
Abstract
Recent studies have reported about the application of volumetric-modulated arc radiotherapy in the treatment of multiple brain metastases. One of the key concerns for these radiosurgical treatments lies in the integral dose within the normal brain tissue, as it has been shown to increase with increasing number of brain tumors treated. In this study, we investigate the potential to improve normal brain tissue sparing specific to volumetric-modulated arc radiotherapy by increasing the number of isocenters and arc beams. Adopting a multi-institutional benchmark study protocol of planning multiple brain metastases via a radiosurgical apparatus, a flattening filter-free TrueBeam RapidArc delivery system (Varian Oncology, Palo Alto, California) was used for a volumetric-modulated arc radiotherapy treatment planning study, where treatment plans for target combinations of N = 1, 3, 6, 9, and 12 targets were developed with increasing numbers of isocenters and arc beams. The treatment plans for each target combination were compared dosimetrically among each other and against the reference Gamma Knife treatment plan from the original benchmark study. We observed that as the number of isocenters or arc beams increased, the normal brain isodose volumes such as 12- to 4-Gy on average decreased by up to 15% for all the studied cases. However, when the best volumetric-modulated arc radiotherapy normal brain isodose volumes were compared against the corresponding reference Gamma Knife values, volumetric-modulated arc radiotherapy remained 100% to 200% higher than those of Gamma Knife for all target combinations. The study results, particularly for the solitary (N = 1) metastases case, directly challenged the general notion of dose equivalence among current radiosurgical modalities. In conclusion, multiple isocenter and multiple arc beam delivery solutions are capable of decreasing normal brain irradiation exposure for volumetric-modulated arc radiotherapy. However, there is further technological development in need for volumetric-modulated arc radiotherapy before similar dosimetric treatment plans could be achievable when compared to Gamma Knife radiosurgery.
Keywords
Introduction
Gamma Knife (GK) technology is considered a reference standard apparatus for the treatment of intracranial lesions with radiosurgery, in particular for treating brain metastases. 1 –5 However, advances in linac-based delivery have enabled this technology to evolve as a potential alternative to GK for radiosurgery. More recently, volumetric-modulated arc therapy and flattening filter-free (FFF) linac designs have resulted in fast delivery with radiosurgical precision. 6 With minutes as opposed to hours required to deliver even complex radiosurgery dose distributions, there are major questions as to what technology is optimal and why in terms of quality and efficiency trade-off.
In order to delineate a qualitative baseline for normal brain tissue-sparing capabilities among contemporary radiosurgical apparatus, multi-institutional benchmark studies have been conducted for both solitary and multiple intracranial targets. 7 –9 In the case of simple solitary target, an equivalent normal brain tissue-sparing effect was observed between GK and linac-based radiosurgery modalities, for example, robotic CyberKnife and dynamic conformal arc deliveries via conventional flattening filter present (FFP) beams. However, for multiple brain metastases, these linac-based radiosurgical treatments were found to yield significantly higher normal brain dosing compared to the reference GK Perfexion (PFX) treatments. 7,8
Without clinical data to show that there is a consequence to these greater integral doses, it may be that the benefit of delivering therapy within minutes with volumetric-modulated arc radiotherapy (VMAT) outweighs any theoretical potential for neurocognitive damage. Our goal is not to address this issue but to examine whether we can adjust the planning technique for VMAT to reduce normal brain tissue dose exposure. One such strategy is to increase the number of arc beams or isocenters, with the rationale that as the number of the beams increases, the dose contribution from individual beams decreases. For example, if we assume for 18 equally weighted coplanar beams (10° apart covering a span of 180°) focused at the isocenter, each beam would contribute approximately 1 (or 6%) of 18 of the total summed dose at the isocenter. However, when the number of beams increases to 180 (eg, 1° spaced apart simulating a continuous arc beam irradiation), then each beam would contribute <1% of the total dose at the isocenter. Consequently, the entrance dose for the 180-beam arrangement would be significantly less than that of the 18-beam arrangement. The goal of the present study is to investigate whether more arc beams could significantly impact normal brain tissue doses for single as well as multiple brain tumors when treated with VMAT.
Materials and Methods
Standard data sets utilized in our prior multi-institutional benchmark study were adopted for the current study. 7 This data set was created from a patient previously treated with stereotactic radiosurgery (SRS), anonymized, reviewed, and approved by the institutional review board. The data set consisted of computed tomography and magnetic resonance (MR) images with contours for a multiple brain metastases case with 12 brain tumors distributed throughout the brain. The total summed target volume was 5.4 mL, and all targets were approximately ellipsoidal in shape. A 3-dimensional rendered MR-referenced planar image showing the location and numbering of these targets is illustrated in Figure 1. Per the benchmark study protocol, 4 preset groups of target combinations (N = 3 [1.8 mL], 6 [3.1 mL], 9 [4.1 mL], and 12 [5.4 mL]) as in Figure 1 were used for VMAT treatment planning. Specifically, for the current study, a solitary target (No. 12 of Figure 1) with a volume of 1.04 mL and N = 3 target combinations was also selected for VMAT treatment planning subject to varied number of arc beam configurations, and isocenters are placed in center of mass of the metastatic lesions.
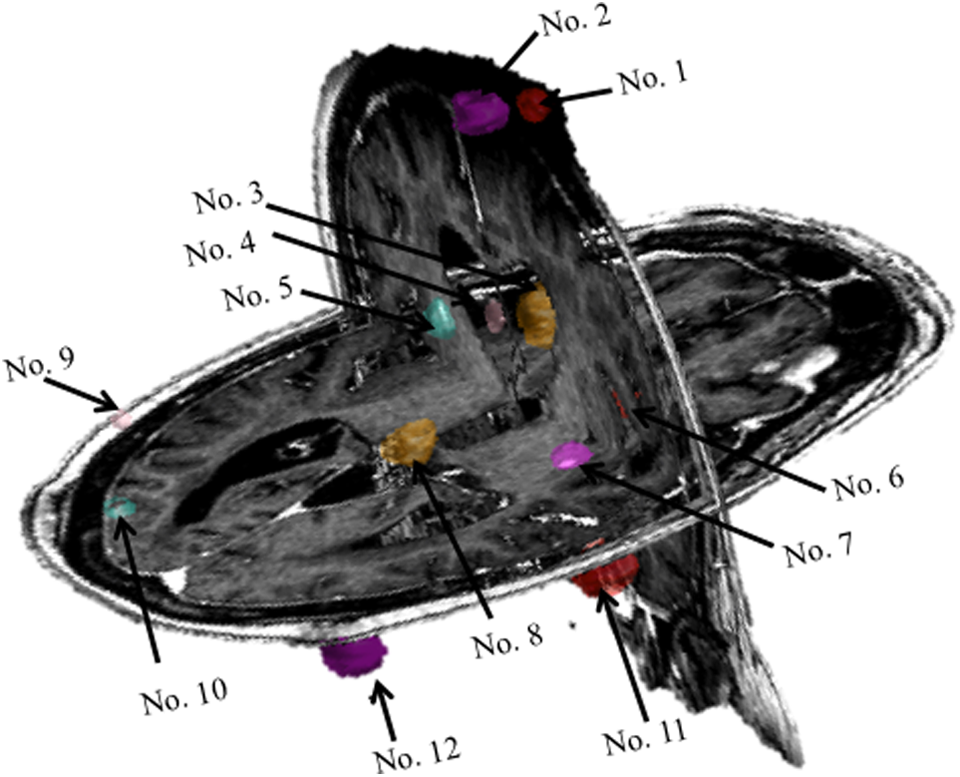
Illustration of the target location for the benchmark case: Target No. 12 was selected for N = 1 target treatment planning; Target No. [9, 11, 12] 7,8 were selected for N = 3 target treatment planning; Target No. [1, 2, 8, 9, 11, 12] were selected for N = 6 target treatment planning; Target No. [1, 2, 4, 7, 8, 9, 10, 11, 12] were selected for N = 9 target treatment planning; and finally all targets were selected for N = 12 target treatment planning.
In order to systematically adjust the total number of arc beams and compare results against the reference data based on the GK radiosurgery system, as described in our previous benchmark study, the linac system of an independent manufacturer (Varian, Palo Alto, California) was adopted for VMAT treatment planning using 6 MV FFF X-ray beams with a 2.5-mm multileaf collimator (MLC) capable of delivering intensity-modulated arc beams with an output of 1400 MU/min. All VMAT (RapidArc [Varian, Palo Alto, California]) plans were calculated on a 2.5-mm grid using Eclipse Version 11 treatment planning system (Varian, Palo Alto, California). The panel inserts of Figure 2 illustrate the multiple arc beam arrangements for the current study, that is, 1-arc, 3-arc, 5-arc, and 7-arc beams for the individual target combinations (N = 1, 3, 6, 9, and 12). Following the general clinical practice of VMAT planning as recommended by the manufacturer, a 360° trans axial arc beam was included in all multiple arc beam arrangement. Plans with 3, 5, and 7 arcs were accomplished using additional noncoplanar beams with couch angles of 0°, 15°, 30°, 45°, 345°, 330°, or 315° in which half-rotation arcs were used. The collimator angle of 30° was used for 1-arc plan, and rest of the multiple arc beam plans used alternate 30° or 330° collimator angle. The gantry and collimator angles for the 1-arc, 3-arc, 5-arc, and 7-arc beam arrangements are described in the legends of Figure 2. Note that these arc beam arrangements were largely derived from the beam configurations of traditional cone-based SRS planning and previously published VMAT planning techniques 10 as well as user experiences.

Plot of normal brain volume enclosed by different levels of isodose values for the solitary target planned with varied volumetric-modulated arc radiotherapy (VMAT) techniques, that is, 1-arc, 3-arc, 5-arc, and 7-arc configurations as illustrated in the graph.
All targets were prescribed 20 Gy to cover at least 99% of each individual target volume regardless of solitary or multiple targets involvement plus normal tissue constraints as stipulated in the benchmark study protocol. 7 In short, all treatment plans were developed with maximal effort to ensure clinical deliverability of these treatment plans. In another word, the goal of our study is to compare clinically feasible treatment plans for both GK and VMAT. Of note, no specific dose constraints were enforced for critical structures for VMAT plans per our previous publication. 8 However, constraints for maximum dose hot spots were ≤110% and (brain–planning target volume (ptv)), with priority of 75 to 85 were used for all VMAT plans. As a general practice, the GK treatment plans tended to posses the dose hot spots up to 200% of the prescription dose, whereas the VMAT treatment plans typically possessed the dose hot spots up to 116% of the prescription dose. This was also contributed by the hardware limitations and clinical practice considerations such as a finite number of shots for GK, and MLC leakage due to the wider jaw opening to cover combined 2 or more targets and also the limitation of MLCs to close completely between targets at different angles when single isocenter was used to plan multiple targets at the same time for VMAT delivery, and so on. Finally, the normal brain volumes at the peripheral isodose levels of 4, 8, 12, 16, and 20 Gy were compared among each VMAT treatment plans of different arc beam combinations and also against the reference GK PFX data.
Results
Results for the solitary target for varied arc beam combinations via FFF beams are shown in Figure 2. When compared with the 1-arc treatment plans, all multiple arc treatment plans exhibited significant decreases in the order of 20% to 30% for all the peripheral isodose volumes (ie, 16, 12, 8, and 4 Gy). Of note, similar improvements were also noted at the prescription isodose level (ie, 20 Gy), indicating higher dose conformity as more noncoplanar arc beams were used for treatment planning. However, when comparing 3-arc, 5-arc, and 7-arc treatment plans, the differences in the isodose volumes among the treatment plans were significantly less with a consistent trend of 5-arc treatment plans producing the highest peripheral isodose values, whereas the 3-arc or 7-arc treatment plans produced the lower values. Such a variation was commonly encountered as in conventional linac SRS and was mostly caused by a preconfigured gantry/couch/collimator arrangements to cover random distributions of multiple intracranial targets. However, when compared to the reference GK PFX values, all VMAT treatment plans produced remarkably higher values (approximately a factor of 2) in the peripheral isodose volumes.
The results for the multitarget VMAT treatment planning via multiple arc (eg, 3-arc, 5-arc, and 7-arc) treatment deliveries are shown in Figure 3. Note that Figure 3 is plotted with a logarithmic scale to highlight the high isodose volumes such as differences in the 20- and the 16-Gy dose levels. Conventional 1-arc configuration was unable to produce treatment plans satisfying dose–volume constraints. For lower isodose volumes, such as the 8- or 4-Gy dose levels, the differences between the multi-isocenter multiple arc deliveries were in the range of 4.4% to 15.4% (average: 8.9% ± 3.8%) from their respective median values for all the cases. For all the VMAT results, the low isodose level volumes such as the 8- and 4-Gy isodose levels were averaged 275% ± 132% higher when compared to the reference GK PFX values. Furthermore, the 12-Gy isodose volumes and the 16-Gy isodose volumes were on average 179% ± 91% and 129% ± 40% higher than the GK PFX values, respectively. These results are in good agreement with previously reported data (9) obtained using tighter optimization constraints, whereas in the present study, clinically deliverable FFF VMAT treatment plans with a maximum dose of <116% of the prescription dose are achieved.
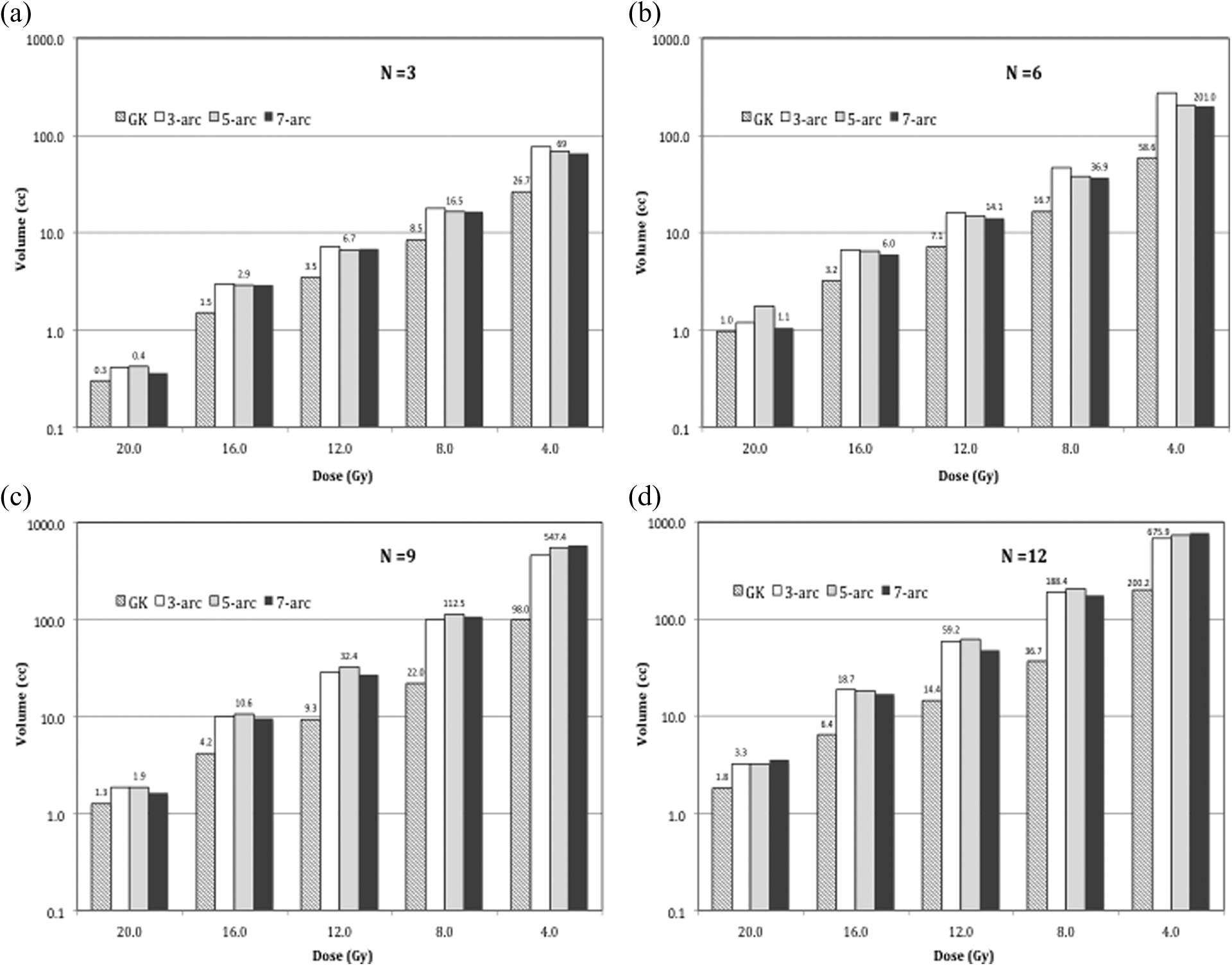
Semilogarithmic plot of normal brain volume dependence on the isodose levels for multitarget (N = 3, 6, 9, and 12) treatment planning with the multi-arc/multi-isocenter technique. Note the large discrepancy between the volumetric-modulated arc radiotherapy (VMAT) technique and the reference Gamma Knife (GK) values at the peripheral isodose volumes such as from the 12-Gy to the 4-Gy isodose levels.
Discussion and Conclusions
The peripheral dose distributions within the normal brain tissue surrounding the radiosurgery target(s) are expected to vary based on treatment technique and specifically for VMAT based on number of arcs and isocenters. In this technical report of VMAT treating brain metastatic lesions, we found that the normal brain tissue-sparing effect can be improved on the order of 5% to 10% in the peripheral 8-Gy to 12-Gy isodose volumes by increasing the number of isocenters and arc beams per routine clinical practices at our institutions. However, the magnitudes of improvements are not significant enough to overcome the differences observed between VMAT and the reference standard GK PFX treatment plans for the same lesions.
Similar levels of discrepancy were further noted for a solitary lesion planned with FFF beam-based VMAT as compared to a standard GK PFX treatment plan. Such an observation suggests that FFF beam-based VMAT of solitary intracranial lesions may be dosimetrically unique when compared to a conventional FFP beam-based SRS for managing solitary lesions as reported in a prior study. 9
Considering the results of the current study to those of prior, 2 essential areas emerged as key to normal brain sparing for multiple target brain SRS: (1) dose fall-off near a single target and (2) dose interplay or dose interference among neighboring targets when multiple targets are involved. The results of the current study suggest that increasing the number of isocenters or FFF-based arc beams does not significantly impact either of these 2 factors. This is likely caused by the peripheral dose characteristics of the FFF beams where narrowly collimated beamlets tend to elevate the peripheral dose compared to those of the GK PFX beams. Therefore, one potential area of improvements lies in sharpening the penumbra of the current FFF beams, as applied to VMAT, as this may directly impact these 2 factors. In fact, such an improvement has already been observed for the GK beam geometry in a prior study, 11 where adding shaped metal flattening filters to intersect individual GK beamlets was found effective in improving the normal brain sparing for majority of the cases.
Given elevated normal brain tissue dose, radiosurgery practitioners need to exercise caution in dose prescription and target margin assessment when applying the emerging technologies such as VMAT in single and multiple target intracranial SRS. Our study highlighted the relationship between the peripheral target dose and the dose to the surrounding normal brain tissues as reported previously. 8 In essence, due to steep dose fall-off surrounding a radiosurgical target, a seemingly small expansion or contraction on the prescription isodose volume can lead to large dose variations to the target periphery, thus dramatically altering the dose to the surrounding normal brain tissue. 12 As a result, care must be taken to ensure proper dose to the target first before comparing or surveying peripheral isodose volumes such as 12, 8, and 4 Gy across different treatment modalities.
The clinical implications of the low-dose irradiation of the normal brain are unknown, awaiting the results of clinical studies such as the North American Gamma Knife Consortium trial and RTOG 0933 trial results. However, animal study 13 and early data 14,15 have all pointed to a low tolerance dose and essential need to spare critical neurostem cell compartments including hippocampi in normal brain irradiation to improve neurocognitive functions of the patients. Given the Quantitative Analysis of Normal Tissue Effects in the Clinic (QUANTEC) practice guideline and known correlation between low-level isodose volumes and the treatment complications, 16 –18 maximally sparing the normal brain via technical improvements is therefore highly warranted. Ultimately, clinical trials such as North American Gamma Knife Consortium will help define acceptable levels of normal brain irradiation on neurocognitive functional outcomes in managing metastatic brain tumors with SRS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Sahgal holds research grants from Elekta AB and Dr Sahgal and Dr Ma received honorarium for past educational seminars from Elekta AB.