
Abstract
Aim:
To evaluate the role of stereotactic body radiation therapy in the retreatment of locally recurrent cervical cancers. Brachytherapy is the main choice to treat gynecologic cancers.
Methods:
Patients with recurrent cervical cancer, previously submitted to radiotherapy, were treated with stereotactic body radiation therapy using a CyberKnife system (Accuray Incorporated, Sunnyvale, California) with a fiducial tracking system.
Results:
From August 2011 to October 2014, 5 patients have been treated. Median age was 81 years (range, 70-84 years). Two patients were diagnosed with adenocarcinoma endometrioid and 3 with squamous cell carcinoma. Toxicity was scored according to the Radiation Therapy Oncology Group/European Organization for Research and Treatment of Cancer criteria. After a median follow-up of 12 months (range, 8-34 months), no severe (>grade 3) acute/late genitourinary or low gastrointestinal toxicity was observed.
Conclusion:
Our preliminary results of stereotactic body radiation therapy “simulating” high dose rate for recurrent cervical cancers confirm a minimal toxicity and an optimal outcome. The stereotactic body radiation therapy is an alternative to high dose rate brachytherapy for gynecologic tumors.
Introduction
Locally recurrent cervical cancer is treated with external beam radiation therapy (EBRT) and concurrent chemotherapy followed by brachytherapy (BT), tumor directed, boost. 1 –4 In patients submitted to previous irradiation, a retreatment represents a challenge. An option could be BT, which is able to deliver high doses to the tumor with normal tissue sparing. However, some patients with gynecologic cancer have clinical conditions that do not allow to deliver BT (ie, patients with several comorbidities or “unfavorable anatomy”). In these instances, stereotactic body radiotherapy (SBRT) could be an alternative to BT because it permits to deliver high doses of external radiation resembling BT dose distribution 5,6 using multimodal imaging. 7 This is confirmed both in several retrospective clinical reports 8 –13 and in retrospective dosimetric reports. 14 Common toxicities using SBRT for treating pelvic tumors are diarrhea, cystitis, and proctitis. 15
The aim of this study was to report, using an endovaginal device such as “fiducials,” outcome, technique, dosimetry, and toxicity after CyberKnife treatment (as BT like) in patient with recurrent cervical cancer. To the best of our knowledge, our study is the first that reports the use of endovaginal device for tracking in an image-guided radiation therapy (IGRT) modality.
Methods
Patients with histologic diagnosis of recurrent gynecologic cancer, previously irradiated (EBRT:45 Gy/25 Fx plus BT boost:15 Gy/3 Fx) with several comorbidities or unfavorable anatomy, were considered for this study. The exclusion criteria for BT, which we used in a recurrent setting, were comorbid conditions of the patients (patients who do not have a good performance status to support a general anesthesia for the insertion process of a BT’s applicator), size and location of the recurrent tumor, stenotic and short vaginal stump in intracavitary cylinder procedures, difficulty in visualization of the tumor and proximity to bladder and bowel for interstitial procedures, and inability to place Smit Sleeve through the uterus and short endocervix in tandem ovoid procedure. Five patients were enrolled, of which 3 had surgery (hysterectomy) followed by EBRT and BT before the recurrence and 2 had not undergone surgery (see Table 1). Besides, patients had a Karnofsky Performance Status >70, a life expectancy >6 months, and some contraindication for BT. The pretreatment evaluation included physical examination, complete blood count, computed tomography/positron emission tomography (CT/PET), pelvis magnetic resonance imaging (MRI), and biopsy in which a small amount of tissue was removed; other investigations were performed in the presence of clinically suspected signs. Fully informed, written consent was required. Patients with cervical recurrence used an intravaginal applicator for fiducials tracking in IGRT modality (Figure 1). The vaginal applicator, CT and MRI compatible and cleaned and sterilized, has a cylinder form with a diameter of 1 cm and a length of 10 cm, adapting to each patient’s anatomy (ie, stenosis). In the cylinder, embedded with wax (a substance with the density of water), we placed 3 gold landmarks for IGRT with fiducials tracking system, and this gold fiducials do not alter dosimetric calculation. 16 The applicator is arranged to maintain contact with the distal stump of the vagina or with the proximal portion of the cervix. A sign positioned on the applicator “that identifies the 12-o’clock position” obtains orientation. However, angles and rotations are corrected by fiducials tracking system. The patient was positioned supine on the treatment couch and immobilized with a vacuum bag for SBRT treatment. For all patients, a multislice CT scan (Siemens Sensation 16 [Siemens AG Medical Solutions, Germany]) and an MRI (Siemens Magnetom 1.5 T [Siemens AG Medical Solutions, Germany]) were performed.

The intravaginal applicator (A) with 2 internal gold fiducials for the fiducials tracking (B) in image-guided radiation therapy (IGRT) modality.
Patients Characteristics.
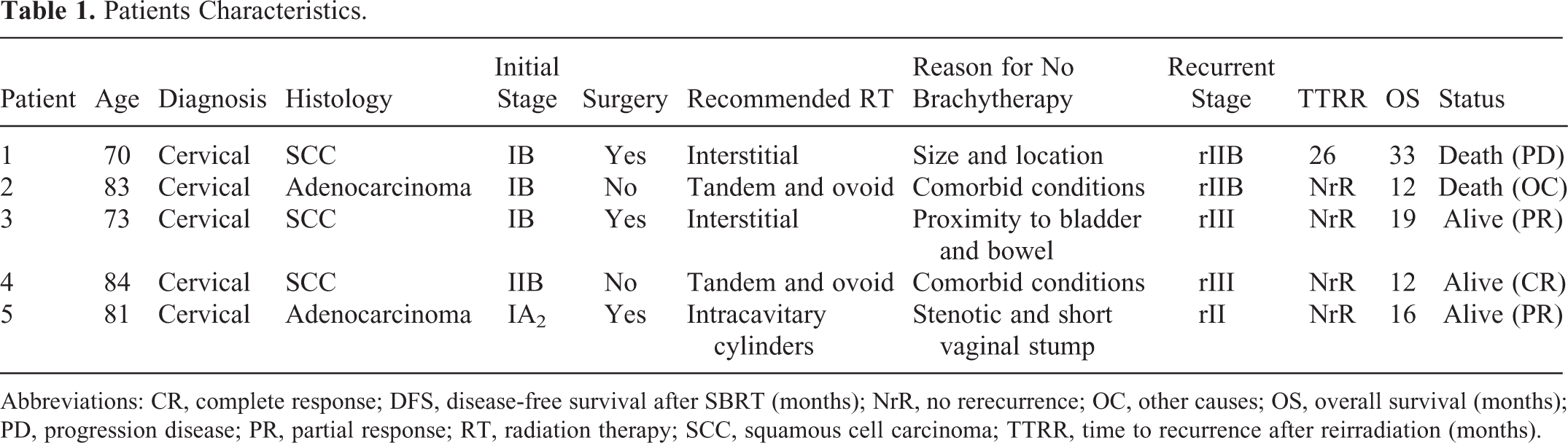
Abbreviations: CR, complete response; DFS, disease-free survival after SBRT (months); NrR, no rerecurrence; OC, other causes; OS, overall survival (months); PD, progression disease; PR, partial response; RT, radiation therapy; SCC, squamous cell carcinoma; TTRR, time to recurrence after reirradiation (months).
The CT protocol followed the CyberKnife-specific requirements, namely acquisition 16 × 0.75 mm, kV 120, effective mAs 320, rotation time 1 second, pitch 1.15, reconstruction slice 1.5 mm, reconstruction increment 1.5 mm, filter reconstruction H31 (smooth), and 512 × 512 matrix. Magnetic resonance imaging was performed with the following parameters: matrix 512 × 512, flip angle 0°, effective thickness 0.88 mm, reconstruction slice 1.5 mm, and reconstruction increment 0 mm. The axial source images were transferred to the CyberKnife workstation for treatment planning (Multiplan System [Multiplan Treatment Planning System - Accuray Incorporated, Sunnyvale, California]) of SBRT modality. The contouring of the tumor and critical volumes were defined with fusion MRI (T1 and T2 sequences) and CT imaging. Stereotactic body radiotherapy target consisted of the gross tumor volume (GTV), which coincided with a gross disease noted on MRI and physical examination. The GTV was uniformly expanded by 2 mm to create a planning target volume (PTV). In patients with small intestine or other critical structures adjacent to targets, the PTV was subtracted from the organs at risk to decrease dose to the organs at risk. The SBRT treatment planning was obtained with inverse planning algorithm using a nonisocentric technique. A heterogeneous dose distribution was generated to emulate HDR-BT. Figure 2 shows isodose distribution. We utilized IRIS collimator with different diameter.

Nonisocentric treatment planning with Multipan-CyberKnife emulating brachytherapy: Dose–volume histogram (DVH; A) and dose distribution (B) are shown.
The dose for retreatment was 15 to 20 Gy in 3 to 4 fractions depending on constraints to critical organs. The constraints of the maximum dose used were 13 Gy for rectum (D1cc < 10 Gy), 5 Gy for bladder (D1cc < 3 Gy), and 5 Gy for intestinal loop (D1cc < 4,5 Gy). Three days before and for all days of treatment, patients were prescribed diet free of slag, and all patients were instructed to empty their rectum by self-administered enemas.
Patients were followed up every 3 months with MRI and 6 months with CT/PET, and the peak toxicity was measured after 2 weeks posttreatment. The acute and late toxicity were recorded using the Radiation Therapy Oncology Group/European Organization for Research and Treatment of Cancer criteria (RTOG/EORTC) criteria. All patients, 3 months after treatment, were submitted to the cervical biopsy to verify freedom from local tumor recurrence. Oncologic outcomes at follow-up were based on combination of both the physical examination and the follow-up imaging.
Results
From August 2011 to October 2014, 5 patients with gynecologic cancer were treated with SBRT modality using the CyberKnife System (Accuray Incorporated, Sunnyvale, California). Enrolled patients had a median age of 81 years (range, 70-84 years), and the median follow-up was 12 months (range, 10-34 months; Table 1). The SBRT dose to the target was 18 Gy (range, 15-20 Gy) delivered in 3 or 4 consecutive sessions, prescribed to the median isodose line of 72% (range, 68%-73%). The median Dmax (maximal dose) was 2500 cGy (range, 2055-2647 cGy). The biologically equivalent dose in terms of equivalent doses given at 2 Gy per day (EQD2) was calculated using the linear quadratic equation. 16 The α–β ratio was taken to be 10 Gy for tumor effects. The median EQD2 for the tumor was 24 Gy (range: 18.8-25 Gy) for the entire group, and the median cumulative EQD2 was 85.2 Gy (range: 81.5-88.8 Gy; Table 2).
Treatment Characteristics.a

Abbreviations: BT, brachytherapy; EBRT, external beam radiation therapy; EQD2 cum, equivalent doses given at 2 Gy per day cumulative; GI, gastrointestinal; GU, genitourinary; LQ, linear quadratic; LQ EQD2, equivalent doses given at 2 Gy per day for LQ model; SBRT, stereotactic body radiotherapy; TTR, time to recurrence after the first course of radiotherapy (months).
aEBRT plus BT: first complete treatment after surgery in patients with gynecologic cancer. SBRT: Retreatment after recurrence.
The median volume of the tumor was 20 cm3 (range, 8.2-47.4 cm3). The median coverage of the target was 96.3% (range, 95.4%-97.5%), the median number of beams was 181 (range, 153-197), the median conformity index was 1.5 (range, 1.13-1.76), the median homogeneity index was 1.39 (1.28-1.47), and the median new conformity index was 1.56 (range, 1.28-1.47). The median number of total monitor unit was 25 436 (range, 16 865-28 340). The median value of Dmax at the critical organ was 1757 cGy at the bladder (range, 1582-1912 cGy), 1747 cGy at the rectum (range, 1444-1945 cGy), 868 cGy at the bowel (range, 391-1997 cGy), 448 cGy at the left femur head (range, 163-649 cGy), and 469 cGy at the right femur head (range, 1582-1912 cGy). The median D2cc value at the critical organ was 3 Gy at the bladder, 8 Gy at the rectum, and 4 Gy at the intestinal loop.
Figure 3 shows the complete clinical remission at CT/PET. The results of clinical responses for all patients were reported in Table 2. Six months after treatment, the biopsy results were absence of neoplastic cells with the presence of inflammatory cells in 3 patients classified as complete response and persistence of neoplastic cells in the other 2 patients classified as partial responses. One patient died for other causes and 1 for progression of disease in 1 site different to the retreatment. During the SBRT boost, 1 patient was noted to have acute toxicity (G2 genitourinary [GU] and G2 gastrointestinal [GI]). There were no grade 3 or greater toxicities during SBRT or within 90 days after SBRT.

Computed tomography/positron emission tomography (CT/PET) shows the clinical remission 6 months after the CyberKnife stereotactic body radiation therapy (A) with respect to CT/PET pretreatment (B; patient 5).
Discussion
Aggressive therapeutic approach is suggested when a locally recurrent cervical cancer occurs. In some instances, age, comorbidities, and unfavorable anatomy contraindicate both surgery and BT. In this article, we describe an alternative curative approach using SBRT in 5 elderly patients who were unsuitable for aggressive treatment. Besides, we report the use of a homemade device in patients with important vaginal stenosis, and this device was necessary to perform an adequate fiducials tracking.
Few reports describe SBRT in primary or recurrent gynecological cancers. 8 –14 We used the CyberKnife system that permits delivery higher doses safely, and this method was also described by Molla et al, 9 Higginson et al, 11 and Kunos et al. 17 In our study, we report our experience in patients with recurrent cervical cancer, unfavorable to be treated with BT, in which we added the use of intravaginal applicator for fiducials tracking. To the best of our knowledge, our study is the first report on the use of a homemade intravaginal fiducials support. This device could replace the cruent insertion of the 3 gold fiducials into the treatment volume.
In fact, Higginson et al 11 have reported data about the treatment with CyberKnife SBRT for pelvic recurrences using the internal gold fiducials for tracking in patients who did not have any reasonable option to receive BT. Guckenberger et al 12 have treated 19 patients with large pelvic recurrences using a body cast for immobilization and cone-beam CT for verification of position. Kunos et al 17 instead attempted to use CyberKnife SBRT and fiducials tracking with intralesion gold fiducials to salvage recurrent vulvar squamous cell.
We confirm the efficacy and safety of SBRT using CyberKnife because we observe negligible GU and GI toxicities. 17,18 The complete response was observed in 3 of the 5 patients and partial response in 2 of the 5 patients. The efficacy of SBRT as curative treatment should be evaluated with the understanding that SBRT currently is reserved for difficult clinical situations, that is, either recurrent disease after prior irradiation or tumor too large or anatomically difficult for BT and when these patients have no other treatment options. 10
In conclusion, we can affirm that BT remains the standard of care to deliver higher radiation doses in gynecological cancers; however, in patients with recurrent cervical cancer previously submitted to irradiation and unable to receive a BT procedure, SBRT is both safe and effective. Further studies are needed to confirm our results.
Footnotes
Authors’ Note
All the authors contributed equally to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.