
Abstract
Prostate cancer is the most common non-cutaneous cancer in males. There are a number of options for patients with localized early stage disease, including active surveillance for low-risk disease, surgery, brachytherapy, and external beam radiotherapy. Increasingly, external beam radiotherapy, in the form of dose-escalated and moderately hypofractionated regimens, is being utilized in prostate cancer, with randomized evidence to support their use. Stereotactic body radiotherapy, which is a form of extreme hypofractionation, delivered with high precision and conformality typically over 1 to 5 fractions, offers a more contemporary approach with several advantages including being non-invasive, cost-effective, convenient for patients, and potentially improving patient access. In fact, one study has estimated that if half of the patients currently eligible for conventional fractionated radiotherapy in the United States were treated instead with stereotactic body radiotherapy, this would result in a total cost savings of US$250 million per year. There is also a strong radiobiological rationale to support its use, with prostate cancer believed to have a low α/β ratio and therefore being preferentially sensitive to larger fraction sizes. To date, there are no published randomized trials reporting on the comparative efficacy of stereotactic body radiotherapy compared to alternative treatment modalities, although multiple randomized trials are currently accruing. Yet, early results from the randomized phase III study of HYPOfractionated RadioTherapy of intermediate risk localized Prostate Cancer (HYPO-RT-PC) trial, as well as multiple single-arm phase I/II trials, indicate low rates of late adverse effects with this approach. In patients with low- to intermediate-risk disease, excellent biochemical relapse-free survival outcomes have been reported, albeit with relatively short median follow-up times. These promising early results, coupled with the enormous potential cost savings and implications for resource availability, suggest that stereotactic body radiotherapy will take center stage in the treatment of prostate cancer in the years to come.
Introduction
As of 2016, more than 3.3 million men are living with prostate cancer in the United States 1 with more than 180 000 new cases diagnosed each year, of whom 92% present with localized disease. Conventional curative treatment options for localized disease include radical prostatectomy, external beam radiotherapy (EBRT), and brachytherapy. Stereotactic body radiotherapy (SBRT) is an emerging treatment option which allows for extreme hypofractionation using modern technologies. This review will outline the efficacy and toxicity outcomes of SBRT and highlight specific issues and controversies surrounding patient selection, treatment planning and delivery, use of androgen deprivation therapy (ADT), and follow-up. The review will conclude by highlighting currently accruing studies and areas for future research.
Rationale for High Dose per Fraction Radiotherapy
Extreme hypofractionation using SBRT for prostate cancer may have radiobiological advantages compared to conventionally fractionated external beam radiotherapy (CFRT). The relatively low α/β ratio of prostate cancer, estimated to be between 1 and 2 Gy, may confer sensitivity to high dose per fraction. 2 -5 In addition, the α/β ratio of prostate cancer may be lower than surrounding organs at risk (OARs), including the rectum and bladder, thereby allowing hypofractionation to improve the therapeutic ratio and deliver similar rates of efficacy with the same or lower rates of complication than conventional fractionation. 3,5 Randomized evidence suggests that dose-escalated CFRT is associated with improvement in biochemical and disease-specific outcomes. 6 -11 Furthermore, medium-term results from recent randomized studies have shown moderately hypofractionated regimens of 2.5 to 3 Gy to be noninferior to CFRT with respect to biochemical control without a detriment to toxicity and have led to the adoption of moderately hypofractionated radiotherapy at treatment centers worldwide. 12 -14 It is important to note, however, that neither use of dose escalation nor hypofractionation has a demonstrated overall survival advantage, and therefore, management of associated toxicities with these approaches is critical.
It is believed that SBRT-induced tumor cell kill may also be mediated through different pathways compared to CFRT. The tumor microenvironment, and specifically the tumor vasculature, may be a significant factor in the effectiveness of SBRT. The endothelial acid sphingomyelinase pathway generates proapoptotic second messenger ceramide, which induces apoptosis of endothelial cells, microvascular dysfunction, and secondary tumor cell death. 15 This pathway appears to be generated in a dose-dependent manner, particularly with doses greater than 8 Gy per fraction. 16 The role of ceramide is further supported by clinical studies which showed elevation in serum ceramide levels following SBRT is correlated with tumor response, suggesting both its mechanistic role in cell kill and its potential future role as a biomarker. 17,18
In addition to radiobiological considerations, SBRT has practical advantages over surgery, CFRT, and brachytherapy, including being noninvasive, time efficient, and cost-effective, potentially resulting in improved access and greater patient satisfaction. 19,20 Although cost arguments in one country may not readily translate to others, there are a number of studies from different countries that aim to quantify the cost benefit of SBRT. A Canadian cost–utility study compared SBRT to low dose rate (LDR) brachytherapy and CFRT for a 66-year-old with low-risk prostate cancer followed annually. 21 The study found that SBRT and LDR were more cost-effective, with SBRT being Can$5266 less expensive and delivering 0.53 higher quality-adjusted life years compared to CFRT. A similar American study also showed cost savings with SBRT compared to CFRT, with a calculated savings of US$13 279 per patient. 20 The same study estimated that if half of the patients currently eligible for CFRT were to be treated instead with SBRT, this would result in a total cost savings of US$250 million per year. The impact of radiotherapy planning and delivery techniques was further investigated in a study that found arc-based SBRT (Can$4368) to be the least expensive and fixed gantry-based CFRT the most expensive (Can$7992) of EBRT techniques to treat prostate cancer. 22 Meanwhile, CFRT with protons has been shown to be over 2.5 times more expensive than SBRT assuming equal effectiveness of therapies. 23 Cost savings with SBRT compared to CFRT are also realized at a patient level, with an average of Can$5517 saved per patient for costs related to time off work, transport, and parking. 24 Cost and time saved for patients are an important consideration, with length of CFRT treatment being cited as one of the most frequent dislikes among patients receiving prostate cancer treatment. 25
Clinical Outcomes—Efficacy, Toxicity, and Quality of Life
There are multiple published prospective single-arm series investigating the use of SBRT (see Table 1). The largest is a multi-institutional report on 1100 patients (641 low, 334 intermediate, and 125 high risk) with clinically localized prostate cancer enrolled in separate phase II trials from 8 institutions between 2003 and 2011. 26 Patients were treated using CyberKnife (Accuray, Sunnyvale, California) to a dose of 35 to 40 Gy in 4 to 5 fractions, with dose normalized to the 90% isodose line, such that the prescription dose covered at least 95% of the planning target volume (PTV). With a median follow-up of 36 months, the 5-year biochemical relapse-free survival (bRFS) defined as nadir + 2 ng/mL was 95%, 84%, and 81% for low-, intermediate-, and high-risk prostate cancer, respectively. No correlation was shown with the total dose delivered or use of ADT. Updated results of this series were presented recently in abstract form for 1644 patients (892 low and 752 intermediate risk), with a median follow-up of 7.2 years. 27 The 5-year and 10-year bRFS rates were 98% and 94% in the low-risk and 96% and 90% in the intermediate-risk group, respectively. The severe acute toxicity rate was only 0.2% (5 patients with grade 3 genitourinary [GU] toxicity). Thirty (2%) patients experienced a late grade 3 GU toxicity (including urinary strictures, hematuria, and retention) and 1 patient a late grade 4 GU toxicity (hemorrhagic urethritis). One patient had a late grade 4 gastrointestinal (GI) toxicity (fistula-in-ano). A subset of these patients (n = 864) also had complete quality of life (QOL) data collected. 28 Using the Expanded Prostate Cancer Index Composite (EPIC), 29 the authors reported mean baseline urinary, bowel, and sexual domain scores of 89, 95, and 53, which worsened to 81, 83, and 48 at 3 months posttreatment. Patients subsequently showed recovery at 6 months in the urinary and bowel domains, with recovery to baseline scores of 91 and 96, respectively, at 5 years. However, sexual function continually declined posttreatment.
Prospective Trials of Prostate Stereotactic Body Radiotherapy With At Least 3-Year Follow-Up.a

Abbreviations: CTC, Common Toxicity Criteria; CTCAE, Common Terminology Criteria for Adverse Events; CTV, clinical target volume; H, high risk; I, intermediate risk; L, low risk; NR, not reported; PTV, planning target volume; RTOG, Radiation Therapy Oncology Group.
a Studies with overlapping patient cohorts.
The largest single-institution series published by Katz et al is from Flushing, New York, with patients from this series also included in the above pooled analysis. 30 There were a total of 324 low-, 153 intermediate-, and 38 high-risk patients included with the 8-year bRFS being 94%, 84%, and 65%, respectively. An updated 10-year analysis of 230 low-risk patients showed 93% bRFS. 31 There was no difference in efficacy seen between 35 and 36.25 Gy. Toxicity was retrospectively reported in a cohort of 477 low- and intermediate-risk patients, with 1.7% of patients experiencing Radiation Therapy Oncology Group late grade 3 to 4 GU toxicity, comprising of retention requiring surgery and bleeding requiring laser coagulation. 32 Both these patients received 36.25 Gy. No severe late GI toxicities were seen; however, this may have been underreported, given it was collected retrospectively. Outcomes appear to be broadly similar across CyberKnife series, including results presented by Meier et al of the largest multi-institutional series 33 and by Tree et al of the first United Kingdom series, which found 2 patients with grade 3 toxicity during radiotherapy, however none following treatment, suggesting that acute toxicities may peak earlier than that captured on studies recording toxicity first at 1 month post-SBRT. 34
Outcomes are similar between CyberKnife and gantry-based platforms. The largest gantry-based series comprised of low-risk patients with cancer treated to 35 Gy in 5 fractions delivered to the clinical target volume (CTV; with 99% of CTV receiving the prescription dose), with an excellent 5-year bRFS of 98% and with 1% rate of late severe GU (temporary catheterization in patient with 300 cm3 bladder diverticulum) and GI toxicity (anal fistula in patient with background diverticulitis). 35
The efficacy and toxicity outcomes in the above larger studies are similar to results published by smaller series. In general, the results show excellent 5-year bRFS rates of 95% or greater for low-risk disease. The reported toxicities are also low, with late grade 3 GU and GI toxicities usually less than 2%. The main exception to this was seen in a dose escalation study of up to 50 Gy in 5 fractions (see Table 2 for biological equivalent dose calculations), which reported a 7% and 6% rate of Common Terminology Criteria for Adverse Events (CTCAE) v.3.0 late ≥ grade 3 GI and GU toxicity, respectively, including grade 4 cystitis requiring ureteroileal diversion, grade 4 rectal bleeding requiring intensive care admission, and 6 patients who required a colostomy. 36 Analysis of rectal dosimetry revealed that patients on this study were significantly more likely to develop late rectal toxicity if the rectal wall received V50 Gy >3 cm3, >35% of the rectal wall circumference received 39 Gy, and >50% of the rectal wall circumference received 24 Gy. Quality of life data also appear consistent across the literature with initial deterioration over the first few months in urinary and bowel domains, followed by subsequent recovery to baseline over the next 6 to 12 months. 37,38 Sexual function, however, usually declined post-SBRT without recovery. 28,38
Doses for Prostate Stereotactic Body Radiotherapy.
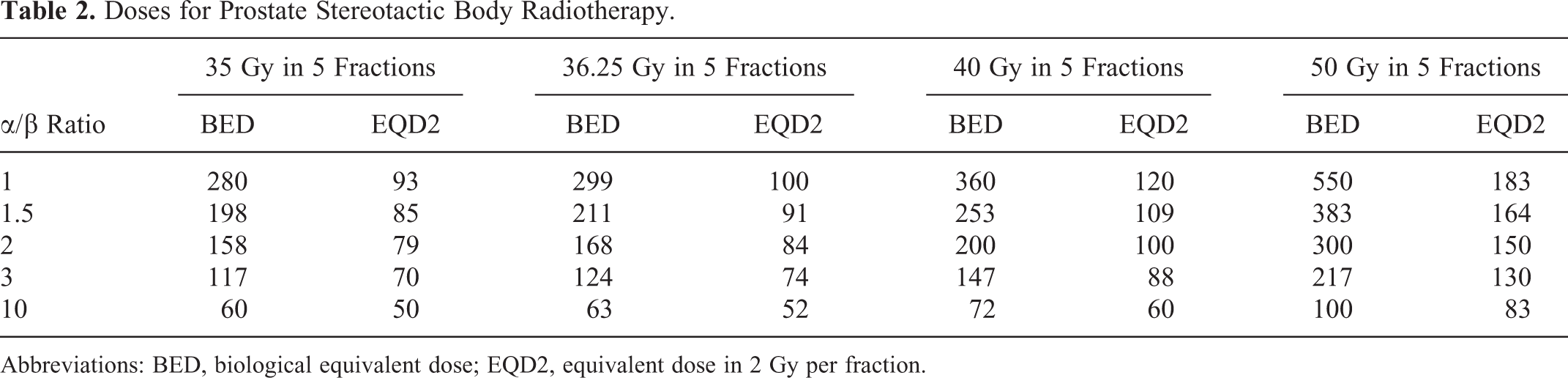
Abbreviations: BED, biological equivalent dose; EQD2, equivalent dose in 2 Gy per fraction.
Which Patients Benefit From SBRT?
As yet, there is only one randomized study comparing SBRT to an alternative treatment modality, the Phase III study of HYPOfractionated RadioTherapy of intermediate risk localized Prostate Cancer (HYPO-RT-PC) trial (see Table 1). 39 This trial compared CFRT (78 Gy in 39 fractions) to extreme hypofractionation (42.7 Gy in 7 fractions, with an equivalent dose in 2 Gy per fraction [EQD2] of 78 Gy for α/β = 3) in 1200 intermediate-risk patients. Radiotherapy was delivered to the prostate alone. A 7-mm CTV to PTV margin was used. Image guidance with fiducial markers was employed. Median follow-up time was 4.2 years. Acute ≥ grade 2 GI toxicity was slightly higher in the SBRT arm (9.4% vs 5.3%, P = .023); however, GU toxicity was similar (27.6% vs 22.8%, P = .11). At 2 years, there was no difference in physician reported ≥ grade 2 GI (2.2 vs 3.7%, P = .20), or GU (5.4% vs 4.6%, P = .59) toxicity, or rates of impotence (34% in both arms). Patient-reported outcome measurement (PROM) data revealed significantly worse acute bowel toxicity in 7 of 10 items in the SBRT arm; however, the difference disappeared at 3 months. Urinary function PROM scores at 1 year were worse in 4 of 10 items in the SBRT arm. Efficacy results are awaited as the data mature.
Another study compared QOL outcomes between 2 sequential phase II studies, with the first study utilizing SBRT to 35 Gy in 5 fractions over 5 weeks and the second 15 Gy high dose rate (HDR) brachytherapy followed by EBRT to 37.5 Gy in 15 fractions. 49 This study revealed significant differences between the 2 studies in EPIC urinary (P < .0001), bowel (P = .0216), and sexual (P = .0419) domain scores, favoring SBRT.
In lieu of randomized efficacy evidence, some centers have compared SBRT to alternative radiotherapy techniques using propensity score-matched analyses, including a Canadian study of 602 low-risk patients, which showed superior bRFS with SBRT compared to CFRT, while bRFS was similar between SBRT and LDR brachytherapy. 50 An American study similarly found, on a propensity score-matched analysis of 263 patients with nonmetastatic prostate cancer, no difference in 5-year freedom from biochemical failure (FFBF) or toxicity between SBRT and CFRT (90% vs 90%, P = .644). 51 A retrospective multi-institutional analysis that compared the outcomes of patients who received either SBRT or HDR brachytherapy as monotherapy for 437 intermediate-risk patients found a bRFS of 96.3% with no significant difference according to treatment type. 52 Overall, survival for SBRT also appears comparable to other treatment modalities, with an analysis of 5430 patients with localized prostate cancer on the US National Cancer Database revealing no difference in overall survival between patients treated with SBRT or CFRT. 53 Another study looking at the comparative effectiveness of various prostate cancer treatment using previously published data suggested that while both HDR and SBRT showed promising results, the available data for these modalities were not as robust as for CFRT as yet. 54
Overall, the above results suggest that SBRT may be an equally effective and safe treatment option compared to alternative radiotherapy modalities for patients with low- and intermediate-risk prostate cancer. We eagerly anticipate results from forthcoming randomized studies, which will allow us not only to better select between radiotherapy options but also to better counsel our patients between radiotherapy and surgery.
Finding the Right Dose
While a spectrum of total doses and fraction sizes are reported in the SBRT literature, most common doses in the order of 35 to 36.25 Gy in 5 fractions delivered to the PTV are employed based upon the isolate-effects principle, which results in an EQD2 of 70 Gy for late effects (α/β = 3 Gy) and 85 Gy for tumor effects (α/β = 1.5 Gy; see Table 2). Yet, there are no published randomized studies assessing the efficacy of SBRT dose escalation. The majority of prospective studies comparing dose regimens are limited by confounding factors including differences in patient population, inconsistent use of ADT, and relatively short follow-up periods, with variable results for efficacy. One report comparing doses used in 2 prospective Canadian trials employing 35 Gy (Prostate Hypofractionated Accelerated RadioTherapy [pHART] 3) and 40 Gy (pHART6) in 5 fractions found no significant difference in 4-year bRFS (98.7% vs 100% respectively, P = .19). 44 Interestingly, 40 Gy was significantly associated with a lower median prostate-specific antigen (PSA) at 3 years on multivariate analysis, suggesting that potentially with longer follow up, a difference in a bRFS may be seen. 55 Supporting this finding is a phase I dose escalation study presented at the 2017 American Society for Radiation Oncology (ASTRO) annual meeting of 136 patients comparing 4 dose levels of 32.5, 35, 37, and 40 Gy in 5 fractions. 41 This study showed improved 3-year bRFS with higher doses (83%, 85%, 90%, and 98% respectively, P < .001) and lower rates of positive posttreatment biopsies (45%, 12%, 17%, 5% respectively, P < .001), with low rates of severe late toxicity (no ≥ grade 3 rectal and 1 late grade 3 urinary toxicity). Further dose escalation of 50 Gy in 5 fractions was studied within a multi-institutional phase I/II trial of 91 low- and intermediate-risk patients treated with SBRT to 45 Gy (n = 15), 47.5 Gy (n = 15), and 50 Gy (n = 61). 36 There was only 1 biochemical failure at 5-year follow-up of a patient treated to 45 Gy in this study; however, the late toxicity rates were unacceptably high as previously discussed. 56
Most recently, a randomized phase II study of 30 patients, published in abstract form only, reported on the use of single-fraction radiotherapy in prostate cancer, comparing 24 Gy in a single fraction to 45 Gy in 5 daily fractions. 57 The end points reported were 3-month acute treatment-related toxicity and patient-reported QOL. The early results were promising with no ≥ acute grade 2 toxicity, although there were higher grade 1 GU and GI toxicities in the single fraction compared to the 5 fraction arm (GU 41% vs 18% and GI 8% vs 0%). Quality of life results revealed no difference in mean EPIC scores between the 2 arms, with both arms finding a decrease in 1-month urinary scores to 6% and 8%, which recovered to baseline at 3 months, with a similar trend seen in International Prostate Symptom Score (IPSS). Importantly, this study utilized volumetric-modulated arc therapy and image-guided radiotherapy techniques, with urethral sparing, real-time motion management, a Foley catheter loaded with beacon transponders, and insertion of an endorectal balloon filled with 150 cc air to induce temporary ischemia of the anterior rectal tissues. Although this study provides an intriguing look into a future when SBRT can be delivered in a single fraction, small patient numbers and short follow-up limit interpretation of this study, with greater patient numbers and longer-term data needed to better assess its efficacy and potential risks of late toxicity. Another single-arm phase I/II trial (NCT03294889) assessing single-fraction SBRT to 19 Gy to the prostate with or without the proximal seminal vesicles is currently accruing and aiming to recruit 45 participants to assess toxicity and 3-year bRFS.
An alternative option to escalate the dose delivered to the prostate is to combine CFRT with a SBRT boost. One study from Georgetown University included 59 high-, 45 intermediate-, and 4 low-risk patients treated with SBRT to 19.5 Gy in 3 fractions followed by EBRT to the prostate, proximal seminal vesicles, and areas of extra-prostatic extension using a 1-cm CTV to PTV margin to a dose of 45 to 50 Gy in 25 to 28 fractions. 58 The 3-year FFBF in this study appeared promising, being 100% for intermediate and 90% for high-risk patients, although noting that 64% of patients received ADT prior to RT. There was a statistically significant deterioration in EPIC GU and GI QOL scores at 1 month, which subsequently improved, although not to baseline, at 24 months, with 13.7% and 5% of men reporting their urinary or bowel function, respectively, to be a “moderate to big problem” at this point.
In addition to total dose and dose per fraction, there is considerable variation applied to the scheduling of treatment within studies. Although no studies to our knowledge have reported improvement in SBRT efficacy with variation in overall treatment time, a prospective study of 67 patients with a median follow-up of 2.7 years suggested that alternate day compared to consecutive day treatment resulted in favorable late grade 1 to 2 GI (5% vs 44%, P = .001) and GU (17% vs 56%, P = .007) toxicities. 59 There was no difference in higher grade toxicities seen. This is supported by the results of the Prostate Accurately Targeted Radiotherapy Investigation of Overall Treatment Time study, which is a Canadian phase II trial with results in press, randomizing 152 patients to 40 Gy in 5 fractions delivered either weekly or on alternate days. 40,60 With a median follow-up of 47 months, this study showed improved acute urinary (78% vs 94%, P = .006) and bowel (68% vs 90%, P = .002) QOL (as defined by the proportion of patients who had a >0.5 standard deviation decline in EPIC scores) in patients undergoing weekly compared to alternate day treatment. There was no significant difference in late urinary or bowel toxicity at 2 years. A similar ongoing study in Europe has randomized 170 patients to alternate day versus weekly SBRT to 36.25 Gy in 5 fractions (NCT01764646), and results are awaited.
Treatment Volume—Prostate, Pelvis, and/or Dominant Nodule
A majority of the studies assessing the role of SBRT in prostate cancer have limited the radiotherapy volume to the prostate alone, without treating the pelvis (see Figure 1). Some studies, however, have used SBRT as a boost to CFRT. This is modeled on studies using brachytherapy as a form of dose escalation, the use of which was supported by the randomized Androgen Suppression Combined with Elective Nodal and Dose Escalated Radiation Therapy trial which combined EBRT with brachytherapy and showed a halving of biochemical failure compared to EBRT alone to a dose of 78 Gy. 61 Most of the SBRT boost series are retrospective and have assessed predominantly intermediate- and high-risk patients and show FFBF rates of between 77% and 100% with low rates of severe toxicities. 62 -66
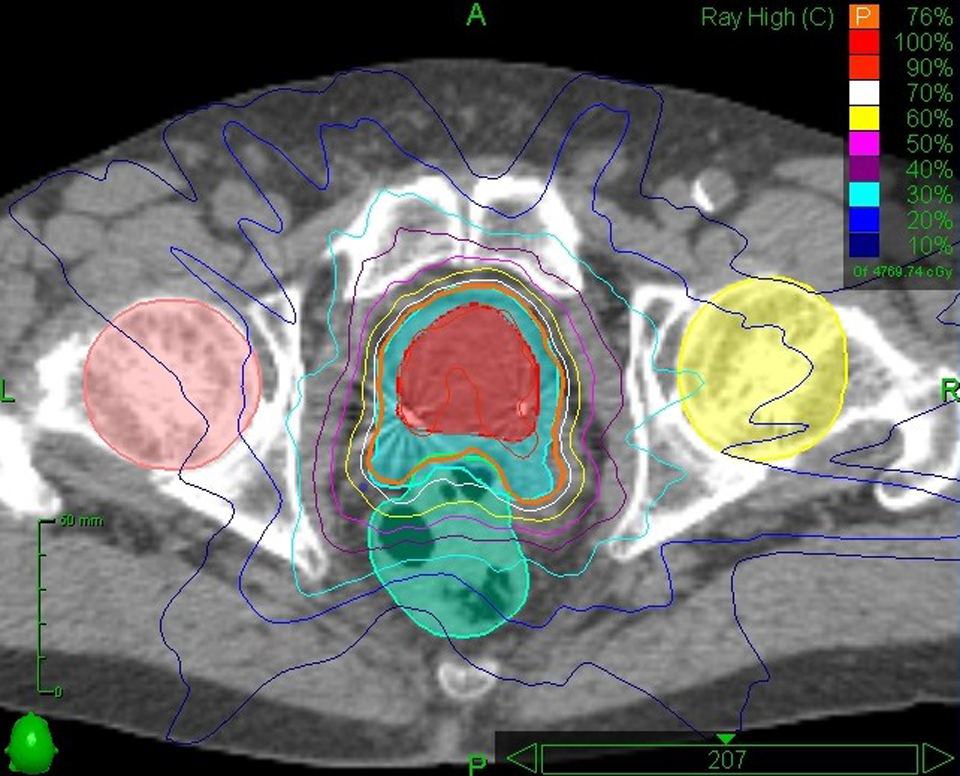
CyberKnife plan to 36.25 Gy in 5 fractions.
Meanwhile, a comparison of high-risk patients treated within a prospective study with SBRT monotherapy (35-36.25 Gy in 5 fractions) or CFRT (45 Gy in 25 fractions to prostate and nodes) followed by SBRT boost (18-21 Gy in 3 fractions) did not show an improvement in bRFS with the addition of pelvic EBRT (P = .86) and found worse late rectal toxicity (grade 2 GI toxicity 0% vs 13%, respectively, P = .002). 63
Another approach to treatment of the pelvis is with SBRT, with a boost to the prostate (see Figure 2). Two studies that assessed this approach were the SABR Including Regional Lymph Node Irradiation for Patients With High Risk Prostate Cancer (SATURN) and Fairly brief Androgen suppression and StereoTactic Radiotherapy for high risk prostate cancer (FASTR) studies. 67 -69 In both studies, patients received 25 Gy in 5 weekly fractions, with a hypofractionated simultaneous integrated boost (SIB) to the prostate and seminal vesicles to 40 Gy. Combined early toxicity results from the studies revealed, in particular, a high rate of rectal toxicity, with 12 out of 45 patients experiencing rectal bleeding. Rectal bleeding was more frequent and of higher grade in patients in the FASTR (8/15 including 5 patients with grade 2 toxicities) compared to the SATURN trial (4 of 30, all grade 1 toxicities). This was thought to be due to inclusion of seminal vesicles in the CTV and larger 5 mm PTV expansions in the FASTR study, as well as differences in PTV planning (FASTR used D95 ≥40 Gy, whereas SATURN used D95 ≥33.25 Gy) and rectal constraints (FASTR used D50 ≤29 Gy whereas SATURN used D50 ≤20 Gy). In particular, the V20 Gy was significantly higher in patients with ≥ grade 2 bleeding (68% vs 40%, P < .001) and V40 Gy was significantly higher in patients with any grade bleeding (1.53% vs 0.69%, P = .006).

Stereotactic body radiotherapy to the pelvis.
A phase I/II study has also assessed the use of SBRT to the pelvis to 25 Gy in 5 weekly fractions, following the initial use of HDR brachytherapy to 15 Gy in a single fraction to the prostate, with up to 22.5 Gy to a magnetic resonance imaging (MRI) identified nodule. 70 Early results with a median follow-up of 13.8 months revealed 45% acute CTCAE v3.0 grade 2 GU and 10% grade 2 GI toxicities. There were also 3 acute grade 3 toxicities, all necessitating urinary catheterization in the immediate post-HDR period, and no grade 3 late toxicities. Mature data for this study are still pending.
Identification and treatment of an MRI-detected dominant intraprostatic lesion using brachytherapy or other focal modalities has been extensively reported 71 and is now also being studied using SBRT. One study reported in abstract form treated 10 low- to intermediate-risk patients to 40 Gy in 5 fractions to the whole prostate with an SIB to MRI detected lesions to 42.5 to 45 Gy in 5 fractions, while treating another 6 patients who were unable to have MRI to 37.5 Gy in 5 fractions without a SIB. 72 Early results with a median follow-up of 8 months showed no grade 3 or 4 acute or late toxicities and a small deterioration in IPSS from 8.2 to 10.4 at 6 weeks (P = .02). The trial continues to collect follow-up data on toxicity and tumor control, and we await long-term results to assess whether this may be a safe and effective method of dose escalation.
Technical Considerations—Treatment Planning and Delivery
Target delineation is critical to the use of SBRT. The CTV typically incorporates the prostate, with or without the proximal seminal vesicles and areas of extracapsular extension. Increasingly, image fusion of MRI sequences is being incorporated into practice. 73 Previous studies have shown significant variation exists in prostate contouring, emphasizing the need for adequate quality assurance. 74,75 Incorporation of MRI images reduces interobserver variation in target delineation compared to computed tomography images alone. 76 Contouring guidelines, such as the recently published European Society for Radiotherapy and Oncology guidelines, aims to standardize the definitions for target volumes and OAR and may also help to improve consistency. 77 Planning target volume expansions are typically 3 to 5 mm, with tighter constraints posteriorly to spare the rectum. The dose is often prescribed to the 90% isodose (may range between 75% and 90%), with the aim of the prescription dose covering at least 95% of the PTV, although other centers aim for the prescription dose to cover at least 99% of the CTV. An example of OAR dose constraints being used for the currently accruing international Prostate Advanced in Comparative Evidence (PACE) trial is given in Table 3. 78 In particular, maintaining a rectal D1 cc <35 Gy and penile bulb V35 Gy <4% (using 5 fraction regimen) has been shown to be critical and independently predictive of decline in bowel QOL scores. 79
PACE Dose Constraints. 78

Abbreviations: PACE, prostate advanced in comparative evidence; V, volume.
The majority of the literature published to date has incorporated the use of CyberKnife to deliver SBRT, although more recent series have used gantry-based linacs with similar outcomes. 35,80 The main technical challenge in delivery of SBRT to the prostate is management of inter- and intrafraction motion of the prostate gland, which can depend on continuous rectal and bladder filling, even while the beam is on. Image guidance systems are key to allowing safe delivery of SBRT, with real-time motion tracking systems incorporating the use of 3 to 4 fiducial markers commonly employed. More recently, the introduction of real-time MRI images during treatment delivery allows for continuous intrafractional tracking of the target and may result in improved toxicity profiles and allow for even further dose escalation. 81 Another method currently under investigation is the use of kilovoltage intrafraction monitoring (KIM), which also offers a real-time automated image guidance system by using periodic X-rays of fiducial markers while the beam is on to facilitate corrections with alignment, or even tracking with multileaf collimators during treatment. 82 There are additional strategies to control for bowel and bladder size including prescription of a strict diet, bowel regimen, and/or laxatives, 38,45,83,84 bladder catheterization, 45 or bladder emptying followed by a specified consistent intake of water. 35 The rectum is of particular concern as not only an organ that contributes to target motion but also as a critical OAR. Some institutions have used endorectal balloons to immobilize the prostate, 84 whereas others have employed SpaceOAR hydrogel spacers to push the rectum away from the prostate (Augmenix Inc, Waltham, Massachusetts). 85
Use of ADT
For many years, ADT has been commonly used in addition to radiotherapy. 86 Although the addition of ADT to CFRT has been shown to improve overall survival in intermediate- and high-risk patients, 87 -89 there are limited data in the dose escalated and SBRT setting. In the pooled analysis of 1100 patients, there was no predefined criteria on the use of ADT, with only 147 patients undergoing endocrine therapy and no difference in 5-year FFBF (93% with ADT vs 91% without ADT, P = .71). 26 The relatively poorer efficacy of SBRT for high-risk patients, however, may prove to be an area in which additional treatment modalities such as ADT may play a role. Further research in this area is required.
Follow-Up
Prostate-specific antigen kinetics following SBRT tend to show lower PSA nadirs (nPSA) compared to CFRT, but comparable or slightly higher than brachytherapy, 50,90 with nPSA levels typically approximating 0.2 ng/mL with a trend for lower nPSA levels with higher biological doses. 26 The nPSA tends to be lower and PSA slopes larger following SBRT compared to CFRT, with the difference becoming evident particularly 2 to 3 years following treatment, with the PSA continuing to fall with SBRT and plateauing for CFRT. 90,91 Time to nPSA, therefore, is usually longer with SBRT, with 1 series showing a median time to nPSA of 7.8 and 5.9 years for doses of 35 and 40 Gy in 5 fractions, respectively. 42,43 Compared to brachytherapy, however, SBRT produces similar or higher nPSA levels. 50,90 Benign PSA bounce is also a phenomenon which is reported at varying rates within the literature between 16% and 44%, with a median bounce height of approximately 0.5 ng/mL, and at a median time between 15 and 36 months, 26,44,90 which urges caution whenever using early PSA as a surrogate for efficacy. Most SBRT trials continue to use the Phoenix definition of biochemical failure (nadir + 2 ng/mL), even though this definition was originally developed as an early end point for patients undergoing conventionally fractionated radiotherapy. There are insufficient data as yet to suggest whether this definition is the most appropriate for patients undergoing SBRT or whether an alternative definition should be used. The PACE trial also incorporates the use of the original ASTRO definition of biochemical failure (3 consecutive PSA rises) within the first 24 months, with the aim of avoiding benign PSA bounces post-SBRT being classified as biochemical failure.
Stereotactic Body Radiotherapy for Local Recurrence
With the advent of improved imaging techniques such as prostate-specific membrane antigen positron emission tomography, isolated prostate-only failures are becoming increasingly recognized. There are a number of small series, albeit with limited follow-up and highly selected patient populations, which have explored the use of SBRT in the setting of local failure. A systematic review of patients receiving pelvic reirradiation with SBRT published in 2017 found 4 studies of prostate cancer with 82 patients. 92 Most of the patients on these studies had intraprostatic or prostate bed recurrence and received ADT. The largest prospective series reported on 29 patients with biopsy-proven locally recurrent prostate cancer treated with SBRT reirradiation without ADT to the whole prostate to 34 Gy in 5 fractions. 93 Median follow-up was 24 months, and, in this time, there were no local failures, with a 2-year bRFS of 82%. Toxicity was acceptable with 7% of patients, experiencing ≥ grade 3 GU toxicity and no severe GI toxicity. The largest retrospective series recently published in 2018 included 50 patients who received SBRT reirradiation to 30 Gy in 5 fractions. 94 Eleven patients were on ADT at the time of SBRT. With a median follow-up of 21 months, 27 (54%) patients had no evidence of disease, 3 (6%) patients pursued ADT with stable PSA levels, and 20 (40%) patients experienced biochemical relapse. Only 1 patient had a severe late toxicity, being grade 3 hematuria. Another recent retrospective study analyzed 18 patients who underwent focal reirradiation with SBRT for intraprostatic recurrence to 35 Gy in 5 fractions. 95 With a short median follow-up of 14.5 months, 10 patients had biochemical no evidence of disease, 5 patients had biochemical recurrence after an initial response, and 3 patients did not respond to SBRT. Treatment was reasonably well tolerated, with 1 late grade 4 GU toxicity and no late grade 3 or 4 GI toxicities. Although these series have a number of limitations, the results are promising and suggest that SBRT may offer a comparable if not favorable alternative to salvage treatment options such as surgery, although further prospective research with larger numbers in this area is needed.
Future Directions
Numerous randomized studies are ongoing that will soon shed light on the comparative efficacy and toxicity of SBRT. These include the Scandinavian HYPO-RT-PC trial comparing SBRT to CFRT, for which early toxicity results are available, and the United Kingdom-led international PACE trial, which includes patients from the United Kingdom, Canada, and Ireland and compares SBRT to surgery (PACE-A) or CFRT/moderately hypofractionated RT (PACE-B) (NCT01584258). The PACE-B has now fully recruited 872 patients with data maturing. The role of SBRT in high-risk patients, however, is still to be elucidated, as well as the role of adjuvant systemic options such as ADT.
Emerging technologies, including the use of KIM and real-time MRI image guidance systems, will likely translate into even lower rates of toxicities. These technologies may also facilitate the safe escalation of even higher daily fractions and potentially the reduction in the number of fractions, including the use of single-fraction radiotherapy in the future. Magnetic resonance image guidance may also enable incorporation of daily adaptive radiotherapy planning, allowing for accommodation of any changes to the prostate or rectal anatomy, without adversely affecting the dosimetry to either the target or OARs.
Conclusion
Multiple prospective studies with medium-term follow-up support the use of SBRT in low- and intermediate-risk localized prostate cancer, with reported high rates of biochemical control and low rates of late toxicity. Additionally, SBRT has practical and economic advantages to alternative modalities, with the potential for large cost reductions at a governmental and patient level, and improved radiotherapy access and waiting times for patients (see Table 4 for advantages and disadvantages of SBRT). Forthcoming randomized trials will allow us to better compare SBRT outcomes with alternative treatment modalities, as well as optimize radiotherapy dose, schedule, and volumes. Further research into the role of SBRT and ADT in high-risk patients, as well as incorporation of emerging technologies, will allow us to continue to improve outcomes for our patients.
Advantages and Disadvantages of Stereotactic Body Radiotherapy.

Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew Loblaw has relationships with AbbVie, Sanofi, and TerSera. Drew Moghanaki has received honoraria and travel expenses from Varian Medical Systems.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Alison C. Tree has received research funding from Elekta and Accuray and honoraria/travel expenses from Elekta and Ferring. Nicholas J. van As has received research funding and consulting fees from Accuray. Piet Ost has institutional receipt of grants and research support from Merck, Bayer and Ferring, and receipt of honoraria or consultation fees from Astellas, Bayer, Ferring, and Janssen.