
Abstract
Introduction:
Whole-gland salvage treatment of radiorecurrent prostate cancer has a high rate of severe toxicity. The standard of care in case of a biochemical recurrence is androgen deprivation treatment, which is associated with morbidity and negative effects on quality of life. A salvage treatment with acceptable toxicity might postpone the start of androgen deprivation treatment, might have a positive influence on the patients’ quality of life, and might even be curative. Here, toxicity and biochemical outcome are described after magnetic resonance imaging–guided focal salvage high-dose-rate brachytherapy in patients with radiorecurrent prostate cancer.
Materials and Methods:
Seventeen patients with pathologically proven locally recurrent prostate cancer were treated with focal high-dose-rate brachytherapy in a single 19-Gy fraction using magnetic resonance imaging for treatment guidance. Primary radiotherapy consisted of external beam radiotherapy or low-dose-rate brachytherapy. Tumors were delineated with Ga-68–prostate-specific membrane antigen or F18-choline positron emission tomography in combination with multiparametric magnetic resonance imaging. All patients had a prostate-specific antigen level of less than 10 ng/mL at the time of recurrence and a prostate-specific antigen doubling time of ≥12 months. Toxicity was measured by using the Common Terminology Criteria for Adverse Events version 4.
Results:
Eight of 17 patients had follow-up interval of at least 1 year. At a median follow-up interval of 10 months (range 3-40 months), 1 patient experienced a biochemical recurrence according to the Phoenix criteria, and prostate-specific membrane antigen testing revealed that this was due to a distant nodal metastasis. One patient had a grade 3 urethral stricture at 2 years after treatment.
Conclusion:
Focal salvage high-dose-rate brachytherapy in patients with radiorecurrent prostate cancer showed grade 3 toxicity in 1 of 17 patients and a distant nodal metastasis in another patient. Whether this treatment option leads to cure in a subset of patients or whether it can successfully postpone androgen deprivation treatment needs further investigation.
Introduction
The high incidence of radiorecurrent prostate cancer poses a significant problem in clinical practice. 1,2 Up to 50% of patients may experience a recurrence within 10 years after primary radiotherapy, 1,3,4 and some of these recurrence will be purely local. Zumsteg et al analyzed recurrences in 2694 patients and found true local recurrences to be the most common form of first recurrence. 2 Eight-year cumulative rates of local recurrence in the prostate were 3.5%, 9.8%, and 14.6% for patients with low-, intermediate-, and high-risk disease. 2
For patients diagnosed with recurrent prostate cancer after primary radiotherapy, various whole-gland salvage options have been described, such as salvage radical prostatectomy, salvage brachytherapy (BT), salvage high-intensity frequency ultrasound (HIFU), and salvage cryosurgery. All of these treatment options have been described in retrospective studies. Some of these studies showed significant failure rates and rates of late toxicity of up to 30%.
5
–9
Severe toxicity consisted of grade
In case of a biochemical recurrence, androgen deprivation treatment (ADT) is the most common treatment worldwide, with approximately 98% of patients being treated in this manner. 12 However, hormonal therapy is associated with significant side effects and has a major influence on QoL. 13,14
Currently, new magnetic resonance imaging (MRI) and positron emission tomography (PET) have become available in clinical practice; these modalities have a high sensitivity and specificity to detect local recurrence in the prostate as well as early metastases. Available imaging techniques for clinical practice include multiparametric MRI (mp-MRI), F18 or C11-choline PET, and 68 Gallium (Ga)-prostate-specific membrane antigen (PSMA) PET-computed tomography (CT). 15 –24
Current studies indicate that radiorecurrences in prostate cancer occur mainly at the site of the index lesion, 25 –27 suggesting that the delivered dose from the primary treatment may not have been sufficient to eradicate all tumor cells. Focal salvage HDR-BT with a high dose to the recurrent lesion may eliminate all prostate cancer cells and prevent another local recurrence or potential future metastasis. The clinical benefit of focal HDR-BT could be cure or postponement of ADT and therefore preservation of QoL by preventing or postponing its severe toxicity.
Several studies regarding focal/hemigland salvage low-dose-rate (LDR) BT of the prostate have already shown this treatment modality to be feasible and safe. 5,6,28,29 Still, a further reduction in treatment volume may be expected when using mp-MRI because it is often possible to clearly identify the gross tumor volume (GTV) and therefore allow truly focal treatment, possibly with less gastrointestinal (GI) and GU toxicity. Magnetic resonance imaging guidance during the procedure allows it to be adaptated to address changes in anatomy and provides an online check of the catheter position and real-time adaptation of the treatment plan if the anatomy changes significantly.
In this study, we describe biochemical outcomes and toxicity after a single 19-Gy fraction of focal salvage HDR-BT guided by a 1.5 T MRI scanner in an outpatient setting.
Materials and Methods
Patients
From July 2013 through June 2016, 17 patients were treated with MRI-guided focal salvage HDR-BT. All patients had a localized prostate cancer recurrence after prior radiotherapy.
Before salvage treatment, all patients underwent 18F-choline PET-CT or 68-Ga-PSMA PET-CT to exclude distant metastases. All recurrences were pathologically proven. Biopsies to detect recurrence were done with a focal transperineal MR-guided procedure. All patients had a recurrence at least 2 years after the primary treatment. At the time of salvage treatment, prostate-specific antigen (PSA) levels were all below 10 ng/mL, the PSA doubling time (DT) was above 12 months, and all patients had International Prostate Symptom Score (IPSS) of less than 15 before focal salvage HDR-BT. All recurrences were T2 as measured by MRI.
This study was approved by our local institutional review boards, and written informed consent was obtained from all patients.
Treatment Procedures
Before treatment, all patients underwent diagnostic MRI with a 3.0 T MRI scanner. A T2-weighted, diffusion-weighted imaging sequence and a dynamic contrast-enhanced sequence were used to delineate the GTV and organs at risk (OARs). A T1-weighted sequence was used to exclude bleeding artefacts, for example, caused by biopsies. Scanning with F18-choline PET-CT or 68-Ga-PSMA PET-CT was used to confirm GTV location and exclude metastatic disease. A margin of 5 mm was added around the GTV within the prostatic contour to obtain the clinical target volume (CTV). No margin was used around the CTV to form a planning target volume, because in HDR BT, the source and dose distribution move along with the tumor.
During treatment, the MR images were imported in Oncentra Prostate (Elekta, Veenendaal, the Netherlands) and intraoperatively rigidly registered with real-time-acquired transrectal ultrasonography images based on the prostate contour, and emphasis was put on a best possible match for the GTV. Catheters were inserted transperineally through a specially designed, manually deconstructable template. The number of catheters placed depended on the CTV volume and shape and its relation with the OARs. After catheter placement, the patient was transported to the 1.5 T MR scanner (Ingenia, Philips Medical Systems, Best, the Netherlands), and catheter reconstruction was done based on the newly acquired MR images. The intraoperative MRI consisted of series of transversal T2-weighted turbo spin echo images and 2 series of 3-dimensional balanced turbo gradient echo images, one with spectral attenuated inversion recovery and one with spectral presaturation with inversion recovery. No endorectal coils were used. All contours were transported from the pretreatment 3.0 T MRI scanner to the intraoperative 1.5 T MRI scanner through rigid registration, followed by manual adaptation of delineations, eg, due to intraoperative swelling. Contours were adjusted by the radiation oncologists to account for prostate swelling and movement of OARs. The urethra was identified by the urethral catheter. Afterward, the final treatment plan was generated based on the adapted MR delineations and catheter positions using dose-volume histogram-based inverse optimization. Then, the single fraction of 19 Gy was administered. Figure 1 shows the MRI/HDR treatment setup. Focal irradiation was delivered in a single fraction. The dose prescribed to the CTV was defined as 19 Gy to at least 95% of the volume (D95) of the GTV. Constraints for the rectum and bladder were defined in terms of D1 cc, that is, a dose to 1 cc of rectum or bladder of <12 Gy; the constraint for the urethra was a dose to 10% of the urethra (D10%) of <17.7 Gy. All treatments were done on an outpatient basis.

Depiction of the treatment area. The patient is lying on the magnetic resonance imaging table and has the catheters inserted in the clinical target volume in the prostate. The high-dose-rate (HDR) afterloader is connected to the different catheters for HDR delivery.
Toxicity Assessment and PSA Measurements
Toxicity was assessed with the Common Terminology Criteria for Adverse Events version 4 and, with PSA monitoring, was reported at 4 weeks after treatment and subsequently every 3 months during the first year after treatment, every 6 months during the second year, and annually thereafter. Patients with biochemical failure according to the Phoenix definition (nadir PSA + 2 ng/mL) were reassessed for local recurrence an distant metastases. For patients with a biochemical failure according to the Phoenix definition, follow-up imaging was done with Ga-68-PSMA.
Results
Baseline Characteristics
Table 1 shows patient characteristics. Median follow-up time was 10 months (range 3-40 months). Eight of 17 patients had follow-up for at least 1 year. The age of the treated patients ranged from 58 to 78 years, with a median of 69 years. At the time of primary treatment, 4 patients had stage T3 disease and the other 13 patients did not have extracapsular extension at that time. One patient had a Gleason score of 8 before primary treatment, and all other patients had a Gleason score of 7 (4 + 3) or less. The PSA leavel at primary treatment was a median 13.2 ng/mL (range 3.3-28 ng/mL). For 9 patients, the primary treatment was LDR-BT with I-125 seeds, and the other 8 patients received external beam radiotherapy (EBRT). Median time to relapse was 8 years (range 2.5-19 years). Median PSA level before salvage was 4.8 ng/mL (range 0.89-6.8 ng/mL) and the PSA-DT was 17 months (range 12-40 months). The median IPSS was 7 (range 1-18). All patients had an IPSS score of <15 except for 1 patient with an IPSS score of 18. At intake, however, his urinary complaints did not match an IPSS score of 18, and so a formal exception was granted and this patient was included in the study.
Patient Characteristics.a,b

Abbreviations: EBRT, external beam radiotherapy; I-125, iodine 125 seed brachytherapy; IPSS, International Prostate Symptom Score; NA, not applicable; PSA, prostate-specific antigen.
aAccording to the D’Amico risk classification, 1 patient (patient 15) had low-risk disease, 9 had intermediate-risk disease (patients 4, 6, 7, 8, 9, 11, 14, 16, and 17), and 7 had high-risk disease (patients 1, 2, 3, 5, 10, 12, and 13).
bGleason score is often difficult to determine in recurrent prostate cancer.
Biochemical Outcomes
In total, 6 of 17 patients had a PSA rise of 0.2 ng/mL or more during follow-up, and 1 patient had a biochemical recurrence per the Phoenix criteria. That patient developed multiple distant metastases visualized on a 68-Ga-PSMA PET-CT scan. Prostate-specific antigen values dropped in all other patients. Prostate-specific antigen curves for all patients are depicted in Figure 2. Biochemical disease-free survival is depicted in Figure 3. The Kaplan-Meier biochemical disease-free survival estimate at 12 months was 92% (95% confidence interval 77%-100%).
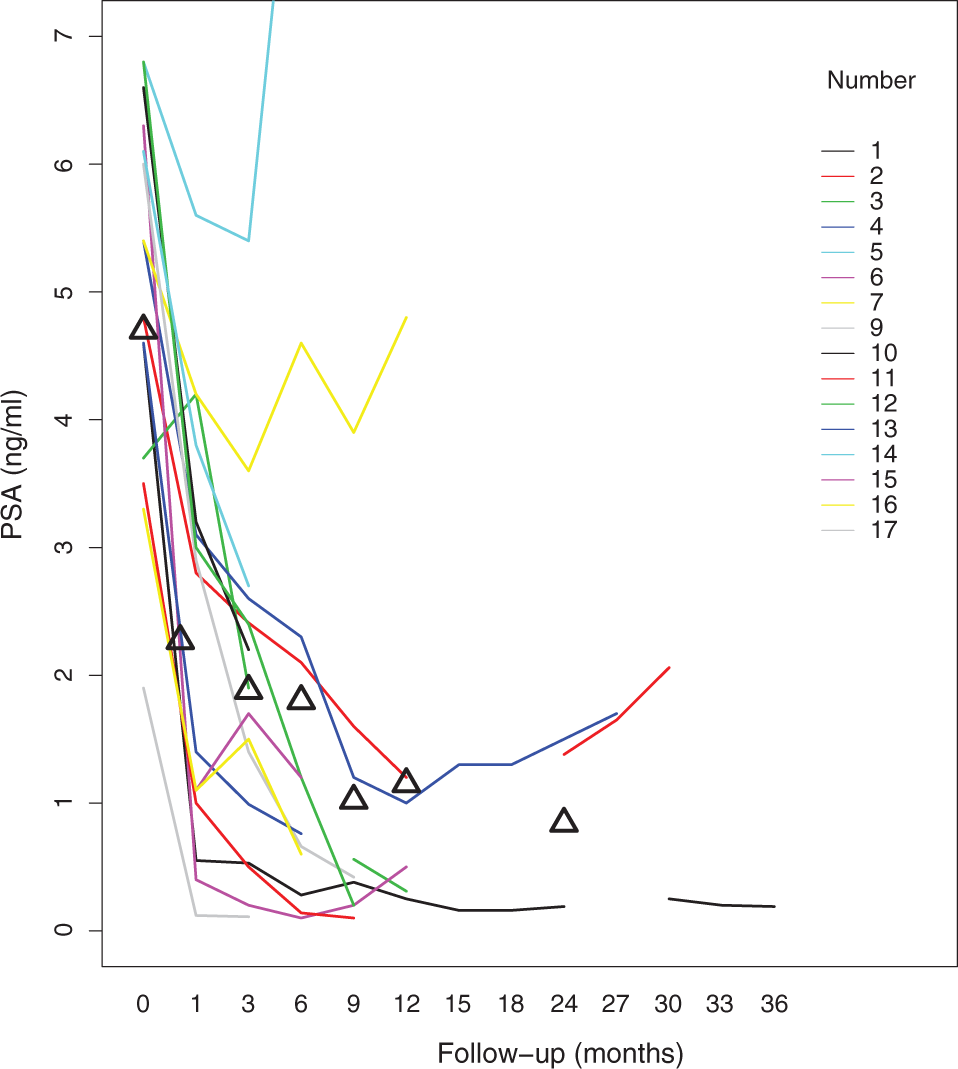
Prostate-specific antigen levels, in ng/mL, for all 17 patients after treatment of recurrent prostate cancer.

Kaplan-Meier estimate of biochemical disease-free survival for 17 men after treatment of recurrent prostate cancer. The gray shading indicates the 95% confidence interval.
Toxicity
Toxicity scores over time are shown in Table 2.
Common Terminology Criteria of Adverse Events V4.0 Toxicity Scores
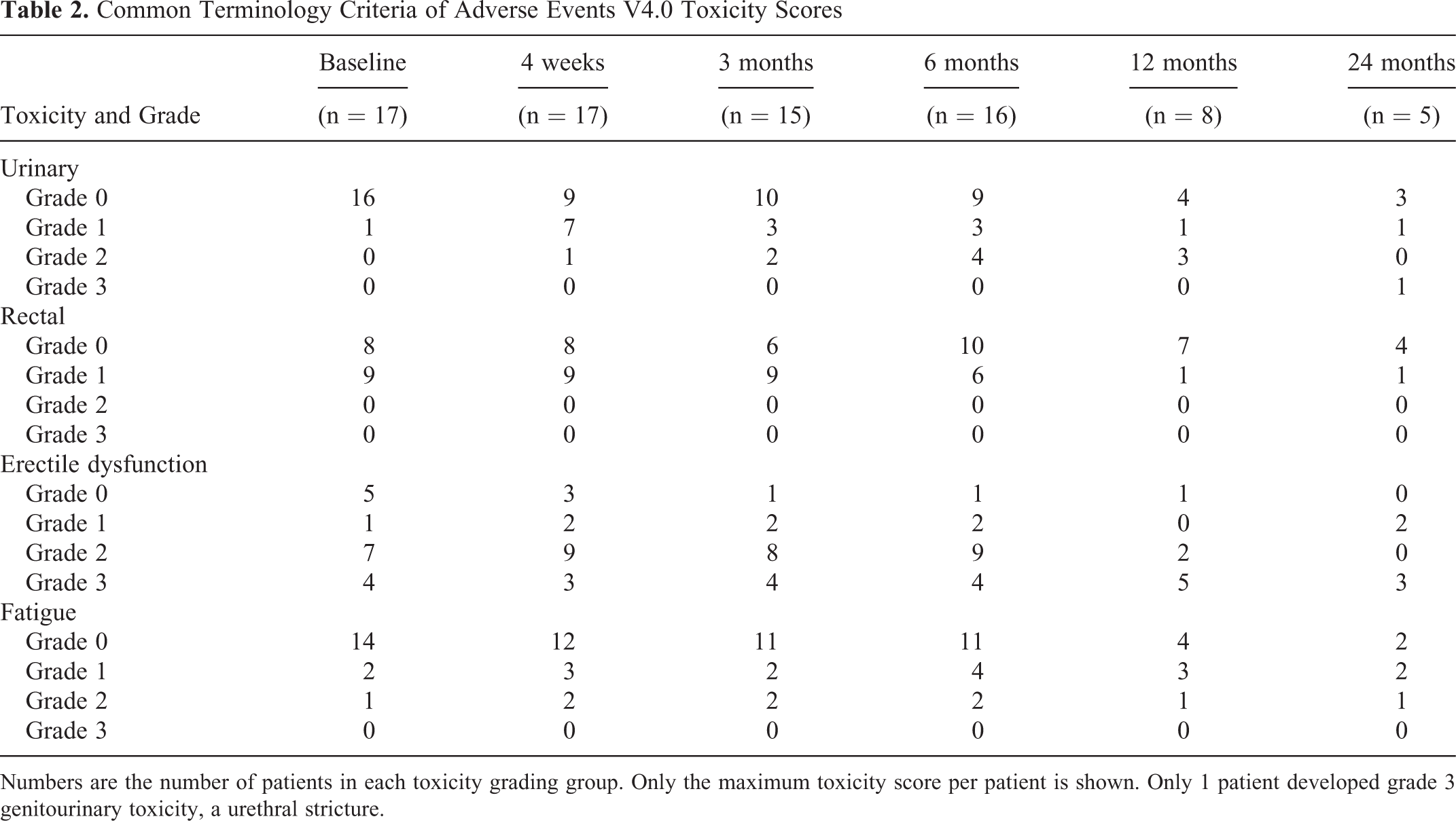
Numbers are the number of patients in each toxicity grading group. Only the maximum toxicity score per patient is shown. Only 1 patient developed grade 3 genitourinary toxicity, a urethral stricture.
Acute toxicity (defined as toxicity occurring within the 90 days after treatment) was limited. For urinary toxicity, only 2 patients developed grade 2, and no patient had grade 3. For rectal toxicity, none of the patients showed grade 2 or 3. Two patients developed grade 2 fatigue.
Late toxicity was defined as toxicity occurring more than 90 days after treatment. For urinary toxicity, 2 additional patients (4 in total) developed grade 2 toxicity. One patient who did not have GU toxicity at baseline developed a grade 3 urethral stricture 2 years after treatment. The CTV in this patient was 9 cc and the tumor fully surrounded the urethra and was partly abutting the internal urinary sphincter. This patient had a D10% urethra of 17.9 Gy, which slightly exceeded the prescribed constraint of 17.7 Gy. For rectal toxicity, no patients developed grade 2 or 3 late toxicity. No patients had grade 2 or 3 late fatigue.
Among the 6 patients with no (n = 5) or grade 1 (n = 1) ED at baseline, 1 patient developed grade 3 ED at 6 months, 2 patients grade 2 ED, and 1 patient grade 1 ED. Of the patients with grade 2 (medication-assisted) ED (n = 7) or grade 3 ED (n = 4) at baseline, 1 patient developed a grade 3 new ED. Furthermore, 2 patients with grade 3 ED showed declines, 1 to grade 2 and 1 to grade 1 ED.
Dosimetry
Prostate volumes ranged from 15.4 to 42.1 cc with an average of 31.7 cc. The average CTV was 7.4 cc (range 3.2-14.8 cc). A median of 9 catheters were placed (range 6-13).
In 9 patients, the D95 to the CTV was more than 19 Gy. In 8 patients, the delivered dose was less than 19 Gy to spare the OARs and to meet the constraints for rectum and bladder. The urethral constraint (D10% < 17.7 Gy) was exceeded in 4 patients, with a maximum of 18.2 Gy. The dosimetry results are presented in Table 3.
Treatment Dosimetric Characteristics

Abbreviations: AVG, average; CTV, clinical target volume; IQR, interquartile range; SD, standard deviation.
Discussion
Magnetic resonance imaging–guided, 19-Gy single-fraction HDR-BT for focal salvage in radiorecurrent prostate cancer was well tolerated with regard to acute toxicity, especially when compared with the results of different whole-gland salvage procedures and techniques described elsewhere.
In our study, acute toxicity was limited and was not severe (grade 3 or higher). The only grade 3 urethral stricture observed in this series occurred 2 years after treatment. Because follow-up in this series was limited to more than 1 year in 8 patients and was more than 2 years in only 4 patients, caution is needed in interpretating these results. A recent study of whole-gland salvage treatment for 33 patients showed a 15% rate of late grade 3 GU toxicity at 5 years. 11 With a median follow-up time of only 10 months in the current study, extended results are necessary to further assess the frequency of late toxicity. The only grade 3 urethral stricture observed in this series occurred at 2 years after treatment. In that specific case, the tumor completely surrounded the urethra and part of it was against the internal urinary sphincter, which may have prompted this complication. However, other patients with tumors around the urethra, with a comparable dose to the urethra and similar dose gradients, did not experience stricture.
Biochemical outcomes were good, despite the short follow-up time; only 1 patient experienced a PSA recurrence and distant metastases. In that patient, a choline PET scan was obtained before salvage therapy, after which his PSA rose to 15 ng/mL at 9 months (PSA-DT 4 months). This was interpreted as a subclinical metastasis that was not detected on the pretreatment PET. The nodal metastasis after salvage treatment was detected with a PSMA-PET. Still, follow-up should be extended to indicate that our focal salvage approach has at least comparable biochemical outcomes to current whole-gland and other focal salvage modalities. The use of the Phoenix definition in this study can be questioned, as it was not designed for salvage. However, to establish such a definition, large series are required. Also, detection of recurrence by using advancing imaging techniques such as use of Ga-68-PSMA in the current case will enable better exclusion of patients with metastases, which will improve outcome.
A 19-Gy single-fraction dose for salvage has not been previously reported. Single-fraction HDR to 19 Gy has been described for primary whole-gland treatment as a way of excluding interfraction catheter movements in an outpatient setting. 30 At the center of the CTV, especially around the catheters, the delivered dose can be extremely high. Therefore, we believe that the dose to the macroscopic tumor can be expected to have a significant ablative effect. In the patient with the salvage relapse, the interval between primary and salvage treatment was 2.5 years, but the PSA-DT was relatively short at 12.1 months. A short disease-free survival time and short PSA-DT may be predictors of subsequent treatment failure in whole-gland salvage iodine-125 BT, 31 which might explain the early progression in this patient.
Limited literature on the CTV margin to be used in a salvage setting is limited. Baumann et al 11 used a margin of 5 mm and found limited toxicity rates. We used the data of Groenendaal et al, which described a 5-mm margin to be sufficient for the treatment of primary disease. 32 The currently available whole-gland salvage pathology studies 25,26,33 do not provide data on an appropriate CTV margin.
One other study described MRI (and PET-CT)-guided focal salvage HDR-BT for 2 patients. 34 Those 2 patients experienced no acute or late toxicity at a follow-up time of 6 months. A range of focal salvage techniques has been described, including cryosurgery, iodine-125 BT, and HIFU, with patient numbers ranging from 15 to 91. However, none of these studies used intraoperative MRI guidance, and only a subset used MRI in treatment planning. Biochemical disease-free survival rates range from approximately 50% to 91% at 3 years. Even though rates of severe GU and GI toxicity seem reduced, some significant toxicity has been reported. 35 Our preliminary results compare favorably with results from these focal salvage modalities in terms of both cancer control and toxicity. In a larger series, it would be interesting to compare patients whose primary treatment was EBRT with those who received BT to clarify toxicity and tumor control after salvage with these different treatments.
This study had some limitations. Patient numbers were small (n = 17) and follow-up was limited to a median of <1 year. Larger patient numbers and longer follow-up intervals would enable more reliable assessment of biochemical control and late toxicity. Notably, the only grade 3 urethral toxicity occurred at 2 years after salvage treatment. This study is unique because, unlike most other studies, it was prospective and made use of MRI and PET/CT scans in a novel way. Multiparametric MRI provides optimal visualization of tumor recurrence within the prostate 32,36,37 and facilitates intraoperative visualization of the catheters. An important advantage is the possibility of “dose painting” through regulation of dwell positions and times, thereby further optimizing dose distribution. Especially for single-fraction focal salvage implants, stable catheter positions and a check on anatomic variations during the complete BT procedure are important. 38 –40
Conclusion
Focal salvage HDR-BT for 17 patients with radiorecurrent prostate cancer showed grade 3 toxicity in only 1 of these patients, and another patient developed a distant nodal metastasis. Whether this treatment option leads to cure in a subset of patients or whether it can successfully postpone ADT needs further investigation.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the following financial support for the research, authorship, and/or publication of this article: Supported in part by Cancer Center Support (Core) Grants from the US National Cancer Institute, National Institutes of Health, to Dana Farber Cancer Center and The University of Texas MD Anderson Cancer Center.