
Abstract
Purpose:
This study aimed to investigate the outcomes of permanent Iodine-125 (125I) radiotherapy for patients with unresectable retroperitoneal malignant tumor.
Methods:
Twenty-six patients with retroperitoneal malignant tumors were implanted with 125I seeds under ultrasound guidance from June 2012 to June 2015. The patients were then followed up for 3 to 36 months after the implantation. During the follow-up, pain relief, control of tumor growth, over survival rate, and complications were evaluated.
Results:
Most of the patients (90%, 24/26) suffered from mild to severe pain before 125I seed treatment. After 1-month treatment, 16 patients had 100% pain relief, 4 patients had at least 50% pain relief, and 4 patients had no response, showing 83.3% of pain relief response. Results of computed tomography scan after 2-month 125I treatment indicated that 3 patients had complete remission in the tumor size, 20 patients had partial remission in tumor size, 2 patients were stable, and 1 patient had progressive disease, accounting for 88.4% response in tumor size remission. The median survival of the 26 patients was 11 months. The 1-year and 2-year overall survival rates were 46% and 27%, respectively. The median survival of the 5 patients with pancreatic cancer was 9.4 months. None of the patients had any severe complications.
Conclusions:
125I implantation could effectively relieve the pain in the patients with advanced primary or metastatic retroperitoneal malignant tumors and suppress local tumor progress.
Introduction
Retroperitoneal tumors include primary and metastatic tumors. Primary retroperitoneal tumor includes liposarcoma, fibrosarcoma, neurofibrosarcoma, and malignant lymphoma, which are malignant in most of types. Most of the metastatic retroperitoneal tumors are in advanced stage and highly malignant and contain primary lesions such as gastric cancer, colorectal cancer, liver cancer, gynecological tumor, urinary and nervous system tumor. Tumors that are large, deep-seated lesions are difficult to resect surgically. The patients with metastatic retroperitoneal tumors often have already received surgical treatment followed by chemotherapy and/or radiotherapy for the primary lesions. Thus, these patients with metastatic tumors, who are generally in very poor health situation, are unwilling to receive or could not receive the surgical treatment again. 1 In addition, severe pain is the apparent symptom in patients with advanced cancer. Relieving severe pain is also a treatment principle to improve quality of life for patients with the advanced cancer.
Radioactive particle implantation is a nonvascular intervention radiotherapy embedded inside the tumor. Because the radial distance is short, the radioactive dose to the target tissue is controllable, and the radiation injury to normal tissue is reduced. In this regard, implanted radioactive particles sustain to produce the radiation effect inside of the tumor tissue. Thus, implanted radioactive particles can very efficiently kill the cancer cells. Iodine-125 (125I) is a radioisotope of iodine with a half-life of 59.43 days and lower energy, and 125I seed implantation has been successfully used in radiation therapy as brachytherapy to treat a number of types of tumors, including prostate cancer, uveal melanomas, brain tumors, rectal carcinoma, 2 advanced pancreatic cancer, 3 and non-small cell lung cancer. 4,5 However, application of 125I seed implantation in the treatment of retroperitoneal malignant tumors has not been widely investigated. In this study, we investigated effect of the permanent 125I seed implantation guided under ultrasound in patients with unresectable retroperitoneal malignant tumors.
Patients and Methods
Patients
This study was approved by the ethical committee of the China-Japan Union Hospital at Jilin University (Changchun, China). Tumor registry abstracts and medical records were reviewed to identify those patients who were treated with 125I seed permanent interstitial brachytherapy from April 2012 to June 2015 and followed up for at least 3 years. Total of 26 patients (8 males, 18 females; median age: 51.7, ranging from 29 to 82 years), who had been treated with ultrasound-guided percutaneous radioactive 125I seed implantation, were selected. All patients were confirmed diagnosis with tumor markers, ultrasound examination, computed tomography (CT) scan, pathology biopsy, or postoperation pathological examination, and they were not eligible for radical surgical excision of the tumors. Data on demographics, TNM stage, primary therapy, sites of recurrence, and outcomes in terms of survival and complications were collected.
Inclusion criteria were: (1) patients with primary or metastatic retroperitoneal tumors, which were not surgically removable; (2) patients could not tolerate surgery, or surgery could not achieve R0 resection; (3) patients could not accept or tolerate external radiotherapy; (4) after the surgical resection, chemotherapy, or external radiotherapy, tumors were in recurrence and metastasis; and (5) tumor malignancy was confirmed by either surgical resection or pathological biopsy.
Exclusion criteria were: (1) patients with wide metastasis, (2) patients were in a poor condition of general health and could not tolerate anesthesia and puncture, (3) patients were in childbearing age or patients planned to have pregnancy, and (4) children and pregnant women.
Preparation Before 125I Seed Implantation
Radioactive particles were purchased from Shanghai Xinke Medicine Co, Ltd (Shanghai, China). Iodine-125 seed source was a sealed source for radionuclide. The parameters of an 125I seed were as follows: activity 0.6∼0.8 mCi; volume 4.5 mm × Φ 0.8 mm (cylinder); energy 27.4 ∼ 31.5 keV gamma source; half-life 59.6 days; tissue penetration 1.7 cm; half value layer 0.025 mm lead; source radiation activity 14.8∼29.6 MBq; and the seed surface was covered with titanium alloy.
All radioactive particles were implanted into the tumors under the ultrasound guidance. Treatment plan was carefully determined before the procedure as follows: preplanned radioactive dose and postoperative dose verification were conducted with the software of 3D particles embedded within the radiation produced by Beijing Feitianzhaoye Sci-Tech Co Ltd (Beijing, China). Specifically, tumor images were imported into the software and analyzed by the system, which guided physicians to avoid blood vessels and to locate the implantation site during the procedure.
Laboratory examinations of routine blood tests, liver and kidney function, blood glucose, and coagulation function were performed for each patient. Oral anti-inflammatory drugs were given to the patients 2 to 3 days prior to the procedure. Laxative administration 1 day before treatment accompanied by 12-hour food fasting and 4-hour water fasting before the operation was performed in order to prevent gastrointestinal infection and to avoid bowel injury during implantation. Gastrointestinal decompression was performed before operation to decrease the gas in stomach, which may affect the ultrasound image, and to prevent acute gastric dilatation after operation.
Intraoperative Considerations
Ultrasound-guided percutaneous radioactive 125I seed implantation was performed as described below. Firstly, combined with preoperative CT image, ultrasound was conducted to determine the border, size, and location of tumor and its connections with surrounding tissues in order to precisely choose the puncture path. Secondly, radioactive 125I seeds were implanted under color Doppler ultrasound guidance, which showed the entire blood vessels on puncture path, and therefore, we could adjust needles to avoid severe bleeding during the operation. For those with blood vessel-rich tumors, or tumors nearby vascular vessels, color Doppler could also indicate the borderline of blood vessel and tumor border so that positioning and implantation could be precisely carried out. After implantation, radio-dose was immediately verified in each patient, and it was reimplanted if necessary.
Postoperative Therapy
Food fasting and water fasting were continued after operation until flatus and defecation. Total parenteral nutrition and acid-inhibitory drugs were also used. Hemostatic drugs were routinely used to prevent topical bleeding in area of the needle insertion. Octreotide was used for at least 3 days after surgery in patients with pancreatic cancer to prevent pancreatic fistula. Appropriate activities were encouraged for the recovery of gastrointestinal motility. Routine blood test was performed 1 day after operation and antibiotics were used if the patients had sign of infection. Radiation protection was used in all clinical and nursing procedures.
Evaluation of Efficacy
According to the degree of pain, patients were grouped as mild pain, moderate pain, and severe pain groups. Mild pain was defined as no pain without movement, but slight pain when patients turn over, cough, or take a deep breath. Moderate pain was defined as impalpable pain without movement that influenced sleep. Severe pain was defined as unbearable pain that affected sleep.
The pain was evaluated as mentioned above and relief of the pain before and after operation was compared. Outcomes of the pain relief were as following: (1) 100% relief: absolutely no pain; (2) at least 50% relief: sleep was not affected by the pain and basic quality of life was ensured; (3) no response: the pain was not relieved at all. Pain relief of 50% or more was counted as effective pain relief.
Tumor treatment response was determined following the World Health Organization criteria 6 : Complete remission (CR) was defined as the complete disappearance of the lesion, which lasted for more than 4 weeks. Partial remission (PR) was defined as a reduction in the tumor size for more than 50% and remained unchanged for 4 weeks. Stable disease (SD) was defined as a reduction in tumor size less than 50% or an increase in the size less than 25%. Progressive disease (PD) was defined as an increase in the tumor size of at least 25%. The sum of CR + PR was used to calculate the overall response rate.
Follow-Up
After 1 month of the implantation, patients were revisited to determine whether reimplantation was required based on the evaluation on symptom relief as well as tumor size alteration. Follow-up was carried out by performing physical examination, complete blood panel, chest X-ray, abdominal CT scan, and ultrasound examination at first, second, and third month after surgery. Afterward, CT scan was carried out every 2 months. The overall survival was calculated.
Results
General Information
A total of 26 patients with primary or metastatic retroperitoneal tumors were included in this study. Among them, 2 patients suffered from primary retroperitoneal tumors, 1 patient was with retroperitoneal recurrence of adrenal carcinoma, 5 patients suffered from pancreatic cancer, 3 patients were with retroperitoneal metastasis of cervical cancer, 5 patients were in postoperative recurrence of renal cancer, 2 patients were suffered from ovarian cancer with retroperitoneal metastasis, 2 patients were in postoperative recurrence of ureteral carcinoma, 1 was with a retroperitoneal metastasis of gastrointestinal stromal tumor, 1 was with a retroperitoneal metastasis of brain glioma, 1 was in postoperative recurrence of rectal carcinoid, 1 was with retroperitoneal metastasis of bladder neoplasms, 1 was in recurrence after excision of malignant angioendothelioma, and 1 patient was with rectal melanoma.
The general information on the demography, tumor type, TNM stage, and 125I seed numbers implanted into the 26 patients is summarized in Table 1. All 26 patients received successful implantation procedure under ultrasound guidance as shown in representative Figures 1 to -4.
Patients’ Clinical Characteristic.


A 46-year-old female patient with retroperitoneal recurrence adrenal carcinoma was given 86 pieces of 125I seeds implanted once. During the operation, the bowels nearby the tumor were pushed to the sides with ultrasonic probe so that the puncture needle passed through the tissue without bowel damage by piercing.

Representative ultrasound images from a 59-year-old male patient with pancreatic cancer of TNM III. Stomach was pushed away from the pancreatic tumor as far as possible by pressing down the ultrasound probe in order to shorten the distance between the peritoneum and the tumor and to reduce the chance of stomach damage caused by multiple punctures and needle shifting. Left: An image indicating 2 retroperitoneal lesions. Right: The ultrasound image indicating the puncture path, which passed through the 2 lesions at 1 puncture.

Ultrasound image of a patient with pancreatic cancer (female, 66 years old, TNM stage III). The patient was successfully implanted 125I seed without hemorrhage under accurate ultrasonic guidance. Left: An ultrasound image indicating the tumor was surrounded by the large number of vessels, where puncture path for 125I seed implantation was hardly found. Right: The ultrasound image indicating the successful puncture without injury of the vessels under ultrasound guidance.

A 70-year-old male patient with ureteral carcinoma at TNM stage IV. The patient was treated with ultrasound-guided percutaneous 125I seed implantation. Hemorrhage was successfully avoided during the procedure under accurate ultrasonic guidance. Left: Tumor near the mesenteric blood vessels. Right: The ultrasound image indicating the distal end of the needle reached to the mesenteric blood vessels.
Pain Relief
The 26 patients had middle to late TNM stage tumors and varying degrees of pain caused by different types of cancer. In addition, sensitivity to the pain was also different in the patients. Before 125I seed implantation, 2 patients had no pain, 6 patients had mild pain, 10 patients had moderate pain, and 8 patients had severe pain. After 1 month of the implantation, 16 patients had 100% pain relief, 4 patients had at least 50% pain relief, and the rest 4 patients had no response to the treatment. Percentage of pain relief after 1 month of 125I seeds implantation was 83.3% (22/26; Table 2). Of the 8 patients with severe pain, 4 had complete relief and 2 had at least 50% pain relief.
Pain Relief After 1 Month’s 125I Seed Implantation Treatment.
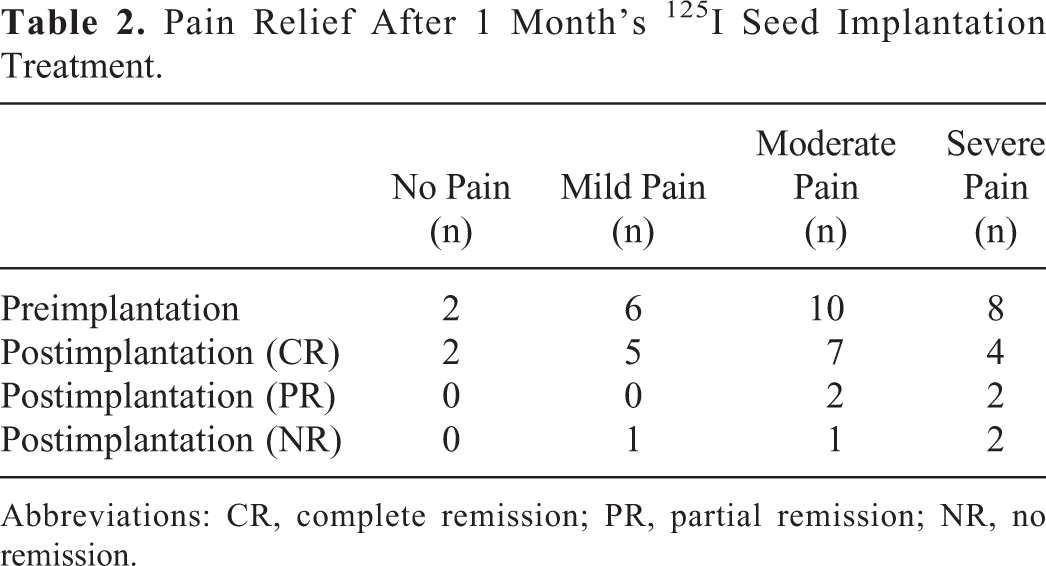
Abbreviations: CR, complete remission; PR, partial remission; NR, no remission.
Tumor Control
After 2 months of 125I seed implantation, outcomes of CT examination showed that 3 patients had complete disappearance of the tumor lesion (CR), 20 patients had PR, 2 patients had SD, and 1 patient had PD. The percentage of tumor control in 26 patients (CR + PR) was 88.4% (Figures 5 and 6). In addition, a patient with rectal cancer (female, 68 years old, TNM stage IV) suffered from right leg swelling, which was remarkably alleviated within 1 week of the treatment.

Representative images showing curative effect of 125I seeds implantation in a patient (female, 46 years old, TNM stage IV) with retroperitoneal recurrence of adrenal carcinoma. Left: An image indicating the left retroperitoneal tumor before the 125I seeds implantation. Right: An image indicating the left-over of 125I seeds at the location of previous tumor after the 125I seeds implantation.

A representative image showing a patient (female, 68 years old, TNM stage IV) with postoperative recurrence of rectal cancer. Partial remission of the tumor after 125I seed implantation was noticed. Left: Before 125I seed implantation. Tumor was located at the right side of the iliopsoas and iliac blood vessels. Right: After 1 month of 125I seed implantation, the implanted particles were ideally distributed and trend of the tumor growing was significantly contained.
Overall Survival
All of the 26 patients were followed up for 3 to 36 months, and none of them was lost during the follow-up. The median survival time of the 26 patients was 11 months. Up to September 2015, 6 out of the 26 patients had survived for the whole 36-month follow-up. The 1-year and 2-year overall survival rates were 46% and 27%, respectively (Figure 7).

Overall survival curve after implantation.
Mean Survival of Pancreatic Cancer
Of the 26 patients, 5 patients were III to IV stage pancreatic cancer and had no opportunity for surgical resection. After the 125I seed implantation, these 5 patients had been followed up for 3 to 36 months. As shown in Figure 8, 1 of the 5 patients, who was alive till the end of the follow-up (36 months), had CR in tumor size. The mean survival after 125I seed implantation in these 5 patients with pancreatic cancer was 9.4 months, which was longer than the average time of 3 to 6 months reported in the literature. 7

Representative images showing curative effect of 125I seeds implantation in a patient with pancreatic cancer (male, 61 years old, TNM stage III). Left: An image showing tumor size before the 125I seed implantation. Right: An image showing dramatic containment of the tumor after the 125I seed implantation.
Complications
None of the patients had any severe complications such as bleeding, intestinal obstruction or fistula, and abdominal infection. Long-term complications such as radiation enteritis and particle-migration were not found during the follow-up period.
Discussion
Radioactive 125I seed implantation has been used to treat malignant tumors and achieved significant clinical effect. 8 -10 This brachytherapy has been shown to be effective in controlling local progress of malignant carcinoma for those patients who have no opportunity for surgical treatment. In the current study, a total of 26 patients with nonresectable retroperitoneal malignant tumors were treated with radioactive 125I seed implantation under the guidance of ultrasonic examination. After 1-month treatment, 22 (83.3%) out of the 26 patients had significant pain relief. After 2-month treatment, 23 (88.4%) out of the 26 patients had at least PR in tumor size. The median survival time of the 26 patients was 11 months, and the 1-year and 2-year overall survival rates were 46% and 27%, respectively.
Radioactive 125I seed implantation has been used to treat variety kinds of malignant tumors including prostate cancer, lung cancer, pancreatic cancer, liver cancer, and metastatic retroperitoneal lymph node cancer. 3,11 -13 The 125I radioactive seed implantation includes visible implantation during laparotomy or open operation, and CT or ultrasound-guided percutaneous radioactive 125I seed implantation. 14,15 Compared to visible seed implantation, percutaneous seed implantation has many advantages: lower operation risk, lesser blood loss, shorter operative time, rapid postoperative recovery, and no abdominal scar. In this study, all patients received percutaneous seed implantation under ultrasound guidance. We believe the cost of the percutaneous seed implantation is similar to that of conventional radiotherapy. However, once it is implanted into the tumor tissue, the effect of radiation lasts longer inside the tumor tissue without injuring normal tissue adjacent to the tumor. Thus, it is more cost-effective and easily accepted by more and more patients.
Most of retroperitoneal malignant tumors were located lower abdominal area, surrounded with gastrointestine and vessel, apt to be influenced by peristalsis enterocinesia and gas inside the loops; CT-guided implantation would help the operators clearly identify the tumor location and avoid the influence of intraperitoneal air, 16 but it is not real-time scan. Therefore, it may damage gastrointestine during implantation and increase the risk of severe complication such as abdominal infection, intraperitoneal hemorrhage, intestinal fistula, and life-threatening risk. In addition, patients inevitably received unnecessary radiation during implantation. 17 In contrast, under ultrasound guidance, the operator can view tumors in real time, keep away from intestine, produce no radiation damage to the tissue, and easier to operate. In the current study, therefore, we chose ultrasound-guided percutaneous radioactive 125I seed implantation. Our experiences for the successful implantation of the radioactive 125I in the patients with retroperitoneal cancers suggested that, firstly, operation had to be carefully planned before the procedure in order to determine perfect puncture pathway; secondly, identification of the tumor board line and its relationship with surrounding organs before implantation was crucial to reduce operational risk and organ injury; thirdly, ultrasound guidance was necessary to ensure accurate percutaneous puncture.
The mechanism of 125I radioactive particle function is different from that of external radiation therapy. Therefore, the radioactive dose for implanted 125I seed was not calculated as the same way as external radiation dose in this study. However, there is no gold standard of radioparticle therapy by national or international standard. Because most of the patients in our study were in advanced stage and were with recurrent or metastatic tumors, referring the domestic and international treatment experiences, we decided that the prescription dose D90 was 110 to 140 Gy, ensured the dose of target area >matched peripheral dose, and we decided that planning target volume was larger than clinical target volume by 1.0 cm. We also sketched the locations of nerves, blood vessels, and organs around tumors to ensure the patient’s safety.
Our results showed the rates of pain relief and tumor control were 84.6% and 88.4%, respectively, which apparently improved the quality of life for the patients. Retroperitoneal tumors often grow fast and reach large size, which often press surrounding tissues and nerves, and thus, leading to an apparent pain. When the tumor shrinks, pressure to the surrounding tissues will be relieved, and thus, it is understandable that pain relief is closely associated with the tumor control. In this study, the 1-year and 2-year overall survival rates were 46% and 27%, respectively. Moreover, median survival of the 5 patients with pancreatic cancer was 9.4 months, and one of them survived over 36 months. Similarly, Doi and colleagues reported that the longest median survival time for the patients with resectable pancreatic cancer was 27.2 months. 18 In the localized and smaller pancreatic adenocarcinoma (<2 cm, stage T1) without lymph node metastasis, complete surgical resection was associated with an actuarial 5-year survival rate of 18% to 24%. 19 However, the patients with pancreatic cancer enrolled into the current study were in stage III to IV with lymph node metastases and were nonresectable. For patients with such an advanced pancreatic cancer, achievement of the 9.4-month median survival, significant containment of the cancer-related pain, and 46% or 27% of 1-year or 2-year survival rates suggested that radioactive 125I seed implantation be an effective palliative treatment for the advanced retroperitoneal malignant tumors.
In the current study, no severe complications were found after the operation or during the follow-up period, suggesting this treatment is highly safe and can be considered as an alternative treatment for retroperitoneal malignant tumors. However, there are limitations in this study. First, limited number of cases were enrolled into this study. Second, tumor size and pathological types of the tumor cells may affect the outcomes of 125I seed implantation therapy. Due to limited case number, association of tumor size or cancer cell type and the outcomes of the implantation therapy was not analyzed. Third, due to limited number of study cases, correlation between tumor remission and pretreatment pain levels was not analyzed. These limitations remain to be further determined in the future studies with accumulation of the cases.
In conclusion, ultrasound-guided percutaneous radioactive 125I seed implantation can effectively relieve pain and control development of retroperitoneal malignant tumors. It is also an alternative choice to treat nonresectable retroperitoneal malignant tumors.
Footnotes
Authors’ Note
This study was approved by ethics committee (approval No. 2018122504) of China-Japan Union Hospital of Jilin University. All patients provided written informed consent prior to enrollment in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.