
Abstract
Glypican-3 has been reported to be one of the most promising serum markers for hepatocellular carcinoma. This study aimed to assess the clinical utility of serum glypican 3 for the diagnosis of hepatocellular carcinoma. We recruited consecutive patients on a large scale, 283 with hepatocellular carcinoma, 445 with chronic hepatic diseases, and 162 normal controls, to assess the diagnostic accuracy of serum glypican 3 for hepatocellular carcinoma by enzyme-linked immunosorbent assay. In addition, we further analyzed the relationship between the serum levels of α-fetoprotein and glypican-3 in patients with hepatocellular carcinoma. The results indicated that serum glypican 3 was elevated in patients with hepatocellular carcinoma (0 ng/mL, range = 0-14.0 ng/mL, P = .033) and liver cirrhosis (0 ng/mL, range = 0-12.5 ng/mL, P = .001) compared to the levels in normal control (0 ng/mL, range = 0-4.3 ng/mL), but there was no difference between hepatocellular carcinoma and liver cirrhosis (P = .097). The area under the curve of the receiver–operating characteristics curve for hepatocellular carcinoma versus all controls was 0.519, with a sensitivity of 39.9%, a specificity of 60.6%, and an optimal cutoff value of 0.002 ng/mL. The positive and negative predictive values were 32.0% and 68.3%, respectively. No significant correlation in serum levels was observed between glypican 3 and α-fetoprotein (P > .05). The diagnostic sensitivity for hepatocellular carcinoma increased to 72.8% (206 of the 283) when glypican 3 was combined with α-fetoprotein. Glypican 3 was not a promising serum maker for the diagnosis of hepatocellular carcinoma alone, but it could be complementary to α-fetoprotein and elevate the sensitivity of hepatocellular carcinoma diagnosis.
Introduction
Alpha-fetoprotein (AFP) is widely used in clinical practice as the best serum maker for the diagnosis of hepatocellular carcinoma (HCC) at present. However, a recent study found that the sensitivity of AFP is only 25% to 65% at the commonly used cutoff of 20 ng/mL, and many patients with chronic hepatitis, liver cirrhosis, other liver diseases, or gastrointestinal cancer also have elevated serum levels of AFP. 1 These reports indicated that AFP determination lacks adequate sensitivity and specificity for effective diagnosis of HCC. 2 Thus, novel and reliable makers are urgently needed to improve the accuracy of HCC diagnosis.
Glypican 3 (GPC3) belongs to the glypican family of glycosylphosphatidylinositol-anchored heparan sulfate proteoglycans, which plays an important role in cellular growth, differentiation, and migration. 3 Several studies have reported that GPC3 is absent in normal human tissues but highly expressed in fetal liver, HCC tissues, and most HCC cell lines. 4 –7 These studies indicate that GPC3 has been regarded as a useful histological maker in the diagnosis of HCC. In 2003, Capurro et al first reported the diagnostic accuracy of serum GPC3 for HCC with a sensitivity of 53%. 8 Since then, several subsequent studies have found elevated serum GPC3 levels in patients with HCC and a lack of correlation with AFP. 9 –12 However, the diagnostic value of serum GPC3 remains controversial, especially when compared to AFP. After analyzing data of 200 patients with HCC and 200 patients with chronic liver diseases, Yasuda et al found no elevation in serum GPC3 levels in patients with HCC in comparison to those with chronic liver disease, indicating that there was no clinical utility of serum GPC3 in the diagnosis of HCC. 13 Similarly, Özkan et al also reported that GPC3 was not a useful diagnostic or prognostic marker for HCC. 14 All of these studies had limitations, such as small sample size, a lack of healthy controls, or a lack of controls with nonmalignant chronic liver disease. In this study, we aimed to evaluate the clinical utility of GPC3 as a serum marker for HCC by analyzing large-scale data from participants with chronic liver disease and healthy controls in the National Cancer Institute’s Early Detection Research Network-defined phase 2 biomarker study. 15 We also examined whether serum GPC3 could improve the diagnostic accuracy of HCC when combined with AFP.
Methods
Patients and Serum Samples
A total of 890 consecutive participants from Tianjin Third Center Hospital, Tianjin Medical University, Tianjin, China, were enrolled in this study between January 2010 and August 2013. The patients were classified into 5 groups: 283 patients with HCC, 267 patients having cirrhosis without HCC (liver cirrhosis [LC]), 162 patients with chronic hepatitis B (CHB), and 16 patients with atypical hyperplasia (AH). In addition, 162 normal controls (NCs) were recruited from people admitted for regular health examinations who were found to have normal liver biochemical function, no history of liver disease, no viral hepatitis, and no history of any other tumor or malignant disease.
The diagnosis of HCC was made by clinical characteristics, imaging evidence (ultrasound, computed tomography, or magnetic resonance imaging characteristics), and biochemistry (AFP level and liver function), and it was confirmed by histopathology after resection according to the American Association for the Study of Liver Diseases guidelines. 16 All of the patients with HCC attended the hospital for the first time and did not receive any surgery or intervention therapy. Tumor stage was defined using the Barcelona Clinic Liver Cancer (BCLC) staging system. Early HCC was defined as 0 and A, and 96 patients were classified in early HCC. A total of 187 cases with HCC were classified in BCLC stages B, C, and D (Table 1). Patients with hepatitis were diagnosed on the basis of biochemical function examination revealing positivity for HBsAg for the previous 6 months and hepatitis B virus (HBV) DNA concentrations higher than 103/mL. Patients with cirrhosis and AH were confirmed by histopathology of liver biopsy samples. Written consent was obtained from all patients when they were recruited.
Correlation Between Serum GPC3 Levels and Clinical Characteristics of Patients With HCC.

Abbreviations: AFP, α-fetoprotein; GPC3, glypican-3; HCC, hepatocellular carcinoma.
All serum samples were obtained using serum separator tubes at the patient’s initial presentation before any treatment. The samples were allowed to clot for 30 minutes at room temperature before centrifugation for 15 minutes at 1000g and then stored at −80°C until testing.
Detection of Serum AFP and GPC3 Levels
The concentration of serum GPC3 was detected by 2 researchers (XJ and JL) who had no access to the patients’ clinical information. Assays were performed with a human GPC3 DuoSet enzyme-linked immunosorbent assay (ELISA) development kit (catalog number: DY2119; R&D Systems, Minneapolis, Minnesota) strictly according to the manufacturer’s instructions. Briefly, a 96-well microplate was coated with the monoclonal antibody to GPC3 and incubated at room temperature overnight. After blocking plates for a minimum of 1 hour, the serum specimens to be detected were added as were the standards and appropriate controls. A detection antibody was added after washing the microplate, incubated for 2 hours at room temperature, followed by the addition of streptavidin-horseradish peroxidase. Color development was observed after adding substrate solution, and then the reaction was stopped with stop solution. Finally, the optical density was determined at 450 nm and referenced to 546 nm on a microplate reader. All measurements were performed in duplicate.
Statistical Analysis
All statistical analyses were performed with SPSS 19.0 software. The results were expressed as the mean ± standard deviation (SD) or median for nonparametric data. Differences between 2 independent groups were compared with the Mann–Whitney U test (continuous variables and nonparametric analyses). Receiver–operating characteristics (ROC) curves were performed to assess sensitivity, specificity, and respective areas under the curve (AUCs) with 95% confidence interval (CI). The optimum cutoff value was set according to the ROC curve. The Spearman correlation coefficient was used to analyze the association of serum levels between GPC3 and AFP. The correlation between serum GPC3 and clinicopathological characteristics were analyzed with the χ2 test. P values of <.05 were considered statistically significant.
Results
The clinicopathological characteristics of the 890 participants in the present study are summarized in Table 2. All 283 patients with HCC included 231 males and 52 females, and their mean age was 59.0 ± 9.6 years. Of them, 228 patients had HBV infection, and the Child-Pugh class of patients with HCC was 140 cases in class A, 93 cases in class B, and 50 cases in class C. The serum AFP levels were ≤20 ng/mL in 121 patients and ≥400 ng/mL in 43 patients.
Clinical Characteristics of the Patients.

Abbreviations: AFP, α-fetoprotein; AH, atypical hyperplasia; CHB, chronic hepatitis B; F, female; HCC, hepatocellular carcinoma; LC, liver cirrhosis; M, male; NC, normal control.
Serum GPC3 Level for the Diagnosis of HCC
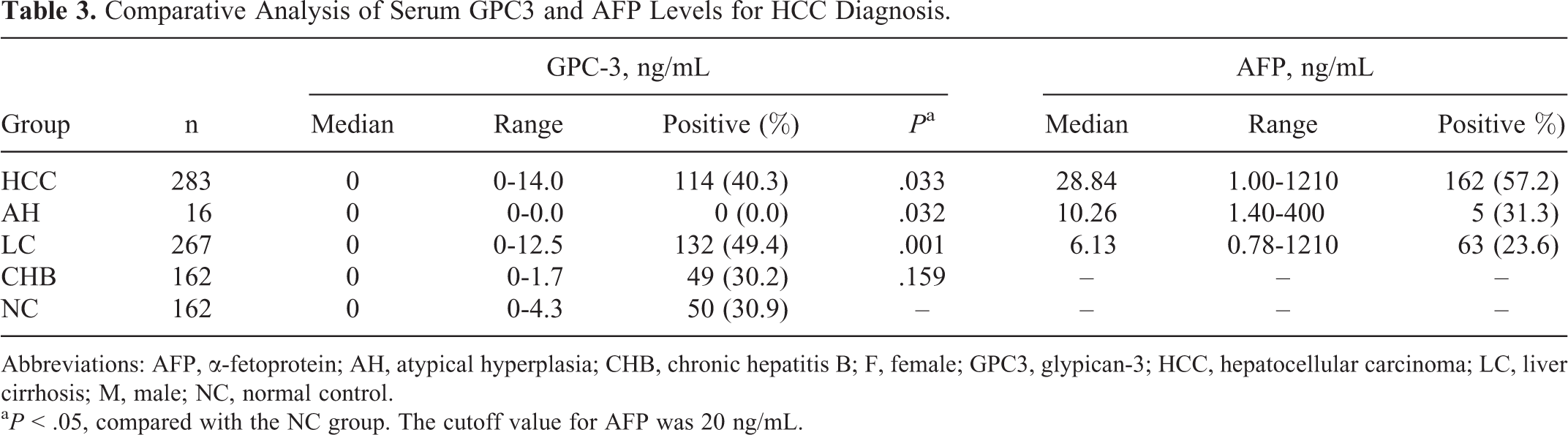
The standard curve of the sandwich ELISA for GPC3, with a linear detection range of 0 to 20 ng/mL (regression coefficient, .9989), is shown in Figure 1A. The intra-assay coefficient of variation (CV) and interassay CV were less than 8% and 10%, respectively. Serum levels of GPC3 were significantly higher in patients with HCC (median, 0 ng/mL, range = 0-14.0 ng/ml; P = .033) and cirrhosis (median, 0 ng/mL; range = 0-12.5 ng/mL; P = .001) compared with NCs (median, 0 ng/mL; range = 0-4.3 ng/mL), but there was no difference between HCC and cirrhosis. Serum levels of GPC3 were significantly lower in patients with AH (median, 0 ng/mL; range = 0-0 ng/mL; P = .032) than in NCs (Table 3, Figure 1B). However, there was no significant difference in serum GPC3 levels between patients with CHB (median, 0 ng/mL; range = 0-1.7 ng/mL) and NCs (P = .159).

A, Standard curve of sandwich ELISA for GPC3. B, Comparative analysis of serum GPC3 levels in HCC and controls. ELISA indicates enzyme-linked immunosorbent assay; GPC3, Glypican-3; HCC, hepatocellular carcinoma.
Comparative Analysis of Serum GPC3 and AFP Levels for HCC Diagnosis.
Abbreviations: AFP, α-fetoprotein; AH, atypical hyperplasia; CHB, chronic hepatitis B; F, female; GPC3, glypican-3; HCC, hepatocellular carcinoma; LC, liver cirrhosis; M, male; NC, normal control.
a P < .05, compared with the NC group. The cutoff value for AFP was 20 ng/mL.
The ROC curve analysis was performed to assess the diagnostic value of HCC versus LC, benign liver disease (BLD, AH + LC + CHB), NC, and all controls. The AUC values of the ROCs for HCC versus LC, HCC versus BLD, and HCC versus NC were 0.463, 0.515, and 0.552, respectively (Figure 2). The ROC shows that the optimum diagnostic cutoff value of GPC3 for HCC versus all controls was 0.002 ng/mL (AUC 0.519, 95% CI: 0.472-0.555). The sensitivity, specificity, positive, and negative predictive values of GPC3 were 39.9%, 60.6%, 32.0%, and 68.3%, respectively. The AUC of the ROC curve, sensitivity, and specificity were all significant low, suggesting that the diagnostic value of serum GPC3 for HCC is low. Therefore, in the present study, GPC3 was not a promising serological maker for the diagnosis of HCC.

The ROC curve analysis: the diagnosis of serum GPC3 for HCC versus LC (A), HCC versus BLD (B), HCC versus NC (C), and HCC versus all controls (D). The AU-ROC was 0.463, 0.515, 0.552, and 0.519, respectively. AU-ROC indicates area under the receiver operating curve; BLD, benign liver disease; GPC3, Glypican-3; HCC, hepatocellular carcinoma; LC, liver cirrhosis; NC, normal control.
In addition, we further analyzed the relationship between serum levels of AFP and GPC3 in patients with HCC. The level of AFP was elevated in 57.2% (162 of the 283) of the patients with HCC. There was no significant correlation between serum levels of AFP and GPC3 (P > .05). As shown in Table 4, 44 patients had an elevated level of GPC3 among the 121 patients who were negative for AFP, which indicated that serum GPC3 may be complementary to AFP for the diagnosis of HCC. The diagnostic sensitivity for HCC was elevated (72.8%, 206 of the 283) when GPC3 was combined with AFP. There was no statistical association between serum GPC3 and age, gender, HBV infection, Child-Pugh score, AFP level, number of tumors, or tumor size (Table 1).
Detection of GPC3 and AFP in the Serum of Patients With HCC.a

Abbreviations: AFP, α-fetoprotein; GPC3, glypican-3; HCC, hepatocellular carcinoma.
aThe cutoff value for AFP was 20 ng/mL.
Discussion
In the present large-scale study, we recruited consecutive patients with either HCC or a chronic hepatic disease and NCs to assess the diagnostic value of serum GPC3 for HCC. We found that the levels of GPC3 in serum were significantly higher in patients with HCC than in NCs, which indicated that serum GPC3 was able to distinguish patients with HCC from NCs. There was no difference in the levels of serum GPC3 between patients with CHB and NCs, and we failed to detect serum GPC3 in patients with AH. Despite being limited by the small number of such patients, additional studies with large samples of patients with AH are needed to assess the serum GPC3 level in patients with AH. However, we also observed a significant elevation in serum GPC3 in patients with cirrhosis compared to NCs. Moreover, no difference was observed in serum GPC3 levels between patients with HCC and cirrhosis. In addition, the sensitivity and specificity of GPC3 for HCC was only 39.9% and 60.6%, respectively. The AUC values from the ROC curves for HCC versus NC and all controls were only 0.553 and 0.519, respectively, suggesting no clinical diagnostic value of serum GPC3 for HCC. All of these results indicated that serum GPC3 was not a promising serological maker for the diagnosis of HCC, especially for those patients with a history of cirrhosis.
Similarly, several previous studies also obtained results indicating poor diagnostic value of GPC3 for HCC as in the present study. Nakatsura et al reported that serum GPC3 was detected in 40% (16 of 40) of patients with HCC and only in 50% (7 of 14) of patients with HCC having GPC3-positive tumor tissue. 17 In another study, Liu et al found the sensitivity of serum GPC3 for the diagnosis of HCC was 46.7% (35 of 75). 18 In the study of Yao et al, serum GPC3 could be detected in only 52.8% (65 of 123) of patients with HCC. 19 Yu et al reported that serum GPC3 was elevated in 42.5% (17 of 40) of patients with HCC, and tissue GPC3 was positive in all 40 patients with HCC. 20 Beal et al detected serum GPC3 levels in patients with HCC and cirrhosis, also to find that serum GPC3 had no role in HCC surveillance. 21 The sensitivity and specificity of serum GPC3 in these studies were close to those in this study. Collectively, the previous studies and our results confirm the poor sensitivity of GPC3 for diagnosing HCC, suggesting no clinical diagnostic value of serum GPC3 for HCC. Thus, it is possible that the proportion of GPC3 positivity is lower in serum than in tumor tissues in patients with HCC. Glypican-3 is a member of the heparan sulfate proteoglycans, and its C-terminal region binds to the cell membrane via glycosylphosphatidylinositol anchors. Therefore, the existence of a secreted type of GPC3 was predicted, which would allow detection of GPC3 in the serum of patients with HCC. Additionally, ELISA detected the secreted type of GPC3 in serum. There might be a significant discrepancy between expression and secretion for GPC3 protein. It might be reasonable that the positive rate of serum GPC3 was only 39.9% in HCC in this study, but many studies have reported high expression of GPC3 in HCC tissues. 22 –24 Possibly being limited by the number of participants, we failed to detect GPC3 in patients with AH.
Furthermore, we also observed an elevation in serum GPC3 in cirrhosis, chronic hepatitis, and even NCs. In several studies, the investigators have confirmed these results. 13,18,21,25,26 In a study, Yasuda et al even found the levels of serum GPC3 were higher in chronic liver disease than in HCC. 13 Özakan et al also observed high levels of serum GPC3 in cirrhosis (median: 5.51 pg/mL) compared with HCC (median: 5.13 pg/mL). 14 Meaningfully, Chen et al found that 5 of 7 GPC3-positive HCC cases had an elevated level of serum GPC3 12 months before their HCC diagnosis. 27 Thus, they assumed that the elevation of GPC3 was at the early stage of liver carcinogenesis or that GPC3 could be produced by nonmalignant or promalignant liver cells. In addition, several recent studies have confirmed the expression of GPC3 in regenerative nodules, hepatitis C samples, and even in normal liver tissues. 28 –30 It might be reasonable that we found elevated serum GPC3 in 50.6% (135 of the 267) of patients with cirrhosis, 30.2% (49 of the 162) of patients with chronic hepatitis, and 30.9% (50 of the 162) of NCs. Whether nontumor cells can express GPC3 protein and whether patients with chronic liver disease and NCs have elevated serum GPC3 need further investigation.
At present, serum AFP is most commonly used for the diagnosis of HCC. However, the sensitivity of AFP is only 25% to 65%, suggesting that approximately 40% of patients with HCC may be false negatives. In this study, serum GPC3 levels had no correlation with AFP, and it was elevated in 36.4% (44 of the 121) of patients who were negative for AFP. Thus, serum GPC3 may be complementary to AFP for the diagnosis of HCC. In this study, we indeed observed an elevation in diagnostic sensitivity (72.8%) when GPC3 was combined with AFP, and several previous studies also clearly stated that GPC3 could be complementary to AFP and provide elevated sensitivity for the diagnosis of HCC. 8,18 –20
In this study, the clinical characteristics of patients with HCC, including HBV infection, Child-Pugh score, number of tumors, tumor size, tumor stage, and portal vein invasion, were also evaluated. No statistical association was observed between serum GPC3 and these clinical characteristics, which indicated no prognostic value of serum GPC3 for HCC.
Conclusion
In conclusion, the levels of serum GPC3 were elevated in patients with HCC compared with NCs. We failed to find the clinical utility of GPC3 as a serum marker for the diagnosis of HCC, especially for patients with a history of cirrhosis. There was also no correlation between GPC3 levels and prognostic parameters. Glypican 3 was not a promising serum maker for the diagnosis of HCC alone, but it could be used as a complement to AFP to elevate the sensitivity of HCC diagnosis.
Footnotes
Acknowledgments
The authors thank the whole nursing staff of the Medical Examination Center of Tianjin Third Central Hospital for their efficient cooperation in blood sample and data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the Key Research Project of Tianjin Healthy Bureau (11KG112).