walk and not returned and to describe the event as if they were talking to a friend about what had happened. None of these caregivers identified the behavior as wandering. The most common term ICs used was “lost” (32%, n = 16).
Informal caregivers of CRs who still drove in the community were asked, “Has your CR ever driven somewhere and not returned when expected?” Only 8.3% (n = 11) of ICs responded yes. None of these ICs described this incident as wandering. Nearly half (45%, n = 5) used “lost.” Informal caregivers of CRs who had not driven somewhere without returning were asked to imagine that scenario and to describe the event as if they were talking to a friend about what had happened. None of these caregivers identified the behavior as wandering, but a little more than half (55%, n = 26) of the ICs described it as lost.
Nearly a quarter (23.5%, n = 30) of the ICs positively responded when asked, “During the past year, was there ever a time when your CR became lost?” Three of the 30 ICs identified this incident as wandering, but the most common term ICs used was “lost” (33.3%, n = 10).
Of the ICs that indicated that they had not experienced a time when they did not know the location of their CR, 38.5% (n = 42) were concerned that this type of situation would happen with their CR at some point in the future. Of the ICs that indicated they had not experience a time when their CR had become lost, a little over a third (34.7%, n = 34) were concerned that this type of situation would happen with their CR at some point in the future.
Prevention efforts
About half (48.5%, n = 62) of the ICs acknowledged the possibility that their CR might become lost due to memory problems, and about 30% (n = 18) of these ICs said they would consider institutionalization if their CR started to get lost. The most common methods ICs indicated they would use to prevent this outcome were watching the CR closely (37.0%, n = 23), using an identification bracelet (22.6%, n = 14), installing exit door alarms (16.0%, n = 10), and using locks that require a key on the interior and exterior of exit doors (9.6%, n = 6). However, most ICs (96.8%, n = 124) had not made any physical changes to their home, and more than half of the CRs (66.5%, n = 85) had spent time alone at home during the week. This poor assessment of risk is likely related to most ICs identifying wandering and getting lost as a problem that begins in the later stages of dementia (70%, n = 90).
Exiting at night
Incidents of CRs exiting the home at night were reported by 6.3% (n = 8) of ICs, half (n = 4) of which identified their CR as a wanderer. Care recipients who exited the home at night made up 100% (n = 4) of the CRs that were identified as wanderers by their IC. In response to their CR exiting the home at night, 6 of the 8 ICs said they watched the CR more closely; 1 IC made no changes and 1 installed a door alarm. Over half (60.0%, n = 72) of the ICs who had not experienced nighttime exiting were not concerned about it occurring in the future.
Wandering themes identified by ICs
For the question, “What does the word wandering mean to you?” Twelve common themes emerged from the ICs’ interview data. Aimless walking (27.3%, n = 35) was the most frequent IC response. Going to an unrealistic or odd location (1.5%, n = 2) and continuing on a path past a destination (1.5%, n = 2) were the least common themes reported. Only 10% (n = 13) endorsed getting lost and 4% (n = 5) of ICs included not returning home in their definition of wandering (see Table 3 for a complete list of responses).
Wandering Themes: Caregiver and Wandering Experts’ Agreement a
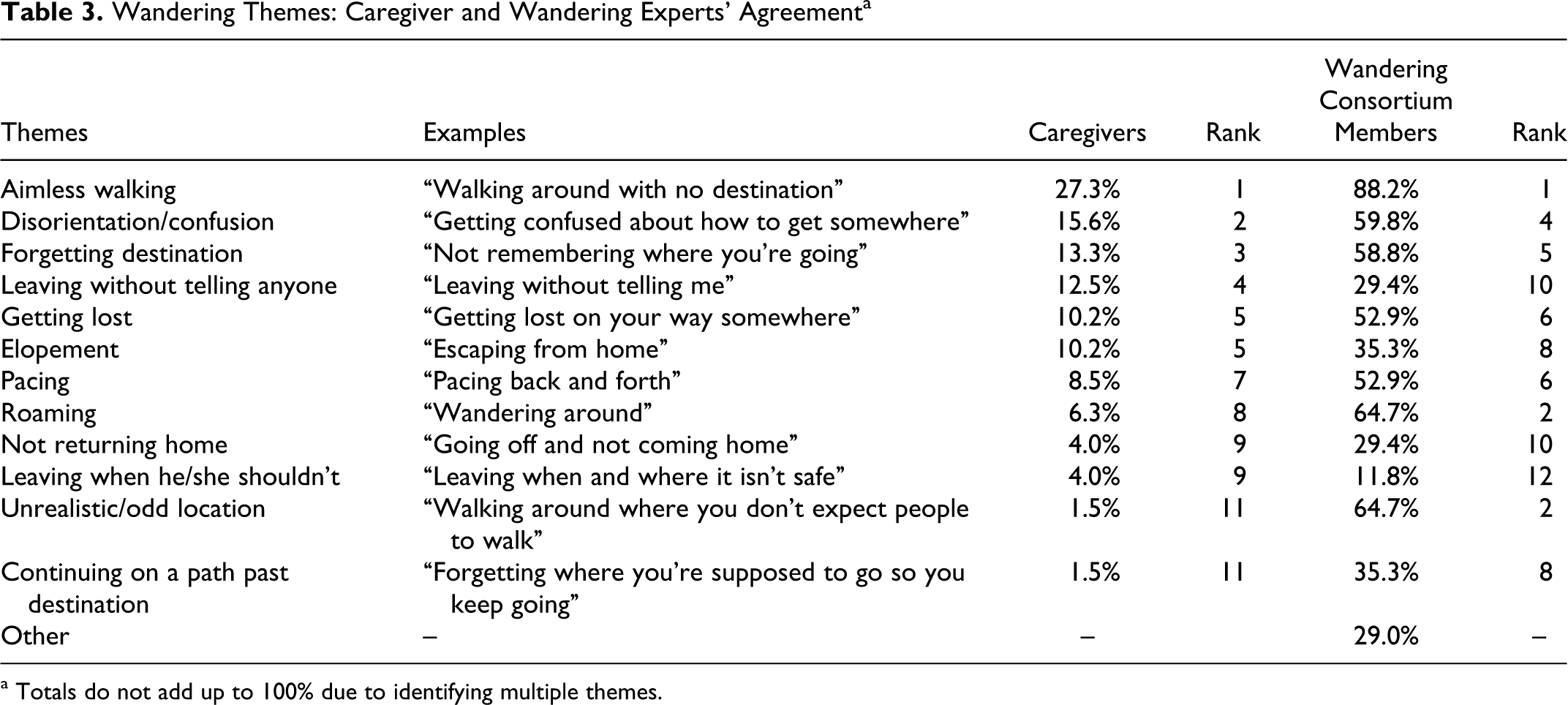
a Totals do not add up to 100% due to identifying multiple themes.
Expert Component
Of the 24 members of the International Consortium on Wandering and Missing Incidents who were asked to complete a survey, 17 (70.8%) participated. Survey answers were collected anonymously and no demographic information was collected from this sample.
Wandering themes
When consortium members selected items they considered consistent with the definition of wandering, aimless walking (88.2%, n = 15), roaming (64.7%, n = 11), and going to an unrealistic or odd location (64.7%, n = 11) were endorsed most frequently. Leaving when he/she shouldn’t (11.8%, n = 2) was the least common item selected by consortium members. About half of the experts (52.9%, n = 9) identified getting lost and 29.4% (n = 5) selected not returning home.
Experts’ definitions of wandering
Consortium members also provided a statement they would use to describe wandering to an IC. Typical responses included, “Wandering is a behavior exhibited by a person with dementia. This behavior may include: pacing, roaming without destination or purpose, walking in laps, eloping without knowledge or permission of ICs,” and “Getting separated or lost from family or ICs.”
Discussion
The inability to clearly define what wandering is and is not has an adverse effect on older adults with dementia and their ICs. For example, the Medic Alert + Safe Return program offers on their Web site an “… emergency response service for individuals with Alzheimer’s or related dementia who wander or have a medical emergency.” 15 ,16 This type of language may be a contributing factor to the low enrollment of ICs and CRs in programs that are intended to facilitate the rapid return of people with dementia who are found in the community. These programs are most beneficial if the CR is enrolled prior to wandering or becoming lost. If ICs minimize current behaviors, believe that these behaviors will not happen with their CR, feel they can adequately monitor and safeguard against these behaviors, and think these behaviors occur late in the disease process, they may not fully grasp the benefits of proactively enrolling in a safe return type of program. It is critical that ICs understand the progressive nature of dementia, what situations can be dangerous, and their potential consequences so that ICs can take appropriate, timely precautions.
In this study, ICs of older adults with dementia rarely used the term wandering to label different scenarios that had been previously identified in the literature as a wandering. Most of the ICs that used the term wandering had not experienced a wandering incident and used it to describe the situation hypothetically. Lost was the most commonly used term by all ICs in this sample. Similar to the results reported in earlier studies, 17 ICs in the current study also underestimated the potential of their CR to wander and failed to appreciate the risk. Although almost a quarter of ICs reported an event in which their CR had become lost, only a small portion of those ICs identified their CR as a wanderer. Furthermore, although almost half of the ICs in this study acknowledged that there was a chance that their CR would become lost due to growing memory problems, most CRs spent time alone during the week and only a few of these ICs had taken any precautions to prevent potential wandering incidents.
It is clear that ICs do not use the term wandering to describe incidents in which a CR is missing, a potentially dangerous situation. To achieve a basic level of awareness, health care professionals should use a broad set of terms including the word lost to describe possible current and future incidents so that ICs’ language is more likely to match with the clinicians’ assessments and recommendations. These discussions should continue as the disease progresses. It is important that ICs understand what they are being told, and that clinicians are asking in-depth questions so they can properly evaluate each situation and make specific recommendations to help both the patient and their IC. 18,19 To further enhance communication, clinicians and researchers should solicit definitions of terms from ICs to ensure that they share an understanding of the meaning.
In our sample there was some concurrence between ICs and wandering experts. “Aimless walking” was the most common theme identified by both wandering experts and ICs. However, there was also disagreement. For instance, the wandering consortium members’ second most common theme of going to an odd or unrealistic location was the least common theme noted by ICs.
Although there is a provisional definition for the term wandering, the structured interview with ICs and the survey of experts provided information that highlights inconsistencies within the consortium and between consortium members and ICs. Even though getting lost, pacing, disorientation and/or confusion, and elopement are expressly stated in Algase’s provisional definition of wandering, few consortium members endorsed these items.
The disparate perspectives and definitions of wandering identified in this study indicate that there is a significant and continued gap in communication between researchers, clinicians, and ICs. Misunderstandings about the terms wandering and getting lost may lead to poorer physical and mental health, under- and overreporting of events, and difficulty evaluating and comparing studies examining wandering. In clinical practice, lack of a face-valid definition of wandering requires that health professionals ask an array of questions to solicit IC definitions when describing CR experiences and to use a range of descriptors to enhance ICs’ understanding of CRs risk for, and potential consequences of, wandering behavior.
Footnotes
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the James A. Haley Veteran’s Affairs Hospital, Tampa, Florida, HSR&D/RR&D Center of Excellence: Maximizing Rehabilitation Outcomes. The authors would like to acknowledge the International Consortium on Wandering and Missing Incidents; Julie Kuhn; Sandra Mutolo, LCSW MSW; Helen Moore, PhD; Mark McCrannie, MA; Barbara McKenzie, MA, and Valerie Larson, MA, for their work related to this manuscript.
Appendix A
During the past year, was there ever a time you did not know where [name] was? Yes
What words did you use to describe that incident? No Are you ever concerned about not knowing where [name] is? Yes No
Does [name] go out or take walks alone? Yes Has [name] ever gone out on a walk and not returned home at the time you expected? Yes What words did you use to describe that event? No If this were to happen to [name] is there a certain word you would use to describe the event? No
Does [name] drive? Yes Has [name] ever driven somewhere and not returned home when he/she was expected? Yes How did you describe this event? No If [name] were to drive somewhere and not return home, how would you describe the event to a friend? No
Does [name] exit the home at night when you are sleeping? Yes How have you tried to prevent this from happening again? No Is a possibility of this something that concerns you?
During the past year, was there ever a time when [name] became lost? Yes What words did you use to describe that incident? No Are you ever concerned about [name] becoming lost? Yes No
Do you think there is a chance that [name] will ever get lost due to his/her memory problem? Yes What are some of the things you would do to keep [name] safe? Have you made any physical changes to your home to keep [name] safe? If [name] were to start getting separated from you, would you consider placing him/her in a facility? No Have you made any physical changes to your home to keep [name] safe?
At what stage do you think people with dementia begin to wander? Is it a problem that occurs during: early stages, middle stages, late stages or at any time when a person has dementia?
Does [name] spend time alone during the week?
What does the word wandering mean to you? -Do you think [name] wanders?
Appendix B
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.
Structured Interview for Caregiver
-
During the past year, was there ever a time you did not know where [name] was?
-
Yes
-
What words did you use to describe that incident?
-
-
No
-
Are you ever concerned about not knowing where [name] is?
-
Yes
-
No
-
-
-
-
Does [name] go out or take walks alone?
-
Yes
-
Has [name] ever gone out on a walk and not returned home at the time you expected?
-
Yes
-
What words did you use to describe that event?
-
-
No
-
If this were to happen to [name] is there a certain word you would use to describe the event?
-
-
-
-
No
-
-
Does [name] drive?
-
Yes
-
Has [name] ever driven somewhere and not returned home when he/she was expected?
-
Yes
-
How did you describe this event?
-
-
No
-
If [name] were to drive somewhere and not return home, how would you describe the event to a friend?
-
-
-
-
No
-
-
Does [name] exit the home at night when you are sleeping?
-
Yes
-
How have you tried to prevent this from happening again?
-
-
No
-
Is a possibility of this something that concerns you?
-
-
-
During the past year, was there ever a time when [name] became lost?
-
Yes
-
What words did you use to describe that incident?
-
-
No
-
Are you ever concerned about [name] becoming lost?
-
Yes
-
No
-
-
-
-
Do you think there is a chance that [name] will ever get lost due to his/her memory problem?
-
Yes
-
What are some of the things you would do to keep [name] safe?
-
Have you made any physical changes to your home to keep [name] safe?
-
If [name] were to start getting separated from you, would you consider placing him/her in a facility?
-
-
No
-
Have you made any physical changes to your home to keep [name] safe?
-
-
-
At what stage do you think people with dementia begin to wander? Is it a problem that occurs during: early stages, middle stages, late stages or at any time when a person has dementia?
-
Does [name] spend time alone during the week?
-
What does the word wandering mean to you? -Do you think [name] wanders?