
Abstract
Purpose:
To investigate high conformality on target coverage and the ability on creating strict lung dose limitation of intensity-modulated radiation therapy in malignant pleural mesothelioma.
Patients and Methods:
Twenty-four radiation therapy plannings were evaluated and compared with dosimetric outcomes of conformal radiation therapy and intensity-modulated radiation therapy. Hemithoracal radiation therapy was performed on 12 patients with a fraction of 1.8 Gy to a total dose of 50.4 Gy. All organs at risk were contoured. Radiotherapy plannings were differed according to the technique; conformal radiation therapy was planned with conventionally combined photon–electron fields, and intensity-modulated radiation therapy was planned with 7 to 9 radiation beam angles optimized in inverse planning. Strict dose–volume constraints were applied.
Results:
Intensity-modulated radiation therapy was statistically superior in target coverage and dose homogeneity (intensity-modulated radiation therapy-planning target volume 95 mean 100%; 3-dimensional conformal radiation therapy-planning target volume 95 mean 71.29%, P = .0001; intensity-modulated radiation therapy-planning target volume 105 mean 11.14%; 3-dimensional conformal radiation therapy-planning target volume 105 mean 35.69%, P = .001). The dosimetric results of the remaining lung was below the limitations on intensity-modulated radiation therapy planning data (intensity-modulated radiation therapy-lung mean dose mean 7.5 [range: 5.6%-8.5%]; intensity-modulated radiation therapy-lung V5 mean 55.55% [range: 47%-59.9%]; intensity-modulated radiation therapy-lung V20 mean 4.5% [range: 0.5%-9.5%]; intensity-modulated radiation therapy-lung V13 mean 13.43% [range: 4.2%-22.9%]).
Conclusion:
With a complex and large target volume of malignant pleural mesothelioma, intensity-modulated radiation therapy has the ability to deliver efficient tumoricidal radiation dose within the safe dose limits of the remaining lung tissue.
Keywords
Introduction
Malignant pleural mesothelioma (MPM) is a rare, aggressive tumor, which is increasing worldwide. 1 Radiation therapy (RT) plays an important role in the multimodality management of MPM. Both the symptom-relieving and the prophylactic effects of RT in MPM are well known. 2 Recently, RT has been used within the multimodality treatment of MPM for curative purposes. 3 –5 En bloc resection of the ipsilateral lung, pleura, diaphragm, and pericardium called as extrapleural pneumonectomy, chemotherapy (CT), and local–regional RT (trimodality treatment [TMT]) has shown promising results in operable patients. 6,7
However, hemithoracal RT is rather challenging in dealing with a large and complex target volume, which involves the entire hemithorax with many radiosensitive critical organs. The conventional techniques that were used previously had substantial technical limitations, of which one of the most important was poor targeting of the pleural bed with efficient doses, especially in larger volume and irregular-shaped targets. Moreover, the critical organs lying within the target volume—spinal cord, liver, kidneys, esophagus, heart, and contralateral lung—limited the full course of photon irradiation. Therefore, the photon–electron combination was thought to be the only option for radiating such a volume. 8,9
More recently, a highly conformal method of irradiation, intensity-modulated radiation therapy (IMRT), yielded marked improvements in radiation delivery. Early studies of IMRT showed improved local control according to the highly conformal radiation of the target. 10,11 However, on follow-up, IMRT failed due to the high rates of treatment-related fatal pneumonia. 12
Additional reports indicated that IMRT is not superior to 3-dimensional conformal radiation therapy (3D CRT) when comparing the balance between toxicity and tumor control. Krayenbuehl et al found that lung dose is an important limitation for IMRT. 6 Allen et al reported that the percentage of lung volume receiving 20 Gy and higher doses (V20) is not sufficient for predicting radiation pneumonia in patients with MPM. Strict limitations for the contralateral lung are needed in the radiation planning of MPM. They concluded that the percentage of contralateral lung volume receiving 5 Gy and higher doses (V5) and mean lung dose (MLD) must be defined and included in IMRT dose constraints. 12 This study is aimed to compare the dosimetric results of IMRT and 3D CRT and to show that IMRT provides delivering efficient tumoricidal dose while keeping lung dose below tolerance for pneumonitis.
Patients and Methods
Radiation therapy planning records of 12 patients who underwent TMT with the diagnosis of MPM were reviewed. The study population presented with stage pT1-T4N0-N2 tumor. Because of the dosimetric nature of the study, all the patients were accepted and planned as N0, in order to simplify plan comparisons. The study protocol was approved by the local ethical committee.
Radiation Therapy Planning
The target volumes (pleural bed) and the critical structures were contoured for each patient. The clinical target volume (CTV) was the pleural bed, and 0.5 cm was added to the CTV to develop the planning target volume (PTV) in order to compensate for set up and an internal margin. Both IMRT and 3D CRT plans were created using the Eclipse Treatment Planning System (Varian Medical Systems, Inc, Palo Alto, California) for each patient.
Dose Prescription
Total radiation dose of 50.4 Gy with 1.8 Gy daily fractions to the entire hemithorax was prescribed, in accordance with the excellent results in locoregional control with doses of 45 to 50 Gy as reported previously by Ahamad et al. 13 No additional boost was planned.
Three-Dimensional Conformal Radiation Therapy Planning Technique
The treatment planning for 3D CRT was anterior and posterior (gantry angles were 0° and 180°) photon fields using 18 MV photon energy. The contralateral lung, heart, spinal cord, liver, and contralateral and ipsilateral kidney were all contoured as organs at risk (OAR). When the tolerance doses of OAR came close to the limiting doses, photon fields were blocked anteriorly at each OAR, and electron fields were applied to compensate for the target dose. The electron energy range selected for planning was 12 MeV. When the total dose reached 41.40 Gy, the spinal cord was shielded. Heart, liver, and ipsilateral kidney were also shielded after the total dose reached 19.80 Gy. A multileaf collimator (MLC) was used for shielding. Separate new electron fields were administered to each shielded field. The gantry angle planned for electron fields was the same as for the photon fields (0° and 180°). Dose calculations were done first for each photon and electron field separately and then for the plan total for each patient. Thus, MLC transmission accounted for all electron fields. Three-dimensional CRT plans were created, as described previously by Kutcher et al. 14
Intensity-Modulated Radiation Therapy Planning Technique
For IMRT plans, 7 to 9 radiation beam angles were corrected and optimized in inverse planning for each patient, to enhance conformality and to protect the contralateral lung. The range of gantry angles was 0° to 342° in patients with right-sided disease and 18° to 216° in patients with left-sided disease. Dose–volume constraints were applied as follows—no volume of spinal cord receiving more than 50 Gy, keeping the volume of the heart receiving 45 Gy below 30% and limiting the mean heart dose below 40 Gy and the MLD below 10 Gy. Additionally, the volume of lung receiving 5 Gy was limited to below 60%, and no more than 10% of the lung volume were allowed to receive more than 20 Gy, as specified in the literature. 6,12 The MLD was limited to below 10 Gy, and the mean dose to the liver was below 30 Gy. The maximum mean dose to the contralateral kidney was 6 Gy, and no volume or point of the contralateral kidney was allowed to receive more than 15 Gy. The ipsilateral kidney receiving >15 Gy was kept at <40%. The optimal dose applied to all the PTV was 95% of the total prescribed dose.
Dose–volume histogram parameters were checked for each plan. Three-dimensional CRT and IMRT plans were compared according to these dosimetric data.
The SPSS for Windows version 15 software program was used for statistical analysis. Two independent groups were compared by the Mann-Whitney U statistical test. A P value of <.05 was considered statistically significant.
Results
The dosimetric data of 24 plans for 12 patients were evaluated in this retrospective study. There were 7 (58.3%) male and 5 (41.7%) female patients. The tumor was located on the right hemithorax in 8 (66.7%) patients and on the left in the others.
According to the data collected from the dose volume histograms, IMRT was statistically superior on target coverage. The target volume receiving 95% of the total dose (PTV95) was on average 100% in IMRT planning and 71.29% in 3D CRT planning. The PTV was covered with 47.9 Gy (95% of the total prescribed dose) on IMRT. Additionally, IMRT was superior on dose homogeneity (IMRT-PTV95 mean 100%; 3D CRT-PTV95 mean 71.29%, P = .0001; IMRT-PTV105 mean 12.25%; 3D CRT-PTV105 mean 35.81%, P = .001; Table 1).
Comparison of PTV95 and PTV105 on 3DCRT and IMRT.

Abbreviations: 3D CRT, 3-dimensional conformal radiation therapy; IMRT, intensity-modulated radiation therapy; Max, maximum; Min, minimum; PTV, planning target volume. Statistically significant p values are shown in bold.
There was no statistically significant difference in OAR mean doses for the heart between IMRT and 3D CRT plans. In addition, the spinal cord maximum doses and the percentage of ipsilateral kidney volume receiving 15 Gy (Ipsilateral kidney V15) did not differ between IMRT and 3D CRT (Table 2). Dose volume histograms of a case sample with both IMRT and 3DCRT are shown in Figure 1A–C.
Comparison of OAR doses and percent volumes on 3DCRT and IMRT.

Abbreviations: 3D CRT, 3-dimensional conformal radiation therapy; IMRT, intensity-modulated radiation therapy; Max, maximum; Min, minimum. Statistically significant p values are shown in bold.

A, Dose–volume histogram—OAR parameters by 3D CRT. B, Dose–volume histogram—OAR parameters by IMRT. C, Dose–volume histogram—PTV and lung parameters by 3D CRT and IMRT. 3D CRT indicates 3-dimensional conformal radiation therapy; IMRT, intensity-modulated radiation therapy; OAR, organs at risk; PTV, planning target volume.
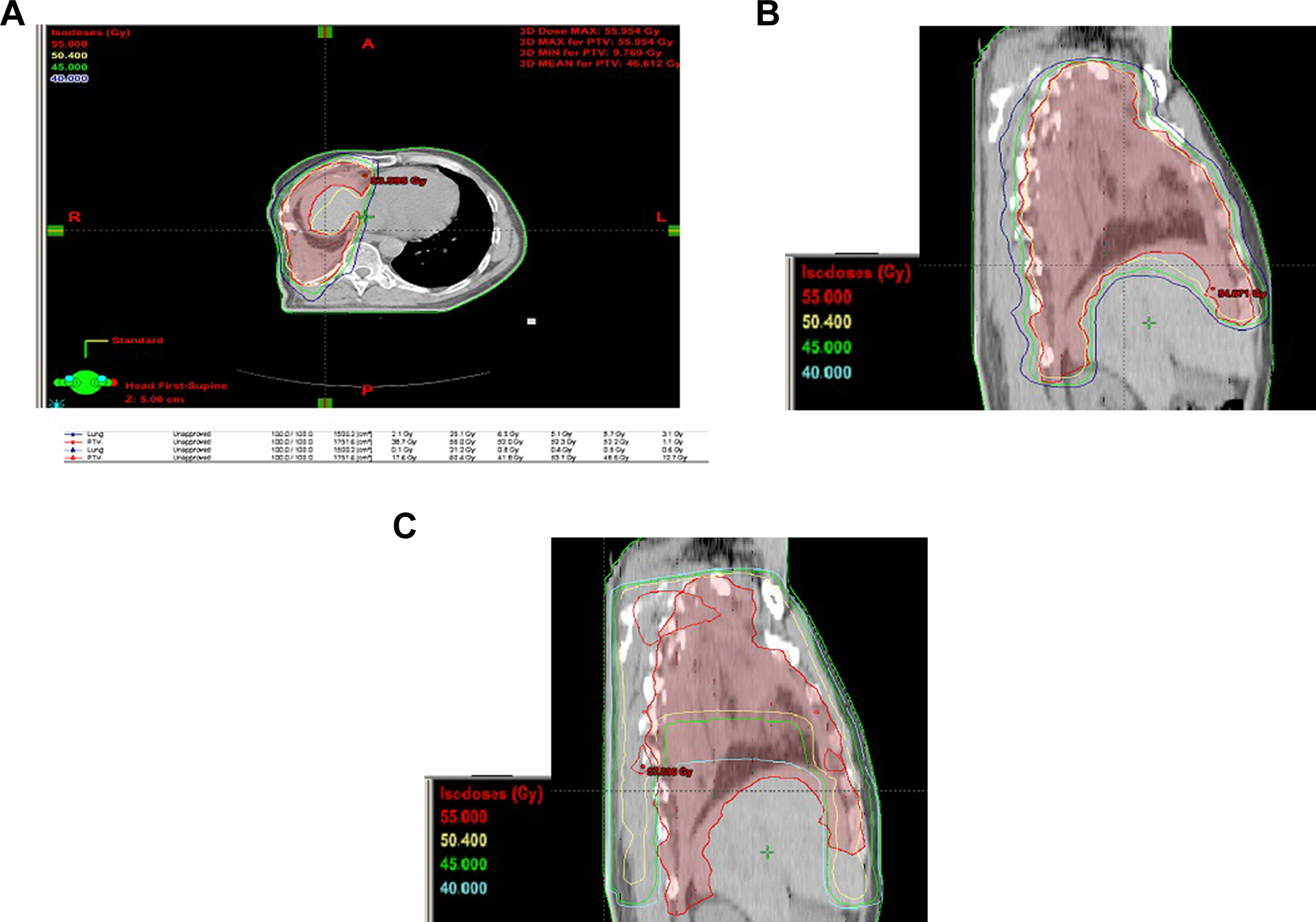
A, Isodose curve of IMRT, suitable to PTV on the axial image. B, Isodose curve of IMRT, suitable to PTV on the sagittal image. C, Isodose curve of 3D CRT, inhomogeneity with PTV on the sagittal image. 3D CRT indicates 3-dimensional conformal radiation therapy; IMRT, intensity-modulated radiation therapy; PTV, planning target volume.
Based on the published dosimetric data that predict fatal pulmonary toxicity, V5 (the percentage of lung volume receiving 5 Gy and higher doses), MLD, V13 (the percentage of lung volume receiving 13 Gy and higher doses), and V20 (the percentage of lung volume receiving 20 Gy and higher doses) were all checked and evaluated on dose–volume histograms. The dosimetric results of the 3D CRT plans on the MLDs and the lung V5 were statistically lower than the results of the IMRT plans. However, higher volumes and doses were obtained in IMRT planning; both the MLD and the lung V5 were considerably lower than the limiting tolerance dose levels. The volume and dose levels determined not to enhance pulmonary toxicity for IMRT in MPM were as follows—MLD < 10 Gy, V5 < 60%, and V20 < 10%; these strict limitations could be generated with beam angle correction and optimization on IMRT plans while irradiating an fairly large, irregular target volume. The dosimetric data for the contralateral lung were as follows—IMRT lung mean dose: 7.36% (range: 5.6%-8.4%), 3D CRT lung mean dose mean: 1.13% (range: 0.62%-1.77%), P = .0001, IMRT lung V5 mean: 57.74% (range: 47.0%-59.9%), 3D CRT lung V5 mean: 2.42% (range: 0.0%-4.9%), P = .0001, IMRT lung V13 mean: 13.43% (range: 4.2%-22.9%), 3D CRT lung V13 mean: 1.95% (range: 0.01%-10.8%), P = .0001, IMRT lung V20 mean: 4.5% (range: 0.5%-9.5%), and 3D CRT lung V20 mean: 0.68% (range: 0.0%-6.22%), P = .04. The maximum MLD found in the IMRT group was 8.4 (could be kept below 10 Gy). Intensity-modulated radiation therapy planning could provide the dose limitation for contralateral kidney (no volume received more than 15 Gy). 6
Isodose curves created with the IMRT plan and with 3D CRT were demonstrated with a case sample in Figure 2A to C to show highly conformal coverage to PTV in IMRT planning, both in axial and sagittal images, with a marked difference from conventional techniques.
Discussion
In the past, mesothelioma was considered as an aggressive and hopeless disease, incapable of cure, and was approached with therapeutic nihilism. With improving experience of surgical procedures, CT, and RT, therapeutic optimism has prevailed. Multimodality approaches and early results offered new hopes. 15,16 Technical developments and new understandings have further refined the multimodality approaches, resulting in lowered mortality and improved outcomes. In the early years of multimodality treatment radiation, oncologists used conventional techniques. The combination of photons and electrons was used to treat such a large and irregularly shaped target with major technical limitations. However, in the early 2000s, studies focused on IMRT as a good alternative for hemithoracal RT, allowing radiation oncologists to treat the pleural bed effectively. But sometimes this treatment caused fatal pulmonary toxicity. 17
Much has been learned about IMRT in MPM in the past decade, notably about radiation algorithms. First, it is now known that lung dose constraints used in lung cancer RT are not capable of predicting radiation pneumonia in patients with MPM. 6,12,18 Second, new dosimetric limits are needed to determine the tolerance levels of the lung for the safe treatment of patients with mesothelioma who must live with only 1 lung.
In this study, we evaluated the dosimetric outcomes of IMRT and compared with those of 3D CRT. Recent studies showed that IMRT provides better dose conformality on the pleural bed, which has an irregular concave shape, and there is a certain agreement between them. However, some studies showed that this positive result is at the cost of increased contralateral lung toxicity. 6,12,18 Allen et al reported unacceptable mortality due to RT pneumonia in the 6 patients of their cohort. 13,17 So we can say that success was tempered by the occurrence of radiation pneumonia in these IMRT studies.
Allen et al concluded that median V20, MLD, and V5 (volume of lung receiving 5 Gy or more) for the patients who developed fatal pneumonitis were 17.6% (range: 15.3%-22.3%), 15.2 Gy (range: 13.3-17.0 Gy), and 98.6% (range: 81.0%-100.0%), respectively. These dose limits seemed extremely high. The general consensus on lung dose constraint in IMRT planning for MPM is (V5) 5 Gy delivered to 60% and less lung volume, with 50% preferable, and a mean total lung dose of 13 Gy and less, with <10 Gy preferable. 6,12,17,18 Moreover, National Comprehensive Cancer Network (NCCN) guidelines suggest a mean total lung dose of <8.5 Gy. 19 Although, reports from research and NCCN identified the inability of IMRT to meet these criteria for most patients, authors conclude that CRT can nevertheless be applied in MPM with an unacceptable conformality of these conventional techniques. Allen et al reported a technique to overcome dose limitations, called restricted field IMRT, in MPM. They showed that strict dose constraints could be imposed with this technique (restricted fields were used to spare the upper portion of the lung). However, as they noted, sparing the upper portion of the lung means also sparing the PTV. 17
While recognizing the limitations of IMRT, we believe that it offers high target conformality and strict OAR dose limits with little beam gantry guidance and dose optimization. The results of our dosimetric study support our opinion. Dosimetric results of IMRT planning showed that V5 could be kept below 60%, and the MLD could be kept below 8.5 Gy. The conformality and homogeneity of IMRT plans were statistically better than 3D CRT plans. This superiority was obtained without any decrement in OAR dose limits.
Technological advances provide different treatment strategies especially in more malignant tumors. One of them is intensity-modulated proton therapy (IMPT) in MPM. Lorentini et al showed that in 7 patients, IMPT is dosimetrically better than IMRT on the OAR doses. However, proton therapy is not widespread, and it is a very expensive treatment in radiation oncology. 20 According to the same target coverage with IMRT and IMPT and more accumulated experience on IMRT, it is believed that IMRT is the appropriate radiation modality in MPM. Additionally in patients with progressive diseases who are not able to undergo resection, IMRT provides efficient tumoricidal dose and good palliation. 21,22
There are some limitations in our study, mainly owing to its retrospective design. This is only a dosimetric study, which means that we can draw no conclusions about patient outcomes in terms of either tumor control or toxicity. However, reviewing the dosimetric data is justifiable because there are documented dosimetric data predicting local–regional control and treatment-related toxicity, which are well described in the literature. Furthermore, the number of patients was small, but considering the rarity of MPM and, moreover, the rarity of curatively managed patients with MPM, the size of the study group could be considered acceptable.
Disease outcomes have been improved by multimodality therapy in MPM, but both local and distant failure remain a significant problem. Local failures in the reported series are 23% to 59% with different fractionation schedules despite RT. 4,8,23 Intensity-modulated radiation therapy is a prominent advanced technology, which can overcome many technical difficulties, according to the target volume of MPM. Superior dose distribution over conventional techniques, conformality, and coherency with target volume has been demonstrated by many investigators. Specifically, studies demonstrated superior target coverage and high conformality in the pleural bed, as well as in the upper abdomen and mediastinum. 10,15,16,24 To overcome high local–regional recurrence, IMRT appears to be the only option for irradiating the target volume with an efficient radiation dose.
Conclusion
In summary, with a large and complex target volume of MPM, IMRT has the ability to deliver an efficient tumoricidal radiation dose while keeping lung dose below tolerance for pneumonitis. Reported lower local recurrence rates of IMRT (13%) in MPM render this irradiation technique necessary for hemithoracal RT. 25 With increasing knowledge of both IMRT and MPM, we will be able to implement more complex and strict radiation treatment plannings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.