
Abstract
Purpose:
We performed this network meta-analysis to compare the diagnostic value of 4 imaging methods (magnetic resonance imaging, positron emission tomography, computed tomography, and diffusion-weighted imaging) for diagnosing lymph node metastases in cervical cancer.
Method:
Diagnostic tests regarding different imaging methods to diagnose lymph node metastases in cervical cancer were retrieved from the Cochrane Library, PubMed, and Embase electronic databases from inception to December 2016. Direct and indirect evidence was performed to calculate the odds ratio and to draw the surface under the cumulative ranking curves of the 4 imaging methods for diagnosing lymph node metastases in cervical cancer.
Results:
Sixteen eligible diagnostic tests were included in this network meta-analysis. The results of network meta-analysis demonstrate that in comparison with the diffusion-weighted imaging, positive likelihood ratio, negative likelihood ratio, and diagnostic odds ratio of positron emission tomography were relatively higher. Additionally, the results further indicate that compared with other diagnosis method, positive likelihood ratio, negative likelihood ratio, and diagnostic odds ratio of positron emission tomography had a higher trend. The surface under the cumulative ranking curve results indicated that in terms of positive likelihood ratio and diagnostic odds ratio, positron emission tomography had a relatively higher diagnostic value for lymph node metastases in patients with cervical cancer.
Conclusion:
Our findings indicate that positron emission tomography might have a relatively higher diagnostic value for lymph node metastases in patients with cervical cancer.
Keywords
Introduction
Cervical cancer (CC) is a common gynecologic malignancy in women. 1 In 2012, the world cancer statistics showed that CC was the fourth most common cancer globally (528 000 new cases each year) and is also the fourth highest leading cause of death in women worldwide (266 000 deaths). 2 A previous study demonstrated that the etiology of CC is very complex and involved external, genetic, and cellular risk factors. 3 The main cause of CC is human papillomavirus (HPV) infection in the whole cervix. Next, the virus substantially metastasizes to the bladder, rectum, and other organs and may result in death. 4 The large growth in HPV and smoking have also been indicated to be vital causes of CC. 5 Cervical cancer is also known as a preventable cancer. 6 Furthermore, a previous study indicated that CC is associated with geographic location and that the incidence of CC has changed over time. 7 Lymph node (LN) metastasis in CC occurs when tumor cells acquire an immune escape mechanism to avoid the host immune system. 8 The presence of LN metastases in patients is common. A study by Sakuragi et al showed that out of 208 patients with stages IB, IIA, and IIB CC who had undergone radical hysterectomy and pelvic lymphadenectomy, 11.5% had stage IB lymphatic metastasis of CC, 26.7% had stage IIA metastasis, and 39.2% were in stage IIB. 9 Imaging is frequently used to determine tumor size, parametrial involvement, LN metastasis, and distant metastasis. Most patients with locally advanced CC are treated with definitive chemoradiotherapy in order to identify the disease extent (especially LN involvement). 10
There are multiple imaging methods that are widely used to diagnose LN metastasis in CC. These include magnetic resonance imaging (MRI), positron emission tomography (PET), computed tomography (CT), and diffusion-weighted imaging (DWI). Diffusion-weighted imaging is a noninvasive imaging method which aims to observe the molecular mobility of biological tissues (especially the water molecule). 11 It is characterized by diffusion gradients, homogeneous or converse imaging, high amplitude, and a short acquisition time. Diffusion-weighted imaging is generally accepted worldwide to be the standardized imaging technique. 12 This study evaluated the usefulness of tumor volume measurement with PET in patients with advanced CC treated by radiation therapy. 13 In terms of treatment planning in radiotherapy, PET has the advantage of tumor delineation and incorporation of biological process descriptions. 14 Hancke et al proposed that a clinical examination is more effective than an MRI or CT in the pretreatment assessment of early invasive CC. 15 The positive predictive value (PPV) of PET in the pelvis and para-aortic region appears sufficient to obviate lymph nodal sampling, but sampling is still required to exclude small-volume disease cranial to sites of abnormality on PET, while MRI has insufficient accuracy for nodal staging to impact management. 16 Furthermore, Exner et al demonstrated that DWI is more useful than a conventional MRI. 17 A larger prospective trial will determine whether this modality should be used routinely in conjunction with, or in lieu of, other imaging studies to detect recurrent disease in a broader population of patients with CC. 18 Despite the abundant literature submitted, there was no comprehensive literature regarding the optimal imaging method to diagnose LN metastasis in CC. The aim of our study is to conduct a systematic review (including a traditional meta-analysis and network meta-analysis [NMA]) on the diagnostic value of 4 imaging methods of diagnosing LN metastasis in CC. We also expected this study to be helpful to physicians in the diagnosis of LN metastasis in CC.
Materials and Method
Literature Search
The Cochrane Library, PubMed, and Embase databases were searched via computer-based and manual retrieval for related references of CC with LN metastasis from inception to December 2016. The combination of keywords and individual words including cervical carcinoma, magnetic resonance imaging, LN metastases, computed tomography, positron emission tomography, anddiffusion-weighted imaging were used as the search terms.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) study design was via diagnostic tests; (2) imaging methods included MRI, PET, CT, and DWI; (3) the age of patients with CC ranged from 21 to 82 years; (4) outcomes included positive likelihood ratio, negative likelihood ratio, and diagnostic odds ratio (OR). The exclusion criteria were (1) studies lacking data integrity or are not related to CC and (2) duplicate studies, conference reports, systematic reviews, summary articles, case–control studies, non-English studies, or nonhuman studies.
Data Extraction and Quality Assessment
Data from included studies were extracted by 2 researchers independently using the standard data collection forms. The main data included the first author, publication time, country, race, age, the gold standard, and so on. Any disagreements were resolved through discussion. Risk of bias of included cohort studies was assessed by 2 or more researchers according to the Quality Assessment of Diagnostic Accuracy Studies (QUADAS). 19 The QUADAS tool includes 4 key domains: discuss patient selection, reference standard, index test, and flow and timing (flow of patients through the study, time of the index tests, and reference standard). The Review Manager 5 software (RevMan 5.2.3; Cochrane Collaboration, Oxford, United Kingdom) was applied to evaluate quality and investigate publication bias.
Statistical Analysis
Firstly, we performed a traditional pairwise meta-analysis of studies that directly compared different diagnostic modalities. Statistics were combined by meta-analysis, and threshold effect should be considered at first, which was tested by calculating logarithm of sensitivity and logarithm of 1 − specificity. A P > .05 indicated nonthreshold effect, while P < .05 showed threshold effect. Sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio could be combined directly if there was no threshold effect. Merge statistics were analyzed via meta-analysis, and if there was heterogeneity caused by threshold effects, data merging was conducted by summary receiver operating characteristic (SROC) curve and then the SROC value was calculated. Area under the curve (AUC) was close to 1, indicating that the clinical value is greater. Area under the curve was between 0.5 and −0.7, indicating that the clinical value was lower. An AUC > 0.7 indicates that the clinical value is good. The straight line of the Deek funnel plot was used as the regression line, and if the included angle of the diagnostic odds ratio (DOR) axis was close to 90°, it indicates that the possibility of publication bias is smaller. 20 The OR and 95% credible interval estimates of CC are also shown. The χ2 and I 2 tests were used to test heterogeneity of the studies. 21 Secondly, R 3.2.1 software was used to draw a network evidence diagram, whereby each node represented a different intervention, node size reflected sample size, and the thickness of the line between nodes represented the number of included studies. Thirdly, a Bayesian NMA was conducted by comparing different diagnostic modalities. Each analysis was based on noninformative priors for effect sizes and precision. We checked and confirmed convergence and lack of autocorrelation after 4 chains and a 20 000-simulation burn-in phase. Eventually, direct probability statements were derived from an additional 50 000-simulation phase. 22 The node splitting method was adopted to evaluate the consistency between direct and indirect evidence, and the decision to use either the consistency or inconsistency model was based on the results. 23 To assist in the interpretation of OR, we calculated the probability of each diagnostic modality. The most effective method was found to be based on a Bayesian approach adopting probability values summarized as surface under the cumulative ranking curve (SUCRA). The larger the SUCRA value, the better the rank of the intervention. 24,25 The cluster analysis method was adopted to evaluate the value of 5 imaging methods in the diagnosis of LN metastasis in CC. This involved clustering different interventions according to the similarity of 2 variables and then determining the advantages and disadvantages of different imaging methods. 24 All computations were conducted using the R (V.3.2.1), package gemtc (V.0.6), and Markov Chain Monte Carlo engine Open BUGS (V.3.4.0) software.
Results
Baseline Characteristics of Included Studies
A total of 5184 relevant studies were initially retrieved from the databases. We excluded 26 duplicate studies, 191 letters and reviews, 22 nonhuman studies, and 604 non-English studies. After a full-text review, we ruled out 156 case–control studies, 1630 cases unrelated to CC, 2538 cases unrelated to imaging methods, and 1 which had low data integrity. Finally, 16 diagnostic tests were eligible and included in this meta-analysis 15 -17,26 -38 (Supplemental Figure 1). These studies included 1172 patients with CC, most adopted MRI, and were published from 1990 to 2016. There were 8 studies on Caucasians and 8 on Asians. All 16 diagnostic tests were 2-arm trials. The baseline characteristics of included studies are displayed in Supplemental Table 1. The Cochrane risk of bias assessment of included studies is shown in Figure 1.

Quality Assessment of Diagnostic Accuracy Studies (QUADAS) included in the network meta-analysis checklist.
Pairwise Meta-Analysis of the Diagnostic Value of 4 Imaging Methods in the Diagnosis of LN Metastasis in CC
In CT, Spearman correlation coefficient = −0.179, calculated by logarithm of sensitivity and logarithm of 1 − specificity, P = .702; in MRI, Spearman correlation coefficient = 0.188, calculated by logarithm of sensitivity and logarithm of 1 − specificity, P = .503; in PET, Spearman correlation coefficient = −0.143, calculated by logarithm of sensitivity and logarithm of 1 − specificity, P = .736. Results of threshold testing indicated that there was no threshold effect in each research, so the sensitivity, specificity, PPV, and negative predictive value could be combined. Bivariate box plot showed that there was heterogeneity in each research (Figure 2). The area of the SROC curve showed that diagnostic value of CT, MRI, and PET was good (AUC = 0. 88, AUC = 0. 84, AUC = 0.88; Figure 3). Deek funnel plot indicated that there was less likelihood of publication bias, which was confirmed by linear regression test (all P > .05; Figure 4). We conducted a direct paired comparison of the diagnostic value of 4 imaging methods in the diagnosis of LN metastasis in CC. The results revealed that positive likelihood ratio, negative likelihood ratio, and diagnostic OR of PET were relatively higher than MRI (Table 1).

Bivariate box plot diagnostic value for 4 imaging methods in the diagnosis of lymph node metastasis in patients with CC. CC indicates cervical cancer.

Summary receiver operating characteristic diagram of diagnostic value for 4 imaging methods in the diagnosis of lymph node metastasis in patients with CC. CC indicates cervical cancer.

Deek funnel plot of diagnostic value for 4 imaging methods in the diagnosis of lymph node metastasis in patients with CC. CC indicates cervical cancer.
Estimated OR and 95% CI of Pairwise Meta-Analysis for 4 Modalities in the Detection of Lymph Node Metastases in Cervical Cancer.a
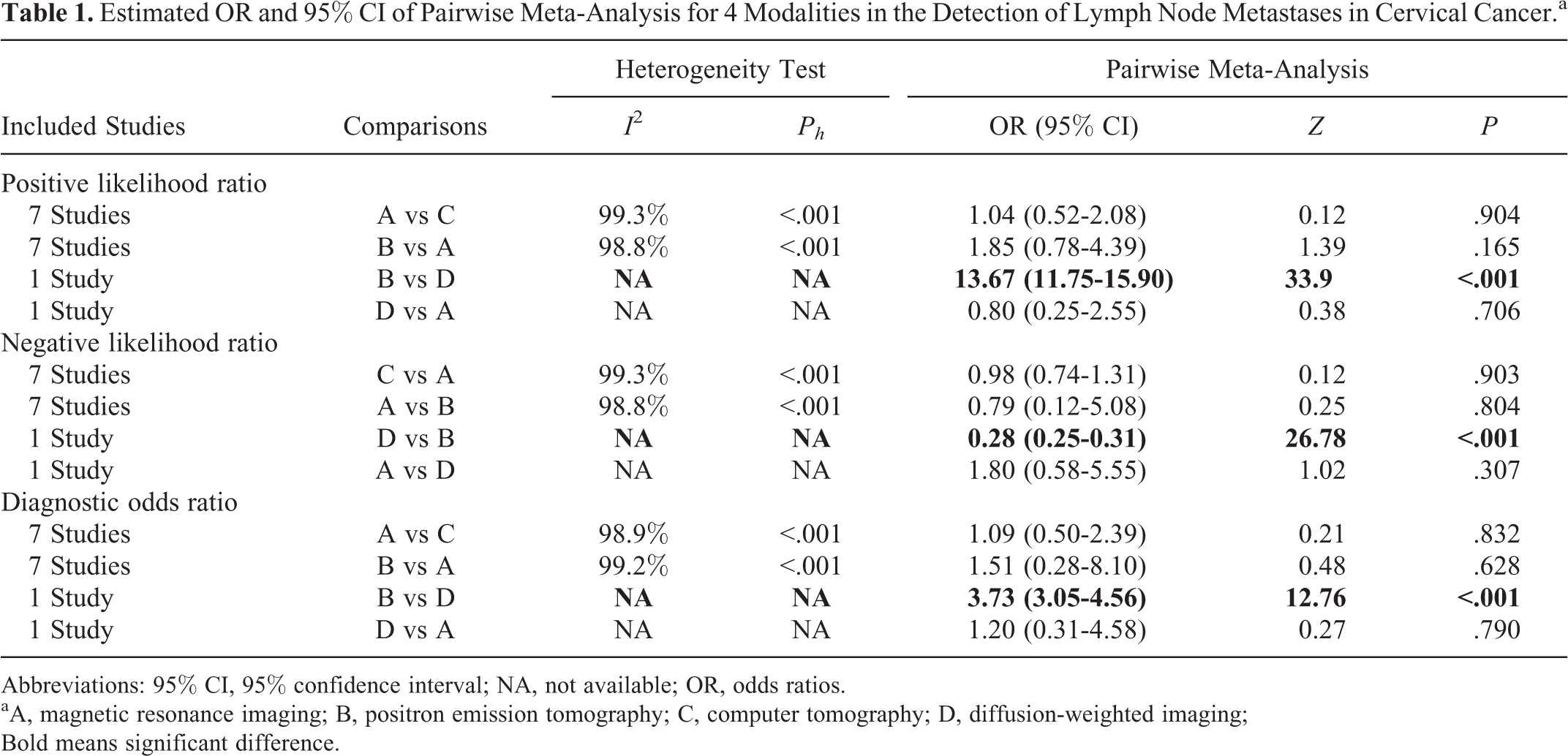
Abbreviations: 95% CI, 95% confidence interval; NA, not available; OR, odds ratios.
aA, magnetic resonance imaging; B, positron emission tomography; C, computer tomography; D, diffusion-weighted imaging; Bold means significant difference.
Evidence Network of the Diagnostic Value of 4 Imaging Methods in the Diagnosis of LN Metastasis in CC
Four imaging methods were included in this NMA. In terms of positive likelihood ratio, negative likelihood ratio, and diagnostic OR, a large number of patients were diagnosed with MRI (as shown in Figure 5).

Network evidence of the diagnostic value of 4 imaging methods in the diagnosis of lymph node metastasis in patients with CC. CC indicates cervical cancer; CT, computer tomography; DWI, diffusion-weighted imaging; MRI, magnetic resonance imaging; PET, positron emission tomography.
Inconsistency Tests of Positive Likelihood Ratio, Negative Likelihood Ratio, and Diagnostic OR
The inconsistency tests demonstrated that the results of the direct and indirect evidence on positive likelihood ratio, negative likelihood ratio, and diagnostic OR were consistent; thus, the consistency model was adopted (both P > .05; Figure 6).

Node splitting plot of the diagnostic value of 4 imaging methods in the diagnosis of lymph node metastasis in patients with CC. A, Magnetic resonance imaging. B, Positron emission tomography. C, Computer tomography; D, diffusion-weighted imaging. CC indicates cervical cancer.
Main Results of the NMA of the Diagnostic Value of 4 Imaging Methods in the Diagnosis of LN Metastasis in CC
The results of this NMA indicated that the positive likelihood ratio, negative likelihood ratio, and diagnostic OR of PET had a corresponding higher trend compared to MRI, DWI, and CT (Table 2).
Odds Ratios and 95% Confidence Intervals of 4 Modalities for the Diagnosis of Cervical Cancer Under 2 End Indicators Based on the Network Meta-Analysis.a
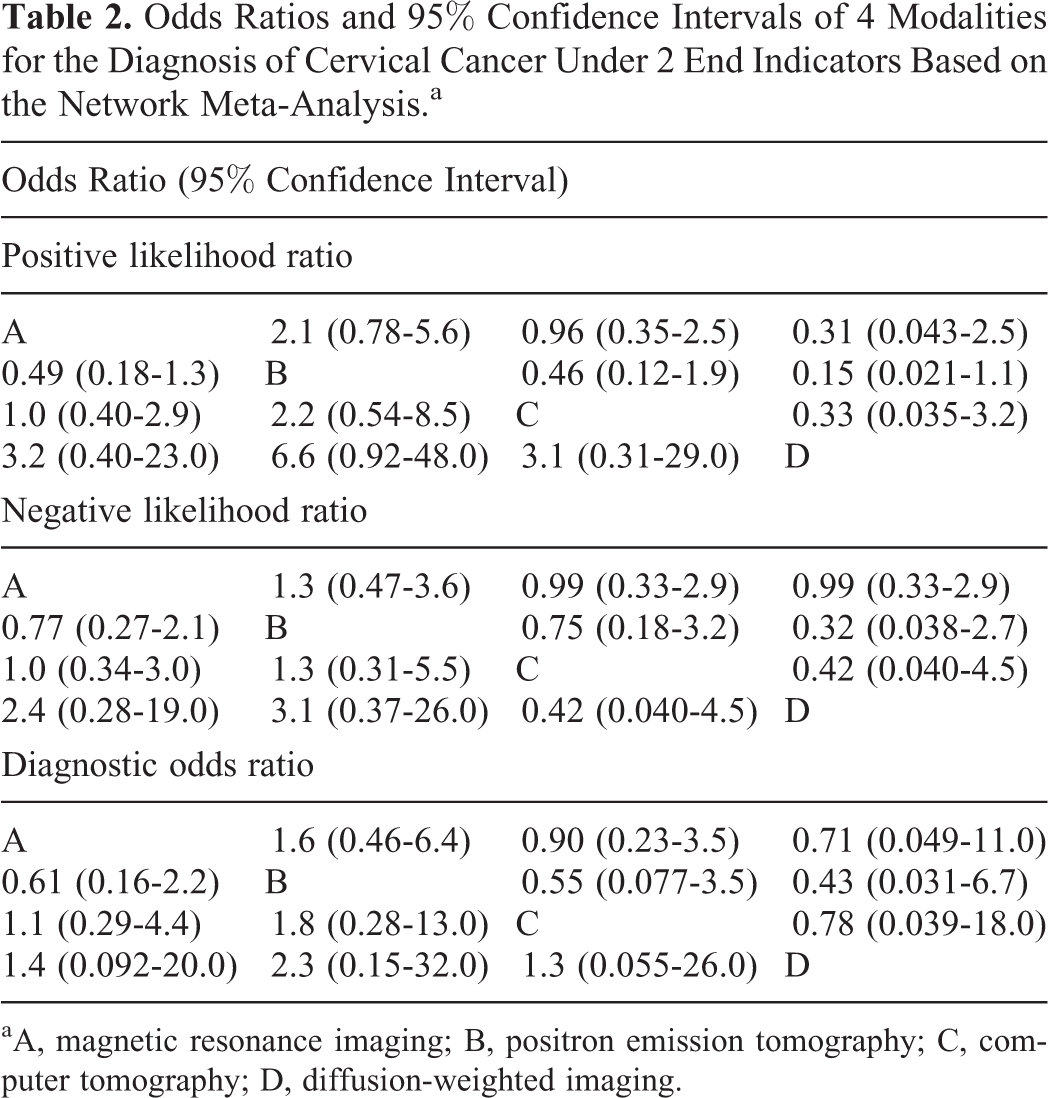
aA, magnetic resonance imaging; B, positron emission tomography; C, computer tomography; D, diffusion-weighted imaging.
The SUCRA Values of the Diagnostic Value of 4 Imaging Methods in the Diagnosis of LN Metastasis in CC
As shown in Table 3, the SUCRA values demonstrated that in terms of positive likelihood ratio and diagnostic OR, PET had a relatively higher diagnostic value for LN metastases in patients with CC.
The SUCRA Values of 4 Diagnostic Modalities Under 3 End Point Outcomes.a

Abbreviation: SUCRA, surface under the cumulative ranking curves.
aA, magnetic resonance imaging; B, positron emission tomography; C, computer tomography; D, diffusion-weighted imaging.
Sensitivity Analysis of the Diagnostic Value of 4 Imaging Methods in the Diagnosis of LN Metastasis in CC
As shown in Supplemental Figure 2, the SROC curves of CT, MRI, and PET had no significant change after rejecting an arbitrary research, which demonstrated that all including researches less affected the outcomes. In Supplemental Figures 3 to 11, the SUCRA values of others had no significant change after rejecting an arbitrary research, which demonstrated that the conclusion was convincing.
Discussion
The lymphatic system is the most important pathway for the spread of CC. 39 A noninvasive technique that could accurately identify LN metastasis in malignant tumors would be strongly beneficial for improving treatment management. 40 This NMA compared 4 imaging methods using 16 diagnostic tests involving 1172 patients with CC. The results of NMA demonstrated that in comparison with the DWI, positive likelihood ratio, negative likelihood ratio, and diagnostic OR of PET were relative higher. The SUCRA results indicated that in terms of positive likelihood ratio and diagnostic OR, PET had a relatively higher diagnostic value for LN metastases in patients with CC.
Firstly, we conducted a direct paired comparison of the diagnostic value of 4 imaging methods in the diagnosis of LN metastasis in CC. The results revealed that positive likelihood ratio, negative likelihood ratio, and diagnostic OR of PET were relatively higher than DWI. Extracapsular spread of LN metastasis has been shown as a negative prognostic factor in cancers of several organs. 41 Positron emission tomography may be a useful follow-up method for CC, thereby providing the patients with early opportunities for sophisticated treatments. 42 Positron emission tomography proved to be valuable for LN staging in patients with early-stage CC, with short-axis diameter greater than 0.5 cm being the size threshold for accurate depiction of metastatic nodes. 43 Positron emission tomography appears useful in the management of CC, in particular for staging extrapelvic metastases or optimally detecting a recurrence. 44
Secondly, the SUCRA values demonstrated that in terms of positive likelihood ratio and diagnostic OR, PET had a relatively higher diagnostic value for LN metastases in patients with CC. Positron emission tomography scan is a sensitive imaging modality for the detection of recurrent cervical carcinoma in both symptomatic and asymptomatic women. 45 Using this modality may reduce unnecessary surgical interventions, help modify radiation fields, and change therapeutic approaches. 46 Therefore, PET in conjunction with MRI can improve the detection of extrapelvic metastasis. 47 Diffusion-weighted imaging is a technique which evaluates the rate of microscopic water diffusion in tissues. 48 It has recently been used in oncologic imaging to depict and characterize tumors and to differentiate benign lesions from malignant lesions in various tumors such as uterine cancer. 49,50 A previous study evaluated its potential in detecting and evaluating pelvic LN metastases via body DWIs in patients with gynecologic malignancies. It showed that body DWI is useful in detecting pelvic LNs in patients with gynecologic malignancy. 51 However, the results of this study were controversial due to the quantitative apparent diffusion coefficient value for differentiation of malignant from benign LNs in uterine cancer. Shen et al evaluated the diagnostic performance of DWI in CC metastasis with a sensitivity, specificity, and AUC of 86%, 84%, and 0.9384, respectively. The results showed a strong diagnostic performance of DWI in relation to sensitivity, specificity, and AUC in comparison with other imaging methods. 52
Conclusion
Our study evaluated the diagnostic performance of 4 different imaging techniques and concluded that DWI, PET, CT, and MRI are the optimal imaging methods for the diagnosis of LN metastases in CC. This may provide theoretical evidence for the diagnosis of patients with CC. However, there are some limitations of this study which should be mentioned. Firstly, because of the limited number of documents and direct imaging method comparisons, our results may have been influenced. Secondly, patients in different stages of CC have different LN metastasis levels, which can affect the preference of imaging method. Thirdly, limited data on the diagnostic efficacy of a single criterion were corresponding, thus may have influenced data pooling with a single criterion. Finally, there were only 2 studies about DWI, so a threshold and SROC curve could not be conducted about it. And we did not obtain the effective methodology applied from the included study of Bellomi et al, which might cause bias for our final results. A well-designed prospective, randomized, multicentered clinical trial is required to evaluate the diagnostic value of these imaging methods in the diagnosis of LN metastases in CC.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank the reviewers for their helpful comments on this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.