
Abstract
Objective:
To compare dose distributions of postoperative plans with preoperative plans for radioactive seed implantation of paravertebral/retroperitoneal tumors assisted by 3-dimensional printing noncoplanar templates and computed tomography.
Methods:
Sixteen patients with paravertebral/retroperitoneal tumors (21 lesions) underwent radioactive seed implantation with 3-dimensional printing noncoplanar templates. Prescribed dose was 110 to 160 Gy. We compared the dose distribution of the postoperative plan with the preoperative plan. Dose parameters were D90, minimum peripheral dose, V100, V150, conformal index and external index of the target volume, and the dose received by 2 cm3 of normal tissue of organs at risk (spinal cord, aorta, and kidney).
Results:
Sixteen 3-dimensional printing noncoplanar templates were produced for 21 treatment areas. Mean gross tumor volume (preoperative) of patients was 61.1 cm3, mean needle number was 17, mean number of implanted 125I seeds was 65, and mean D90 of postoperative target area (gross tumor volume) was 131.1 Gy. Actual number of seeds postbrachytherapy increased by 1 to 12 in 8 cases. For postoperative plans, the mean D90, minimum peripheral dose, V100, V150 was 131.1 Gy, 67.1 Gy, 90.2%, and 64.1%, respectively, and 135.0 Gy, 64.7 Gy, 90.9%, and 64.1%, respectively, in preoperative plans. Comparing with the preplanned cases, the dose of the target volume was slightly lower and the high-dose area of the target volume was larger in postoperative cases, but the difference was not statistically significant (P > .05). Actual dose conformity of the target volume was lower than preplanned, and the difference was statistically significant (P = .005).
Conclusion:
Three-dimensional printing noncoplanar templates can provide good accuracy for positioning and direction in radioactive seed implantation.
Introduction
The effect of radioactive seed implantation (RSI) in the treatment of prostate cancer has been confirmed. 1 However, RSI also has an important role in therapy of nonprostatic tumors. 2 –5 The dose distribution is the most important factor affecting the therapeutic effect of RSI. 6 With improvements in computer and imaging technology, brachytherapy treatment planning systems (BTPSs) have been used widely for the planning and design of RSI. However, RSI under pure image guidance can be affected by anatomic factors, clinical experience, and consistency between the preoperative dose and postoperative dose.
For tumors of the head and neck, the use of 3-dimensional printing individual noncoplanar templates (hereafter known as “3D printing noncoplanar templates” [3DPNCTs]) can be helpful. Using a 3DPNCT, the implantation needle can avoid blood vessels and bones to realize noncoplanar and multiple-angle insertion, which improves the accuracy and safety of RSI. 7 However, few data are available for the preoperative plan and postoperative plan after use of 3DPNCTs (ie, whether the postoperative dose can achieve the dose anticipated before brachytherapy).
The present study compared the result of preoperative dosimetry and the result of postoperative dosimetry of RSI for paravertebral/retroperitoneal malignant tumors assisted by 3DPNCTs and computed tomography (CT) guidance. Also, we verified the application accuracy of this technology at the planning level.
Materials and Methods
Ethical Approval of the Study Protocol
The ethics committee of Peking University Third Hospital (Beijing, China) approved our study protocol. All patients provided written informed consent to participate in this study.
General Clinical Data
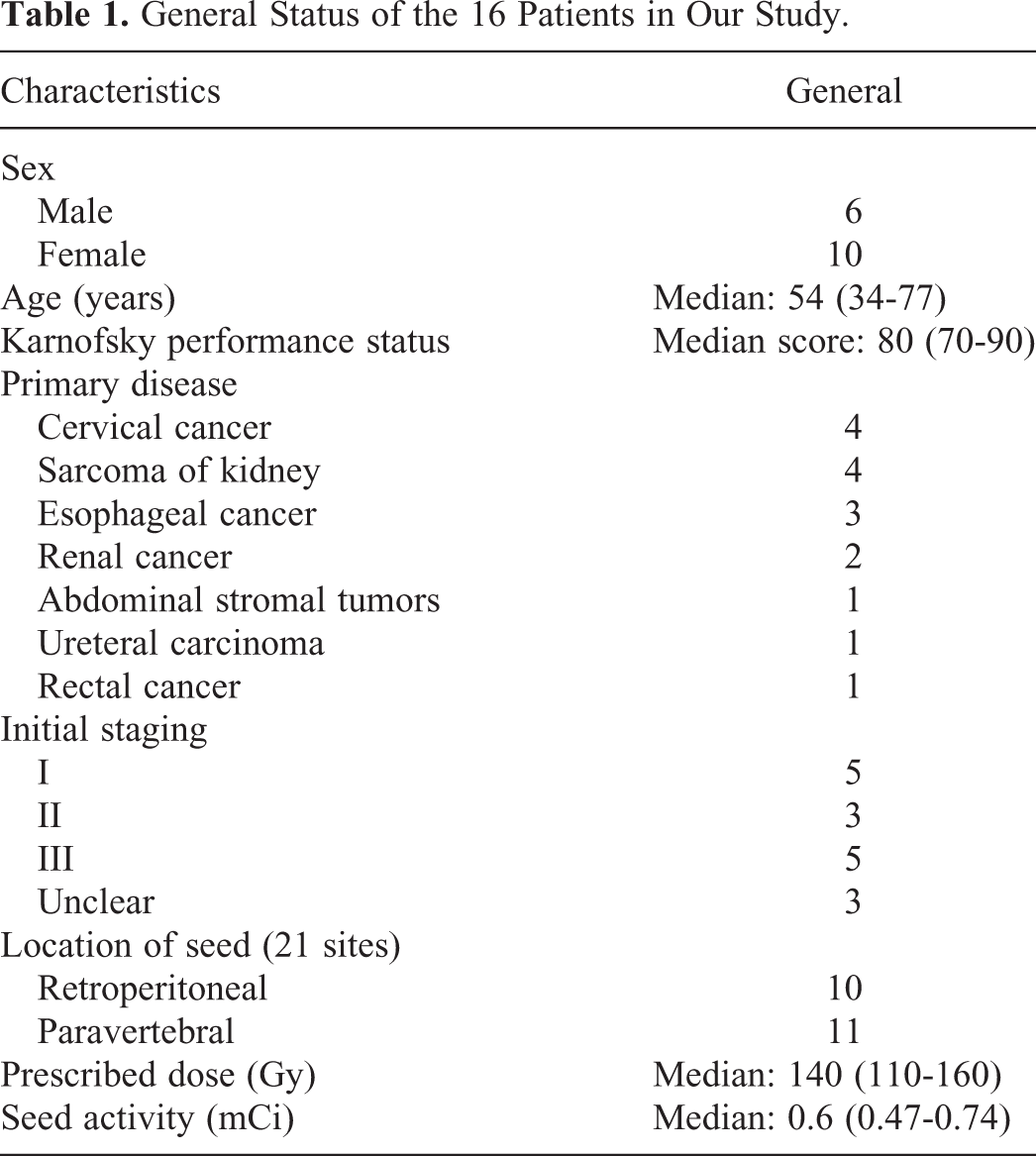
Sixteen patients (21 lesions) with a paravertebral/retroperitoneal malignant tumor undergoing implantation of 125I seeds with a 3DPNCT and CT guidance in our center from December 2015 to December 2016 were selected. The basic information of these patients and their tumors is shown in Table 1. According to the literature and clinical experiences gained at our center, 110 to 180 Gy is the dose range that elicits a good therapeutic effect. 2,4,8 –14 The dose prescribed in our study was set at 110 to 160 Gy.
General Status of the 16 Patients in Our Study.
Materials and Equipment
125I seeds (BT-125-I) with a half-life of 59.4 days and dose rate constant of 0.965 cGy/(h·U) were obtained from Shanghai GMS Pharmaceuticals (Beijing, China). A Mick radionuclear instrument (Eckert & Ziegler BEBIG, Berlin, Germany) was used for all treatments. A Seed Implantation Planning System-3D BTPS (Beijing University of Aeronautics and Astronautics, Beijing, China) was employed. The source configuration data of this BTPS was referred to as “TG43” according to recommendations by the American Association of Physicists in Medicine. 15,16 We used 3-D imaging and reverse-engineering software (Magics 19.01; Materialise, Leuven, Belgium). We also used a 3-D printer (UnionTech RS6000; Shanghai Union Technology, Shanghai, China) with an accuracy of 0.1 mm, and the printing material was light-cured resin.
Design of the Preoperative Plan
All patients underwent CT (Brilliance Big Bore; Philips, Amsterdam, the Netherlands) 2 days before brachytherapy. The slice thickness was 5 mm, and a vacuum pad was used to fix the body position. The positioning line and alignment reference line of the template were marked on the surface of the patient. The CT data were transmitted to the BTPS to design the preoperative plan (Figure 1), which mainly comprised drawing of the gross tumor volume (GTV); setting of the prescribed dose and activity of 125I seeds; determination of the implantation needle path (direction, depth, and distribution); simulation of the spatial distribution of 125I seeds; and calculation of dose distribution of the target volume and organs at risk (spinal cord, large vessels, and adjacent organs). The dose received by 90% of the GTV (GTV D90) achieved the prescribed dose as much as possible. Also, the doses received by the organs at risk were as low as possible using optimization.
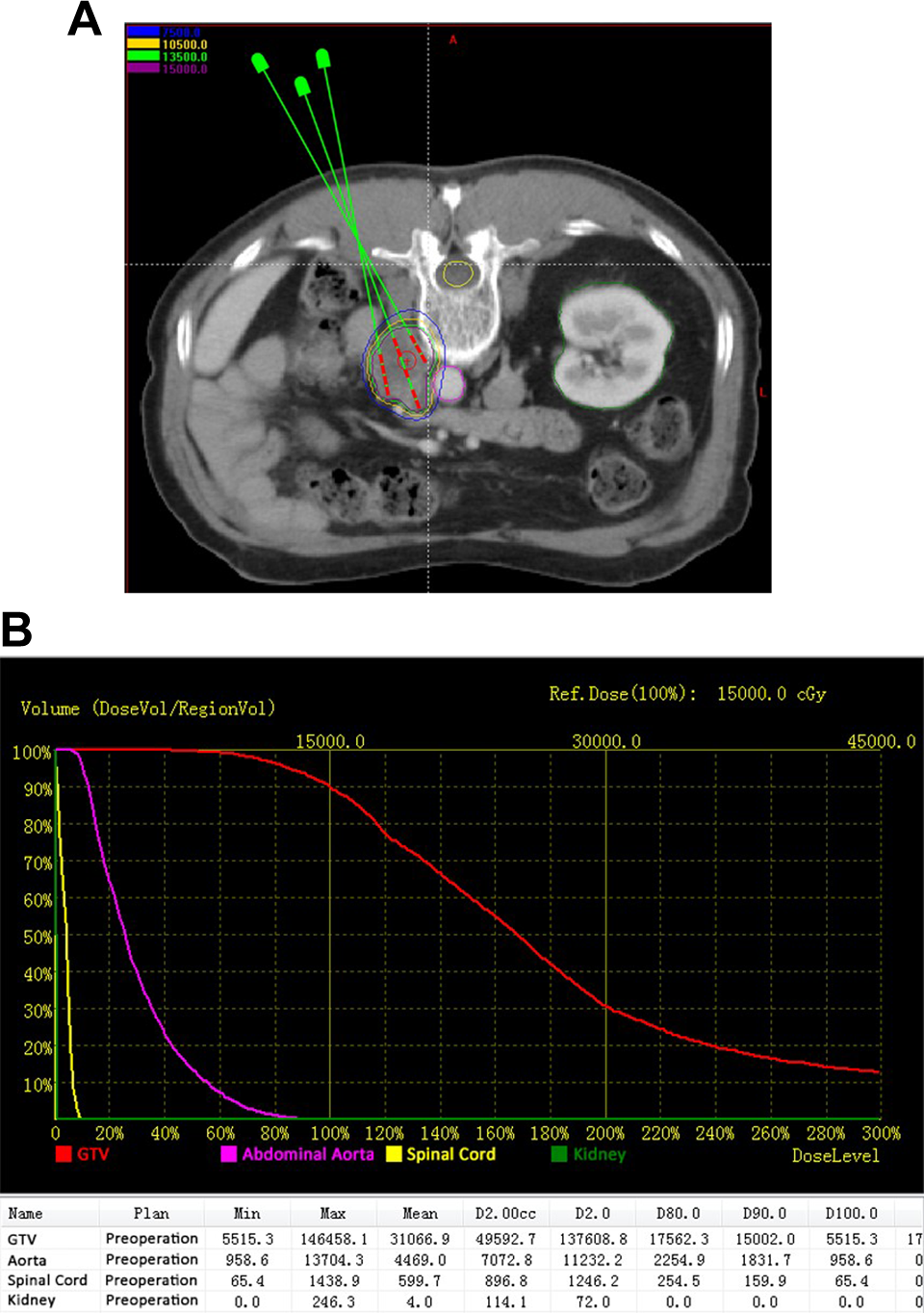
Preoperative planning design. A, Determining the needle tract, calculating the dose distribution of target volume. B, Dose volume histogram of preoperative plan.
Design and Fabrication of an Individual 3DPNCT
The data in the BTPS were imported to Magics 19.01 to construct digital modeling for an individual 3DPNCT. Information about the needle-path direction was added to the model (Figure 2). The 3DPNCT was printed by the 3-D light-cured rapid-forming printer. The 3DPNCT included the biologic surface characteristics of the therapy area, a registered mark, and information on the simulated needle path; the first 2 were used to guide accurate alignment to the 3DPNCT, and the latter was used to guide needle implantation.

Individual template design.
Puncturing and RSI
The RSI was carried out under local infiltration anesthesia. The 3DPNCT was aligned to the surface of the therapy region by virtue of the outline characteristics of the patient; positioning line and 3DPNCT alignment reference line marked on the patient; register mark of the 3DPNCT; and positioning laser. The CT was performed before puncture to accurately determine the relative position of the 3DPNCT and tumor. If an error occurred, the error between the actual image and positioning image was measured and adjusted in real time. The implantation needle was used to puncture to the predetermined depth percutaneously through a guide hole in the 3DPNCT when the latter was aligned exactly. The CT was performed during puncturing to verify the position of the implantation needle (Figure 3), and “fine-tuning” was performed if necessary. Finally, 125I seeds were implanted with the radionuclear instrument. The CT was performed again upon completion of RSI to observe the actual distribution of 125I seeds; the latter were implanted again if the 125I seeds in the target volume were not distributed satisfactorily.

Actual distribution of inserted needles.
Verification of Postoperative Dosimetry and Comparison of the Plan
The final postoperative image was transmitted to the BTPS (Figure 4). The actual dose distribution in the target volume was evaluated by means of a dose–volume histogram. The verification result after brachytherapy was compared with the parameters corresponding to the preoperative plan: D90, volume percentage of the GTV receiving 100% of the prescribed dose (V100), volume percentage of the GTV receiving 150% of the prescribed dose (V150), and the minimum peripheral dose (MPD) of the GTV. The conformity of the dose distribution was evaluated using the CI via the following equation 17 :


Postoperative dosimetry verification. A, Actual dose distribution of postoperation. B, Dose volume histogram of postoperative plan.
where VT, VT, ref, and Vref are the target volumes (GTV), the volume of the target volume receiving the prescribed dose, and the total volume (cm3) in the prescribed dose, respectively. The best CI was 1, which means the GTV was just covered by the prescribed dose and the dose outside the GTV was lower than the prescribed dose. In general, the greater the value of the CI, the greater was the volume receiving the prescribed dose within the GTV, and the smaller was the volume receiving the prescribed dose outside the GTV. The volume exceeding the prescribed dose outside the GTV can be described by the EI 18 :

The best EI was 0. The dose received by tissue outside the GTV was smaller than the prescribed dose if the EI was 0. The greater the value of the EI, the greater was the prescribed dose received outside the GTV. The dose received by 2 cm3 of normal tissue (D2cc) was used to evaluate the dose of normal tissues (spinal cord, abdominal aorta, and kidney).
Results
Brachytherapy and Condition of Use of Individual 3DPNCTs
Sixteen individual 3DPNCTs were designed and fabricated for 21 therapy areas (lesions). Each 3DPNCT had, on average, 17 implantation needle paths (range 6-35). All patients received RSI under CT guidance with the assistance of a 3DPNCT. The preoperative mean volume of GTV of patients was 61.1 (4.0-263.0) cm3. The mean activity of a single 125I seed used was 0.6 (0.47-0.74) mCi. The mean number of puncturing needles was 18 (6-35). The mean number of seeds implanted was 69 (15-162). The mean seed activity of GTV implantation was 0.86 (0.42-1.63) mCi/cm3. The mean D90 of the postoperative GTV was 131.1 (90.2-167.4) Gy, and 62% of postoperative D90 was higher than the prescribed dose. The number of 125I seeds implanted for 8 patients was increased to 1 to 12 compared with the preoperative plan.
Dosimetry Verification and Comparison Results
The direction of the needle implanted was controlled accurately to ensure it was away from important organs and bones. Parameters such as D90, V100, V150, and MPD of the GTV, D2cc of normal tissue (spinal cord, abdominal aorta, and kidney) as well as the EI and CI of the 21 lesions in the preoperative plan and postoperative verification of RSI are listed in Table 2. The values of all parameters before and after brachytherapy were compared using the nonparametric Wilcoxon symbols test with P < .05 being considered significant (Table 3). The mean values of D90 and V100 after brachytherapy were smaller than those before brachytherapy, and the mean values of V150 and MPD after brachytherapy were greater than those before brachytherapy. All parameters in the 2 groups were not significantly different (P > .05). The mean value of the CI after brachytherapy was small compared with that before brachytherapy (0.56 and 0.64, respectively), and the difference was significant (P = .005). The mean value of EI after brachytherapy was greater than that before brachytherapy (62.3% and 40.8%, respectively), but the difference was not significant (P = .098). The mean dose (in Gy) given to the spinal cord, abdominal aorta, and kidney after brachytherapy was 18.1, 44.1, and 22.2, respectively, and was increased compared with that before brachytherapy (15.8, 42.9, and 21.4, respectively), and this difference was not significant (P = .211, .715, .619, respectively). Moreover, the mean GTV was greater than that before brachytherapy and did not achieve a significant difference (P = .099).
Preoperative and Postoperative Dosimetry Parameters for 16 Patients (21 Lesions).
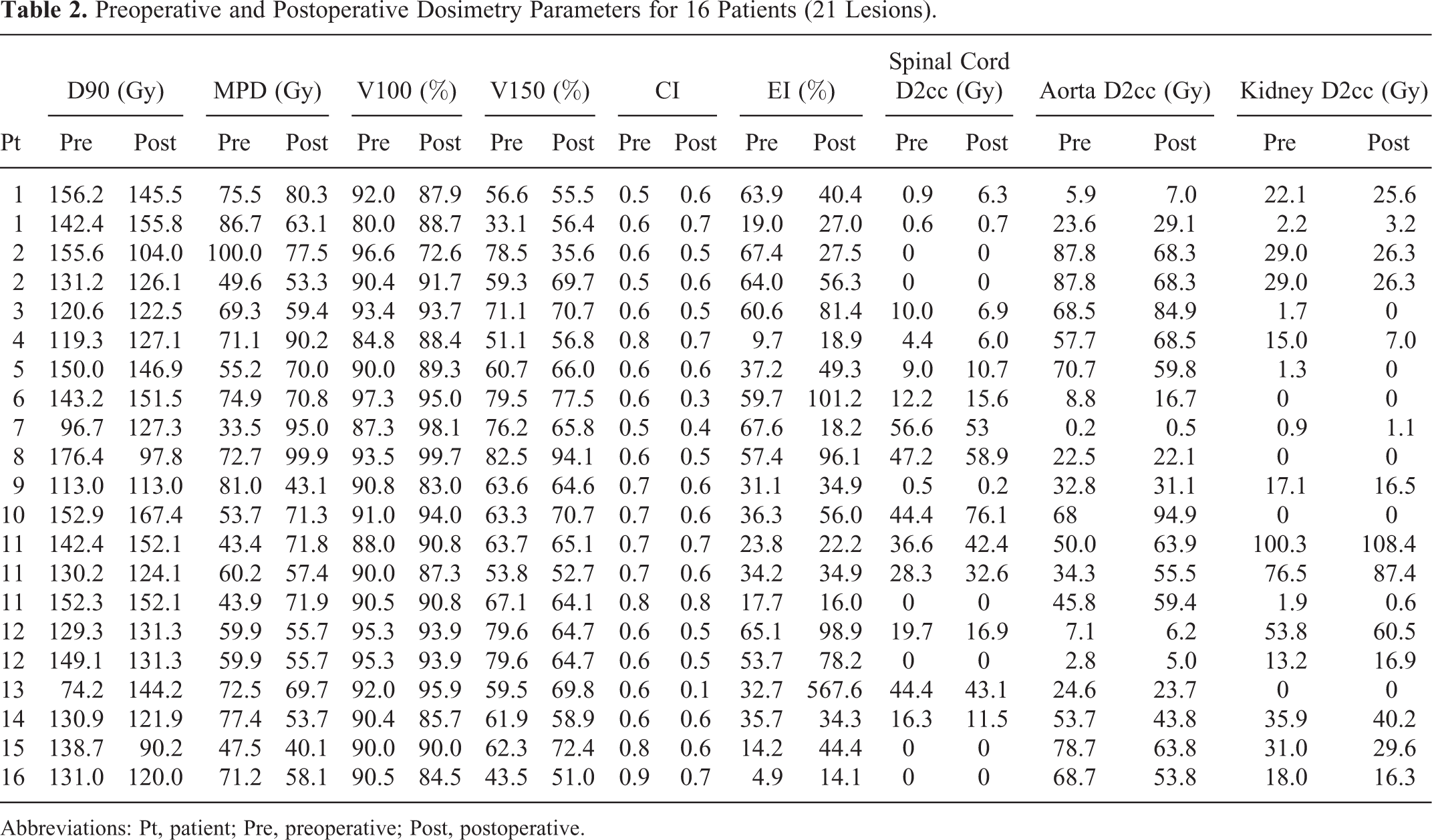
Abbreviations: Pt, patient; Pre, preoperative; Post, postoperative.
Comparison of Preoperative and Postoperative Dosimetry Parameters (21 Cases).

Abbreviations: M, mean; SD, standard deviation.
Discussion
The dose distribution of radioactive seeds is determined by their activity and spatial distribution. To a large extent, the spatial distribution of seeds is determined by the spatial distribution (distance, depth, and angle) of the implantation needle. 6 Implantation based purely on image guidance suffers from 3 main defects. First, RSI is highly operator dependent. Second, the implantation depth and angle of the puncturing needle can be affected by the infiltration and irregular growth of the tumor, risk of organ puncture, and physical blockade by bones. Third, accurate control of the implantation needle is difficult. Also, the angle and depth of the needle must be adjusted under CT guidance during the procedure, which increases the possibility of complications. In view of such limitations, accurate design of a BTPS for brachytherapy is extremely important.
Application of a planar guidance template combined with transrectal ultrasonography has become the standard for RSI in the treatment of prostate cancer and can facilitate intraoperative planning. 19 Unlike a regular planar template, a 3DPNCT includes information on the path of the implantation needle, characteristics of the surface of the therapy area of the patient, and positioning and orientation effects. In this way, the 3DPNCT fully reflects the individual characteristics and realizes accurate alignment between the 3DPNCT and therapy area as well as accurate control of the implantation needle. Zhang et al were the first to report (in 2012) RSI for tumors of the head and neck using a 3DPNCT. 7 However, the needle path was arranged and designed only in the preoperative plan, detailed information of the dose distribution was not available, and CT guidance was not applied in tandem with implantation. They concluded that the postoperative dose could achieve the dose requirement (D90 of the target volume was higher than the prescribed dose), but conformity with the preoperative plan was not clear.
The condition of preoperative dosimetry and condition of postoperative dosimetry of implantation of 125I seeds under guidance of a 3DPNCT was studied and compared by Chinese scholars. 20 Four of the postoperative dosimetry indices (D90, V90, V100, and V150) showed no significant difference compared with those before brachytherapy, which suggested that the requirements of the preoperative plan could be met. 20 However, the studied sample size was too small (8 cases) and the treatment sites were diversified: the head and neck, chest, abdomen, and pelvis. The present study subdivided the analysis and further clarified the accuracy of 3DPNCT technology while reporting the uniformity of the dose of the target volume and normal tissue when the 3DPNCT was applied on therapy of paravertebral/retroperitoneal tumors. The analysis was performed together because the anatomic positions of the paravertebral lesion and retroperitoneal lesion were close to each other, and the body position of the patient was similar to the surrounding organs at risk.
In the present study, D90 and V100 in the postoperative verification were smaller than those before brachytherapy, whereas MPD and V150 after brachytherapy were increased compared with those before brachytherapy. These findings suggest that the prescribed dose received by the target volume after brachytherapy was smaller than that in the preoperative plan and that the high-dose range in the target volume was greater than that before brachytherapy. However, the 2 groups of parameters were not significantly different (P > .05). After further comparison, the preoperative EI and postoperative EI were not significantly different (62.3% and 40.8%, respectively). This observation suggests that the range of the high dose was centralized in the target volume though the high-dose range after brachytherapy was increased, whereas the range of the high dose outside the target region was not significant. Some scholars have suggested that the high-dose range in the target volume could be more useful for tumor control for RSI if there is no organ at risk within the target volume. 21 The postoperative CI was smaller than that before brachytherapy (0.56 and 0.64, respectively) and the difference was significant (P = .005), which indicated that the conformity of the actual dose in the target volume after brachytherapy was poorer than that before brachytherapy. These errors could have occurred because (i) an operating error during puncturing led to deviation of the implantation needle, (ii) the position of the implantation needle was changed (direction or depth) due to movement/squeezing of the organ, and (iii) an operating error might have been generated during RSI (eg, the actual withdrawing distance and spatial distribution of 125I seeds were not in line with those in the preoperative plan, which also explain why the number of preoperative seeds was different from the number of postoperative seeds). Also, the conformity of the target volume might have affected the dose distribution. The GTV after brachytherapy was increased (62.8 vs 61.1 cm3) compared with that before brachytherapy. This increase might have been related to hemorrhage, edema, or delineation error, but was not significant (P = .099).
For most normal tissues, the relationship among the dose, volume, and toxicity in brachytherapy based on RSI is not clear, and appropriate parameters are not available for such an evaluation. The D2cc was selected as the EI using RSI for prostate cancer as the reference 22 only with regard to dosimetry. The doses received by the spinal cord, abdominal aorta, and the kidney after brachytherapy were increased slightly compared with those before brachytherapy, and this slight increase was not statistically significant. In RSI, even a slight change in the source distance can lead to a significant change in the dose distribution according to the inverse-square law and exponential damping. Hence, we believe that this deviation can be controlled within a small range under CT guidance using a 3DPNCT.
Our study had 3 main limitations. First, the running time of this new technology was short, and the number of samples was small. Second, the study was limited to a comparison of dosimetry; differences in the puncturing needles and distribution of 125I seeds before and after brachytherapy were not analyzed. Finally, a lack of clinical data (ie, whether the improvement in therapeutic accuracy could promote a therapeutic effect) were lacking. We are planning another study with a larger study cohort to enable more detailed research.
Conclusions
The CT-guided RSI using a 3DPNCT can enable exact positioning and orientation for paravertebral/retroperitoneal lesions. Most of the dosimetry parameters of the actual target volume and organ at risk were close to those anticipated before brachytherapy. The conformity between the preoperative plan and postoperative plan was satisfactory.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.