
Abstract
The treatment methods available for large primary hepatocellular carcinomas (diameter >5 cm) are inadequate. Here, we report the successful management of 80 cases of large hepatocellular carcinoma, using a combination of custom-designed permanent interstitial iodine-125 seed brachytherapy and palliative surgery. Patients were enrolled in the study between 2011 and 2014. All patients underwent surgical treatment along with permanent interstitial iodine-125 seed brachytherapy; for the latter, patients received minimum doses covering 90% of the target (D90 s) of iodine-125 seeds ranging from 100 to 160 Gy (median: 110 Gy). All patients received 6 cycles of chemotherapy and were followed up at 6, 12, 24, and 36 months postoperatively. The clinical symptom remission rate was 95.3% (61 of 64). Alanine aminotransferase and aspartate aminotransferase levels decreased to normal in 80% (50 of 60) and 75% of the patients (45 of 60), respectively. The posttreatment alpha-fetoprotein levels decreased by 50% in 80% of the patients (40 of 50). The effective therapy rates were 80% (76 of 95) for 95 tumor nodules (diameters 5-10 cm) and 78.6% (33 of 42) for 42 tumor nodules (diameters >10 cm). The 3-year disease-free survival rate was 66.6%. Palliative surgery plus permanent interstitial iodine-125 seed brachytherapy appears to be a reasonable therapeutic alternative for large hepatocellular carcinoma.
Introduction
Hepatocellular carcinoma is the fifth most common cancer worldwide and the third leading cause of cancer-related death, but the prevalence varies according to endemic risk factors. 1 –3 Surgical treatment is currently not recommended for large hepatocellular cancers (diameters >5 cm), which are considered advanced-stage diseases. Despite therapeutic advances in surgical resection, radiotherapy, and chemotherapy, the overall survival of patients with large hepatocellular cancers has not improved in the last 2 decades. 4 Currently, hepatic resection is the primary treatment option for the few patients with hepatocellular carcinomas arising in normal livers with well-preserved hepatic function and for patients with single tumors. 5 However, the median survival duration of most patients with large hepatocellular cancer is approximately 6 months. 6 Therefore, more effective treatments are needed.
Recently, novel treatments, including permanent interstitial iodine-125 (125I)-seed brachytherapy, interventional therapy, and radiofrequency ablation, have been applied in clinical settings. 7 –9 Permanent interstitial 125I-seed brachytherapy, which has been used widely for clinical cancer treatment worldwide, plays an important role in prostate cancer treatment with curative intent. 8 –11 Compared with conventional radiotherapy, 125I seeds can kill many more cancer cells during the propagation phase by continuously emitting low-dose X- and γ-radiation. Additionally, the low energy and short tissue penetration of the radiation waves will not damage surrounding normal tissues. 10 –12 However, very few studies have examined the applications and effectiveness of 125I-seed brachytherapy for large hepatocellular carcinomas.
To investigate the curative effects of permanent interstitial 125I-seeds brachytherapy combined with palliative surgery for large hepatocellular carcinoma, we studied 80 patients treated at our hospital between 2009 and 2012. Our results indicated that this treatment combination could relieve clinical symptoms and significantly increase therapeutic effectiveness.
Patients and Methods
Patient Information and Selection
Our study was approved by the review board of The Second People’s Hospital of Yunnan Province. Eighty patients with large hepatocellular carcinoma were diagnosed using computed tomography (CT), echography, and biopsy between 2011 and 2014. These patients comprised 51 men and 29 women with a mean age of 52.5 years (range: 28-68 years). Forty patients had a single tumor, 28 had 2 tumor nodules, and 12 had ≥3 tumor nodules. The diameters of 38 nodules ranged from 5 to 10 cm, whereas the diameters of the remaining 42 nodules exceeded 10 cm. Fifty-four and 71 patients had underlying hepatitis B infections and liver cirrhosis, respectively. Sixty-six patients had portal hypertension. Fourteen and 66 patients had Child A- and Child B-stage liver function, respectively.
Based on the Barcelona clinic liver cancer criteria and the neoplasm size or patient’s symptoms, 55 patients were treated via enucleation, 18 via left liver resection, and 7 via hepatic segmentectomy after definitive diagnosis.
All 80 patients were treated using a combination of surgery and 125I-seed implant brachytherapy.
Chemotherapy
At 2 to 4 weeks postoperatively, all patients received a single administration of 130 to 150 mg/m2/d of oxaliplatin in 500 mL of 5% glucose liquor via 3- to 6-hour continuous infusion, followed by an intravenous administration of 20 to 100 mg/m2/d of leucovorin in 250 mL of 5% glucose liquor via 2-hour continuous infusion and 370 to 400 mg/m2/d of 5-Fu in 250 mL of 5% glucose liquor via 2-hour continuous infusion on the same day. The leucovorin and 5-Fu regimen were administered daily on the following 4 days. The entire oxaliplatin, leucovorin, and 5-Fu regimen were administered once every month for 6 months. In other words, each patient received a total of 6 cycles of the triple-drug regimen.
Radiation Source
For permanent implants, 125I is commonly used as the radiation source. 13 Iodine−125 has a half-life of 60.1 days and energies of 27.4 to 31.5 Kev for X-rays and 35.5 Kev for γ-rays. In this study, 125I was purchased from American Company.
Surgery and 125I Seed Implantation
Patients’ tumor volumes were determined from CT scans obtained 1 week before seed implantation. The hepatic tumor images were obtained at 5-mm intervals. Under a radiologist’s guidance, the surgeon outlined the gross tumor volume (GTV) on each image; using a 3-dimensional treatment plan system (3D-TPS; KL Medical Technical Company, China) before or during surgery; the planning target volume included the GTV plus a 0.5 to 1.0 cm margin of peripheral tissue. The minimum doses covering 90% of the target (D90 s) of 125I seeds ranged from 100 to 160 Gy with a median of 110 Gy, and the number of 125I seeds to be implanted was calculated using the TPS. Sixty to 80 seeds (0.5-0.6 mCi/per seed) were implanted in each patient (Figures 1 and 2).
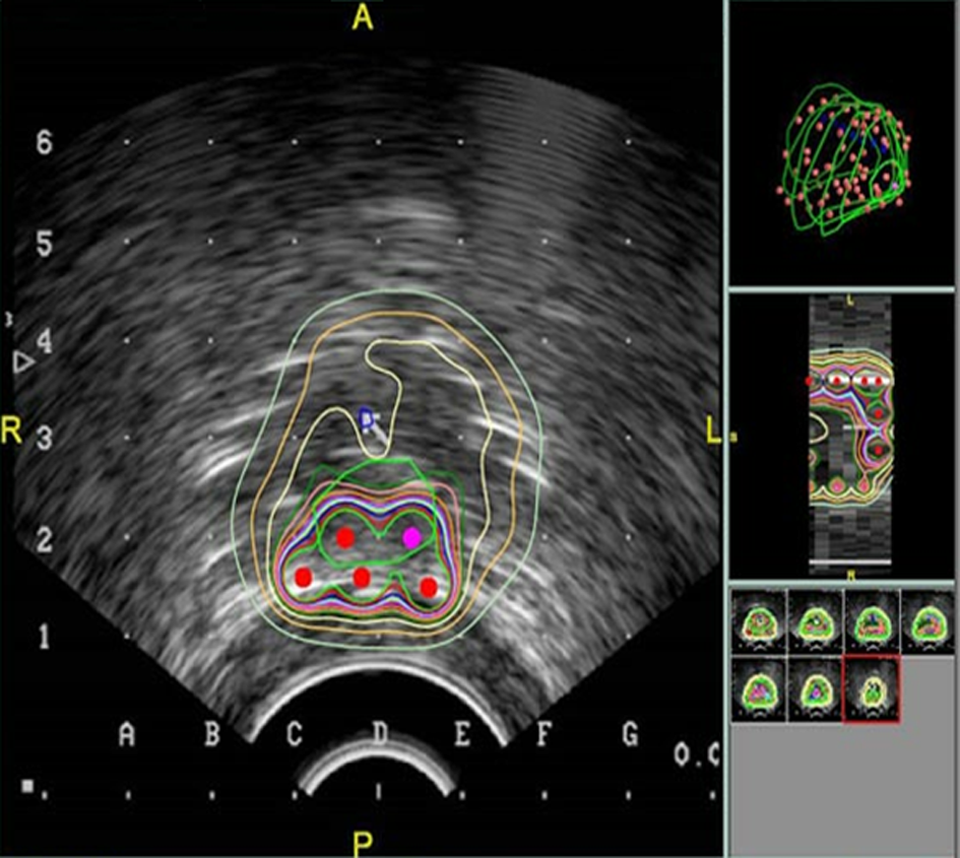
Treatment planning system.

Iodine-125 seeds implantation.
The specific resection strategy depended on the tumor size, location, and relationships to the major afferent and efferent vasculature and bile ducts. We estimated the planned resection margin by palpation and scored the liver capsule with a cautery to outline this margin. In most cases, resection with a 1- to 2-cm margin of normal liver was required. Fifty-five cases were treated via enucleation, 18 via left liver resection, and 7 via hepatic segmentectomy. The intraoperative blood loss volumes ranged between 780 and 1500 mL (mean: 958 mL). Thirty-eight and 22 patients required red blood cell transfusions of 500 and 900 mL, respectively.
Iodine-125 seeds were implanted in the following locations: the sites of the removed tumor, the sites of metastases, the peritoneum and hepatoduodenal ligament, and the mesenteric lymph nodes surrounding the liver, hepatic artery and vein, and celiac aorta. Implantation was achieved under ultrasonic guidance using a sterilized 18-gauge radiation-proof needle. The interstitial distance between seeds was 1 to 1.5 cm. After the needles were placed, the numbers and locations of seeds were monitored quantitatively using a radiometer and X-ray film or a gamma camera to maintain spacing at approximately 1.0 cm.
Radiation Monitoring and Protection
The numbers and locations of implanted seeds were monitored quantitatively using a radiometer and X-ray film or a gamma camera. During implantation, we were careful to verify that the correct number of 125I seeds had transferred without damage to the shells. The surgeons and nurses wore lead–rubber coats and protective goggles during the procedure.
Response Evaluation
To evaluate radiation exposure, we compared the patients’ preoperative and postoperative immunoglobulin (IgA, IgG, and IgM) levels and white blood cell (WBC) counts. We also evaluated hepatic function, clinical symptom remission, alpha-fetoprotein (AFP) levels, local cancer control, and survival rates at follow-up visits conducted 6, 12, 24, and 36 months postoperatively. We assessed tumor responses from CT and/or magnetic resonance imaging findings, using the Response Evaluation Criteria in Solid Tumors. 14 A complete response (CR) was defined as disappearance of all target lesions, maintained for 1 month; a partial response (PR) was defined as a ≥30% decrease in the sum of the longest diameters of target lesions, maintained for 1 month; progressive disease (PD) was defined as a ≥20% increase in the sum of the longest diameters of target lesions or the appearance of ≥1 new lesion; and stable disease (SD) was defined as neither sufficient shrinkage to qualify as a PR nor sufficient increase to qualify as PD. Complete response or partial response was considered as positive responses.
Complications
None of the patients died during the perioperative period. Thirteen (16%) patients experienced extravasation from the abdominal cavity. Two (2%) patients experienced bile leakage, and 17 (21%) developed fever.
Statistics Analysis
Using SPSS 19.0 software (SPSS Inc, Chicago, Illinois), quantitative preoperative and postoperative indicators were compared using a paired t test or nonparametric methods. 15 White blood cell counts and Ig levels were compared statistically, and local recurrence and survival rates were analyzed using the Kaplan-Meier method. A P value <.05 was considered statistically significant.
Results
White Blood Cell Counts and Ig Levels
The preoperative WBC counts for all patients were higher than those at 1 week and 3 months postoperatively, although all counts remained within the normal range. There were no significant differences between preoperative and postoperative Ig levels in the 2 groups (P = .032). No suppression of bone marrow or immunological functions was observed (Table 1).
The WBC and Immunoglobin Levels Between Preoperative and Postoperative Patients.

Abbreviation: Ig, immunoglobin; WBC, white blood cell.
Clinical Effects
Sixty-four of 80 patients developed clinical symptoms. After palliative surgery plus permanent interstitial 125I-seed brachytherapy, 61 patients reported significant remission of clinical symptoms (95.3%, 61 of 64), including those affecting appetite, pain, and body weight. The alanine aminotransferase and aspartate aminotransferase (AST) levels decreased to normal in 80% (50 of 60) and 75% of patients (45 of 60), respectively. Postoperatively, the AFP levels decreased by 50% in 80% of patients (40 of 50). The effective therapy rates were 80% (76 of 95) among 95 tumor nodules with diameters of 5 to 10 cm and 78.6% (33 of 42) among 42 tumor nodules with diameters >10 cm. After therapy, the following responses were recorded for 132 target lesions in 80 patients: CR, 83; PR, 26; SD, 13; and PD, 10. The actuarial overall positive response rate was 82.6% (109 of 132; Table 2). The mean survival duration was 30.940 months (95% confidence interval [CI]: 28.821-33.059; Figure 3). The 1-, 2-, and 3-year actuarial overall survival rates were 91.9%, 90.0%, and 66.6%, respectively (median: 20 months, 95% CI: 16-24, longest survival: 7.5 years; Table 3).
The Actuarial Overall Positive Response Rate in the 125I Therapy.

Abbreviations: CR, complete response; 125I, iodine-125; PD progressive disease; PR, partial response.
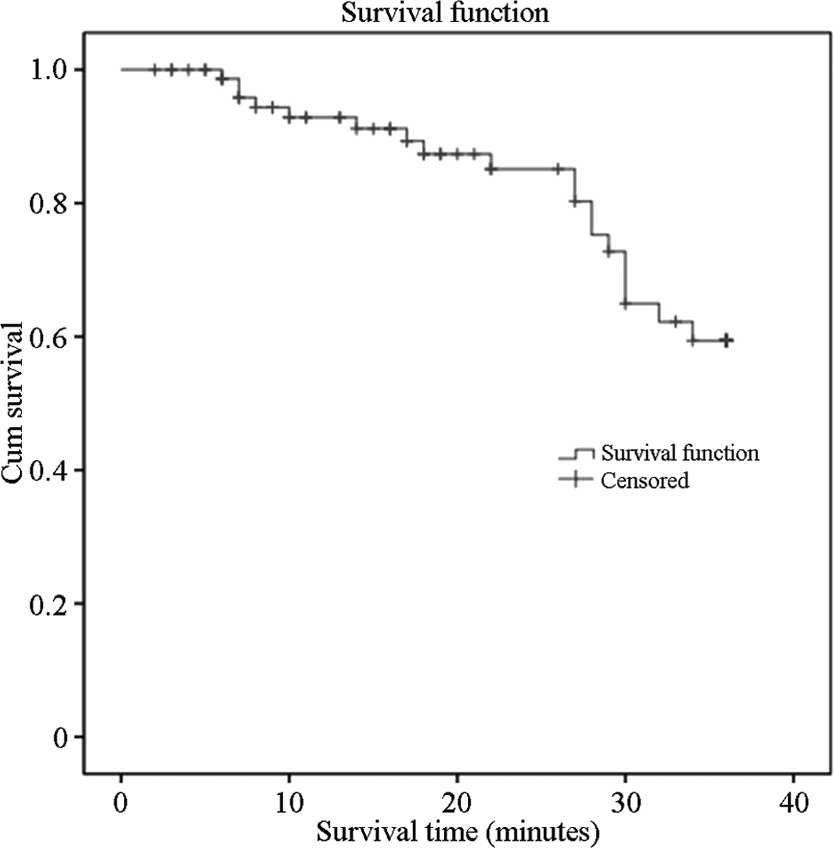
The means for survival time after therapy.
The 1-Year, 2-Year, and 3-Year Actuarial Overall Survival Rates.

Discussion
To date, most hepatocellular cancers have been treated via radical surgery. Despite therapeutic advances, however, the overall survival of patients with large hepatocellular cancer, especially those with indistinct margins, has not improved significantly. 16,17 In this study, we explored the combined use of permanent interstitial 125I-seed brachytherapy and palliative surgery as an alternative treatment for large hepatocellular cancers. We found that this combination yielded satisfactory outcomes with minimal side effects or radiation exposure to patients, family, and health personnel.
The 1-, 2-, and 3- actuarial overall survival rates in this study were 91.9%, 90.0%, and 66.6%, respectively (median: 20 months, 95% CI: 16-24, longest survival: 7.5 years). The actuarial effective rates were 80% (76 of 95) among 95 tumor nodules with diameters of 5 to 10 cm and 78.6% (33 of 42) among 42 tumor nodules with diameters >10 cm. The actuarial overall positive response rate was 82.6% (109 of 132). Alanine aminotransferase and AST levels were reduced to normal in 80% (50 of 60) and 75% (45 of 60) of patients, respectively. The AFP levels decreased by 50% postoperatively in 80% of patients (40 of 50). No suppression of bone marrow and immunological functions was observed.
We attribute the lower recurrence rate and longer survival duration to the long half-lives, low energy levels, and continuous activities of 125I seeds, which allow greatly increased killing of cancer cells during the propagation phase. Cancer cells are extremely radiation-sensitive during the mitotic (M) and the postsynthetic (G2) phase. 18 Continuous irradiation can redistribute the ratio of radiation-sensitive to -insensitive cancer cells. As cancer cells in the M and G2 phases are killed, those in resting phases will continue through the cell cycle and transition to the M and G2 phases. 19 Accordingly, the continuous activity and cumulative effects of radiation from 125I seeds can damage more cancer cells. 20,21 Concurrently, the total radiation doses from 125I seeds that were detected in patients remained within international exposure limits; in other words, 125I-seed brachytherapy is safe for medical workers, patients, and their relatives.
Further investigations are needed to confirm these results, as our study had a relatively small sample size and short follow-up. Despite these limitations, however, the combination of 125I-seed brachytherapy plus palliative surgery may be considered a reasonable alternative to other local treatment options and can relieve clinical symptom while significantly increasing the effectiveness of large hepatocellular cancer treatment.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.