
Abstract
The aim of this study was to evaluate the effectiveness of CyberKnife-based stereotactic ablative radiotherapy on prostate cancer lymph node metastases. Our material consisted of 18 patients with 31 metastatic lymph nodes irradiated between 2011 and 2014 using CyberKnife-based stereotactic ablative radiotherapy. Patients were irradiated using fraction dose varied from 6 to 15 Gy (median 10), to the total dose of 24 to 45 Gy (median 30). Irradiated lymph node size varied from 0.4 to 4.0 cm. In all, 9 patients had single lymph node metastasis and 9 patients had metastases of 2 to 4 lymph nodes. Prostate-specific antigen concentration before radiotherapy varied from 0.01 to 15.58 (mean 6.97; median 4.66). All patients at the time of radiotherapy and follow-up received androgen deprivation therapy. Mann-Whitney U, Kaplan-Meier method, and log-rank tests were used in statistical analysis. We obtained the following results: after CyberKnife stereotactic ablative radiotherapy, prostate-specific antigen concentration dropped in majority of cases and during the last control varied from 0.00 to 258.00 (median 2.5), and was lower in patients without dissemination to other organs (P = .01). Complete regression was found in 12 lesions, stable disease in 13, and progression in 4. In 7 patients, the dissemination to other organs occurred. Our results allow us to conclude that CyberKnife stereotactic ablative radiotherapy of prostate cancer lymph node oligometastases gives good local control and relatively good prostate-specific antigen response.
Introduction
Prostate cancer (PC) is the second most common malignant disease and second cause of death due to cancer among men in Poland in 2011. Despite improvements in surgical and irradiation techniques, tumor relapse after radical radiotherapy is not rare. 1,2
Improvements in the early detection of the disease relapse allow us now to diagnose single or organ-limited metastases in patients with rising prostate-specific antigen (PSA) after primary treatment. According to many authors, conventional computed tomography (CT) and magnetic resonance imaging (MRI) are approximately equivalent in detecting lymph node (LN) metastases, and all nodes exceeding minimal size of 6 to 15 mm could be considered as potentially involved. 3 Despite that, pathologic reports on specimens of nodal dissections for PC showed that metastatic deposits could be found in about 25% of normal size LN in patients with T3 stage of the disease. 4
New imaging modalities like 11 C-choline, 18 F-choline, or 11 C-acetate positron emission tomography (PET)-CT may be used to identify patients with limited LN relapse who may benefit from local treatment. 11 C-Choline PET-computed tomography has a high sensitivity and specificity for detecting soft tissue metastases of PC and has a high diagnostic ratio for identification of LN metastases in case of PSA concentration increase, therefore, it should be considered as a first-line diagnostic tool in those patients. 5
Androgen deprivation therapy (ADT) is a commonly used treatment in LN recurrent PC but it is a non-curative approach, and long-term use might induce significant side effects and negatively influence general health status and patient’s quality of life because of cognitive and sexual impairment, fatigue, cardiovascular dysfunction, metabolic syndrome, and osteoporosis. 6,7
Radiotherapy is commonly used in the treatment of primary PC and metastatic lesions including LN metastases. 1,6 –14 Stereotactic ablative radiotherapy (SABR) is a radiation therapy in which very high doses of radiation are delivered in a small number of fractions. The SABR was initially confined to patients with unresectable or medically inoperable tumors. Nowadays, its use has been extended and some of the results are encouraging. 15 The SABR in treatment of small metastases is less invasive than surgery and has the potential to deliver ablative treatment sparing the surrounding healthy tissue. 2 The aim of SABR is to achieve good local control (LC) of oligometastases and possibly the cure of some patients. In general, indications for SBRT are the same as those for metastasectomy, but without the limits regarding the feasibility of it in patients unfit for surgery. The best candidates for SABR are younger patients in good performance status with controlled primary tumors, 5 or fewer oligometastases in size under 5 cm. 2,16 The number of metastases may reflect the biologic aggressiveness of the tumor. Published reports showed that patients with PC with equal to or less than 5 metastases had a significantly better survival rates than those with more than 5 lesions, therefore, more aggressive treatment may improve long-term survival. 8
The SABR allows delivering high-radiation dose to relatively small-volume tumors using small number of fractions (“radioablation”).2 CyberKnife (CK) SABR is a high-precision technique with tight planning margins and a sophisticated treatment plan allowing for steep dose gradient outside the target. It provides good target coverage and spares healthy tissues. 15,17 Reports so far published referring to the use of radiosurgery in metastatic abdominal LN treatment suggest that this is an effective method of therapy and its toxicity is acceptable. 1,2,6,8 –11,13,16 –21,22 –25,26,27 Use of SABR with higher fds results not only in direct cytotoxicity but also in different vascular mechanism of the killing tumor cells.2 The concept of spatial cooperation between radiation and systemic therapy is also attractive in case of oligo-recurrent LN clinical scenario, which has the potential to delay the time to castrate resistance. 16,21,22
The CK SABR is used for palliative treatment of metastases originating from different cancer sites. Recent reports concerning the treatment of brain, hepatic, and bone metastases from lung, colorectal, or prostate cancer indicate that CK SABR has provided good LC and analgesic effect in cases of painful lesions. 14,28 –30
Aim of the Study
The purpose of this study was to evaluate the effectiveness and toxicity of SABR on prostate cancer LN metastases.
Materials and Methods
Our material consisted of 18 patients with PC with 31 metastatic LN. All cases were treated using CK SABR from December 2011 to March 2014. The age of patients ranged from 58 to 80 years (mean 69, SD ± 6.2). In all, 16 patients had been treated with SBRT due to recurrence of the disease and 2 patients received SBRT as part of primary treatment (radiotherapy (RT) + SBRT boost to metastatic LNs). The diagnosis of the PC recurrence was based on biochemical (PSA concentration) progression according to Phoenix criterion (in 12 patients) and/or local relapse evaluation (PET-CT). In 12 cases, metastases were diagnosed with CT-18F-choline PET (11 cases) or 11C-choline PET (1 case), in 3 cases with CT and in 3 cases with MRI. The PSA concentration at the time of PET-CT ranged from 1.04 to 23.16 ng/mL (median 5.7 and mean 9.1). All scans were interpreted by the radiologist and nuclear medicine specialists. Patients who had PET-CT were considered LN-positive if visible on CT LN had increased uptake of radionuclide (size: 4-40 mm). Computed tomography was used to diagnose patients who had metastatic LNs of size 17 to 21 mm and MRI used to diagnose those who had metastatic LNs of size 9 to 21 mm. All metastatic LNs were located in retroperitoneal region and among them 17 along iliac vessels. In all, 9 patients presented a single metastasis and 9 were diagnosed with 2 to 4 metastases. The PSA concentration at the time of metastasis detection varied from 0.01 to 18.7 ng/mL (median 4.7 and mean 6.7). Other metastases were found in 2 patients. One of them had bone metastasis (also treated with CK SABR). For these 2 patients, chemotherapy based on docetaxel was delivered. Despite that metastases were found in more than 1 location, their number did not exceed 5. No other local therapy for recurrent LN was delivered.
Size of the oligo-recurrent LN (mean from 3 dimensions) ranged from 4 to 40 mm (median 17, mean 19, and SD ± 9.13). Case characteristics in details are presented in Table 1.
Clinical Features of Irradiated Patients.a
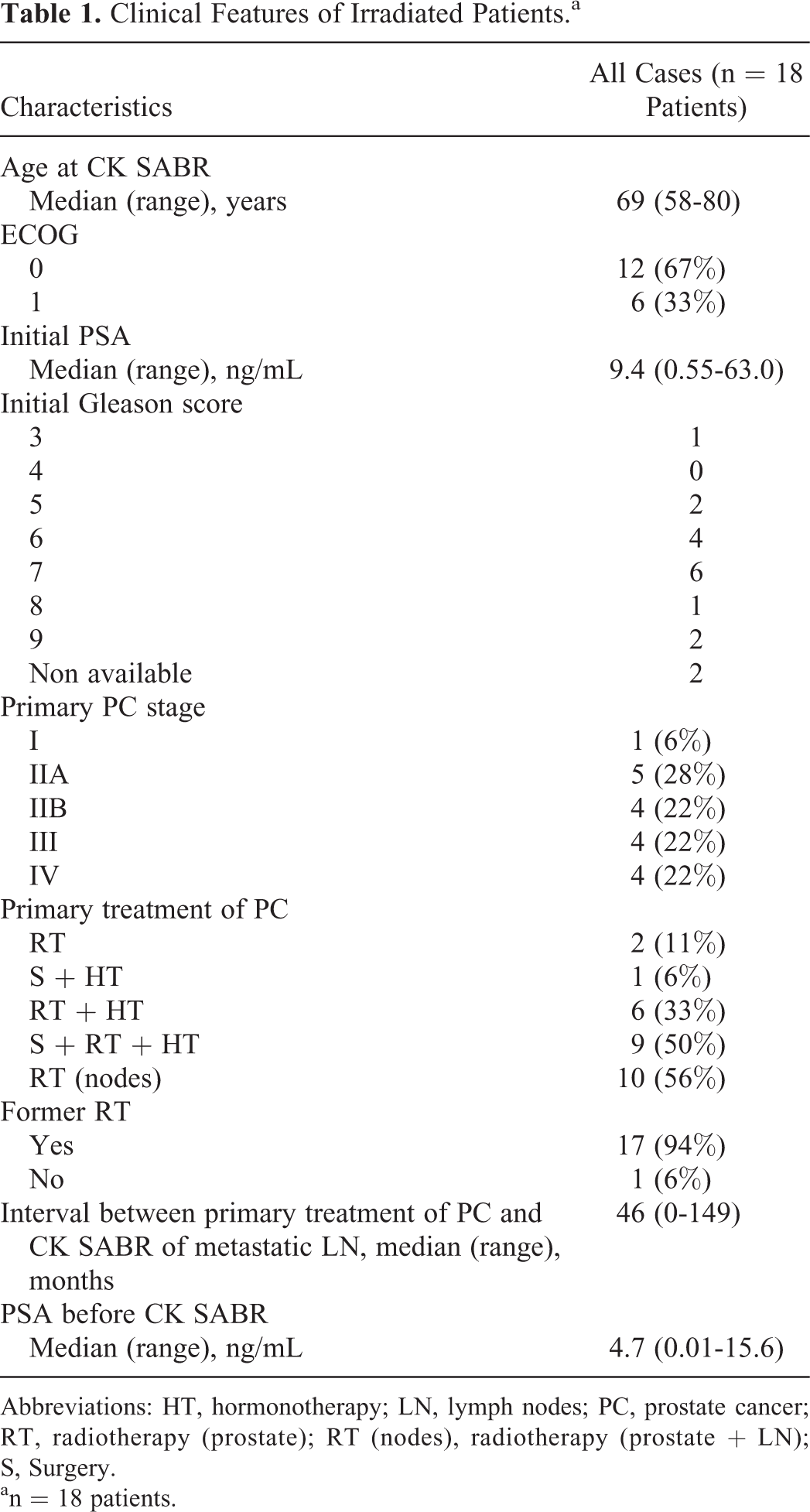
Abbreviations: HT, hormonotherapy; LN, lymph nodes; PC, prostate cancer; RT, radiotherapy (prostate); RT (nodes), radiotherapy (prostate + LN); S, Surgery.
an = 18 patients.
Radiotherapy was part of the primary treatment in 17 cases (in 3 cases prostate bed and pelvic LN, in 7 prostate and pelvic LN, in 5 only prostate bed, and in 2 prostate only was irradiated). Total dose (TD) delivered to prostate gland/bed ranged from 46 to 77 Gy (median 74 and mean 71.5) and TD delivered to LN regions ranged from 44 to 50 Gy (median 44 and mean 47.1).
Gleason score was equal to or greater than 7 in 9 cases. The PSA concentration was greater than 20 ng/mL at the time of PC diagnosis in 4 cases. Time from previous treatment to CK SABR of LN metastases ranged from 0 to 149 months (median 46 months). Time from detection of the LN oligometastases to the beginning of the radiosurgery ranged from 1 to 4 months. All patients were in good performance status. All patients were treated with ADT during the SABR and follow-up (FU). The PSA before CK SABR varied from 0.01 to 15.6 (median 4.66 and mean 6.97).
The PET-CT was used to improve planning target volume (PTV) in 9 cases. Target in SBRT consists of 2 volumes: gross tumor volume (GTV) which is a lesion itself and PTV, which provides margins in order to correct for inaccuracies in the delivery system (set-up margin), or/and interfracion and intrafraction organ motion. The imaging modalities used in PTV are presented in Table 2.
Imaging Modalities Used in Planning Target Volume.

Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; PET, positron emission tomography.
The PTV margins in all directions were 5 mm in 28 lesions and 4 mm in 3 lesions. Organs at risk (OAR), such as the aorta, were excluded from PTV. Dose volume histograms were calculated for PTV, PTV-OAR, and OAR. The main OARs considered were dependent on the site of GTV and included the spinal cord, rectum, urinary bladder, kidneys, stomach, small bowel, femoral heads, aorta, and liver. All those structures were contoured in order to reduce the delivered dose. Reference isodose (covering whole lesion and corresponding to planned and delivered dose) varied from 78% to 89% (mean 85.2 and median 86).
Our planning priorities were not to exceed a dose to OARs (as in many cases CK SABR was a reirradiation) and to cover 100% of PTV to a minimum of 95% of the prescribed dose, which in some cases was impossible due to the proximity of OARs. In spite of the above, a mean dose delivered to PTV was usually higher than dose prescribed.
All patients were immobilized by the use of a customized external vacuum system. The treatment planning was performed using MultiPlan system (New York). Metastases were irradiated using tracking technology, which allowed us to follow the location of the lesion during SABR session, and to correct the beam position and position of the patient depending on the change of its (target) location. According to the published reports applying position correction on bone for nodal field gives the best target coverage. 31 The tracking system Xsight Spine was used to verify the correct setup during each fraction in all but 1 of the patients. As it is a tracking system based on locating bones, all treated LNs were located at a distance of not more than 6 cm from spine (based on data provided by the Accuray [Sunnyvale, California], it is not appropriate to treat an LN up to 6 cm away from spine with Xsight Spine tracking system). Repositioning was performed according to spine levels, which were closest to the LNs treated (it varied depending on the LN location). The lowest vertebra used for tracking/repositioning was S1. In 1 patient, the implantation of suitable marker near left external iliac vessels was performed before irradiation, and Fiducial Tracking was used to detect the location of this marker during the radiosurgery. If more than 1 lesion was irradiated, all were treated in the same session. Particular attention was paid to those patients who already have undergone irradiation. In all such cases, the original plans were reviewed. No additional premedication was used before CK SABR. All patients signed written informed consent for CK SABR.
Patients had metastases treated with fd of 6 to 15 Gy (mean 10.43, median 10, and SD ±2.15) to a TD within the range of 24 to 45 Gy (mean 31.3, median 30, and SD ±6.00) delivered in 3 (29 lesions), 2 (1 lesion), and in 5 fractions (1 lesion). The overall treatment time (OTT) varied from 6 to 15 days. Dose constraints for OAR were followed. The number of cases and lesions treated with a particular radiation schedule is presented in Table 3. Table 4 presents doses delivered to GTV, PTV, and PTV-OAR for each patient. All patients completed CK SABR as planned.
CyberKnife Stereotactic Ablative Radiosurgery—TD and fds in Particular Cases.

Abbreviations: fd, fractional dose; TD, total dose.
aOne patient with 3 metastatic lymph nodes had 2 lesions treated with 3 fractions of 10 Gy to the total dose of 30 Gy and 1 lesion treated with 5 fractions of 6 Gy to the total dose of 30 Gy.
Doses Prescribed and Delivered in Particular Patients.

Abbreviations: fd, fraction dose; GTV, gross tumor volume; m, metastases; OAR, organs at risk; PTV, planned target volume; TD, total dose.
Patients were followed 1 month after the SABR completion and next every 3 and 6 months to the end of FU period. During FU, the PSA concentration, lesion regression, and presence of other metastases were checked. The size of treated LN and the presence of other metastases were evaluated using CT or MRI. In all these cases, comparative radiologic analysis with CT/MRI images taken before treatment was performed. Response to treatment was classified according to Response Evaluation Criteria In Solid Tumors into 1 of 4 categories: complete regression/response (CR), partial regression/response (PR; decrease in size of the assessed LN compared to initial size), stable disease (SD; size of the LN the same as that of initial size), or progression (increase in size of the lesion compared to initial size). The appearance of other lesions was not considered in this system. Progression in uninvolved LNs (not treated) was scored as disseminated failure. Based on that classification, LC was evaluated in terms of freedom from local progression (FLP), defined as SD, or CR or PR.
Acute radiation-induced toxicity was analyzed in all cases and late treatment-related toxicity was evaluated in patients with FU over 3 months. Radiation Therapy Oncology Group/European Organization for Research and Treatment of Cancer (RTOG/EORTC) criteria were used to evaluate treatment toxicity. 32 There was no acute toxicity. Late urinary and rectal toxicity grade 1 occurred in 1 patient and late urinary toxicity grade 1 was developed in 1 patient. These 2 patients had radiotherapy as a part of the primary treatment of prostate cancer, and this toxicity could be a result of previous irradiation.
Patients and treatment data were collected retrospectively. The FU time from the date of the end of CK SABR to the date of death or last control ranged from 0 to 33 months (mean 16.4 and median 15.6).
For statistical analysis, Mann-Whitney U, Kaplan-Meier method, and log-rank tests were performed. Mann-Whitney U test was used to analyze possible correlations between TD, Gleason score, PSA concentration, and size of the LNs treated. Log-rank test was performed to find possible prognostic factors that might affect overall survival or LC of the lesions. P values of less than .05 were considered to indicate statistical significance. Kaplan-Meier method was used to evaluate overall survival and progression-free survival. Time to progression was measured from the date of the end of CK SABR to the data of local progression.
Results
Size of treated metastatic LN was evaluated based on CT/MRI images during the FU in 16 cases. Three months after the CK SABR among treated metastatic LN, 5 resulted in CR and 3 with PR according to criteria described in the “Materials and Methods” section. Stable size of LN was achieved in 5 lesions. During the last control, CR and stable size of LN were observed in 12 and 13 lesions, respectively (LC rate of 76.9%). In 4 lesions, progression of the size of treated LN occurred. The FLP was achieved in 14 (78.5%) patients during the FU. Size of treated metastatic LN during the FU is presented in Table 5. One- and 2-year LC rate was 93% and 70%, respectively.
Irradiated LN Regression During the FU Period.a

Abbreviations: CK, CyberKnife; CR, complete regression; LN, lymph node; P, progression; PR, partial regression; SABR, stereotactic ablative radiotherapy; SD, stable disease.
an = 31 lymph nodes.
Metastases to other organs occurred during the FU in 7 patients. Dissemination of the disease was found in 1 case, 1 month after the CK SABR; in 2 cases, 3 months after the radiosurgery; in 2 cases, 6 months after the treatment; and in 2 cases, 15 months after CK SABR. Only 2 patients had dissemination to other organs and local progression after CK SABR. During the FU, 2 patients died due to progression of the disease (20 and 21 months after CK SABR). One- and 2-year overall survival was 100% and 67%, respectively.
The PSA concentration decreased after the CK SABR. Six months after the radiosurgery, median of PSA concentration was 0.26. During the FU, the PSA level was stable, and at the last control, its median was 2.52 (range 0.00-258.0 ng/ml). The PSA concentration was lower at last control in patients without dissemination to other organs (P = .01). No correlation between TD of CK SABR and PSA concentration or regression of the size of treated LN was found with Mann-Whitney U test. In log-rank test, none of investigated factors was associated with statistically significant impact on overall survival—Gleason score ≥7 (P = .158), primary stage ≥III (P = .475), PSA at diagnosis >20 ng/mL (P = .180), ECOG performance status (P = .076), TD in CK SABR ≥30 Gy (P = .626), presence of other metastases (P = .086), or number of treated metastases (P = .856). Also none of these factors was associated with statistically significant impact on LC in log-rank test—Gleason ≥7 (P = .970), primary stage ≥III (P = .069), PSA at diagnosis >20 ng/mL (P = .566), ECOG performance status (P = .893), TD in CK SABR ≥30 Gy (P = .390), presence of other metastases (P = .053), or number of treated metastases (P = .131). Precise values of PSA median during the FU are shown in Table 6. Treatment results of particular patients are presented in Table 7.
Results—Median of PSA Concentration During the Follow-Up.

Abbreviations: CK, CyberKnife; PSA, prostate-specific antigen.
Treatment Results of Particular Patients.

Abbreviations: ADT, androgen deprivation therapy; CR, complete regression/response; Diss. distant metastases; DoD, dead of disease; fd, fraction dose; FU, follow-up; Gl, Gleason; HT, hormonal therapy; m, metastases; N/A, not available; PROG, progression in size of lymph node; PR, partial regression in size of lymph node; PSA, prostate-specific antigen; RT, radiotherapy; RT(n), radiotherapy (nodes); S, surgery; SD, stable size of lymph node; TD, total dose; Y, yes.
Discussion
Evaluation of the results is not easy because of the retrospective nature of this study and the small number of patients included. The dosing of metastases was quite variable for several reasons. First, as we started to treat patients with CK in 2011, there were only a few available studies with SBRT for metastatic LNs and only Jereczek-Fossa described 14 patients with metastatic LNs of PC who received this treatment (other authors described the treatment of patients with gastric cancer, colorectal cancer, and gynecological malignancies). 16,9,20,24 As shown in Table 8, total and fds varied among those studies. What is more, the location of LNs (paraaortic and pelvic) treated and the previous treatment (some patients had been irradiated before SBRT) varied among these authors. Second, as 94% of our patients received radiotherapy in primary treatment (and 56% on LN regions), we were worried about possible toxicities, and some patients treated in 2011 to 2012 received lower total dose (especially those who had metastases in pelvic LN). As other studies (with higher total and fds and no toxicities observed) were published, we decided to increase total and fds hoping that we could achieve better LC of the metastases. In 2013, patients were treated with total and fd of 24 to 36 Gy and 8 to 12 Gy, respectively. At present, based on recent studies and our own experience, patients with metastatic LNs of PC are usually treated with total dose of 45 Gy in 3 fractions of 15 Gy (depends on previous treatment, time between previous irradiation if patient had been treated with radiotherapy, location of the metastatic LN, and dose delivered to organ at risk).
SBRT of Abdominal LN Oligometastases—Review of Literature.

Abbreviations: CK, CyberKnife; CR, complete response; FR, fraction dose; FU, follow-up; LC, local control; LN, lymph node; OS, overall survival; PFS, progression free survival; PR, partial response; SABR, stereotactic ablative radiotherapy; SBRT, stereotactic body radiotherapy; SD, stable disease; TD, total dose; tox, toxicity.
The relatively small number of analyzed cases and short time of observation do not allow for evaluation in subgroups. Despite these issues, the obtained results are encouraging and show that CK SABR could be a feasible approach for PC nodal oligometastases. The SBRT seems to be particularly advantageous in case of previously irradiated lesions and small volume tumors (extreme hypofractionation cannot be applied to large volumes). Hypofractionation used in CK SABR could be of particular value for PC—recent studies suggest that PC may benefit from hypofractionation due to its low α/β ratio. 10
Only a few reports concerning SBRT and CK SABR treatment of PC LN metastases have been published to date. 9,10,11 Groups presented in those publications are also small (comparable to ours), which makes their interpretation difficult.
Results obtained in our study are similar to those in articles relating to treatment of patients with PC LN metastases. Progression of the size of treated LN was observed in our group at the end of FU in 2 patients and other authors report no in-field progression. 9,10,11 Patients presented in those reports had single or a very limited number of metastases. In our study, 9 patients had 2 to 4 treated metastatic LN that could have affected our results. 9,10,11 Similar observations were reported by Bignardi et al, in which patients with solitary LN metastasis had significantly longer progression-free survival. 18 In-filed progression and statistically significant correlation between the response of the size of treated LN observed in Bae et al’s report could suggest that higher doses are needed to provide better LC and more careful patient selection should be considered. 21
Androgen deprivation therapy is a standard treatment for patients with metastatic or recurrent PC. 6 Some patients receive conventional palliative RT to manage metastases in case of symptoms increase, but this is not the standard treatment and most of them have substantial disease progression. To our knowledge, there is only 1 randomized phase II trial comparing stereotactic radiation therapy (SRT) or surgery versus active surveillance with the commencement of ADT at time of progression in patients with oligometastatic disease (http://clinicaltrials.gov: NCT01558427). In 2013, the previously mentioned trial started recruiting patients and an estimated completion date is May 2017. As no other local treatment options are available, use of SARB seems to be a potential alternative compared to only ADT (with or without palliative RT). In 2 of the 3 cited studies concerning treatment of PC LN metastases, patients were taking ADT during the SABR (57% and 75% of patients), and a combination of these 2 treatment methods seems to provide LC and PSA concentration response. 9,10 In case of multiple metastases as reported in a third study conducted by Berkovic et al, ADT was introduced after SABR and the PSA concentration level increased, resulting in 1 year of no ADT, in 82% of treated patients. 11 It has been proven that ADT improves RT effectiveness in patients treated with curative intention and prolongs the overall survival and progression-free survival in this group. 33 There are no studies that prove that ADT acts differently in patients with metastatic or localized disease so it might also improve effectiveness of SABR. Further studies are needed to compare the results of SABR with and without ADT in patients with PC having metastatic LN.
Publications referring to SABR of abdominal LN are numerous but still only a few have been published so far 17,18,19 –21,23 –25,27,28 , and there is still no consensus about optimal TD and fd. In 4 reports, colorectal cancer was the primary disease 18,21,23,13 and in 2 reports, the results of treatment of metastases from gynecologic malignancies were described. 17,20 Results of SABR treatment of LN metastases originating from other cancers also showed a high rate of LC (60 to 95—100%) and progression usually outside the treated field observed in 5% to 62% of treated patients during the FU. 17,18,19 –21,23 –25,28
The TDs used in cited studies ranged from 20 to 60 Gy and were comparable with doses used in our institution, however, a greater TD of 45 Gy was used in our institution. 9 –11,17 –21,23 –25,27,28 Despite that the obtained results are good in terms of LC and could be a first step in the estimation of the optimal treatment dose.
Toxicities observed in our group and in cited studies are low and only a small number of patients had developed late complications (in all patients treated in cited articles ,10 had grade 3 toxicity, 2 had grade 4 toxicity, and 1 patient died due to intestinal perforation). It is unlikely that late toxicities of grade 1 seen in our group are related to SABR (treated LN sizes: 17-21 mm, TD of CKRS 24 and 45 Gy) and it is more likely that they are the results of previous irradiation (doses delivered to the rectum and bladder were much higher and cover much more volume of those organs than doses delivered with CK SABR), surgery, and the patients’ age (65 and 77 years).
A review of results and treatment factors in cited studies is presented in Table 8.
Conclusions
Based on the results obtained and discussion, it can be concluded that CK SABR of PC LN oligometastases seems to be a safe and effective treatment modality, causing lesion regression and decreasing PSA concentration.
Footnotes
Authors’ Note
All authors certify that this manuscript has not been published in whole or in part nor is it being considered for publication elsewhere.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.